HIV AND AIDS KNOWLEDGE, ATTITUDES,
PRACTICES AND BEHAVIOUR (KAPB) STUDY IN
NAMIBIA
KEY FINDINGS
Acknowledgments
The key findings of the KAPB study will support the GRN-UNICEF Country Programme interventions for 2006-2010 with particular emphasis on HIV prevention for young people. We acknowledge the work of Research Facilitation Services, Namibia, for their expertise in developing the tools, data collection, processing and reporting. We also acknowledge the all out support of the Regional Directors for
Education, school principals, teachers and learners of schools and community members from Omaheke, Ohangwena and Kavango Regions. The study was made possible with the financial support from SIDA and German National Committee for UNICEF. The HIV Prevention Programme of UNICEF provided technical support and overall guidance.
TABLE OF CONTENTS
EXECUTIVE SUMMARY... i
1. INTRODUCTION... 1
2. METHODOLOGY AND RESEARCH PROCEDURES ... 1
2.1 Questionnaire... 1
2.2 Sample Selection and Size ... 2
2.3 Fieldwork Procedures ... 2
2.4 Statistical Procedures ... 3
3. SEXUAL KNOWLEDGE, ATTITUDES AND BEHAVIOURS ... 4
3.1 10-14 Age Group... 4
3.2 15-24 Age Group... 5
3.3 Adults ... 7
4. CONDOM USE AND ATTITUDES ... 8
4.1 10-14 Age Group... 8
4.2 15-24 Age Group... 8
4.3 Adults ... 10
5. RISK MANAGEMENT AND HIV RISK PERCEPTIONS... 11
6. STIGMA AND HIV ANXIETY... 13
7. SOCIAL RELATIONSHIPS ... 14
7.1 Access to emotional support ... 14
7.2 Parental Monitoring and Connectedness ... 14
7.3 Intimate Discussions with Parents and Caregivers ... 15
7.4 Teacher Connectedness ... 16
7.5 Exposure to Antisocial Behaviour... 17
7.6 Sexual Abuse ... 18
8.0 ALCOHOL ABUSE ... 19
9. ORPHANS ... 21
10. PROGRAM PARTICIPATION AND IMPACT ... 22
Executive Summary
The main purpose of this study was to assess the current state of HIV risk behaviour through knowledge, attitudes and practices of young Namibians aged 10 to 24 as a baseline and to inform future programming. This study was conducted in three regions namely: Kavango, Omaheke and Ohangwena. It captured the perceptions of 1000 respondents in three categories: 10-14 year olds, 15-24 year olds (in and out of school) and adults. A particular emphasis was placed on the most sexually active group of 15-24. This summary reflects the key findings only. For an in-depth analysis and to review statistical procedures, reference should be made to the main report. Some of the key results include:
Knowledge of HIV transmission and prevention is high amongst youth but knowledge of sexually transmitted infections (STIs) is extremely low.
Males are more likely to take sexual risks than females for instance; younger male
respondents are less likely to use condoms. Males are more likely to engage in sexual risks due to their direct actions while females are put at risk through actions of their partners. The 10-14 year old group expressed most stigma and the most negative attitudes towards HIV-positive people. There is less stigma in older groups and the least in the adult group. HIV anxiety was highest amongst 10-14 years and least among adults.
Condom efficacy is lowest among females 15-24 years. Coupled with the fact that they are more likely to have sex with unfaithful partners, they are particularly vulnerable to HIV. As age increases intent for safe sex declines and more people put themselves at risk for HIV through their own sexual experiences.
The most important social relationship that young people report having is with their parents. Discussions of HIV/AIDS were the most common between parents and children.
Exposure to antisocial behaviour is extremely high which could have detrimental effects on young people.
One in four respondents of the 10-14 year olds and 15% of the 15-24 year olds experienced one or more forms of sexual abuse.
Alcohol abuse was the only single significant risk factor that contributed to the spread of HIV through higher sexual risk taking. Exposure to antisocial behaviour regarding alcohol use
and drunkenness was extremely high among 10-14 and 15-24 year olds.
Key Indicators for 15-24 year olds M F Value
% Young people voluntary requesting an HIV test 12.2% 15.3% 27.5%
% Young people requesting an HIV test and received their results 40.6% 50.9% 91.5%
% Young people with multiple partners in past year 10.3% 5.5% 15.8%
% Young people who could correctly identify two ways of HIV transmission 50.9% 48.7% 99.6% % Young people correctly identifying two ways of preventing sexual
transmission of HIV
50.9% 48.7% 99.6%
% Condom use at last sex 42.0% 34.4% 76.4%
Median age of sexual debut 15
years
16 years
15 years
% Youth using alcohol at least once a month 11.7% 8.7% 19.7%
% Youth ever sexually involved 29.5% 20.7% 50.2%
% Young women ever pregnant - 18.9% 18.9%
% Youth having sexual intercourse before age 15 10.9% 4.9% 15.8%
% Youth confident of using condoms correctly 37.2% 36.3% 73.5%
% Youth whose parents have discussed HIV with them 40.6% 40.4% 81.0%
% Youth whose parents have discussed sexuality with them 25.4% 25.5% 50.9%
1. INTRODUCTION
The Government of Namibia and UNICEF Country Programme (2006-2010) has a strong emphasis on prevention, care, support and impact mitigation of HIV/AIDS on critical services for
women and children. The strategic focus is on three main components: Maternal and Child
Survival and Development, Education for HIV Prevention and Mitigation, and Special Protection
for Vulnerable Children. This study was commissioned to act as a baseline for the programme
component on HIV prevention among young people and to assist in strengthening interventions that reduce risk behaviour among young people. Research Facilitation Services (RFS) conducted a Knowledge Attitude Practice and Behaviour (KAPB) survey for UNICEF during March and April 2006.
The main purpose of the study was to assess the current state of HIV risk behaviour through knowledge, attitudes and practices of adolescents and young Namibians aged 10 to 24 as a baseline and to inform future programming. The study also assessed stigma and anxiety, condom use and attitudes, self-efficacy and HIV risk perceptions. A detailed analysis was carried out regarding social relationships looking at issues including emotional support, parent and teacher connectedness, exposure to antisocial behaviour and sexual abuse. Alcohol abuse was scrutinized exclusively. A brief review of orphans was also conducted. Finally programme participation and impact, including some recommendations for programme implementation is discussed. This paper will only summarize the key findings and will highlight the salient information. For detailed data and statistical analysis please refer to the complete report available in electronic format from UNICEF upon request.
2. METHODOLOGY AND RESEARCH PROCEDURES
2.1 Questionnaire
The questionnaire was developed with key indicators adapted from pertinent resources such as the Demographic Health Survey and from UNICEF’s global guidelines taking into account the programme interventions supported by UNICEF Namibia. Three different questionnaires were developed: one for the 10-14 year olds, one for 15-24 year olds and another one for adults. The 10-14 year old and 15-19 year old questionnaire covered school-going children. The 10-14 year old age group is of significant importance as it is this group that will become sexually active and this is a window of opportunity to target specific programming at this group. Ascertaining behaviour among this group would help us understand the attitudes, and risk perceptions around sexual issues, including HIV/AIDS. The 15-24 age group is probably the most critical group as this is the stage when youth engage in sexual activities and potentially put themselves at risk. The 15-24 year old questionnaire included out-of-school youth to ensure that the breadth of perspectives would be covered. The adult sample included parents who were above 30 years with children between the ages of 10-19. The rationale for including this group in the survey was to provide contextual information about the socio-personal and relational environment within which the children and youth grow up. This would further inform of the potentially important generational gaps that might exist between the youth and their parents/caregivers on issues relevant to HIV/AIDS including their risk perceptions.
