65
Clustering of Strokes in Association
With Meteorologic Factors in the
Negev Desert of Israel: 1981-1983
Vladimir M. Berginer, MD, PhD, John Goldsmith, MD, MPH, Uri Batz, MSc, Hilell Vardi, MSc, and Yair Shapiro, MD
Clinical observations of the apparent clustering of daily stroke admissions to a regional hospital in an arid climate prompted our investigation of possible meteorologic factors associated with stroke admissions. Daily hospitalization and meteorologic data were studied for 895 patients with stroke admitted to Soroka Medical Center, Beer-Sheva, Israel, during 1981, 1982, and 1983. The average daily incidence of stroke was about twice as great on relatively warm days as on relatively cold ones. This increase may be explained by increases in thromboembolic mecha-nisms secondary to physiologic changes in response to heat. When heat waves are predicted, information on the added risk for stroke needs to be disseminated to both the population and to health care providers so preventive measures can be instituted. Special attention should be devoted to air conditioning and adequate consumption of liquids, and antiplatelet aggregation medication such as aspirin should be considered. (Stroke 1989;20:65-69)
S
troke is the third leading cause of death in Israel, as in other countries.1-5 Epidemio-logic studies have confirmed a significant decline in the mortality rate from both cardiovascu-lar disease and stroke over the past 20 years.5-9 Possible reasons include treatment of modifiable risk factors such as hypertension, cardiac diseases, hyperglycemia, and hypercholesterolemia.One of us observed for many years that stroke admissions to Soroka Medical Center appear to occur in clusters. On some days there are one or no admissions, and these days tend to be grouped; on other days or groups of days there are multiple admissions. In such a short period as a few days, risk factors such as age, sex, and heredity and variable disease risk factors such as hypertension, cardiac disease, and diabetes mellitus are unlikely to change. We looked for risk factors that could change over a period of hours to days and decided that meteorologic factors should be evaluated. This
From the Neurological Department, Neurovascular Unit (V.M.B.), The Unit of Epidemiology and Health Services Eval-uation (J.G., H.V.), and the Soroka Medical Center and Faculty of Health Sciences (Y.S.), Ben-Gurion University of the Negev, Beer-Sheva and The Israeli Meteorological Service, Beit Dagan (U.B.), Israel.
Presented in part at the Inaugural Meeting of the European Neurological Society, June 21, 1988, Nice, France.
Address for reprints: V.M. Berginer, MD, PhD, Chief, Neu-rovascular Unit, Department of Neurology, Soroka Medical Center, PO Box 151, Beer-Sheva 84101, Israel.
Received September 24, 1987; accepted August 4, 1988.
led us to examine the possible associations of meteorologic factors and daily stroke admission for Soroka Medical Center.
The influence of climate on health is known empirically from ancient times.10 Regional differ-ences in standardized mortality ratios for stroke (suggesting environmental factors) have been doc-umented in Europe, the United States, Japan, and other countries.1'-15 Studies of the relation between stroke and meteorologic parameters have yielded controversial results in different geographic areas, but in most cases the studies confirmed a correla-tion of weather with strokes.16-27 However, these comparisons were made between different years, seasons, or months rather than over days or weeks. Our investigation is based on day-by-day data for 3 consecutive years (1981, 1982, and 1983).
Soroka Medical Center is the sole regional hos-pital and provides nearly all services for a popula-tion of approximately 300,000 in a relatively iso-lated region of the Negev Desert. Virtually every patient with stroke arrives at the emergency room and is admitted to the hospital. Average time from the onset of stroke until hospitalization is several hours, and the time is rarely more than 1 day.
Subjects and Methods
We defined stroke according to the World Health Organization as rapidly developing clinical signs of focal (or global) disturbance of cerebral function, which led to death or lasted >24 hours (strokes) or
66 Stroke Vol 20, No I, January 1989
<24 hours (transient ischemic attacks, TIAs), with no apparent cause other than vascular.2 Patients with mild TIAs who were not hospitalized were not included, nor were patients with strokes who died before admission. Subdural and extradural hemato-mas were excluded because they primarily reflect external trauma.
