Allergen
Focus
A
llergic Con-tact Dermati-tis (ACD) is an important disease that notably affects 14.5 million Americans each year.1 The economic impact of this disease is high in terms of both patient morbid-ity and loss of income, school and work, not to mention significant expenditures for visits to health care provid-ers and for medicaments.1 Once patch testing is performed and a culprit has been identified, education becomes the critical intervention to ensure adher-ence to an avoidance regimen. With al-lergen avoidance, remission of the der-matitis ensues. If the patient is unable to comply with the avoidance regimen, he or she becomes at risk for recurrent or sustained dermatitis or progression to a systematized presentation.2,3 In fact, education of the patient often begins before the diagnostic patch test is ever placed. This ensures that the patient has an appropriate understanding of poten-tial outcomes and his or her central role in both disease and treatment.During the initial consultation, pa-tients are often taught about the patho-physiology of ACD: its delayed presen-tation, its relationship with the immune system (sensitization to a chemical and then elicitation of a dermatitis with re-exposure) and its occurrence at any point in time, even to something that the patient has been using regularly for a short period of time or intermittently for years. In certain cases, the other key players, such as irritant contact dermati-tis (ICD) and contact urticaria, may be
explained via patient history, rather than patch testing, as the correct diagnosis for the patient. It is important to note that ICD, the most prevalent form of contact dermatitis, can, at times, precede, or be a concomitant diagnosis with, ACD.4,5 Unlike ACD, ICD is not immune-me-diated, but occurs secondary to contact with an irritating or abrasive substance. Contact urticaria (wheal and flare reac-tion), on the other hand, represents the least prevalent form of contact derma-titis. It is important to note that it is an immune-mediated phenomenon whose hallmark is an IgE and mast cell-medi-ated, immediate-type hypersensitivity reaction. We acknowledge this form of hypersensitivity due to the severity of the potential deleterious anaphylactic type reactions and direct the reader to key sources.6-8
In this section, we highlight ACD and explore top relevant allergens, re-gional-based dermatitis presentations, topic-based dermatitis presentations and clinical tips and pearls for diagnosis and treatment.
Allergic contAct DermAtitis of the eyeliD
The eyelid is one of the most sensi-tive areas of the body.9 The skin of the eyelid is extremely thin compared to facial skin, rendering it vulnerable to penetration by contact allergens. It is exposed to an extraordinary number of substances, in part due to the fre-quent rubbing of the eye area by our fingers and hands.9 In fact, ACD of the eyelids is more often an ectopic mani-festation caused by cosmetics applied to the hair, face, scalp or fingernails than materials applied directly to the
Allergic contAct DermAtitis
of the eyeliD
VeronicA A. russo, mPh, AnD lisA e. mAier, mD
Veronica A. Russo, MPH
20 April 2012 | The DermaTologisT®
| www.the-dermatologist.com
Allergen Focus
eyelid or periorbital area.9 The eyelid is also particularly susceptible to ACD from airborne substances.9
ACD is deemed one of the most common causes of eyelid dermatitis. In some published reports, ACD is es-timated to be responsible for at least half of all cases.9-13 The manifestations of ACD of the eyelid depend on the chronicity of exposure.14 Acute ACD may present with intense pruritus and erythema with macules, papules or vesicles;11,14 whereas subacute and chronic forms of contact dermatitis are markedly less pruritic and character-ized by dry, lichenified, scaly eyelids.14 The subjective symptoms and physical manifestations are usually limited to the area of the eyelid that came into
direct contact with the allergen, and it is not uncommon for a primary site of substance application, remote from the eyelid area, to remain unaffected.9,14,15 Scratching or picking as a result of the dermatitis may have several adverse consequences, including an increased risk of infection, loss of eyelashes, dis-ruption of tearing and visual obstruc-tion secondary to eyelid and periorbital edema.13 Moreover, the eyes are often viewed as important cosmetic struc-tures of the face; therefore, disfiguring visible changes to the aesthetic appear-ance of the eyes may have significant effects on the self-confidence and well-being of the individual.