Certain sections of the survey were designed to be comparable across the three questionnaires. The questionnaires were developed in consultation with UNICEF, and piloted extensively. In addition, two focus groups were conducted amongst 10-14 year olds in order to make the language and content “child-friendly”.
2.2 Sample
Selectionand Size
The sample was selected based on a non-random, clustered-based means that revolved around school clusters. The sample was purposive and selected for My Future My Choice participants and orphans to ensure these groups were adequately captured. The clusters of schools were randomly selected, and included at least two to three different constituencies in each region and captured both rural and urban populations. Once the clusters of schools were identified, the selection of students in schools was left to teachers and principals to determine MFMC participation and to include orphans in a non-discriminatory manner using pre-defined guidelines. A random, systematic sampling method was employed for selection of households around the selected schools for the adult survey.
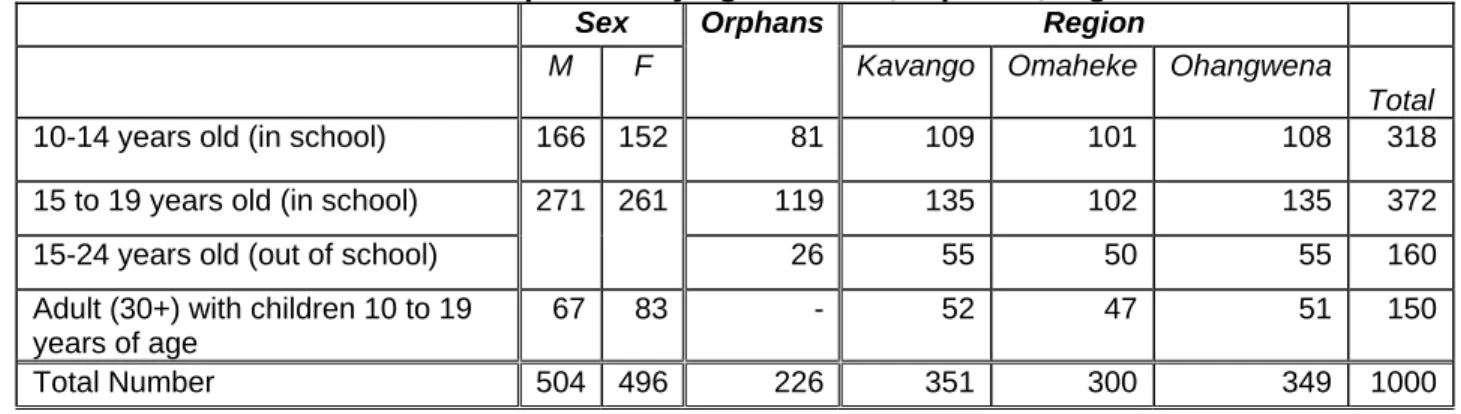
The study was conducted in 3 regions (Omaheke, Kavango and Ohangwena) with a total sample size of 1000 divided in 4 groups as outlined in Table 1. The sex ratio was balanced with approximately 50% males and 50% females. Orphans represented 226 of the respondents.
Table 1. Sample size by age and sex, orphans, region
Sex Region
M F
Orphans
Kavango Omaheke Ohangwena
Total
10-14 years old (in school) 166 152 81 109 101 108 318
15 to 19 years old (in school) 119 135 102 135 372
15-24 years old (out of school)
271 261
26 55 50 55 160
Adult (30+) with children 10 to 19 years of age
67 83 - 52 47 51 150
Total Number 504 496 226 351 300 349 1000
The study does NOT reflect national figures and is specific to the clusters sampled. Nevertheless, some inferences will be made that will help explain the current situation and inform future programming.
2.3 Fieldwork Procedures
RFS employed trained interviewers with skills from different language groups. The interviewers had experience in interviewing and the survey methods, and were specifically trained and familiarized with the questionnaires. Fieldwork teams consisted of four interviewers and one supervisor each. No names were recorded on the questionnaire. The questionnaire was administered specifically to each group. For the 10-14 age group, a parental consent form was received from each respondent. The questionnaire was explained item by item to this and those who did not understand a question were individually assisted. The 15-19 age group in-school self-administered the questionnaire. The out-of-school youth (15-24) and the adults were individually interviewed. The participants were provided with some incentives such as refreshments for their participation. The field supervisors reported to the RFS offices on a daily basis. Upon completion of data collection, the questionnaires were checked for quality, and then coded and captured in SPSS1 format at the RFS offices. Fieldwork was also facilitated with the official support of the Regional Education offices in the respective regions.
1
2.4 Statistical Procedures
Several statistical methods were used in this study, which include: data reduction through factor analysis, reliability analysis, regression techniques, multi-variate analysis, and correspondence analysis. The report will only reflect the statistically significant findings and the corresponding values will not be included in this report. For more statistical information and values see complete report.
3. SEXUAL KNOWLEDGE, ATTITUDES AND BEHAVIOURS
Knowledge or having the correct information is one of the primary steps and a precursor to attitude and behaviour change. The cohort or age specific analysis will help us deduce some of these behaviours. Knowledge of STIs including HIV, knowledge of transmission and prevention of HIV and other sexual variables were considered. Overall the knowledge level of STIs other than HIV was much lower as illustrated in Figure 1. Knowledge of chlamydia, herpes and genital warts was the lowest of all STIs. This remains of serious concern that requires action because of the association between HIV and other STIs.
Figure1: Knowledge of STI’s all age groups
0 20 40 60 80 100 HIV Syphilis Gonorrhea Genital warts Herpes Chlamydia 10-14 years
15-19 years (in school) 15-24 years (out of school) Adults
3.1 10-14 Age Group
Knowledge about HIV/AIDS was high among this group (96.5%) and knowledge about transmission was higher than that of prevention. However, knowledge of other STIs was very low for this group.
When asked about relationships and sexual activity, 87.4% reported not being in a relationship
and 91.8% had not had sex. Among those who had had sex, the median age of sexual debut
was 13 years. From those who had had sex (26 out of 318), 50% reported to have had sex because they wanted to, 42.3% because they were forced to and 7.7% because they were paid or received a gift. Also from those who had sex, approximately half had sex with someone the same age as themselves and 34.6% had sex with someone older or much older. More notably, 23.1% had their first sexual encounter with someone ten or more years older. Of those who engaged in sexual activity only a third (34.6%) reported condom use the last time they had sex. Even though the actual number of sexually experienced children in this age group is very small, there is concern about the nature of sexual relations particularly intergenerational sex. Sexual
patterns at this young age needs to be addressed, as this might become the established norms for sexual relations later. In addition, exposure to high risk this early in life results in more prolonged exposure to risk and increases the likelihood for HIV infection. In this age group, pregnancy was not a common occurrence.
Concerning Sexual Issues
Among 10-14 year olds who have had sex, 42.3% were forced and 23.1% had their first sexual encounter with someone ten or more years older.
Among 15-24 year olds, 18.3% were forced to and 7.3% had their first sexual encounter with someone ten or more years older
3.2 15-24 Age Group
Knowledge about HIV/AIDS was high among this group (96.4%) while knowledge of STIs was very low among this group. The 15-24 year old out-of-school respondents knew more about STI than their in-school counterparts. In the out-of-school youth, knowledge of HIV transmission was similar to knowledge of prevention. In the in-school youth knowledge of HIV transmission was higher than knowledge of prevention. Age and being out of school were positive predictors of knowledge for STIs other than HIV/AIDS. An explanation for this could be because those out of school are older and more exposed to STIs and hence more knowledgeable.