In the Negev population the medical policy is to hospitalize all patients with acute stroke. The diag-nosis of acute stroke was made primarily by the emergency room staff, which included a resident from neurology; the emergency room is also the admissions unit of our hospital.28 The majority of patients were hospitalized in the neurology depart-ment, with the remaining patients in the internal medicine departments. Final diagnosis of ischemic or hemorrhagic stroke was confirmed or excluded by the staff of the neurology department, which includes several residents and senior neurologists. Diagnosis was based on clinical criteria supple-mented when indicated by cerebral computed tomography (CT), ultrasonography, and electroen-cephalography. All patients undergo laboratory investigations, including blood count and chemis-try, which allow us to exclude metabolic causes of mental or neurologic abnormalities. Cerebrospinal fluid was examined when meningeal findings were present. Cerebral angiography was performed if arteriovenous malformation or aneurysm was sus-pected or before vascular surgery.
The number of daily stroke admissions was obtained from the computerized file of hospital discharges, based on ICD code numbers 431-436. In 1981, there were 333, in 1982 there were 283, and in 1983 there were 279 admissions with acute stroke as the primary diagnosis.
The number of daily admissions was compared with the following meteorologic parameters mea-sured every 6 hours in the Beer-Sheva area near the hospital: air temperature, barometric pressure at the elevation of the observatory, relative humidity, dew point temperature, wind velocity, and wind direction. At an elevation equal to 500 mbars of pressure, only air temperature, wind direction, and wind velocity were registered at noon and midnight. These data were obtained from the Israeli Meteo-rological Service on a daily basis for 1981, 1982, and 1983. After examining these parameters in a prelim-inary study, we selected four commonly used mete-orologic conditions29 for tabulation and analysis.
1. A cold high, or cold anticyclone, is a high-pressure (5-15 mbars above the monthly mean barometric pressure) system on the surface that weakens with elevation and changes into an upper trough. A cold high is characterized by air that is colder near its center than around its periphery. In the Negev Desert a cold high occurs only during the winter. Maximal daily temperature (T°) drops to 5 -10° C below the monthly mean but freezing is rare. 2. A warm high, or warm anticyclone, is a high-pressure system on the surface that intensifies with
TEMPERATURE G
J A N F E B U A R A P n U / y j U N J U L A U O S E P O C T N C W D F C MONTH
FIGURE 1. Monthly mean maximal daily temperatures
over 30 years for weather station of Beer-Sheva, Israel, within 1 km of Soroka Medical Center. Temperatures below freezing are rare.
elevation into an upper ridge. A warm high is characterized by air that is warmer at its center than around its periphery. The atmosphere is stable. T° increases to 5-15° C above the monthly mean. Relative humidity decreases to <20%.
3. A cold low, or cold cyclone, is a low-pressure system on the surface that intensifies with elevation into an upper trough. A cold low is characterized by air that is colder at its center than around its periphery. T° drops to 5-10° C below the monthly mean, and barometric pressure decreases to 5-15 mbars below its monthly mean. The atmosphere is unstable.
4. A warm low, or warm cyclone, is a low-pressure system (5-10 mbars below the monthly mean barometric pressure) on the surface that weak-ens with elevation and changes into an upper ridge. A warm low is characterized by air that is warmer (5-15° C above the monthly mean) at its center than around its periphery. Relative humidity decreases to <25-3O%.
5. A nonspecific system is one not exactly defin-able as any of the previous conditions.
Daily meteorologic parameters were compared with historic monthly means. For example, monthly mean T° in Beer-Sheva for the last 30 years is shown in Figure 1. A warm day therefore is one for which T° is above the historic monthly mean T°, and a cold day is one for which T° is below the historic monthly mean T°.