Studies have consistently demon-strated a predominance of females
(>80%) suffering from eyelid der-matitis,13,16-22 most likely due to the use of cosmetic substances.23 ACD affecting the eyelids has been previ-ously reported secondary to allergens contained in makeups, eye shadows, lotions, fragrances, preservatives and applicators such as brushes.10 For ex-ample, shellac, a resin derived from the insect Coccus lacca that is present in popular brand mascaras, has been identified as a cause of ACD of the eyelid.24 Nail polishes containing the resins toluene-sulfonamide formal-dehyde or tosylamide formalformal-dehyde and nail acrylates containing benzo-phenone are well known sources of eyelid ACD due to frequent finger-to-eyelid contact.9 Hair products, such as
Table 1. DIFFERENTIAL DIAGNOSIS OF EYELID ALLERGIC CONTACT DERMATITIS9,14,15,27-32
Diagnosis clinical Presentation comments
Allergic contact dermatitis Pruritic, erythematous, vesicular or papular inflammation. subacute and chronic forms
are less pruritic and erythematous and appear more scaly and lichenified. myriad of allergens possible. irritant contact dermatitis Dryness, fissuring, lichenification of eyelid skin; often experience stinging and burning of
eyes and lids upon application of irritant; may manifest with vesiculation and oozing. common agents implicated include detergents, solvents, sunscreens, propylene glycol and volatile compounds. Atopic dermatitis symmetric, pruritic, scaly, erythematous plaques on upper eyelids (inner canthus)
+/- lower eyelids. chronic lesions are darker and more lichenified. conjunctivitis and keratoconjunctivitis;“allergic shiners;” Dennie-morgan folds; allergic rhinitis; and asthma commonly associated.
Personal and family history of atopy. Various triggers and allergens induce flares. commonly affected by AcD and staphylococcal colonization.
contact urticaria eruption appears within 1 hour of exposure to contactant. results in erythema, pruritus, burning and urticaria.
Protein contact dermatitis eczematous lesions, usually clinically indistinguishable from AcD; manifests as an
immediate type i sensitization. induced by substances containing animal proteins, vegetable proteins, cereal grains or enzymes. Angioedema edema of skin involving deeper subcutaneous layer. overlying epidermis is intact,
nonpruritic, nonpitting. eyelids, lips, genitalia most commonly involved areas. trig-gers include foods, medications and insect stings. seborrheic dermatitis
(blepharitis) symmetric erythematous inflammation with scaling yellow plaques, often greasy and crusting, involving the periocular tissues. history and physical typically make the diagnosis. other typical areas of involvement include scalp, ears, nasolabial folds, chest, axilla and inguinal region.
rosacea blepharitis lid: blepharitis, chalazion. conjunctiva: conjunctivitis, keratoconjunctivitis, sicca. sclera: scleritis, episcleritis, perforation. iris: iritis. cornea: scarring, perforation, neovascularization, ulceration, blindness.
other stigmata of rosacea may be present, including erythe-ma, edeerythe-ma, papules or telangiectasias on cheeks, forehead and nose. should be evaluated by ophthalmologist. Viral infections (herpes
simplex, herpes zoster) Usually uni-ocular with a pruritic, painful aura. lesions on eyelid are grouped vesicles on erythematous base (hsV) or vesicles/papules/pustules on erythematous patch that follow dermatomal distribution (hZV). Associated with itching and burning. may involve cornea and conjunctiva.
serum antibody tests or viral cultures help distinguish hsV from hZV.
Bacterial infections
involving periorbital tissues Acute eyelid edema and swelling, +/- purulent discharge. Usually secondary to trauma or skin infection with Staphylococcus aureus, Haemophilus influenza type B or Streptococcus.
Dermatophyte infections Key features include presence of scaling, exacerbation with use of topical
corticoste-roids, loss of eyelashes/eyebrows. confirm diagnosis with Koh preparation.
Dermatomyositis symmetrical, violaceous discoloration of eyelids. Proximal muscle weakness, gottron’s papules, shawl sign
and nailfold capillary loops may be present.
lichen planus flat topped, polygonal, purple, pruritic papules. Very rarely presents solely on eyelids.
Psoriasis Burning and itching, erythematous swollen eyelid(s). Uncommon to have periocular
and eyelid psoriatic plaques. Pustules may be present. eyelid psoriasis may be an indicator of severe psoriasis.