Overall 50.4% of those in the 15-24 year olds age category had had sex and the median age of
sexual debut was 15 years. There are quite significant gender differences with 58.3% of males and 42.1% of females being sexually active. Of those who had sex 75.7% had sex because they wanted to, 18.3% because they were forced to, and 6% were paid or offered a gift. About one-third had their first sex with a person older or much older than themselves, and about half had their first sexual encounter with someone their own age. Only a quarter of those who had sex were not in relationships. In total, 54.9 % (29.7% of males and 25.2% females) of respondents in the 15-24 year old group were in relationships. From those who were in-school only 43% were in relationships while 82.5% of out-of-school youth were in relationships.
The median number of sexual partners for the 15-24 year olds was 2 since they started having sex and 1.87 partners in the past year. The majority (91.4%) have had between one to five sexual partners. Once someone has become sexually active, it is unlikely that they would not continue to have sexual relations.
Pregnancy among the 15-24 year olds merits some attention. In this age group 18.9% (50 out of 265) of women have been pregnant before, of which 60% was the result of voluntary sex while 40% was due to forced sex. In 78% of the cases, the mother and father were in a relationship at the time of pregnancy. In 56% of the cases the father was either older or much older than the mother, and in 32% of cases they were of the same age.
Risk behaviour was assessed through a self-reported risk index where only respondents who had engaged in sex identified the risks they had taken. It should be noted that people tend to under-report their own risk but the assessment of risk factors has important implications. The most common risk actions for this age group were sex with an unfaithful partner (36.7%), having multiple partners (31.1%), possibly having a STI (23.6%)2, and having unprotected sex (17.6%), having sex against one’s will (14.6%) and having sex with someone one did not know well
2 Have been for an STI test is regarded as a proxy for having contracted a STI because it is unlikely that someone without any symptoms or suspicion of having a STI would go for such a test.
(13.9%). Male and female respondents show much the same risk profile with regard to the five most common risk activities: multiple sexual partners, sex with an unfaithful partner, sex with someone much older, sex against one’s will and possibly having a STI. However, there are some significant differences between the types of sexual risks taken by males and females as described in Table 2.
Table 2: Types of sexual risks taken: male and female
Male Female
More than one sexual partner 35.0 25.5
Unprotected sex with one or more partners 19.7 14.5
Sex with a partner who I know cheats on me 34.4 40.0
Sex with someone who is much older than me 9.6 10.0
Sex with someone I did not know well 17.8 8.2
Sex with someone who paid me or gave me a gift to do so 5.7 4.5
I have/had paid someone to have sex with me 10.2 3.6
I have/had sex against my will 15.3 13.6
Sex with more than one person at the same time 4.5 1.8
I have been tested for a STI 22.9 24.5
I have/had showed signs of a STI 7.6 2.7
I have/had anal sex with one or more partners 5.7 1.8
These sexual risk profiles suggest that men are more likely to be put at risk by means of their direct actions, whereas women are put at risk through the actions of their partners. Men do take more sexual risks than women overall.
In the 15-24 year old group, 72.6% knew of a place where they could get tested for HIV, but only 27.5% had been tested for HIV before. 91.5% of those who had been tested for HIV went back for their results. The nine respondents who had not gone back for their results provided three reasons for this: intention to go in the future, not having had time to go, or being afraid to go back. Therefore encouraging sexually young people to get tested would be an important intervention to focus on, as well as, a good opportunity and venue to provide them with information on sexual and reproductive health.
Gender dynamics in sexual behaviours among 15-24 year old respondents
More males (79.1%) than females (70.9%) had their first sexual encounter because they wanted to.
More females (23.6%) than males (14.6%) had their first sexual encounter because they were forced to.
Males and females are equally likely to have a gift in exchange for sex during the first encounter (6.3% and 5.5% respectively).
Females (41.8%) are far more likely than male respondents (17.1%) to have had their first encounter with someone older than themselves.
Males (53.8%) are far more likely than female respondents (37.3%) to have a first encounter with someone of the same age.
Male respondents (13.3%) are more likely than female respondents (5.5%) to have a first encounter with someone younger than them.
3.3 Adults
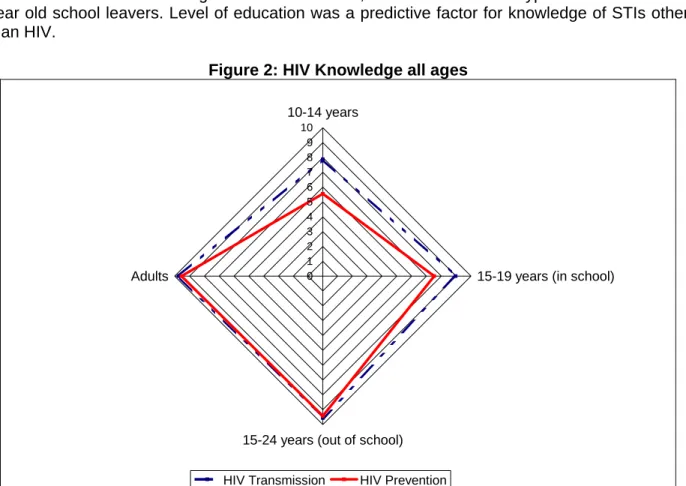
With regard to knowledge of HIV prevention and transmission, knowledge among adults was
the highest among all groups surveyed and very similar to that of the 15-24 year old out-of-school youth as illustrated in Figure 2. While HIV was identified as an STI, knowledge of other STIs still remains low among this group. In fact, with the exception of Herpes and Chlamydia, the adults had less knowledge about Gonorrhoea, Genital Warts and Syphilis than the 15-24 year old school leavers. Level of education was a predictive factor for knowledge of STIs other than HIV.
Figure 2: HIV Knowledge all ages
0 1 2 3 4 5 6 7 8 9 10 10-14 years
15-19 years (in school)
15-24 years (out of school) Adults
HIV Transmission HIV Prevention
The median age of sexual debut among the adult sample was 20 years, which was 5 years
older than that of the 15-24 year group and 7 years older than the sexually active among the 10-14 year old group. This suggests that there is a significant decrease in age of sexual debut from one generation to the next, something which would have a significant impact on the vulnerability of future generations. Less than 10% of the adult sample had their first sexual encounter before the age of 15, and 54% did so at 20 years or older. The potential explanation for the difference in age of sexual debut between adults and other groups may be that the older generations had more rigid regulations around sexuality and were exposed to sex more in the traditional sense through cultural norms. About one-third of this sample had their first sexual encounter with someone older than them which is similar to the 15-24 year old group. More than one in five respondents (23.3%) had a first encounter with someone younger than themselves.
Among adults, 80.7% knew of a place where they could get tested for HIV, but only 50.4% had gone for testing. Only one person did not go back for his results, the reason for this being that he/she was afraid.
4. CONDOM USE AND ATTITUDES
By the time 10-14 year olds become sexually active, a large portion of them will be vulnerable to HIV due to their lack of confidence to use condoms correctly, their unwillingness to use it during sexual encounters and their incomplete knowledge on the preventative role of Condoms.
Most HIV education programmes include modules on condom and condom use as a method for preventing the spread of the virus. Such modules typically focus on:
1) promoting consistent condom usage as a means to preventing the spread of HIV; 2) teaching young people the correct way to use condoms;
3) enhancing their self-efficacy with regard to condoms to ensure that they are confident about condom use even under difficult circumstances; and
4) changing restrictive perceptions about condoms and their use in building associations between consistent condom use and a healthy life style.