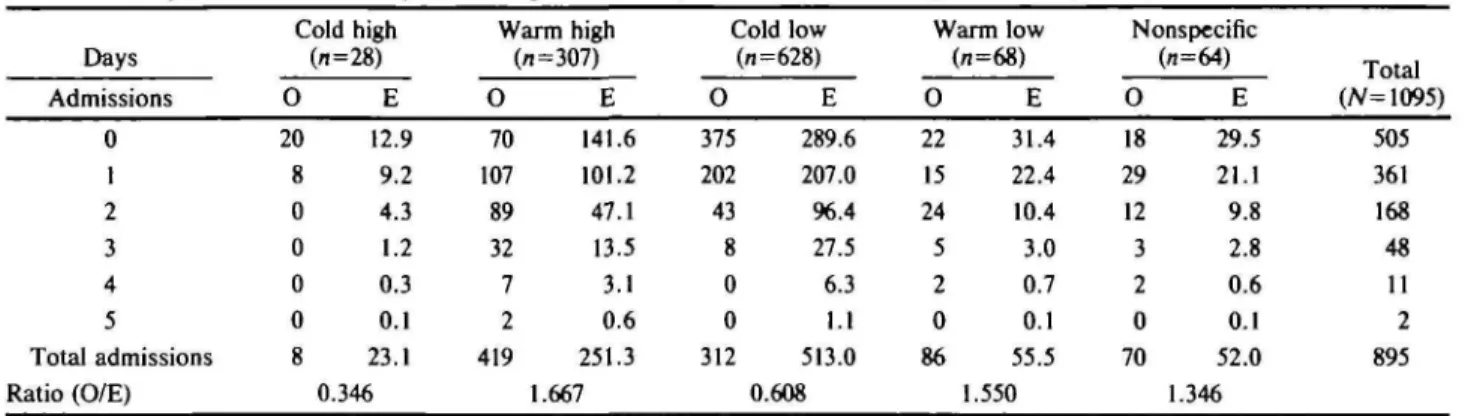
The expected number of days with 0, 1, 2, 3,4, or 5 admissions for each set of meteorologic condi-tions was computed by multiplying the overall pro-portion of days with 0, 1,2,3,4, or 5 admissions by the total number of days with a given meteorologic condition. Observed-to-expected ratios were tested for significance by the x1 t est (see data in Table 1). Thus, overall 48 of 1095 days had three admissions; 48-^ 1095 x number of days in a meteorologic con-dition gives the expected number of days with three admissions in that condition.
TABLE 1. Daily Stroke Admissions by Meteorologic Conditions, Soroka Medical Center, Beer-Sheva, Israel, 1981-1983 Days Admissions 0 1 2 3 4 5 Total admissions Ratio (O/E) Cold high 0 20 8 0 0 0 0 8 (n=28) E 12.9 9.2 4.3 1.2 0.3 0.1 23.1 0.346 Warm high (/i=307) O 70 107 89 32 7 2 419 E 141.6 101.2 47.1 13.5 3.1 0.6 251.3 1.667 ( O 375 202 43 8 0 0 312 Hold low (n=628) E 289.6 207.0 96.4 27.5 6.3 1.1 513.0 0.608 Warm low O 22 15 24 5 2 0 86 (n=68) E 31.4 22.4 10.4 3.0 0.7 0.1 55.5 1.550 Nonspecific O 18 29 12 3 2 0 70 («=64) E 29.5 21.1 9.8 2.8 0.6 0.1 52.0 1.346 Total (JV=1095) 505 361 168
m
11 2 895Data are days within meteorologic condition with indicated number of stroke admissions. O, observed; E, expected. Results
The observed and expected number of days with given numbers of stroke admissions for the five meteorologic conditions are shown in Table 1. When the atmosphere was unstable and the ambient tem-perature was lower than the historic monthly mean (i.e., a cold low), there were no or only a few stroke admissions per day; the mean number of daily admissions was 0.28, compared with 0.817 for the entire 3-year period. Conversely, when the atmo-sphere was stable and the ambient temperature was higher than the historic monthly mean (i.e., a warm high or a warm low), the number of admissions for stroke increased to two, three, or even five per day; the mean number of daily admissions was 1.347 under these two conditions.
