This presentation contains forward-looking statements - that is,
statements related to future, not past, events. These statements
may be identified either orally or in writing by words as "expects",
"anticipates", "intends", "plans", "believes", "seeks", "estimates",
"will", "may" or words of similar meaning. Such statements are
based on our current expectations and assumptions, and
therefore are subject to various risks and uncertainties that could
cause the actual results, performance or achievements to differ
materially from any future results, performance or achievements
that may be expressed or implied by such forward-looking
statements. These factors include, without limitation, those
discussed in our public reports filed with the Frankfurt Stock
Exchange. The company does not assume any obligations to
update or revise any of these forward-looking statements, even if
new information becomes available in the future.
Medigene – a strong player in immunotherapy
Medigene's immunotherapies are tailored to
address different types and stages of cancer
DC vaccines low tumour burden TCR-modified T cells T cell-specific mabs high tumour burden unwanted T cells DCs TCRs TABs
Platform 1: Therapeutic dendritic cell (DC) vaccines
5 As monotherapies, DC vaccines will likely be most effective for use in
patients with minimal residual disease. They can be used in combination therapies for larger tumour burdens and to induce antitumour responses in patients where spontaneous responses have not occurred. Audio-visual DCs
DC vaccines
TCR-modified T cells
T cell-specific antibodies
arms patient-derived T cells ex vivo with suitable T cell receptors
that enable them to detect and efficiently kill cancer cells in vivo
deplete unwanted T cells
Monotherapy or Combination therapies
Adoptive T cell therapy with TCRs:
T cell-specific antibodies (TABs):
What are Medigene's “now generation” DC vaccines?
maturation cocktail GM-CSF + IL-4maturation cocktail
with TLR 7/8 agonist
“now generation”
for optimal innate and
adaptive immunotherapy
IL-12high IL-10low mDC monocytes 1st generation immature DCs 2nd generation 7-9-day mature DCs “Now generation“ 3-day polarized mDCs (2nd generation)Medigene‘s DC vaccine phase I/II trial in AML
Started on 24 March 2015
Trial design:
Phase I/II multi-centre, open-label, prospective, non-randomized
trial
20 AML patients (6 phase I + 14 phase II) with complete remission
after chemotherapy who are not eligible for allo-transplantation
Primary objectives: Feasibility and safety
Secondary objectives: Induction of immune responses, Control of
minimal residual disease (MRD), Clinical response: time to
progression (TTP)
Vaccinated for 50 weeks and a follow-up period of one year or until
progression.
Medigene’s DC vaccines display optimal properties
Optimal biological properties for improved clinical efficacy
Defined antigen loading replaces unknowns with peptides and lysates Use of full length antigen requires no need for HLA selection
Positive co-stimulatory profile with young 3-day mature dendritic cells Optimal cytokine polarization to induce innate and adaptive responses High yields allow extended vaccination of patients
Optimal product characteristics for commercialization
3-day production is cost effective and amenable to automation
RNA as source of antigens is versatile, inexpensive and no need for tumour material Single-batch production reduces time, costs and is patient friendly (only one apheresis) Frozen vaccine formulation gives long shelf-life and simplified logistics
TCR-modified T cells
Platform 2: TCR-modified adoptive T cell therapy
9
induce the maturation of own, cancer-specific dendritic cells and
trigger both T cells and natural killer cells to attack the tumour
DC vaccines
T cell-specific antibodies
deplete unwanted T cells
Dendritic cell (DC) vaccines:
T cell- specific antibodies (TABs):
Adoptive cell therapy with TCR-modified lymphocytes allows patients to be given ready-made immune responses with large numbers of activated T cells that are needed to eradicate large tumour burdens. Billions of TCR-modified T cells can be prepared in a matter of weeks. Audio-visual TCRs
Large advanced and bulky tumour loads
DC vaccinesTCR-modified T cells
Patient T cells TCR-engineered patient T cells with antitumour specificity viral-vector mediated TCR transfer