With condoms being one of the most effective ways to prevent HIV/AIDS among the sexually active, attitudes towards condoms and condom use necessitates analysis by itself.
4.1 10-14 Age Group
Since the 10-14 year old age group was less likely to be sexually active, only a few questions of condom use were included in the questionnaire and therefore the findings should be interpreted with caution. The proportion of respondents who felt confident that they could use a condom correctly (43.4%) are equal in size to that of respondents who claimed that they could not use a condom correctly (43.1%). A further 14% was unsure about their ability to use condoms correctly. When asked about their future intent to use condoms, 61% agreed that they would ensure that a condom is used whenever they have sex, 25% said no and 13.5% were undecided. Although members of this age group are generally aware of the potential role of condoms in the prevention of HIV infections, a substantive number are still unconvinced of its benefits. Some 19% disagreed or were unsure that condoms can prevent HIV infections if used with a new partner, and 31.5% disagreed or were unsure that condoms used with a sex worker can reduce risk for HIV infection. A substantive number of 10-14 year olds will be vulnerable as soon as they become sexually active due to the lack of confidence to use condoms correctly, the low future intent to use condoms, and the incomplete knowledge of the preventative role of condoms. This is one area where a specific focus in future programmes is required.
4.2 15-24 Age Group
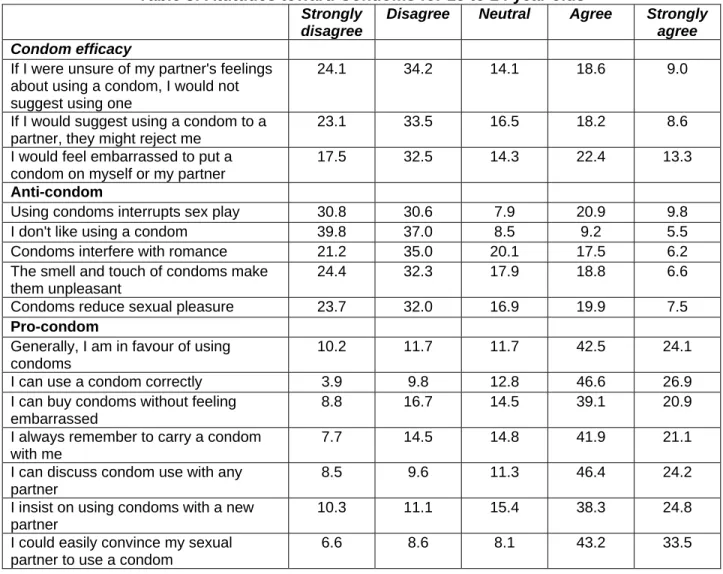
Among the 15-24 year olds attitudes towards condom used was measured extensively as this is the most sexually active group. Significant proportions of 15-24 year olds did not have favourable views on condoms as demonstrated through Table 3. Overall almost 77% of sexually active respondents used a condom the last time they had sex. Men (71.4%) are significantly less likely to have used a condom during their last sexual encounter than women (84.1%). Those respondents still in school (70.9%) are also significantly less likely to have used a condom than those who are no longer in school (82.7%). Thus, although condom use is high overall, significant gender and age gaps do exist and it is the younger and male respondents who are less likely to use condoms.
Table 3: Attitudes toward Condoms for 15 to 24 year olds Strongly
disagree
Disagree Neutral Agree Strongly agree Condom efficacy
If I were unsure of my partner's feelings about using a condom, I would not suggest using one
24.1 34.2 14.1 18.6 9.0
If I would suggest using a condom to a partner, they might reject me
23.1 33.5 16.5 18.2 8.6 I would feel embarrassed to put a
condom on myself or my partner
17.5 32.5 14.3 22.4 13.3
Anti-condom
Using condoms interrupts sex play 30.8 30.6 7.9 20.9 9.8
I don't like using a condom 39.8 37.0 8.5 9.2 5.5
Condoms interfere with romance 21.2 35.0 20.1 17.5 6.2
The smell and touch of condoms make them unpleasant
24.4 32.3 17.9 18.8 6.6
Condoms reduce sexual pleasure 23.7 32.0 16.9 19.9 7.5
Pro-condom
Generally, I am in favour of using condoms
10.2 11.7 11.7 42.5 24.1
I can use a condom correctly 3.9 9.8 12.8 46.6 26.9
I can buy condoms without feeling embarrassed
8.8 16.7 14.5 39.1 20.9 I always remember to carry a condom
with me
7.7 14.5 14.8 41.9 21.1 I can discuss condom use with any
partner
8.5 9.6 11.3 46.4 24.2 I insist on using condoms with a new
partner
10.3 11.1 15.4 38.3 24.8 I could easily convince my sexual
partner to use a condom
6.6 8.6 8.1 43.2 33.5
Females between 15 and 24 generally have the lowest condom efficacy suggesting that their vulnerability stems from the fact that they are less capable of insisting that condoms be used during sexual encounters. Their problem is thus related to notions of relational power and influence. Within the same group, negative feelings towards condoms are associated with age and with years of sexual activity but not with the number of sexual partners an individual has had. Older members of this age group who are sexually active are more likely to have negative feelings about condoms and have lower efficacy in using them. There is also a statistically significant relationship between the number of sexual risks an individual has undertaken in the past year, and anti-condom feelings and low efficacy. Sexually active individuals, who have undertaken one or more sexual risks, have more negative feelings towards condoms and lower efficacy than those who did not take a single risk.
Slightly over 50% of 15-24 year olds were accessing condoms through clinics and hospitals and approximately 22% from shebeens and 22% from local shops. Very few youth were accessing condoms through schools (approximately 1%).
4.3 Adults
Among the adults surveyed, current condom use was 30%. Approximately half of the adults (47.3%) have used a condom before even though they might not use it currently. Over 70% of adults were in favour of using condoms, about 30% did not like using condoms, 35% felt it interfered with romance. Many adults felt that condoms encouraged young people to have sexual intercourse (56%). Figure 3 illustrates some of the attitudes of condom use for 15-24 year olds and adults. The main difference between the two groups is that more adults (33%) don’t like using condoms compared to only 15% among the 15-24 year olds. Most of the other condom attitudes of adults are mirrored by the 15-24 year olds.