22 April 2012 | The DermaTologisT®
| www.the-dermatologist.com
Allergen Focus
shampoos, contain various fragrances, preservatives (formaldehyde releas-ers) and surfactants (cocamidopropyl betaine) that can induce eyelid ACD, sometimes even in the absence of concomitant scalp and facial derma-titis.9,25 The North American Contact Dermatitis Group (NACDG) recently identified the contact allergens most frequently causing eyelid dermati-tis.25 Their results, collected between 2003 and 2004, demonstrated that, of 5,145 patch-tested patients, 268 pa-tients (5.2%) had ACD dermatitis of the eyelids as the sole site of involve-ment. Moreover, 65% of these cases were the result of 1 of 26 clinically relevant contact allergens identified in the study, with fragrances and various ingredients in cosmetic and personal care products, including preservatives, comprising the majority of allergens. Of note, 33 cases yielded a positive patch test (PPT) to an allergen not included among 65 standard NACDG screening allergens and were primarily derived from personal care and beauty products. Likewise, Guin26 reported that 25% of 215 patients with eyelid dermatitis patch tested between 2001 and 2003 had a PPT to a cosmetic or personal care product, and 7% of those with ACD produced a reaction to cos-metic applicators. Similarly, Amin and Belsito18 determined that ACD was the cause of nearly 44% of 105 cases of eyelid dermatitis, of which 28.3% of patients had a relevant patch test reac-tion to fragrances and fragrance mix. Nethercott et al21 investigated 79 cases of eyelid dermatitis between 1980 and 1987, of which 46% of patients had ACD. Several relevant sources of re-actions were identified, with fragrance ingredients and cosmetic preservatives occurring as contact allergens more frequently compared to patients with-out eyelid dermatitis.
Additional relevant sources of ACD affecting the eyelids include metals and rubber (jewelry, makeup tools), medicaments (topical corticosteroids, antibacterial and ophthalmic prepa-rations), fingernail products, hair care product ingredients (surfactants, pre-servatives), cosmetics, plants (Rhus ge-nus) and airborne allergens (volatile chemicals and sprays).9,10,13,17-21,23,26
DifferentiAl DiAgnosis
Determination of the diagnosis and treatment plan for a patient presenting with eyelid dermatitis can be difficult. The differential diagnosis for eyelid der-matitis is broad and most commonly in-cludes the conditions listed in Table 1. Notably, a single cause for eyelid derma-titis may be challenging to define and, in fact, may be the result of a multitude of factors. For example, ACD of the eyelid may be superimposed on or associated with another pre-existing condition such as atopic eczema10,21,26 or seborrhe-ic dermatitis.18,26 In a large case series of 215 patients presenting for the first time with eyelid dermatitis, 89% of patients with atopic eczema of the eyelids had PPTs to contact allergens.26 Similarly, a retrospective analysis of 1,215 patients patch tested over a 10-year period dem-onstrated that several patients present-ing with seborrheic dermatitis of the eyelids had an associated ACD.18 Given these findings, the authors suggested that patch testing is a valuable diagnostic modality for patients with recalcitrant seborrheic dermatitis.
Distinguishing the etiology of a con-tact dermatitis as either allergic- or irritant-induced may prove especially challenging. In general, the inflam-mation associated with ICD tends to manifest earlier and more diffusely than ACD and is dependent on the dose of the agent, its duration of contact with the skin and the condition of the skin’s surface.9,14 Additionally, a vesicu-lar eruption is rare in ICD compared to ACD.9 However, although ICD has consistently been shown to be less prevalent, ranging from less than 1% to 21% of all cases of eyelid dermati-tis,10,12,17,18,21 the defining features of both are not always readily discernable. Both may present with equivalent de-grees of inflammation and similar time intervals between exposure and the on-set of symptoms.9
Therefore, when the cause of contact dermatitis involving the eyelid is elu-sive, a detailed exposure history is para-mount, including inquiries about the time between substance exposure and development of symptoms; cosmetics and other agents applied to the eyelids in addition to the face, hair, scalp, hands and fingers; introduction of new
