Orthopaedics&Traumatology:Surgery&Research101(2015)655–659
Available
online
at
ScienceDirect
www.sciencedirect.com
Original
article
Change
in
acetabular
version
after
lumbar
pedicle
subtraction
osteotomy
to
correct
post-operative
flat
back:
EOS
®
measurements
of
38
acetabula
T.
Masquefa
∗,
N.
Verdier
,
O.
Gille
,
L.
Boissière
,
I.
Obeid
,
C.
Maillot
,
C.
Tournier
,
T.
Fabre
Serviced’orthopédietraumatologie,hôpitalPellegrin,placeAmélie-Raba-Leon,33076Bordeauxcedex,France
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received15December2014 Accepted16July2015 Keywords: Acetabularretroversion Transpedicularosteotomy Pediclesubtractionosteotomy Totalhiparthroplasty Sagittalbalancea
b
s
t
r
a
c
t
Background:Abnormalitiesinacetabularorientationcanpromotethedevelopmentofhiposteoarthritis,
femoro-acetabularimpingement,orevenacetabularcupmalposition.Theobjectiveofthepresentstudy wastodeterminewhetherpediclesubstractionosteotomy(PSO)tocorrectsagittalspinalimbalance affectedacetabularorientation.
Hypothesis:PSOperformedtocorrectsagittalspinalimbalanceaffectsacetabularorientationbychanging
thepelvicparameters.
Materialsandmethods: Thiswasadescriptivestudyinwhichtwoobserversmeasuredtheacetabular
parametersonbothsidesin19 patients(38acetabula)beforeandafterPSOforpost-operative flat-backsyndrome.MeantimefromPSOtopost-operativemeasurementswas19months.Measurements weretakentwiceata2-weekinterval,onstandingimagesobtainedusingtheEOS®imagingsystem
andsterEOS®softwaretoobtain3Dreconstructionsofsynchronised2Dimages.Acetabularanteversion andinclinationweremeasuredrelativetotheverticalplane.Meanpre-PSOandpost-PSOvalueswere comparedusingthepairedt-test,andPvalueslowerthan0.05wereconsideredsignificant.Toassess inter-observerandintra-observerreproducibility,wecomputedtheintra-classcorrelationcoefficients (ICCs).
Results:ThemeasurementsshowedsignificantacetabularretroversionafterPSO,of7.6◦ontherightand
6.5◦ontheleft(P<0.001).Acetabularinclinationdiminishedsignificantly,by4.5◦ontherightand2.5◦ ontheleft(P<0.01).Inclinationoftheanteriorpelvicplanedecreasedby8.4◦(P<0.01).Pelvicincidence
wasunchanged,whereassacralslopeincreasedby10.5◦(P<0.001)andpelvictiltdecreasedby10.9◦
(P<0.001).TheICCwas0.98forbothinter-observerandintra-observerreproducibility.
Conclusion:Changingthesagittalspinalalignmentmodifiesboththepelvicandtheacetabular
parame-ters.PSOsignificantlyincreasessacralslope,thusinducinganteriorpelvictiltwithsignificantacetabular retroversion.ThemeasurementsobtainedusingsterEOS®showedgoodinter-observerandintra-observer reproducibility.Toourknowledge,thisisthefirststudyofchangesinacetabularversionafterPSO.
©2015ElsevierMassonSAS.Allrightsreserved.
1. Introduction
Thepelvisconstitutesthejunctionbetweenthetorsoandthe lowerlimbs,asillustratedbythewell-known‘pelvicvertebra’ con-ceptintroduced byJ. Dubousset [1–4]. Loss of lumbar lordosis relatedtoarthrodesiscanresultinpost-operativeflat-back syn-drome,whichischaracterisedbyanteriorsagittalimbalance[5]as definedbythesagittalverticalaxis(SVA)orC7plumbline[6].
∗ Correspondingauthor.Tel.:+33675015402.