Figure 3: Attitudes of Condom Use for Adults and 15-24 year olds
0 10 20 30 40 50 60 70
Condoms interrupt sex play I don't like using condoms I am in favour of using condoms Condomes interfere with romance Smell and touch of condoms makes them
unpleasant
Condoms reduce sexual pleasure
% Agreement
5. RISK MANAGEMENT AND HIV RISK PERCEPTIONS
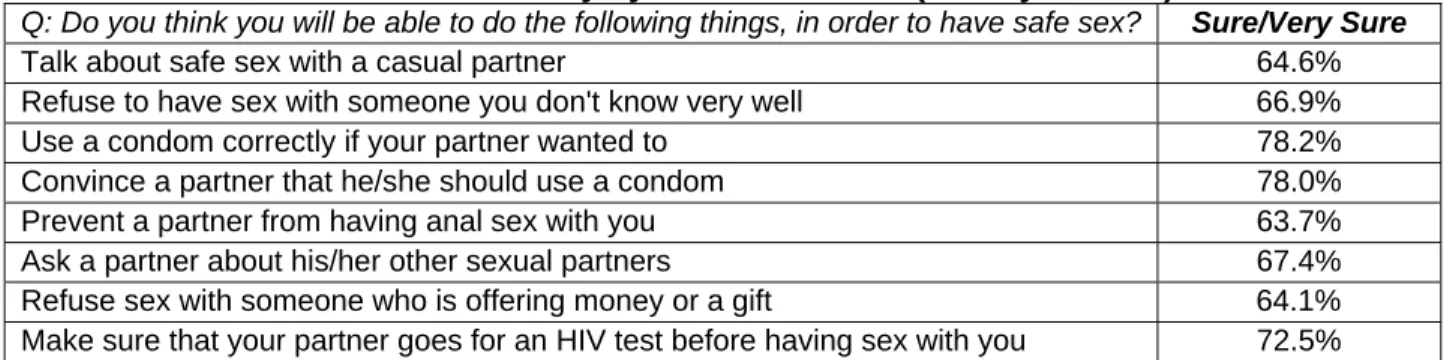
A key factor in the management of risk is an individual’s ability to assert him or herself in a potentially risky situation in order to avoid or at least reduce that risk. Self-efficacy for reducing HIV risk behaviour was measured among 15-24 year olds only by means of eight items included in Table 4. Self-efficacy based on ability to convince partners to use condoms and to use a condom correctly is highest overall. On the negative side, self-efficacy is lowest when it comes to negotiation with casual partners and during transactional sex. Ideally, self-efficacy should be much higher overall, and much higher across all items, because even where efficacy is at its highest, one-in-five respondents will not be able to assert themselves successfully. As most HIV education and awareness programmes usually have a strong focus on condom usage, it is perhaps not surprising that items related to condoms are connected with highest self-efficacy.
Table 4: Self-efficacy by individual items (15-24 year olds)
Q: Do you think you will be able to do the following things, in order to have safe sex? Sure/Very Sure
Talk about safe sex with a casual partner 64.6%
Refuse to have sex with someone you don't know very well 66.9%
Use a condom correctly if your partner wanted to 78.2%
Convince a partner that he/she should use a condom 78.0%
Prevent a partner from having anal sex with you 63.7%
Ask a partner about his/her other sexual partners 67.4%
Refuse sex with someone who is offering money or a gift 64.1%
Make sure that your partner goes for an HIV test before having sex with you 72.5% Self-efficacy for reducing risk behaviour was 3.7 (on a 5 point scale) which was slightly above the midpoint therefore suggests only very modest self-efficacy across this group. Also age is directly correlated with self-efficacy, which means that self-efficacy increases with age. It is therefore not surprising that the out-of- school youth had a slightly higher self-efficacy of 4.02 compared to 3.90 of those in school.
HIV Risk perception is a key element of risk behaviour where an individual’s self-assessment of his or her own risk of contracting or being exposed to HIV. This is different from the actual sexual risks taken as discussed in Section 3. Past surveys showed that respondents typically underestimate their own risk. Respondents in the 15-24 year age group and adults were asked to assess their own risk through several items categorized in 3 groups:
1. Self reported personal risk consists of four items: my sexual experiences make it very likely
that I will get HIV/AIDS; I may have HIV /AIDS; I may have had sex with someone who was very likely to have HIV/AIDS; I am very likely to get HIV/AIDS. Only one in five or less respondents reported themselves to be at risk from HIV, most reported their risk to come from sexual experiences. Self-reported risk correlates significantly and positively with age which means that older respondents are likely to report higher risk for contracting HIV than younger respondents.
2. Denial of personal risk consists of three items: people like me do not get HIV/AIDS; I am
healthy so my body can fight off an HIV infection; I am too young to get an HIV infection. More than one in four respondents felt that “people like them” do not get HIV, slightly less felt they were healthy and thus could fight off an HIV infection, and a further 23% felt that they were too young to contract HIV. Overall and across all three items, more than one in five respondents felt
that they were not at risk. The only statistically significant factor was that those in school were more likely to deny that they are at risk than those out of school.
3. Intent to practice safe sex consists of four items: I will make sure that a condom is used when
I have sex; I do not plan on having sex until I am married; I would only have sex with a person with whom I’ve had a long term relationship; and I will not have sex with someone who refuses to use a condom. Intent to have safe sex is most clearly articulated in terms of condom use with more 73.1% indicated that they would make sure a condom is used when having sex, and 65% indicated that they would not have sex if no condom is used. Only 50% of the respondents were willing to abstain until married, and less than two in five are willing to confine sex to a monogamous relationship. Respondents currently in school showed statistically significant higher intent to practice safe sex than those who left school. Age and intent for safe sex are negatively correlated which means that as age increases the intent for safe sex declines and vice versa.
Adults perceived themselves to be more at risk than 15-24 year olds with their sexual experience putting them most at risk for HIV/AIDS.
6. STIGMA AND HIV ANXIETY
Stigma was most apparent in the 10-14-age group: Children among this group would like to see HIV+ children kept out of school, they do not want to be friends with HIV+ children, would not buy food from a HIV+ seller, they would like to keep the infection of a family member secret and feel that someone with AIDS should not be allowed to work where food is sold. These responses may be expected as children this age may not understand the epidemic fully and are afraid to have any interactions with the disease. Nevertheless, this information is critical to ensure that interventions in this age group promote pro HIV+ messages and aim at curbing stigma.
In-school 15 to 19 year olds supported the notion that HIV+ teachers who are not yet sick should be allowed to teach. The view most closely associated with the 15-24 year olds and adults is that they would care for a family member who has AIDS. Age had a positive correlation with stigma and therefore those in higher grades had more pro-HIV+ attitudes. There was a small but significant difference between male and female participants with women being slightly more pro-HIV+. Generally, there is less stigma in the older groups and the least in the adult group. This could be explained by the fact that they more exposed to HIV through dealing with care and support of the sick. This is encouraging in terms of role modelling behaviour for their children.
Anxiety is an uncomfortable feeling caused by a fear that something bad might happen and has a potential to shape risk behaviour. Anxiety about getting infected with HIV could potentially inspire someone to reduce his or her risks. Anxiety about HIV/AIDS might be caused by personal experiences or consistent exposure to the media and/or other sources of mass information. More anxiety is to be found among the younger age groups, with adults being least anxious on all items. Education reduced general anxiety and those out-of-school had more general anxiety than their in-school counterparts. Most respondents had more general anxiety (“I am afraid of getting AIDS”, “I worry about the disease in general”, “Because of AIDS, I feel nervous about making the first move to have sex”) than personal anxiety (“That a partner may be positive”, “That HIV might influence me, my family or friends” and “that I might be HIV positive”) which suggests that HIV anxiety is removed from personal experience.
7. SOCIAL RELATIONSHIPS
The environment within which children and adolescents find themselves as they grow up is important for their socialization. It forms and shapes key attitudes, values and important elements of behaviour. Much of their environment stems from their relationships with others such as their parents, caregivers, teachers and peers. This section explores how and in what ways the surrounding environment within which young Namibians grow up influences their risk behaviour.
7.1 Access to emotional support
Most people in the 10-14 year old group were close to their parents and rely heavily on family for emotional support. When asked if they were worried about something, 72% felt they could talk to their parents or caregivers, while 9% talked to siblings and 7% to other family members. Only 3% consulted with peers or friends, 4% talked to their teachers and 2% had no one to talk to when they were worried about something.
The emotional support system of the 15-24 year olds is quite different from that of the 10-14 year olds. When they felt worried, the reliance on parents was 55%, on siblings was 11%, other family members was 7%, and teachers was only 2%. Almost 4% indicated that they had no one to turn to and 15% demonstrated a higher reliance on friends.
7.2 Parental Monitoring and Connectedness
The most important social relationship young people have is with their parents. Parental monitoring consisted of four items: knowing where children are after school, children having to
call when late; knowing where children are if out; and knowing who children are with when out.