prod-ucts and the renewal of previously ap-plied ones; cleansers and methods used for cosmetic removal; make up applica-tion techniques (eg, use of nickel- or rubber-containing eyelash curlers and foam rubber make up applicators); and occupational and hobby histories.9,11,15 Moreover, a thorough examination of the eyelids, face and hands is warrant-ed, as previous studies have shown that the likelihood of ACD as the primary diagnosis for eyelid dermatitis may in-crease with all quadrants of the eyelid involved12 or concurrent dermatitis in-volving the face or other body areas.16,18
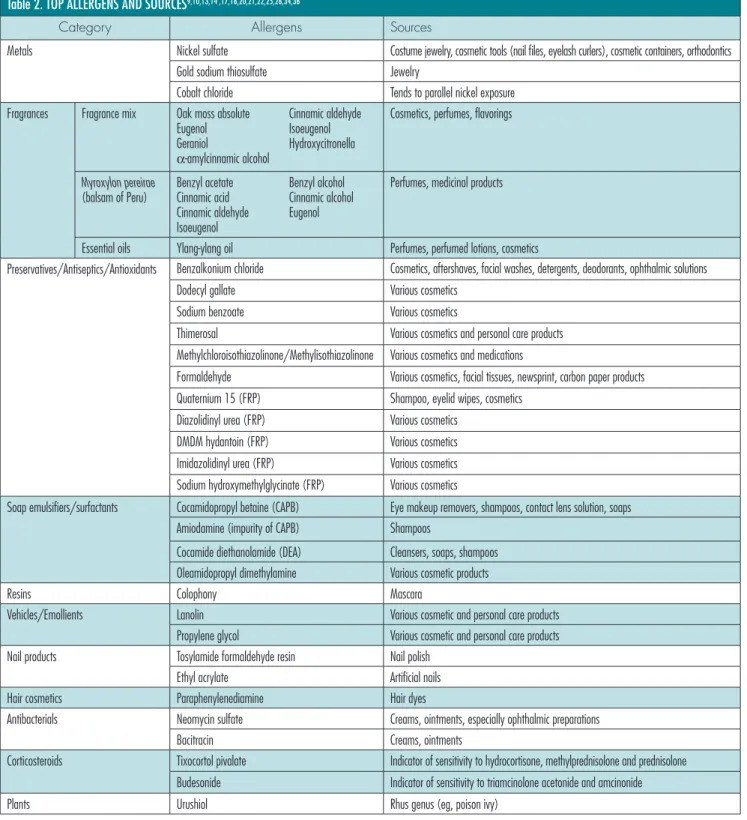
toP Allergens
Results from patch testing patients with eyelid dermatitis have been ex-tensively published, listing several al-lergens as common causes of ACD of the eyelid (see Table 2). As previously mentioned, chemicals contained in cosmetic and personal care products are the most frequently encountered agents responsible for eyelid ACD. For example, Herro et al22 cited formalde-hyde, a preservative in various cosmetic and topical products, as the most com-mon allergen inducing eyelid ACD. Likewise, the NACDG25 reported that fragrance mix 1, Myroxylon pereirae (balsam of Peru), methyldibromo gluta-ronitrile (preservative), quaternium-15 (formaldehyde releasing preservative) and methylchloroisothiazolinone/me-thylisothiazolinone (preservative), were among the main cosmetic allergens. Fragrance mix 1 was also listed as one of the most common relevant allergens in studies from the United States,13,18 United Kingdom19 and Italy.17
Additionally, in the NACDG analy-sis, gold was determined to be the most common contact allergen inducing eyelid-only ACD (8.2% of patients).25 It has been proposed that various cosmetic powders that contain abrasive agents such as titanium dioxide may chafe gold-containing jewelry, resulting in lib-eration of fine gold particulate that may subsequently travel and come in direct contact with the hands, face and eyelids, resulting in sensitization of the patient.33 Nickel was the fourth most common allergen in the NACDG study to in-duce ACD affecting only the eyelid;25 the prevalence of this allergy has been
corroborated by several other stud-ies.10,12,13,16-17,19-20,22,26 Likely sources of nickel include eyelash curlers and twee-zers, which are commonly plated with nickel,23 mascara tubes,17 glasses,20 jewel-ry and other accessories,14 and handling of objects such as coins and keys.20
Pharmaceutical products are a fre-quent cause of ACD of the eyelids. The NACDG listed the antibiotic neomycin,
an active principle ingredient in many topical ophthalmic preparations, as the fifth most common allergen.25 The find-ing of neomycin as a frequent contact al-lergen involved in eyelid ACD is similarly reported elsewhere.17,20,21 Moreover, tixo-cortol pivalate, a corticosteroid used as a marker for sensitivity to corticosteroids such as hydrocortisone, methylpredniso-lone and prednisomethylpredniso-lone,34 and budesonide,
a marker for sensitivity to corticosteroids such as triamcinolone acetonide and am-cinonide,34 were both included among the top 26 relevant allergens for eyelid ACD, according to the NACDG.25
PAtch testing
As mentioned above, in addition to a thorough history and physical examina-tion, patch testing is often necessary to Table 2. TOP ALLERGENS AND SOURCES9,10,13,14 ,17,18,20,21,22,25,26,34,36
category Allergens sources
metals nickel sulfate costume jewelry, cosmetic tools (nail files, eyelash curlers), cosmetic containers, orthodontics
gold sodium thiosulfate Jewelry
cobalt chloride tends to parallel nickel exposure
fragrances fragrance mix oak moss absolute cinnamic aldehyde
eugenol isoeugenol
geraniol hydroxycitronella
α-amylcinnamic alcohol
cosmetics, perfumes, flavorings
Myroxylon pereirae
(balsam of Peru) Benzyl acetatecinnamic acid Benzyl alcoholcinnamic alcohol
cinnamic aldehyde eugenol
isoeugenol
Perfumes, medicinal products
essential oils ylang-ylang oil Perfumes, perfumed lotions, cosmetics
Preservatives/Antiseptics/Antioxidants Benzalkonium chloride cosmetics, aftershaves, facial washes, detergents, deodorants, ophthalmic solutions