E-mailaddress:[email protected](T.Masquefa).
Posturalchangesdesignedtocorrecttheanteriorsagittal imbal-ance consist of posterior pelvic tilt with hip extension and, subsequently, knee flexion. Thus, compensation by the global extension reserve, which is the sumof the extrinsicextension reserveallowedbythelumbo-sacraljunctionandoftheintrinsic extensionreserveallowedbythehips[7,8],restoresthesagittal balanceuptoapoint[9].Whentheglobalextensionreserveisno longersufficient,sagittalimbalanceoccurs.
Totalhiparthroplasty(THA)withrestorationofagoodintrinsic extensionreservedoesnotseemtoaffectthepelvicparameters
[10]yet,insomepatients,resultsinreliefoflowbackpain[11]. Thisfactsupportsthehip-spinesyndromeconceptdevelopedby OffierskiandMacNab[12].
http://dx.doi.org/10.1016/j.otsr.2015.07.013
656 T.Masquefaetal./Orthopaedics&Traumatology:Surgery&Research101(2015)655–659
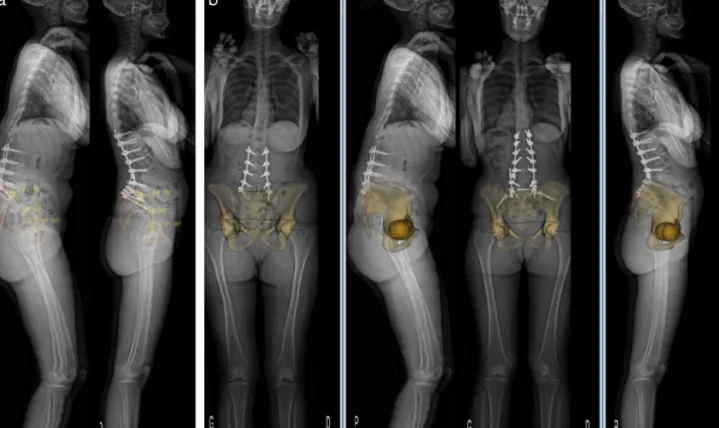
Fig.1. a:pelvicparametersbeforeandaftertranspedicularosteotomy.PI:pelvicincidence(◦);PT:pelvictilt(◦);SS:sacralslope(◦);b:3Dreconstruction.
Closeassociationslinkingpelvicparameterstoacetabular ori-entationhavebeendemonstrated[13].Legayeetal.[14]showed thatacetabularinclinationdependedchieflyonsacralslopeand,to alesserextent,onpelvicincidence.
Thedevelopmentofnewimagingtoolssuchasthelow-dose EOS®radiographicsystem(EOSImaging,Paris,France)hasallowed notonlya globalpostural analysis,butalsodynamic studiesof thefemur-pelvis-spinejunction[15–19].Whenmovingfromthe standingtotheseated position,thepelvis tiltsposteriorly [20]
andchangesoccurintheacetabularparameters[21,22],including increasedacetabularcupanteversion[23,24].
To correct the sagittal imbalance that characterises post-operative flat-back syndrome, one of the treatment options is surgery via the posterior approach with transpedicular closed-wedgeresectionosteotomy(pediclesubtractionosteotomy,PSO). Byinducinganteriorpelvictilt,PSOcausessignificantchangesin thepelvic parameters [25,26]. Themagnitude of thechange in pelvicorientationdepends onthelevelof thePSO [27].Toour knowledge,nostudieshavedirectlyinvestigatedtheinfluenceof lumbarPSOonacetabularparameters.
Theobjectiveofourstudywastodeterminewhetherlumbar PSOperformedtotreatpost-operativeflat-backsyndromeinduced statisticallysignificantchangesinacetabularversion.Asa prelim-inarystep,weevaluatedtherepeatabilityandreproducibilityof native-hipacetabularparametermeasurementsusingthesterEOS® system.