Thus, when warm conditions occurred, there were more stroke admissions (clustering); when the pressure system was a cold high or a cold low there were only a few or no stroke admissions. Table 1 contrasts the number of stroke admissions per day under different meteorologic conditions. In Figures 2 and 3 only warmer and colder days are shown.
Discussion
This study was performed in a specific area of dry climate conditions, the Negev Desert, which has a sparse population and includes more than half the land area of Israel. Virtually all of the population is served by a unified health care system with a single receiving hospital. Since our policy is to admit all patients with stroke, the stroke admission rate closely reflects the stroke incidence rate, and their fluctuations are similar.
We set out to analyze the associations of stroke incidence with the meteorologic parameters temper-ature, barometric pressure, humidity, and wind speed in terms of both absolute value and devia-tions from monthly means. However, after initial examination we decided to categorize the meteoro-logic parameters into the four conditions commonly used by meteorologists.29 In each year approxi-mately 20 days could not be categorized; these 20 days have been designated nonspecific. We recog-nize that many meteorologic parameters change
together, and our choice of temperature as the principal parameter in further analysis does not preclude any one or another parameter's having an influence. We did not find significant seasonal dif-ferences in daily stroke admissions, but we did find a significant influence of short-term changes of T°. Therefore, we analyze and discuss our data in terms of daily deviations from monthly mean temperature (Figures 2 and 3).
Table 1 shows that under cold low conditions there were 60.8% of the stroke admissions expected based on the 3-year average. On the other hand, the warm high condition showed the opposite results, with 66.7% more stroke admissions than expected. These results are consistent for all 3 years, and based on appropriate statistical procedures are highly unlikely to be the result of chance variation. Because the greater contrast is across two groups based only on temperature compared with two groups based only on barometric pressure, we focus our discus-sion on the possible effects of temperature, shown in Figures 2 and 3.
One may speculate concerning possible mecha-nisms of the association of stroke admissions and
2.0MEAN NUMBER OF ADMISSIONS Pf!n DAY
0.6 0.0 1961 1882 YEARS 1983 • I (XXDFH H 5 W.RMER
FIGURE 2. Mean number of daily stroke admissions by
year, Soroka Medical Center, Beer-Sheva, Israel, accord-ing to whether each day's maximal daily temperature was warmer or cooler than historical mean for that month. Differences between warmer and cooler days are signifi-cant, p<0.01, for each year, by x2 test.
1 Stroke Vol 20, No 1, January 1989
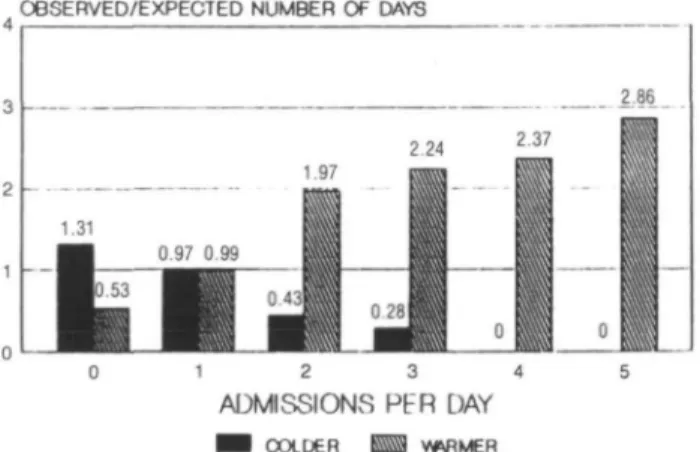
OBSERVED/EXPECTED NUMBER OF DAYS
2.86
1 2 3
ADMISSIONS Pt"R DAY
COLDER WRMER
FIGURE 3. Ratio of observed days with given number of
stroke admissions and days expected if there were no meteorologic effects on number of stroke admissions per day. Days warmer than historical mean have relatively more daily admissions. There were never more than three stroke admissions on any colder day.