Platform 2: Adoptive T cell therapy with TCR-modified
patient T cells for high tumour burden
Patient T cells are isolated from
blood samples and activated
Appropriate TCR is selected
from off-the-shelf library
Anti-tumour TCR is introduced
using a viral vector
Modified T cells are expanded to
large numbers in 10-15 days
Modified T cells are reinfused
into patient
11
Patient T cells are tailored to tumour type
using library of therapeutic TCRs
TCR-modified
patient T cells
Library of therapeutic TCRs
(as recombinant vectors)
TCR-1 TCR-2 TCR-3 TCR-4 TCR-5 TCR-6 TCR-7 TCR-8 TCR-9 AML NSCLC Prostate cancer
Medigene's technology delivers high versatility to
build library of therapeutic TCRs
No need for patient blood
In vitro system using healthy donors
TCRs specific for any HLA and antigen
mDCThe Process: T cells to acquire therapeutic TCRs
The Product: Therapeutic TCRs to modify patient T cells
High affinity without mutation
Specific for well selected target antigens
Extensively screened for safety
TCRs allow many more antigens to be targeted
compared to CARs
TCR/CD3 complex ITAM chain CM I: CD28 ITAM chain CM I: CD28 CM II: CD134/CD137 ITAM chain ε CD3 δ CD3 Cα Cβ Vα Vβ γ CD3 CD3 εChimeric antigen receptor (CAR)
TCRs:
• Recognize
intracellular targets
,
with many thousands of options
• Recognition is
MHC-restricted
CARs:
• Limited to
cell surface antigens
, only tens of
options
• Recognition is
MHC-independent
Adapted from Cartellieri et al, 2010
Medigene’s threefold value creation along the
TCR development chain
Value creation through:
TCR R&D collaborations with external academic/commercial partners
TCR product development collaborations with commercial partners
Medigene Immunotherapies’ own TCR product development programme
TCR
generation
module
TCRs
GMP
production
module
TCR
therapies
TCR clinical
development
programme
1 2 3 1 2 3Medigene’s TCR-based therapy displays
optimal properties
Optimal biological properties for improved clinical efficacy
TCRs are easily isolated for diverse MHC allotypes and antigens from healthy donors Wide range of affinities allow selection of lead TCRs with optimal sensitivity
Natural sequences of lead TCRs with no need for mutation to improve sensitivity
Optimal product characteristics for commercialization
TCR library allows patients with different MHCs to be included in treatment
High safety profile established through extensive in silico, in vitro and in vivo assays TCR-modified T cells display optimal functional characteristics
Platform 3: T cell-specific monoclonal antibodies
induce the maturation of own, cancer-specific dendritic cells and
trigger both T cells and natural killer cells to attack the tumour
DC vaccines
TCR-modified T cells
arms patient-derived T cells ex vivo with suitable T cell receptors
that enable them to detect and efficiently kill cancer cells in vivo
Dendritic cell (DC) vaccines:
Adoptive T cell therapy (TCR):
T cell-specific antibodies
TABs can be used to eliminate unwanted T cells without causing deleterious cytokine storm. Elimination of unwanted T cells can be made while leaving normal T cell immunity intact for pathogen defense. Audio-visual TABs
T cell leukemia and autoimmunity
DC vaccinesTCR-modified T cells
Platform 3: TABs - TCR-specific monoclonal antibodies
for removal of misguided or unwanted T cells
Full-scope platform
for antibody isolation
Unique animal models
to assess MoA and clinical efficacy
Proof-of-principle of technology
is established
Ongoing studies establish
proof-of-concept in pre-clinical models
17
Unwanted T cells:
T cell leukemia
T cell drivers of autoimmunity
TCR-modified T cells:
T cell tracking
ex vivo
Characteristics of Medigene's TAB technology
Selective depletion
of unwanted T cells with
low toxicity
by TABs
Vector libraries
available to make
cellular screening
reagents
HT cellular screening systems
have been established and validated
Prototype antibodies
have been isolated using standard hybridoma methods
Unique humanized T cell-bearing mice
are available to study effects of
TABs in vivo
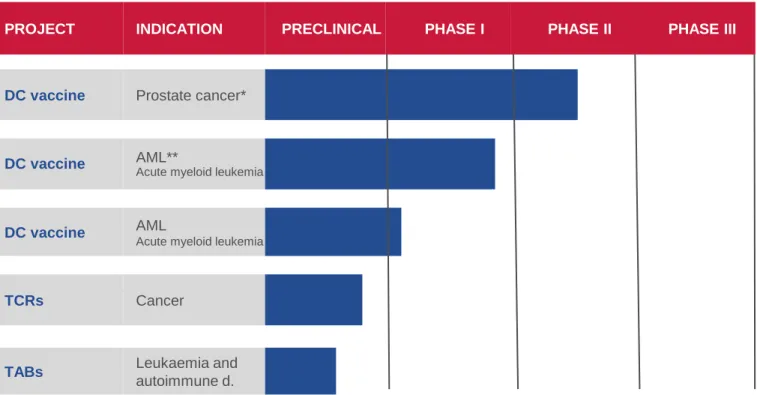
Medigene‘s immunotherapy pipeline
19
PROJECT INDICATION PRECLINICAL PHASE I PHASE II PHASE III APPROVAL MARKET
DC vaccine Prostate cancer*
DC vaccine AML** Acute myeloid leukemia
DC vaccine AML
Acute myeloid leukemia
TCRs Cancer
TABs Leukaemia and
autoimmune d.