2. Materialandmethods
Aretrospectivedescriptivestudyofradiographicmeasurements was performed. Inclusion criteria were age>18years, lumbar transpedicular closed-wedge osteotomy to treat post-operative flat-back syndrome, and standing whole-body low-dose EOS® imagingbeforeandafterPSO.Exclusioncriteriawerethepresence, inadditiontoflat-backsyndrome,oflumbarorthoracicscoliosis
andinsufficientvisibilityoftheanatomicstructurescompromising theabilitytodeterminepelvicandacetabularparametersonthe EOS®images.
Twoobserversmeasuredpelvicandacetabularparameterson bothsidesinallpatients. Thesemeasurementswereperformed twice,atanintervalof2weeks,usingsterEOS®3Dsoftware(Fig.1a and b),which converts 2D imagesinto a 3D model. Thestudy parametersaredescribedbelow.
Pelvicparameters:
•pelvic incidence (IPI): angle formed by a perpendicular line throughthemiddleofthesacralendplateandtheline connect-ingthemiddleofthesacralendplatetothecentresofthefemoral heads;
•sacralslope(SS):angleformedbythehorizontalandaline tan-genttothesacralendplate;
•pelvictilt(PT):angleformedbytheverticalandtheline connect-ingthecentresofthefemoralheadstothemiddleofthesacral endplate;
•lumbarlordosis(LL):angleformedbythelinestangenttothe upperL1endplateandsacralendplate;
•anteriorpelvic plane(APP):planecontainingthetwo antero-superioriliacspinesandthepubis;
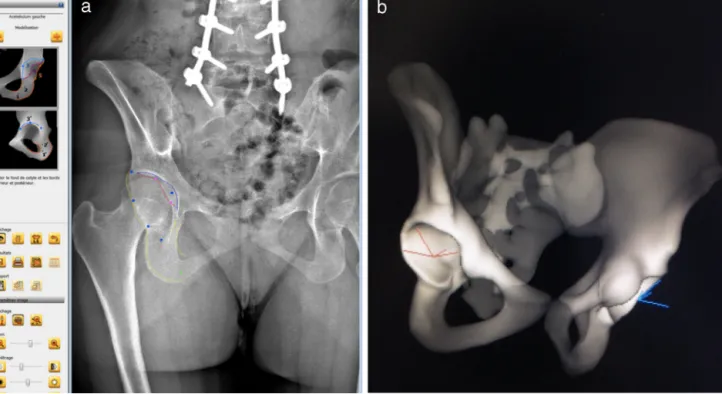
•APPinclination:angleformedbytheverticalandtheAPP. Acetabularparameters(Fig.2aandb):
•acetabularinclination(AI):angleformedbytheprojectionofthe horizontalplanecorrectedbytheaxisconnectingthecentresof theacetabulaandtheprojectionoftheacetabularopeningonthe coronalplane;
•acetabularanteversion(AA):angleformedbytheprojectionof thesagittalplanecorrectedbytheperpendiculartotheaxis con-nectingthecentresoftheacetabulaandtheprojectionofthe acetabularopeningonthecorrectedhorizontalplane.
T.Masquefaetal./Orthopaedics&Traumatology:Surgery&Research101(2015)655–659 657
Fig.2. a:acquisitionoftheacetabularparameters;b:3Dmeasurementofacetabularanteversionandacetabularinclination.
Theacetabularparameters(AIandAA)andAPPweremeasured relativetotheverticalplane,definedastheplanecontainingthe centresoftheacetabula(coronalplane).
Statistical analysis: ananalysis using thehistogram method establishedthatallstudyvariableswerenormallydistributed.The mean pre-operative and post-operative values of each variable werecomparedusingthepairedt-test.ValuesofP<0.05were con-sideredsignificant.Alinearregressionmodelwasbuiltusingthe least-squaresmethod.
Inter-observerandintra-observerreproducibilitywasassessed by computing the intra-class coefficients (ICCs) [28,29]. Cor-relations are considered very strong when the ICC is>0.95
[30].