hot weather. Exposure to heat is likely to cause dehydration, increasing the viscosity of the blood. Peripheral vasodilatation, especially of the blood vessels of the skin, is a response to heat; such vasodilatation does not occur in the central vascu-lature. While the brain is an autoregulated organ, there are some experimental observations showing a reduction of blood supply to the central nervous system during heat exposure.3031 Consequently, there might be a decrease of perfusion to the internal organs and brain. An increase in clotting factors might also occur as a consequence of an increase in body temperature.32-34 These effects in persons without vascular diseases might cause no damage, while in older patients with vascular dis-ease the effects could predispose to thromboem-bolic episodes.33 During cold conditions, even if body temperature remains stable, the blood is some-what less viscous, the blood volume as well as the Wood pressure is likely to increase, and perfusion of the brain and internal organs is favored because of peripheral vasoconstriction. This could increase the incidence of hemorrhage in the internal organs and brain.2534
Thus, during hot conditions thromboembolic epi-sodes are more likely, whereas during cold condi-tions hemorrhagic episodes are likely. In patients hospitalized in departments other than the neurol-ogy service, we were less able to separate clearly thromboembolic and hemorrhagic stroke. We have therefore lumped all cases of stroke, realizing that thromboembolic cases would predominate.
Based on our results, the risk of stroke is 2.76 times greater during warm than during cold days. Similar results were obtained in a preliminary pilot study on stroke in the Beer-Sheva area in 1970-1974.36 These findings are similar to those of Oechsli and Buechley,37 who studied three Los Angeles heat waves, of Keatinge et al33 from London, of
Ellis and Nelson38 from New York, and of Olivares et al22 from Mexico. Our findings differ from the results of Christie20 from Melbourne, Ohno et al21 from Japan, and Barer et al39 from Nottingham, who did not find associations between stroke incidence and temperature. Sontaniemi et al23 and Ramirez-Lassepas et al25 observed more hemorrhagic sodes in the winter and more thromboembolic epi-sodes in the summer. This may be explained by additional studies of Ohno,40-42 who showed that climatic effects tend to increase as one moves away from the "comfort zone"; more cases of stroke were found when the temperature was greater than 30° C or less than -10° C. When the temperature was 15-26° C, the number of strokes was minimum. Similar findings were published by Rogot and Padgett.43 Where air temperature very rarely drops below -10° C and low temperatures occur at night when most of the population is indoors, these populations are in effect not exposed to the cold. By contrast, in the Negev Desert during hot weather, with temperatures above 30° C and relatively little air conditioning, our population actually experi-ences the impact of heat. In the first article by Ohno et al21 as well as in the observations from Notting-ham of Barer et al39 and Christie's20 study from Melbourne, a climate pattern different from ours was observed. The populations were not exposed to unusually high temperatures because the summer in those studies is characterized by mean tempera-tures of <24° C.
In summary, we have shown that in an arid zone, warm days are days of greater incidence of stroke (Table 1, Figures 2 and 3). This increase can be explained by increases in thromboembolic mecha-nisms secondary to physiological changes in response to heat (dehydration, increased blood vis-cosity and hemoconcentration, decrease in blood pressure, and increased concentration of platelets). When heat waves are predicted, the facts concern-ing the added risk for stroke should be disseminated to both the population and to their health care providers so preventive measures can be instituted. Attention should be devoted on such days to air conditioning and adequate consumption of liquids, and antiplatelet aggregation medication such as aspirin should be considered.