* investigator initiated trial (IIT) Oslo University Hospital
Marketed/partnered pipeline (non-core)
Licence agreement with Falk Pharma for RhuDex® in hepatology and gastroenterology
Falk Pharma will fully fund all costs for development and commercialisation of RhuDex® in PBC
Medigene retains RhuDex® rights for rheumatoid arthritis and other autoimmune diseases
Numerous marketing partnerships for Veregen® in place
Currently marketed in the US, Canada, 17 European countries and Taiwan
Exclusive global license and development agreement for EndoTAG® with SynCore
Biotechnology
Outlook for immunotherapy platforms
DCs
Deliver therapeutic data in patients vaccinated for more than 1.5 years Conduct the company-sponsored phase I/II study in AML
Continue investigator-initiated trials and compassionate use programme
TCRs
Isolate TCRs with optimal affinities for lead candidate targets Develop up to 10 lead TCR candidates
Implement process for good manufacturing practice (GMP) Initiate clinical development
Start IIT phase I trial in H1 2016 (subject to grant funding) Commence two Medigene clinical trials in H2 2017/ H2 2018
TABs
Advance pre-clinical studies with the aim of achieving „proof of principle“
Expand pipeline with three immunotherapy programs
(DC/TCR/TABs) acquisition of Trianta
Integrate Trianta (now Medigene Immunotherapies) and
establish R&D team
Raise capital and expand lab capabilities
Present data at ASH and AACR
Start own clinical DC trial in AML
Secure mid-term financing
Develop up to 10 lead candidates in TCR platform
IND/IMPD for IIT Phase I TCR trial
IND/IMPD for 2 Medigene TCR trials
Anticipated and completed milestones
(summary)
Q1/Q2 2014
Q2/Q3 2014
Q3/Q4 2014
Q4 2014 / Q1 2015
Q1 2015
Q3 2015
2016 ff
H1 2016
2017 / 2018
23
Financial guidance 2015 confirmed
2014 Guidance 2015
Veregen® royalties €2.4 m double digit percentage increase
Veregen® total revenue €5.2 m stable
R&D expenses
Immunotherapies €2.9 m €7-9 m
Funding for immunotherapy platforms through
capital measure successfully completed
Raising of €46.4 m by issuance of 5,594,178 new shares
Placement of all offered new shares for a subscription price of EUR
8.30
Participation of new renowned institutional investors from USA and
Europe, including QVT, a leading US-based sector specialist as
cornerstone investor
Enables Medigene to achieve important milestones in clinical
validation of the immunotherapy platforms
Continuation of DC vaccine & acceleration of TCR clinical
development programmes
Cash reach at least until H2 2019
25
Capital measure added new institutional
investors
*
*Capital increase July 2015/ based on last voting right notifications **Shareholding below 3%
Key share information
• Current number of shares outstanding: 19,678,055 • Current market cap of ~ €140 m
Before capital measure
10,1% 5,5% 5,0% 4,4% 3,9% 71,1% Aviva SynCore Ridgeback DJS Montana RTW Master Fund Freefloat **
Current shareholder structure
15,6% 9,7% 3,9% ~3,0% 6,2% 3,3% 4,0% 54,3% QVT Aviva SynCore Ridgeback Morgan Stanley DJS Montana RTW Master Fund Freefloat **
A fully established biopharmaceutical company
Complete infrastructure with expertise in Medical Affairs, CMC (QM, GMP, GLP, GCLP), Quality Control, Regulator Affairs, Business Development, Alliance Management, IP,
Management team: Track record from pre-clinical
development to marketed products
Frank Mathias Ph.D. – CEO
• Pharmaceutical marketing experience at general management level with international companies • To 2008 corporate VP and General Manager Germany of Amgen
• Responsible for Commercial Operations & Alliance Management, Supply Chain Management,
CMC/Quality Control, Quality Assurance and Regulatory Affairs
Prof. Dolores Schendel Ph.D. – CSO
• Served as Member of the German Cancer Aid Grants Review Panel and Chair of a Life Science
Study Panel of the European Research Council
• To 2014 Director of the Institute of Molecular Immunology of German Research Center for
Environmental Health
• Professorship in immunology at the Ludwig Maximilians University of Munich
• Founder of Trianta Immunotherapies GmbH (now Medigene Immunotherapies GmbH)
• Responsible for Research / Immunotherapies, Preclinical Development, Clinical Development
and Medical & Scientific Affairs
Peter Llewellyn-Davies – CFO
• Commercial and financial experience at C level in international companies • To 2012 CFO of Wilex AG
• Responsible for Administration, Business Development, Finance, Purchasing, Corporate
Communications, Human Resources, IT, Intellectual Property and Legal Affairs
Medigene AG
Lochhamer Straße 11
82152 Planegg / Martinsried
Germany
Listed on Frankfurt Stock Exchange (MDG, Prime Standard)
T +49 - 89 - 20 00 33 - 0
F +49 - 89 - 20 00 33 - 2920
www.medigene.com
Medigene AG
Lochhamer Strasse 11
82152 Planegg / Martinsried
Germany
Listed on Frankfurt Stock Exchange (MDG1, Prime Standard)
T +49 - 89 - 20 00 33 - 0
F +49 - 89 - 20 00 33 - 2920
www.medigene.com