3. Results
Thissingle-centrestudywasperformedfromMarch2010toJuly 2013.Ofthe22patientsincludedinitially,3wereexcluded, includ-ing2becauseofpoorvisibilityoftheacetabulum,mostnotablyits anteriorwall;and1becausetherightiliacwingwasoutsidethe acquisitionfield.Thisleft19patientsforthestudy,13femalesand 6 males,withameanageof61years(range,22–77years).Thus, 38 acetabulawerestudiedand76 measurementswereobtained byeachofthetwoobservers.MeantimefromPSO tothe post-operativemeasurementswas19months(range,1–35).
Table1 reportsthefindings ineach patientand Table2 the comparisons of the mean pre-operative versus post-operative
Table1
Radiographicvariablesmeasuredindegrees.
Pre-operativevalues(◦) Post-operativevalues(◦)
PI PT SS LL AAR AIR AAL IAL PI PT SS LL AAR AIR AAL AIL 56.9 27.9 27.2 18 27.9 57.1 23.8 58.5 52.4 17.4 34.3 46 22 57.6 22.2 59.9 33.6 20.1 13.7 4 27.4 51.2 21.5 50.2 31.9 5.4 26.3 37 11.5 51.4 14.3 49 47.8 22.7 26.3 23.1 29.6 56.1 23.6 54.6 53 23.7 31.5 41 25.4 54.9 20.1 56.1 66.1 49.1 15.9 27 33.9 64.2 35.6 62.8 68.1 40 25.2 53 27.5 56.1 25 61.5 76.7 55.3 20.7 20 39.9 66.6 36.8 64.8 80.3 44.5 34.5 70 32.2 53.8 28.5 57.6 37.8 42.6 −4.6 −6 36.4 69.5 34.1 67.8 44.1 34.2 10 40 30.1 61.2 29.3 60.6 59.2 36.6 22.3 30.6 34.1 62.5 34.2 62.5 58.6 12.9 46.6 54.8 14.4 52.9 15.7 52.4 48.7 29.4 17.9 12 23.4 60 26.2 60.4 51.7 15.7 35.8 42 15.6 54.4 17.7 56.7 59.8 32 25.1 17 23 60.8 25.8 58.3 61.3 21 42.2 52 20.6 55.1 20 55 40.4 17.6 20.2 15 24.6 54.6 20.7 55.3 39.1 8.3 28.6 50 19.9 53.7 17.7 60.3 56.6 26.3 28.3 41.9 30.2 62.7 26.3 57.4 46.8 11.7 35 67 23.3 56.8 22.1 56.1 57.7 33.7 22.9 30 30.9 58.9 33 60.2 58.5 28.7 29 53 22.5 59.3 24.7 57.1 45.2 7.2 38 15.8 22.7 43.2 31.2 45.5 40.1 −1.7 41.1 48 11.5 42.7 20.9 44.8 65.9 38.4 28.6 35 30.6 60.4 26.6 55.1 68.2 43.2 29.5 56 29.4 60.5 29.8 59.2 52.7 29.5 23 21 30.5 55.9 27.7 55.2 52.5 20.1 31.3 45 25.1 55.9 24.3 53.9 42 32.5 10.1 1 28.7 57.2 25.9 60.2 42.4 13.4 27.2 49 17.1 53.1 17.2 54.7 54 36.1 15.3 11 38.3 54.9 36.1 55.2 49.8 19.7 28.3 52 28.6 49.6 24.2 46.9 69.1 33.7 30.6 14 31.3 68.1 29.1 67.8 61.1 17.9 41.1 57.3 23.3 56.6 24.6 64.6 63.6 46.7 13.6 2.1 29.8 67.4 30.6 67.1 64.8 40.5 26 38 27.9 60 25.9 64.6
PI:pelvicincidence;PT:pelvictilt;SS:sacralslope;LL:lumbarlordosis;AAR:acetabularanteversionontheright;AIR:acetabularinclinationontheright;APPI:anterior pelvicplaneinclination.