Acknowledgments
The authors express their thanks to Dr. A. Cohen, Assistant Medical Director, to Mr. S. Barashi, Administrative Director, to Mr. Y. Leibovich, Med-ical Receptions Service, and to Mrs. R. Lichten-heim, Medical Records Office, for their assistance and to Mrs. B. Savell for typing the manuscript.
References
1. Malmgren R, Bamford J, Warlow C, Sandercock P: Geo-graphical and secular trends in stroke incidence. Lancet 1987;2:1196-1200
2. Aho K, Harmsen P, Hatano S, Marquardson J, Smirnov V, Stresser T: Cerebrovascular disease in the community: Results of a WHO collaborative study. Bull WHO 1980; 58:113-130
3. Adler E. Stroke in Israel. Jerusalem, Polypress Ltd, 1969, p264
4. Melamed E, Cahane E, Carmen A, Lavy S: Stroke in Jerusalem district 1960 through 1967. An epidemiological study. Stroke 1973;4:465-471
5. Epstein L, Zaaroor M: Mortality from ischemic heart dis-ease and cerebrovascular disdis-ease in Israel, 1969-1978. Stroke 1982;13:570-573
6. Soltero 1, Liu K, Cooper R, Stamler J, Garside D: Trends in mortality from cerebrovascular diseases in the United States, 1960 to 1975. Stroke 1978;9:549-558
7. Whisnant JP: The decline of stroke. Stroke 1984; 15:160-168 8. Ueda K, Omae T, Hirota Y, Takeshita M, Katsuki S, Tanaka K, Enjoji M: Decreasing trends in incidence and mortality from stroke in Hisayama residents, Japan. Stroke 1981;12:154-160
9. Alfredsson L, von Arbin M, de Faire U: Mortality from and incidence of stroke in Stockholm. Br Med J 1986; 292:1299-1303
10. Jones WHS (trans). Hippocrates' Air, Waters and Places. London, Heineman, 1923
11. Garraway WM, Whisnant JP, Furlan AJ, Phillips LH II, Kurland LT, O'Fallon WM: The declining incidence of stroke. N Engl J Med 1979;300:449-452
12. Tanaka H, Tanaka Y, Hayashi M, Ueda Y, Date C, Baba T, Shagi H, Horimoto T, Owada K: Secular trends in mortality for cerebrovascular diseases in Japan, 1960 to 1979. Stroke
1982;13:574-581
13. Fratiglioni L, Massey EW, Schoenberg DG, Schoenberg BS: Mortality from cerebrovascular disease. International com-parisons and temporal trends. Neuroepidemiology 1983; 2:101-116
14. Takeya Y, Popper J, Shimizu Y, Kato H, Rhoads GG, Kagan A: Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California. Incidence of stroke in Japan and Hawaii. Stroke 1984;15:15-23
15. Alperovitch A, Mas J, Doyon B, Myquel D: Mortality from stroke in France 1968-1982. Neuroepidemiology 1986; 5:80-87
16. Saviola GA, Lazzari C, Scipione VL, Troianello B, Poloni A, Civili S: Comparative study between cerebral seizure and the climate trend in the province of Brescia. Minerva Med 1986;77:2187-2190
17. Thakur CP, Anand MP, Shahi MP: Effect of variation of temperature on the incidence of stroke. J Assoc Physicians
India 198634:855-857
18. Troshin VD, Suckina EG: Effect of meteorologic and solar factors on the psychophysiologic responses of healthy sub-jects and patients with vascular lesions of the brain. Zh
Nevropatol Psikhiatr 1986;86:1320-1323
19. Diachenko VK: Relation between the occurrence of acute cerebral circulatory disorders and changes in meteorologic factors. Zh Nevropatol Psikhiatr 1983;83:48-53
20. Christie D: Stroke in Melbourne, Australia: An epidemio-logical study. Stroke 1981;12:467-469
21. Ohno Y, Aoki N, Horibe H, Hayakawa N, Okada H: Biometeorologic studies on cerebrovascular disease. V. A multivariate analysis of meteorologic effects on cerebrovas-cular accident. Jpn Circ J 1974;38:195-208