When parental monitoring was assessed among the 10-14 year olds the following general observations were made: 1) parental monitoring is less strict for boys than for girls in this age group; and 2) parental monitoring is only slightly lower in the more rural regions of the sample. Among the 15-24 age group, parental monitoring was significantly higher among those in-school than those out-of-school. One would expect parental monitoring to decline as children get older and become more independent but the converse happens with these 15-24 year olds. Parental monitoring among those in-school was positively and significantly correlated with school grade, which means that monitoring is more intense among those of higher grades.
Connectedness or closeness to parents was measured by means of nine question items as outlined in Figure 4. The parent connectedness scale also revealed that the majority of the 10-14 year olds felt close to their parents, as there was over 50% agreement on the nine question items. In fact, 77% felt that their parents/caregivers made them feel good about themselves, 74% felt they were understood, and 72% felt their parents listened to them. Also among the 15-24 year old sample, respondents positively connected to their parents with almost over 60% agreement on the nine question items. Some 80% of the 15-24 year olds felt that their parents let them know that they cared about them, some 77% made them feel good about themselves, some 75% felt their parents/caregivers understood when they told them things.
Figure 4. Parent Connectedness among 10-14 and 15-24 year olds (% Agree/Strongly Agree)
0 10 20 30 40 50 60 70 80 My parents/caregivers let me know that they care about me
My parents/caregivers really listen to me My parents/caregivers like to spend time with me My parents/caregivers are there when I need them My parents/caregivers make me feel good about myself My parents/caregivers care about my feelings My parents/caregivers trust me My parents/caregivers pay enough attention to me My parents/caregivers understand when I tell them things
15-24 years 10-14 years
7.3 Intimate Discussions with Parents and Caregivers
When discussions around sex and sexuality are considered, intimate discussions between parents and their children do take place as reflected in Figure 5. Among the 10-14 year olds, most discussions (58%) were about changes in ones body while growing up. Only 22% had discussions about sex with their parents/caregivers, 33% had discussions about reproduction, 37% discussed how to avoid pregnancies and a similar proportion discussed menstruation. Only 47% discussed how to avoid HIV/AIDS. Building on the relationships and increasing communication between parents and young children is an area that needs to be strengthened. Parents and caregivers would thus be a good entry point for programming and ensuring young people have the adequate information and skills.
Figure 5. Intimate Discussions between parents and children as reported by children/youth 0 10 20 30 40 50 60 70 80 90 Changes in Body Sex Reproduction Avoiding Pregnancy Avoiding HIV/AIDS Menstruation Percentage 15-24 years 10-14 years
As is to be expected, intimate discussions are more common with 15-24 year olds than with 10-14 year olds as this group is more sexually active. The most common discussion with parents among 15-24 year olds is about avoiding HIV/AIDS (81%). Surprisingly only 51% have discussed sex, and even less reproduction (48%). The fact that discussions about HIV/AIDS take priority is certainly positive. When adults were asked who should educate adolescents on sexual issues, over 80% felt that is the role of parents. The deficit lies in parents having the skills to communicate to their children. Discussions and the skills to discuss sexual issues between parents and their children should be encouraged.
Looking more closely at the discussions between parents and children with effect of age and gender, discussion about HIV/AIDS dominates among all groups. Discussions on sex were almost twice as likely to occur for male (69%) and female (72%) respondents who have left school than for those still in school (41% for both male and female). There might be an expectation that these discussions would take place in school and hence parents would not have to discuss these sensitive topics with their children. Further analysis revealed that females 15-24 tend to discuss more topics with their parents than males. Males out of school tend to discuss more topics with their parents than those in school. Age and school grade are significantly correlated with the number of topics discussed, suggesting that the number of intimate topics increase, as respondents get older.
7.4 Teacher Connectedness
After parents/caregivers and grandparents, teachers are the most important adults in any school going child’s life. Given that these children spend at least half their days in the presence of teachers, the potential influence of teachers is enormous and this could be positive or negative. With this in mind, this study assessed the extent to which children still in school feel connected to one or more of their teachers. Teacher connectedness was measured by six times each with a agree/disagree response.
Among the 10-14 year olds, close to 87% of children indicated that they enjoyed going to school; 82% has respect for their teachers; 71% cared about what their teachers thought of them; and 74% felt that they could go to one of their teachers if they have a problem. Less than
three in five felt close to one or more of their teachers. Among the 15-24 year olds, 89% indicated they enjoyed going to school; 88% has respect for teachers; 76% felt that they could go to one of their teachers if they had a problem; and 52% felt close to their teachers. The main difference between the 10-14 year olds and the 15-24 year olds was that the older group cared less what teachers thought of them (63%). Interestingly, among the 15-24 age group, teacher connectedness was positively and significantly correlated to parent connectedness and parental monitoring which means that those who are closer to their parents or caregivers have closer relations with their teachers.
Overall, the connectedness with teachers seems quite positive. Further analysis revealed that teacher connectedness is reduced over time as children grow older. However this information should be reviewed with caution as very few young people turned to teachers when something worried them. (4% in the 10-14 year age group, and 2% in the 15-24 age group). Nonetheless, It is apparent that teachers can play a significant role in children’s lives particularly at a younger age and can be effective agents to channel critical information and ultimately influence behaviour change.
7.5 Exposure to Antisocial Behaviour
Exposure to antisocial behaviour is an important aspect of youth socialization. It is likely that children’s current and future behaviour is shaped by the behaviour of adults around them. This was measured at two levels: antisocial behaviour between parents and caregivers (such as fighting, drunkenness, threats etc.); and antisocial behaviour amongst other adults around the house. It is important to bear in mind that only exposure was measured and not the frequency. Figure 6 illustrates the exposure of children and youth to antisocial behaviour.
Respondents were exposed to a substantive amount of antisocial behaviour even in the 10-14 year old age group. More than 60% were exposed to alcohol abuse and drunken behaviour, and approximately 55% to behaviour that frightened them. Approximately one in three were exposed to people having sex and the same proportion to people using drugs. In their own households, some 45% were exposed to their parents drinking and being drunk, and some 35% to their parents shouting at each other. More than one in five has seen their father beating their mother, and 16 % witnessed a parent being threatened with a gun.
Overall, 15-24 year olds report more exposure to antisocial behaviour than 10-14 year olds. As is the case with 10-14 years old, the most exposure was to people abusing alcohol and being drunk (68%) and being scared by the behaviour of others (55%). Nearly one-in-two (48%) was exposed to their parents being drunk and two-in-five (40%) were exposed to other people using drugs. Nearly one-in-two (46%) was exposed to others having sex and 35% were exposed to people screaming at each other. Slightly more than seven in ten (73%) have been exposed to some form of inter-personal abuse3 either by their parents/caregivers or by others. This means that exposure to inter-personal abuse is also the norm rather than the exception. Further analysis revealed that those out-of- school have significantly higher exposure to inter-personal abuse and alcohol abuse than those in-school. This is probably due to the fact that those out of school spend more time in the home environment.
The exposure to antisocial behaviour is disturbingly high and necessitates some interventions. One can infer that young Namibians grow up in a social environment that contains a substantive amount of antisocial behaviour, which could heavily influence their sexual risk behaviour.
3
The following items are included here: people behaving in a way that frightened you, parents/caregivers being threatened with a weapon, parents/caregivers screaming and shouting at each other, parents/caregivers calling each other names, and actual beating of one parent by the other.