658 T.Masquefaetal./Orthopaedics&Traumatology:Surgery&Research101(2015)655–659
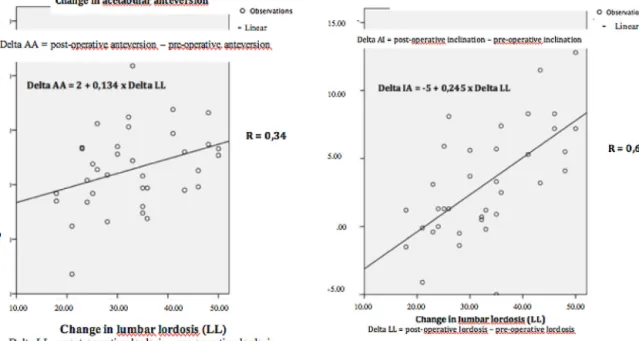
Fig.3. Linearregressionmodelbuiltusingtheleast-squaresmethod.
Table2
Radiographicvariablesmeasuredindegrees(mean±SD).
Variable BeforePSO(◦) Atlastfollow-upafterPSO(◦)
PI 54.4±11.4 53.9±11.9 PT 32.4±11.4 21.9±13.3 LL 17.5±12.2 50±8.9 APPI −15.9±14.4 −7.4±11 AAR 30.1±4.8 22.5±6.2 AAL 28.8±5.0 22.3±4.5 IAR 59.5±6.4 55±4.2 IAL 58.8±5.8 56.3±5.3
PSO:pediclesubtractionosteotomy;PI:pelvicincidence;PT:pelvictilt;LL:lumbar lordosis;APPI:anteriorpelvicplaneinclination;AAR:acetabularanteversionon theright;AAL:acetabularanteversionontheleft;AIR:acetabularinclinationon theright;AIL:acetabularinclinationontheleft.
Table3
Differencesinmeanvaluesindegrees. Variable Differenceinmeans
beforeandafterPSO(◦)
95%confidenceinterval P-value
PI 0.47 (−1.6;2.5) 0.63 PT 10.56 (7.4;13.7) <0.01 LL −32.56 (−37.2;−28) <0.01 APPI −8.48 (−14.3;−2.6) <0.01 AAR 7.65 (5.4;9.9) <0.01 AAL 6.56 (1.1;4.3) <0.01 IAR 4.5 (1;2.4) <0.01 IAL 2.5 (0.6;4.4) 0.013
PSO:pediclesubtractionosteotomy;PI:pelvicincidence;PT:pelvictilt;LL:lumbar lordosis;APPI:anteriorpelvicplaneinclination;AAR:acetabularanteversionon theright;AAL:acetabularanteversionontheleft;AIR:acetabularinclinationon theright;AIL:acetabularinclinationontheleft.
valuesofeachstudyvariable.ApartfromPI,allvariableschanged significantlybetweenthepre-operativeandpost-operative mea-surements (Table3). From pre-operative topost-operative, the meanchangeinLL(LL)was32◦andthemeanchangein acetab-ularversionconsistedin retroversionof 7.65◦ onthe rightand 6.56◦ontheleft.AImeasurementsshowedashifttowardsamore horizontalpositionof4.5◦ontherightand2.5◦ontheleft.
Changes from pre-operative to post-operative in AA (AA) and AI (AI) correlated significantly (R =/ 0) with LL. The
linear regression model built using the least-squares method showed simple linear relationships: AA=2+0.134·LL; and IA=−5+0.245·LL.ThecorrelationcoefficientswereRAA=0.34 andRIA=0.64(Fig.3).
Forquantitativevariables,boththeinter-observerICCandthe intra-observerICCvalueswere0.98.