Dodecyl gallate Various cosmetics
sodium benzoate Various cosmetics
thimerosal Various cosmetics and personal care products
methylchloroisothiazolinone/methylisothiazolinone Various cosmetics and medications
formaldehyde Various cosmetics, facial tissues, newsprint, carbon paper products
Quaternium 15 (frP) shampoo, eyelid wipes, cosmetics
Diazolidinyl urea (frP) Various cosmetics
DmDm hydantoin (frP) Various cosmetics
imidazolidinyl urea (frP) Various cosmetics
sodium hydroxymethylglycinate (frP) Various cosmetics
soap emulsifiers/surfactants cocamidopropyl betaine (cAPB) eye makeup removers, shampoos, contact lens solution, soaps
Amiodamine (impurity of cAPB) shampoos
cocamide diethanolamide (DeA) cleansers, soaps, shampoos
oleamidopropyl dimethylamine Various cosmetic products
resins colophony mascara
Vehicles/emollients lanolin Various cosmetic and personal care products
Propylene glycol Various cosmetic and personal care products
nail products tosylamide formaldehyde resin nail polish
ethyl acrylate Artificial nails
hair cosmetics Paraphenylenediamine hair dyes
Antibacterials neomycin sulfate creams, ointments, especially ophthalmic preparations
Bacitracin creams, ointments
corticosteroids tixocortol pivalate indicator of sensitivity to hydrocortisone, methylprednisolone and prednisolone
Budesonide indicator of sensitivity to triamcinolone acetonide and amcinonide
Plants Urushiol rhus genus (eg, poison ivy)
24 April 2012 | The DermaTologisT®
| www.the-dermatologist.com
Allergen Focus
distinguish ACD from other causes of eyelid dermatitis, and to identify the rel-evant allergen(s) responsible. The Thin-Layer Rapid Use Epicutaneous (TRUE) patch test is an FDA-approved, com-mercially available patch test panel that is widely used. The TRUE Test can help identify some of the common causes of eyelid ACD, such as nickel, thimero-sal, cobalt, fragrance mix and balsam of Peru.35 However, several possible con-tactants inducing ACD of the eyelid are not represented on the TRUE Test, and, in comparison with the NACDG data, clinically relevant allergens may be overlooked.25,35 Since determination of the etiology of eyelid dermatitis may be challenging with routine patch test-ing, the top 38 most commonly relevant allergens based on recent publications that would constitute a reasonable initial screening series for the evaluation of pa-tients with dermatitis exclusively involv-ing the eyelids is defined in Table 3.
Patients may be tested with their own products alongside the standard trays to increase the yield of finding the culprit. It is important to note that many products containing putative allergens may require preparation prior to testing. For example, it is imperative that mascaras and liquid eyeliners be allowed to dry before occlu-sion.36 If topical medicaments, cosmetics or other personal care products are sus-pected to be the culprit, one may consid-er using a “repeat open application test” (ROAT) or “use test.” This is occasion-ally employed before formal closed patch testing when an allergen in a cosmetic or personal care product is unknown or if there is no known safe and standard con-centration of that allergen chemical for formal patch testing.9 More commonly, the open use test is an additional measure to confirm that an allergen present in its typical-use concentration in a product is indeed capable of triggering ACD.9 In the open use test, the implicated cosmetic or personal care product is applied to intact skin of the antecubital fossa over a 3-cm diameter area twice daily for one week and the skin is subsequently assessed for evidence of dermatitis in the area.
treAtment
Avoidance of specific allergens, es-pecially in cosmetic and personal care products, is the foremost way to treat
ACD of the eyelids. Although this can prove to be a tedious task, especially for women, there are programs available to aid in this endeavor. Both the Con-tact Allergen Management Program (CAMP), a service offered through the American Contact Dermatitis Society (ACDS),37 and the Contact Allergen Replacement Database (CARD), de-veloped by Mayo Clinic,38 enable a pro-vider to enter a patient’s known con-tact allergens and produce a “shopping list” of products void of those particular chemicals. The programs also have the ability to exclude cross-reactors.