22. Olivares L, Castaneda E, Grife A, Alter M: Risk factors in stroke: A clinical study in Mexican patients. Stroke 1973; 4:773-781
23. Sotaniemi E, Palva IP, Hakkarainen HG: Effect of environ-mental temperature on hospital admissions for cerebrovas-cular accidents. Ann Clin Res I972;4:233-235
24. McDowell FH, Louis S, Monahan K: Seasonal variation of nonembolic cerebral infarction. J Chronic Dis 1970^3:29-32 25. Ramirez-Lassepas M, Haus E, Lakatua DJ, Sackett L, Swoyer J: Seasonal (circannual) periodicity of spontaneous intracerebral hemorrhage in Minnesota. Ann Neurol 1980; 8:539-541
26. Haberman S, Capildeo R, Rose FC: The seasonal variation in mortality from cerebrovascular disease. J Neurol Sci 1981;52:25-36
27. Sulman G: Human weather sensitivity. Isr Meteorolog Res
Papers 1977; 1:45-49
28. Gross J, Goldsmith JR, Zangwill L, Lerman S: Monitoring of hospital emergency room visits as a method for detecting health effects of environmental exposures. Sci Total Environ 1984;32:289-302
29. Pettersen S: Introduction to Meteorology. New York, McGraw-Hill Book Co, 1960
30. Hales JRS, Dampney RAL: The redistribution of cardiac output in the dog during heat stress. J Thermal Biol 1975;
1:29-34
31. Hales JRS: Effects of exposure to hot environments on the regional distribution of blood flow and on cardiorespiratory function in sheep. Pflugers Arch 1973,344:133-148
32. Schafer AI: The hypercoagulable states. Ann Intern Med 1985;102:814-828
33. Keatinge WR, Coleshaw SRK, Easton JC, Cotter F, Mat-tock MB, Chelliah R: Increased platelet and red cell counts, blood viscosity and plasma cholesterol levels during heat stress and mortality from coronary and cerebral thrombosis.
Am J Med 1986;81:795-800
34. Morimoto T, Nose H, Miki K: Blood volume and cardiovas-cular function during acute hyperthermia and hypothermia, in Hales JRS (ed): Thermal Physiology New York, Raven Press Publishers, 1984, pp 385-388
35. Collins KJ, Excton-Smith AN: Thermal homeostasis in old age. J Am Geriatr Soc 1983^1:519-524
36. Berginer VM, Korczyn AD, Bendel J: Stroke in the
Beer-Sheva Area and the Negev Desert. Excerpta Medica
(abstract), No 427, 1977, p 222
37. Oechsli FW, Buechley RW: Excess mortality associated with three Los Angeles heat waves. Environ Res 1970; 3:277-284
38. Ellis FP, Nelson F: Mortality in the elderly in a heat wave New York City, August 1975. Environ Res 1978;15:504-512 39. Barer D, Ebrahim S, Smith C: Factors affecting day to day incidence of stroke in Nottingham. Br Med J 1984;289:662 40. Ohno Y: Biometrical studies on cerebrovascular diseases I.
Effects of meteorologic factors on the death from cerebrovas-cular accident. Jpn Circ J 1969^3:1285-1298
41. Ohno Y: Biometrical studies on cerebrovascular diseases II. Seasonal observation on effects of meteorologic factors on the death from cerebrovascular accident. Jpn Circ J 1969; 33:1299-1308
42. Ohno Y: Biometrical studies on cerebrovascular diseases
III. Effects by the combination of meteorologic changes on
the death from cerebrovascular accident. Jpn Circ J 1969; 33:1309-1314
43. Rogot E, Padgett SJ: Association of coronary and stroke mortality with temperature and snowfall in selected areas of the United States, 1962-1966. Am J Epidemiol 1976; 103:565-575
KEY WORDS • cerebrovascular disorders • epidemiology • Israel • meteorological factors