4. Discussion
Thisstudydemonstratesthatspinalsurgicalproceduresaimed atinducinglargecorrectionsinsagittalalignmentmodifythe orien-tationoftheacetabula.Thus,PSOperformedtotreatpost-operative flat-back syndrome induces statistically significant acetabular retroversionandhorizontalisation.
Weselectedpatientswithpost-operativeflat-backsyndrome andweexcludedpatientswithscoliosisinordertofocusourstudy ondeformitiesinthesagittalplane.Althoughthesestrictinclusion criteriaresultedinlimitedstatisticalpower,themajoreffectofPSO incorrectingsagittalmalalignmentallowedustodetectsignificant changesinoursmallsample.Inallpatients,theinstrumentation extendeddowntothepelvisandthereforeimmobilisedthe sacro-iliacjoints.Thisfacteliminatedallriskofmeasurementbiasrelated tosacro-iliacjointmotion.
Despitethelimitedstatisticalpowerofthestudy,the measure-mentsmadeonEOS®imagesusingsterEOS®3Dsoftwareshowed verygoodreproducibilityandrepeatability.Althoughthechanges inacetabularorientationseemedtocorrelatewiththechangesin LL,thefairlylowcorrelationcoefficients(RAA=0.34andRI=0.64) indicatethatourresultsarenotsufficientlyrobusttoallow defini-tiveconclusions. A study offering greaterstatistical power and including the identification of potential confounders would be needed.
Inourstudy,theacetabularparametersweremeasured rela-tivetotheverticalplaneandnottotheAPP.Thetermsfunctional inclinationandanteversionarethereforeappropriate,sincethese measurementsvarywiththepositionofthepelvis[20].
Restoringfemoral-pelvic-spinalbalanceshouldbeamongthe goalsconsideredwhenplanningTHA.Althoughthefrequencyof prosthetichipdislocationhasdecreasedsincetheintroductionof large-diameterfemoralheadsanddual-mobilityacetabularcups
T.Masquefaetal./Orthopaedics&Traumatology:Surgery&Research101(2015)655–659 659
[31],theacetabularretroversioninducedbyPSOincreasestherisk ofposteriordislocationinpatientswithTHA.Severalauthorssuch asLafageet al.[32] and Boissière etal. [33] developed mathe-maticalformulasdesignedtopredictwhetherPSOwasneededto correctasagittalimbalance.WhenaneedforPSOispredicted,given theeffectsofPSOonacetabularversion,thehipsurgeonshould considertheseparameterswhen planningTHA and shouldgive preferencetoadual-mobilitycupinordertominimisetheriskof posteriordislocationafterPSO.Inturn,thespinalsurgeonshould takethepresenceofoneortwoprosthetichipsintoaccountwhen planningPSOtotreatpost-operativeflat-backsyndrome.
CuporientationbasedonthesaferangedefinedintheAPPby Lewinneketal.[34]remainsunchangedafterPSO.Thechangein acetabularorientationissignificantinthevertical(orfunctional) planebutnotintheAPP,whichistheplaneofreferenceusedfor navigationduringTHA.Todate,nostudieshaveaddressedthe clini-calconsequences(mostnotablytheriskofdislocation)offunctional acetabularretroversioninducedbyPSOinpatientswithahistory ofTHA.
5. Conclusion
PSO performed to treat post-operative flat-back syndrome inducesstatisticallysignificantacetabularretroversionand hori-zontalisation.Thesechangesshouldbetakenintoaccountwhen planningacetabularcuporientationduringTHA.
Nevertheless,todate,noproofexiststhatPSO-inducedchanges areassociatedwithclinicaleffects,mostnotablyinpatientswitha historyofTHA.
Disclosureofinterest
Theauthorsdeclarethattheyhavenoconflictsofinterest con-cerningthisarticle.