Detailed education about allergen avoidance is also crucial. For example, patients must understand the difference between “unscented” and “fragrance-free” products in order to ensure avoid-ance of a sensitizing contactant. “Un-scented” products are devoid of odor but not necessarily fragrance, as many “unscented” products contain mask-ing fragrances designed to disguise un-derlying scents that may be present in the product.39 Conversely, “fragrance-free” products generally do not con-tain fragrance chemicals, including odor-masking agents,39 and thus may be more appropriate for individuals with known fragrance allergies. Individuals with a gold allergy may be counseled to wear gold jewelry for short periods of time on special occasions only,9 and individuals allergic to nickel may look for tweezers and eyelash curlers plated with stainless steel.23 Patients with an allergy to cocamidopropyl betaine, a surfactant contained in many makeup removers and also listed among the top 26 relevant eyelid allergens by the NACDG,25 should avoid wearing wa-terproof makeups that necessitate use of special makeup removal products.36 Instead, sensitive individuals should opt for wearing exclusively water-soluble eye makeups requiring only a gentle cleanser for removal. In general, patients should be encouraged by their health-care providers to health-carefully read the la-bels of their personal care and cosmetic products and inspect the packaging or the insert for the ingredient list. The first item listed is present in the great-est concentration and subsequent items are listed in the order of decreasing con-centrations present in the product.9 By
Table 3. RECOMMENDED SCREENING SERIES FOR EVALUATION OF PATIENTS WITH DERMATITIS EXCLUSIVELY INVOLVING THE EYELIDS18,22,25
Allergen 1. Amidoamine 0.1% aq 2. Bacitracin 20% pet
3. Benzalkonium chloride 0.1% aq 4. Benzyl alcohol 1% pet‡ 5. Black rubber mix 0.6 pet 6. Bronopol 0.5 pet 7. Budesonide 0.1% pet 8. cinnamic alcohol 2% pet‡ 9. cinnamic aldehyde 1% pet 10. cobalt chloride 1% pet 11. cocamide DeA 0.5% pet‡
12. cocamidopropyl betaine (cAPB) 1% aq 13. colophony 20% pet
14. d-α-tocopherol acetate 100% 15. DmDm hydantoin 1% aq 16. Dodecyl gallate‡ 0.25/pet 17. ethyl acrylate 0.1% pet 18. formaldehyde 1% aq 19. fragrance mix i 8% pet 20. gold sodium thiosulfate 0.5% pet 21. hydroxylcitronellal 2% pet‡ 22. imidazolidinyl urea 2.0 aq/pet 23. lanolin 30% pet
24. methylchloroisothiazolinone/ methylisothiazolinone 100 ppm aq 25. methyldibromo glutaronitrile 2% pet 26. methyl methacrylate 2% pet
27. myroxylon pereirae (balsam of Peru) 25% pet 28. neomycin 20% pet
29. nickel sulfate 2.5% pet 30. Paraphenylenediamine 1.0 pet 31. Propylene glycol 30% aq 32. Quaternium-15 2% pet 33. sodium benzoate 5% pet 34. thimerosal 0.1% pet 35. thiuram mix 1% pet 36. tixocortol pivalate 1% pet
37. tosylamide formaldehyde resin (tsfr) 10% pet 38. ylang ylang oil 2% pet
Abbreviations: aq, aqueous; pet, petrolatum; ppm, parts per million. ‡ recently reported relevant allergens22
developing the habit of reading product labels, patients will be more successful at avoiding the allergens to which they are most sensitive.
If relief from symptoms is not achieved following avoidance of the putative al-lergen, the application of low potency topical corticosteroids, preferably with a vinyl glove to ensure isolation of the eyelids from contactants present on the hands, may be necessary for resolution of acute flares.10,15,26,34 However, an ex-tended duration of topical corticoste-roids use in the periorbital region is not without potential side effects and has been associated with the development of cataracts, elevated intraocular pres-sure, increased risk of ocular infections, poor wound healing and eyelid skin pigmentation changes, atrophy and tel-angiectasias.40 Topical immune modula-tors such as calcineurin inhibimodula-tors (eg, tacrolimus) are steroid-sparing agents that may serve as viable alternatives to topical steroids. These agents have been shown to reduce erythema, edema and lichenification associated with eyelid ACD.41 Common side effects include burning and itching41 and, currently in the United States, these agents carry a controversial black box warning due to concerns for promoting malignancy and lack of long term safety data.41,42 For severe flares of eyelid ACD, systemic steroids may be used to decrease inflam-mation; however, due to significant side effects, they should not be used as a long-term treatment strategy.
sUmmAry
In conclusion, the delicate eyelid skin is particularly susceptible to der-matitis, and ACD is considered among the most common causes. Although the etiologies of eyelid ACD are vast and often elusive, chemicals contained in fragrances, cosmetics and personal care products are some of the most impli-cated agents in eyelid ACD. Moreover, patients suffering from eyelid dermatitis are mostly women, given the frequen-cy of cosmetic and fragrance use. It is important to have a high suspicion for ACD in patients presenting with recal-citrant dermatitis involving the eyelids, especially when the manifestation is bi-lateral or involves additional, including non-facial, areas of the body. Moreover,
the practitioner must keep in mind that eyelid ACD is most often caused by ma-terials applied to the hair, face, scalp or fingernails. Therefore, a comprehensive exposure history is essential for an ac-curate diagnosis and to inform manage-ment, which always begins with strict avoidance of the offending allergen. n
Dr. Maier is an Assistant Professor in the University of Michigan Department of Dermatology.