Figure 6. Exposure to Anti-Social Behaviour
0 10 20 30 40 50 60 7
Parents/Caregivers was drunk Father beat mother Mother beat father Parents/caregivers screames and shouted at each other Parents/caregivers calling each other nasty things Parents/caregivers threatened with a weapon People having sex People drank alcohol and got drunk People using drugs People behaving in a way that frightened you
Percentage Exposed 0
15-24 years 10-14 years
`
7.6 Sexual Abuse
Sexual abuse by parents and caregivers in the household was measured by three items: having been forced to have sex with a parent/caregiver, having been forced to touch him or her in a sexual way, and having been touched in a sexual way.
Overall, one in four respondents in the 10-14 year sample had experienced one or more forms of sexual abuse. Some 12% had been touched by a parent/caregiver once or more, 15% had to touch a parent or caregiver once or more, and 15% had been forced to have sex with a parent or caregiver once or more. Some 12% of the total experienced one form of sexual abuse, 8% experienced two forms and 5% experienced all three. In the sample, 23.5% of males and 26.3% of females experienced one or more forms of sexual abuse.
Reported levels of abuse among the15-24 age group were lower than among the 10-14 year olds. Some 15% of this age group had experienced one or more forms of sexual abuse. A parent or caregiver had touched almost 9% inappropriately, 7% were forced to sexually touch a parent or caregiver, and 8% were forced to have sex with a parent or caregiver.
Sexual abuse not only has emotional impacts on children and youth but may also perpetuate the spread of STIs and HIV/AIDS. It is noteworthy to mention the implications of forced sex at first sexual experience. Forced sex on the first sexual encounter was 42.3% among 10-14 year olds and 18.3% among 15-24 year olds. For female adolescents, nearly one in four had a forced sexual encounter (23.6%) and even the rate for males (14.6%) was very high. Of the 15-24 year olds who fell pregnant, 40% were forced into sex. This phenomenon reflects deep-rooted gender imbalances in Namibian society, and should be seen in the context of high domestic violence. While intergenerational sex does not necessarily constitute abuse, it is an issue that needs to be addressed. Approximately one third of both groups had sex with people older and much older than themselves and 8% of the 10-14 year olds and 6% of the 15-24 year olds had received gifts or were paid for sex.
8.0 ALCOHOL ABUSE
Alcohol abuse is commonly recognized as a wide-spread social problem in the country and linked to violence, abuse and various types of risk taking, including sexual risk taking. The impact of alcohol thus warrants an exclusive analysis.
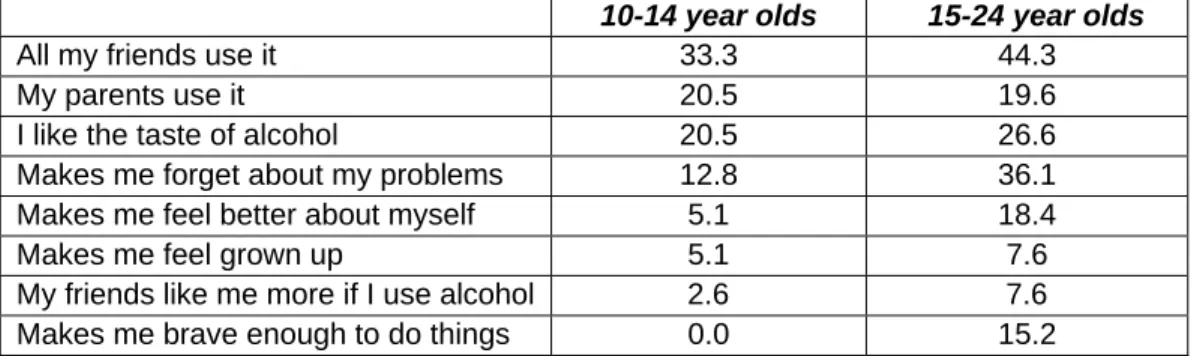
Approximately, one in ten, 10-14 year olds in the sample indicated that they have used alcohol at some point. The median age at which this group started using alcohol was 10.5 years. Alcohol usage increases with age. Among the 15-24 year olds, three in ten, had used alcohol before and the median age at which this group started drinking was 15 years. Table 5 lists the reasons for using alcohol comparing the 10-14 year olds and the 15-24 year olds among those who drink.
Table 5: Reasons for using alcohol (%)
10-14 year olds 15-24 year olds
All my friends use it 33.3 44.3
My parents use it 20.5 19.6
I like the taste of alcohol 20.5 26.6
Makes me forget about my problems 12.8 36.1
Makes me feel better about myself 5.1 18.4
Makes me feel grown up 5.1 7.6
My friends like me more if I use alcohol 2.6 7.6
Makes me brave enough to do things 0.0 15.2
Members of both the groups use alcohol primarily because of peer pressure. Among the 10-14 year olds parents use of alcohol and liking the taste of alcohol were the second most common reasons contributing to alcohol use. Among the 15-24 year olds, alcohol was also commonly used to help forget problems. The sources of alcohol in Table 6 could possibly reflect their reasons for drinking. For the 10-14 year group their main source of alcohol was their parents while the 15-24 year old group got most of their alcohol from parties, then friends and self purchase.
Table 6: Sources of Alcohol (%)
10-14 year olds 15-24 year olds
At parties 23.3 37.8
From friends 27.9 29.7
From my parents 32.6 5.6
I buy my own 14.0 26.5
I don't drink any more 2.3 0.4
Urban respondents started drinking a year earlier (14 years) than their rural counterparts (15 years). Not only is the alcohol consumption an issue but also the frequency of consumption is concerning. Six percent of the sample who use alcohol, were imbibing alcohol daily. Nearly half the sample drank (48%) at least once a week. Age is significantly correlated with the frequency of drinking. Those out of school also drink more frequently than those who are still in school.
Alcohol Consumption among different groups*
Ç
Female 10-14 years: This group drinks primarily because their parents do it, and because their friends do it. This suggests that of all the groups discussed here, this group is the most susceptible to the influence of those close to them when it comes to the use of alcohol. Their drinking habits are best explained by external influences.Male 10-14 years: They drink mostly because it makes them feel grown up, and because they like the taste of alcohol. Another reason more closely corresponding with this group than with any other group is that their friends like them more if they drink. Their drinking habits are best explained by a budding
Ç
macho culture, i.e. the need to appear older than they are, and to do so
Ç
Ç
n in this age group, because alcohol gives them confidence (or makes them brave to do
h correspondence analysis
among their friends.
Female 15-24 years: This group drinks primarily to forget their problems and to feel better about themselves. They also drink to feel more grown up and because their friends do it, but these are more distant reasons. This group’s drinking habits is best explained by emotional considerations. Alcohol makes young women feel better about themselves, thus boosting their self-image.
Males 15-24 years: Like their female counterparts, men of this age group drink to forget their problems. Although their drinking is also driven by emotional considerations, they are different for the wome
things). * throug
All groups are exposed to significant alcohol related antisocial behaviour. Over 60% in the 10-14 age group were exposed to abuse of alcohol and drunken behaviour around their homes and 45% were exposed to their parents/caregivers being drunk. Among the 15-24 years group, approximately 68% were exposed to abuse of alcohol and drunken behaviour around their homes and 48% were exposed to alcohol abuse by their parents. In both cases the children and youth received a double exposure to abuse of alcohol and drunken behaviour. Being exposed to an environment where alcohol is used by parents and others increases the probability of alcohol risk behaviour by a factor of 3.53. This possibly indicates that alcohol risk behaviour is learned behaviour and a result of the environment within which respondents live and grow up. In addition, connectedness to parents reduces the probability of alcohol risk behaviour by a small factor of 0.15.