Ms. Russo is a fourth-year medical stu-dent at Michigan State University and will begin her dermatology residency at the Uni-versity of Cincinnati in 2013.
References
1. Bickers DR, Lim HW, Margolis D, et al. The burden of skin diseases: 2004 a joint project of the American Acad-emy of Dermatology and the Society for Investigative Dermatology. J Am Acad Dermatol 2006;55(3):490-500. 2. Hsu JW, Matiz C, Jacob SE. Nickel Allergy: localized, id, and systemic manifestations in children. Pediatr Dermatol. 2011;28(3): 276-280.
3. Salam TN, Fowler JF Jr. Balsam-related systemic con-tact dermatitis. J Am Acad Dermatol. 2001;45(3):377-381. 4. Nijhawen RI, Matiz C, Jacob SE. Contact derma-titis: from basics to allergodromes. Pediatric Annals. 2009;38(2):99-108.
5. Militello G, Jacob SE, Crawford GH. Allergic contact dermatitis in children. CurrOpin Pediatr. 2006;18(4):385–390.
6. Valks R, Conde-Salazar L, Cuevas M. Allergic contact urticaria from natural rubber latex in healthcare and non-healthcare workers. Contact Dermatitis. 2004; 50(4): 222-4. 7. Walsh ML, Smith VH, King CM. Type 1 and type IV hypersensitivity to nickel. Australas J Dermatol. 2010;51(4):285-6.
8. Gimenez-Arnau A, Maurer M, De La Cuadra J, Mai-bach H. Immediate contact skin reactions, an update of Contact Urticaria, Contact Urticaria Syndrome and Pro-tein Contact Dermatitis -- “A Never Ending Story.” Eur J
Dermatol. 2010;20(5):552-62.
9. Rietschel R, Fowler JF. Fisher’s Contact Dermatitis. 6th ed. Hamilton, ON: BC Decker Inc; 2008: 1-7; 12; 66-70; 266-308; 319-320; 731-741.
10. Guin JD. Eyelid dermatitis: experience in 203 cases. J
Am Acad Dermatol. 2002;47(5):755–765
11. Morris S, Barlow R, Selva D, Malhotra R. Allergic contact dermatitis: a case series and review for the oph-thalmologist. Br J Ophthalmol. 2011;95(7): 903-908. 12. Ayala F, Fabbrocini G, Bacchilega R, et al. Eyelid der-matitis: an evaluation of 447 patients. Am J Contact
Der-mat. 2003;14(2): 69-74.
13. Landeck L, Schalock PC, Baden LA, Gonzalez E. Periorbital contact sensitization. Am J Ophthalmol. 2010;150(3):366-370.
14. Parelejo B, Beltrani V, Bielory L. Dermatologic and allergic conditions of the eyelid. Immunol Allergy Clin N
Am. 2008; 28(1): 137-168.
15. Beltrani VS. Eyelid dermatitis. Curr Allergy Asthma Rep. 2001; 1(4):380-388.
16. Cooper SM, Shaw S. Eyelid dermatitis: an evaluation of 232 patch test patients over 5 years. Contact Dermatitis. 2000; 42(5): 291-293.
17. Valsecchi R, Imberti G, Martino D, Cainelli T. Eyelid dermatitis: an evaluation of 150 patients. Contact
Dermati-tis. 1992;27(3):143–147.
18. Amin KA, Belsito DV. The aetiology of eyelid der-matitis: a 10-year retrospective analysis. Contact Dermatitis. 2006;55(5): 280–285.
19. Shah M, Lewis F, Gawkrodger D. Facial dermatitis and eyelid dermatitis: a comparison of patch test results and final diagnoses. Contact Dermatitis. 1996; 34(2): 140–141. 20. Goossens A. Contact allergic reactions on the eyes and eyelids. Bull Soc belge Opthalmol. 2004; 292: 11–17.
21. Nethercott JR, Nield G, Holness DL. A review of 79 cases of eyelid dermatitis. J Am Acad Dermatol. 1989; 21(2 Pt 1): 223-230.