The influences of alcohol on behaviour are substantial. Among the 15-24 year old group who used alcohol, 46.8% had forgotten things, 30.4% had been involved in a physical fight, 15.8% had gotten in trouble with the police, and 26.6% had participated in sexual activities while under the influence. Also 53.8% had so much to drink that they had gotten drunk. Alcohol increases the probability of having taken one or more HIV risks (through sexual risks) by a factor of 3.51. Therefore alcohol abuse is a significant contributor to the spread of HIV/AIDS and needs to be addressed.
9. ORPHANS
Orphans are defined as those under 18 years who have lost one or both parents which may not necessarily be attributed to HIV/AIDS. In total 226 orphans were represented in the sample. While it was purposive to include orphans in the sample, no major differences in terms of sexual behaviour and risks were observed between orphans and non-orphans. The supportive environment that surrounds orphans may explain this indifference. Most orphans’ material and emotional needs are met through a single parent or extended family support. Orphans are usually absorbed into existing family structures and not left to their own devices. It is generally the mother or grandparents who carry the financial burdens of school fees and other household expenses such as food for orphans which may also be the case for non-orphans. Among the 81, 10-14 year old orphans school absenteeism for a period exceeding a week was only among 22%. Two out of three orphans missed school because they were ill, one out of five because they had to go live with someone else, and none missed school because they had to work. As for risk behaviours only 42.1% of orphans had sex versus 54% of non-orphans among the 15-24 year age group. Also, among the 15-24 year old group, non-orphans had been sexually active for 4.1 years compared to orphans which was 2.8 years. A plausible explanation for these factors is that orphans are more aware of their personal risks. However, non-orphans had more self-efficacy for reducing HIV risks than orphans though the difference between these two groups was very small.
10. PROGRAM PARTICIPATION AND IMPACT
Impact is difficult to measure because of the attribution; how does one ensure that programme interventions actually enable behaviour change and whether or not other factors or a combination of factors contribute to behaviour change? The intention of this study was not to measure impact; nonetheless, programme participation can be assessed and some deductions can be made on the outcomes of programmes.
UNICEF supports many programmes for youth and children. The Window of Hope is a life skills programme for 10-14 year old children implemented by teachers as an extra-curricular activity in primary schools. My Future My Choice (MFMC) is a life skills programme for young adults (15-24 years) also implemented as an after school activity for both in and out of school youth implemented by youth. Open Talk is a monthly newspaper insert addressing youth issues around sexuality. UNICEF is one of the core members and key supporters of Take Control – the National Namibian HIV/AIDS and Media Campaign.
Almost half (48.4%) of the 10-14 year olds in the sample have taken part in the Window of Hope programme (at least at some stage) and 34.3% had read Open Talk. Among the 15-24 year olds, 69.2% had read Open Talk and 87.2% had heard of Take Control.
Overall, 44.2 % of all 15-24 year old respondents participated in MFMC. Similar proportions of those currently in school (44.1%) and those who have left school (44.4%) have participated in the MFMC programme. Some 45% of male respondents and slightly less female respondents (42.5%) participated in MFMC. Some interesting observations can be construed from participation in MFMC. MFCM participants on average have been sexually active for a shorter time (3.3 years), than non-participants (4.3 years). MFMC participants are generally less anxious about HIV. These differences were statistically significant. From the factor and correspondence analysis of condom use, the 15-24 year olds out-of-school males who have not participated in MFMC had more anti-condom attitudes and those males who had participated in MFMC had pro-condom attitudes. Condom use was also slightly higher among MFMC participants (78.8%) than among non-participants (74.8%). This difference was not statistically significant. MFMC participants also consumed alcohol less frequently than non-participants, and this difference, albeit weak, was statistically significant.
11. CONCLUSIONS AND RECOMMENDATIONS
Any programme targeting youth faces challenges from the social environment within which these young people grow up. The formative powers of this environment are significant and might either increase or decrease its effectiveness. Programme implementers not only have to acknowledge the opportunities and constraints stemming from this environment, but are often powerless to reduce or reverse these negative effects. Environmental factors that increase probability for sexual risk taking include exposure to alcohol abuse, sexual abuse and interpersonal abuse and violence. The recommendations based on this study are put forward for future HIV prevention programmes:
Knowledge about HIV/AIDS (both transmission and prevention) as an STI is near complete; however, knowledge of other STI’s is much lower. Therefore knowledge levels of STIs’s other than HIV/AIDS should be incorporated into future programmes.
The 10-14 age group displayed the most stigma and hence it is important to promote more pro HIV+ messages and information aimed at curbing stigma with this age group.
Sexual patterns among 10-14 year olds and 15-24 year old females are of concern (forced sex, and sexual debut with much older partner); more emphasis should be placed on educating these groups and creating an enabling environment that reduces vulnerability.
Building on the relationships and increasing communication between parents and young children is an area that needs to be strengthened as this is a good entry point for programming and ensuring young people have the adequate information and skills. The communication skills of parents to discuss sexual issues with their children should be highlighted.
The median age for sexual debut for 15-24 year olds is 15, and within this age group males are more likely to be sexually active than females. Special attention should be paid to males because for the majority of males, the first sexual encounter is voluntary.
Ninety percent of the sexually active 15-24 year olds engages in sexual risk behaviour. Programmes should emphasize reduction of all types of risk behaviour particularly: sex with unfaithful partners, sex with multiple partners and unprotected sex. The last two are more commonly associated with males than with females. Females are more likely to have had sex with an unfaithful partner. Programmes should therefore acknowledge the fact that males are more likely to be put at risk by their own actions, versus females who are put at risk by their partners’ actions.
Among 15-24, the median number of sexual patterns was two. This calls for program interventions to reduce multiple sexual partners to ideally one faithful partner.
Testing for HIV amongst 15-24 year olds is low, despite the fact that around half of them are sexually active. More attention should be paid to the need for testing within this age group who start their sexual activity at a young age, engage in sexual risk taking and are sexually active.
Females between 15-24 have the lowest condom efficacy. Together with the fact that they are more likely to have sex with unfaithful partners, this makes them particularly vulnerable to HIV/AIDS risks. Condom efficacy in this group should be addressed.
Males are less likely to use condoms than females. Condom usage is also lower amongst younger members of the 15-24 year old group who are still in school. This calls for a specific age and gender focus.
Young Namibians grow up in a social environment that contains a substantive amount of antisocial behaviour, which could heavily influence their sexual risk behaviour. The exposure to antisocial behaviour is disturbingly high and necessitates some interventions.
15-24 year olds consume alcohol on a regular basis, and they start drinking fairly early (at the age of 15). Those who drink often expose themselves to risks when under the influence of alcohol. In turn, these risks lead to sexual risk taking. This necessitates the inclusion of the dangers of alcohol into programmes about HIV AIDS.
Photographs
UNICEF library, Silke Felton, Tariq Bhanjee
© UNICEF Namibia November, 2006 ISBN: 99916-835-1-8
“Alcohol is a social lubricant that some people feel they can relate
more easily to each other after drinking. They are also more likely
to initiate sexual relationships and put themselves at risk. Alcohol
reduces inhibitions and can therefore increase the risk of violent
behaviour such as rape.”
L.H. Mandema – Student at Polytechnic of Namibia
ISBN: 99916-835-1-8 November 2006
United Nations Children’s Fund Namibia Country Office
1st Floor, Sanlam Building
P.O. Box 1706 Windhoek, Namibia Tel: 264 61 204 6111 Fax: 264 61 204 6206 www.unicef.org