22. Herro EM, Elsaie ML, Nijhawan RI, Jacob SE. Rec-ommendations for a Screening Series for Allergic Con-tact Eyelid Dermatitis. Dermatitis. 2012;23(1):17-21. 23. Bielory L. Contact dermatitis of the eye. Immunol
Al-lergy Clin North Am. 1997;17(1):131–8.
24. Shaw T, Oostman H, Rainey D, Storrs F. A rare eyelid dermatitis allergen: shellac in a popular mascara.
Dermati-tis. 2009; 20(6):341-5
25. Rietschel RL, Warshaw EM, Sasseville D, et al. Com-mon contact allergens associated with eyelid dermatitis: data from the North American Contact Dermatitis Group 2003-2004 study period. Dermatitis. 2007; 18(2): 78-81. 26. Guin JD. Eyelid dermatitis: a report of 215 patients.
Contact Dermatitis. 2004;50(2):87-90.
27. Hernandez-Bel P, de la Caudra J, Garcia R, Alegre V. Protein contact dermatitis: a review of 27 cases. Actas
Dermosifiliogr. 2011;102(5): 336-343.
28. Tovilla-Canales JL, Nava A, Tovilla y Pomar JL. Or-bital and periorOr-bital infections. Curr Opin Ophthalmol. 2001;12(5): 335-341.
29. Basak SAF, Berk DR, Lueder GT, Bayliss SJ. Com-mon features of periocular tinea. Arch Ophthalmol. 2011;129(3):306-309.
30. Munoz ER, Martinez-Escala ME, Juanpere N, Ar-mentia J, Pujol RM, Herrero-Gonzalez JE. Isolated con-junctival lichen planus: a diagnostic challenge. Arch
Der-matol. 2011;147(4): 465-467.
31. Rehal B, Modjtahedi BS, Morse LS, Schwab IR, Maibach HI. Ocular psoriasis. [published online ahead of print May 5 2011]. J Am Acad Dermatol. 2011. http://www.sciencedirect.com/science/article/pii/ S0190962210020190. Accessed September 20, 2011. 32. Gul U, Soylu S, Aslan E, Yazar Z, Demiriz M. Uncom-mon presentation of mycosis fungoides: eyelid margin involvement. J Dermatol. 2008;35(9): 581-584.
33. Nedorost S, Wagman A. Positive patch test reactions to gold: patients’ perception of relevance and the role of tita-nium dioxide in cosmetics. Dermatitis. 2005;16(2):67–70. 34. Baeck M, De Potter P, Goossens A. Allergic contact dermatitis following ocular use of corticosteroids. J Ocul
Pharmacol Ther. 2011;27(1): 83-92.
35. Krob HA, Fleisher AB, D’Agostino R, Haverstock CL, Feldman S. Prevalence and relevance of contact dermatitis allergens: a meta-analysis of 15 years of published T.R.U.E. Test data. J Am Acad Dermatol. 2004;51(3): 349-353. 36. Draelos ZD. Special considerations in eye cosmetics.
Clin Dermatol. 2001;19(4): 424-430.
37. ACDS CAMP. American Contact Dermatitis Soci-ety. 2011. Available at: http://www.contactderm.org/ i4a/pages/index.cfm?pageid=3489. Accessed Septem-ber 21, 2011.
38. CARD: Contact Allergen Replacement Database. 2011. Available at: http://www.preventice.com/card/. Accessed September 21, 2011.
39. Jacob SE, Castanedo-Tardan MP. Alternatives for fra-grance-allergic children. Pediatr Ann. 2008;37(2): 102-103. 40. Carnahan MC, Goldstein DA. Ocular complications of topical, peri-ocular, and systemic corticosteroids. Curr
Opin Ophthalmol. 2000; 11(6): 478-483.
41. Katsarou A, Armenaka M, Vosynioti V, Lagogianni E, Kalogeromitros D, Katsambas A. Tacrolimus ointment 0.1% in the treatment of allergic contact eyelid dermatitis.
J Eur Acad Dermatol Venereol. 2009;23(4): 382-387.
42. Ring J, Möhrenschlager M, Henkel V. The US FDA ‘black box’ warning for topical calcineurin inhibitors: an ongoing controversy. Drug Saf. 2008; 31(3):185-98.
Dr. Jacob, the Section Editor of Allergen Fo-cus, is Associate Clinical Professor of Medicine and Pediatrics WOS (Der-matology) at the Univer-sity of California, San Diego.
Disclosure: Dr. Jacob is the principal investiga-tor for Smartchoice USA PREA-2 trial.