References
[1]DuboussetJ.Importancedelavertèbrepelviennedansl’équilibrerachidien. Applicationàlachirurgiedelacolonnevertébralechezl’enfantetl’adolescent. In:RocheF,editor.Recueildecongrès« pied,équilibreetrachis ».Paris; 1998.
[2]LeHuecJC,SaddikiR,FrankeJ,RigalJ,AunobleS.Equilibriumofthehuman bodyandthegravityline:thebasics.EurSpineJ2011;20(Suppl.5):558–63. [3]ObeidI,HaugerO,AunobleS,BourghliA,PelletN,VitalJM.Globalanalysis
ofsagittalspinalalignmentinmajordeformities:correlationbetweenlackof lumbarlordosisandflexionoftheknee.EurSpineJ2011;20(Suppl.5):681–5. [4]RoussoulyP,Pinheiro-FrancoJL.Biomechanicalanalysisofthespino-pelvic organization and adaptation in pathology. Eur Spine J 2011;20(Suppl. 5):609–18.
[5]JosephJrSA,MorenoAP,BrandoffJ,CasdenAC,KuflikP,NeuwirthMG.Sagittal planedeformityintheadultpatient.JAmAcadOrthopSurg2009;17:378–88. [6]RosePS,BridwellKH,LenkeLG,CronenGA,MulconreyDS,BuchowskiJM,etal. Roleofpelvicincidence,thoracickyphosis,andpatientfactorsonsagittalplane correctionfollowingpediclesubtractionosteotomy.Spine2009;34:785–91. [7]HovorkaI,RousseauP,BronsardN,ChalaliM,JuliaM,CarlesM,etal.[Extension
reserveofthehipinrelationtothespine:comparativestudyoftwo radio-graphicmethods].RevChirOrthopReparatriceApparMot2008;94:771–6. [8]LazennecJY,BrussonA,RousseauMA.Hip-spinerelationsandsagittalbalance
clinicalconsequences.EurSpineJ2011;20(Suppl.5):686–98.
[9]LazennecJY,BrussonA,FolinaisD,ZhangA,PourAE,RousseauMA.Measuring extensionofthelumbar-pelvic-femoralcomplexwiththeEOSsystem.EurJ OrthopSurgTraumatol2015.
[10]BlondelB,ParratteS,TropianoP,PaulyV,AubaniacJM,ArgensonJN.Pelvictilt measurementbeforeandaftertotalhiparthroplasty.OrthopTraumatolSurg Res2009;95:568–72.
[11]Ben-GalimP,Ben-GalimT,RandN,HaimA,HippJ,DekelS,etal.Hip-spine syndrome:theeffectoftotalhipreplacementsurgeryonlowbackpainin severeosteoarthritisofthehip.Spine2007;32:2099–102.
[12]OffierskiCM,MacNabI.Hip-spinesyndrome.Spine1983;8:316–21. [13]RadcliffKE,KeplerCK,HellmanM,RestrepoC,JungKA,VaccaroAR,etal.
Doesspinalalignmentinfluenceacetabularorientation:astudyofspinopelvic variablesandsagittalacetabularversion.OrthopSurg2014;6:15–22. [14]LegayeJ,Duval-BeaupereG,BarrauA,BoulayC,HecquetJ,MontignyJP,etal.
Relationshipbetweensacralpelvicincidenceandacetabularorientation.Hip Int2011;21:87–97.
[15]IllesT,SomoskeoyS.TheEOSimagingsystemanditsusesindailyorthopaedic practice.IntOrthop2012;36:1325–31.
[16]MonazzamS,AgasheM,HosalkarHS.Reliabilityofovercoverageparameters withvaryingmorphologicpincerfeatures:comparisonofEOS®and radiogra-phy.ClinOrthopRelatRes2013;471:2578–85.
[17]BittersohlB,FreitasJ,ZapsD,SchmitzMR,BomarJD,MuhamadAR,etal.EOS imagingofthehumanpelvis:reliability,validity,andcontrolledcomparison withradiography.JBoneJointSurgAm2013;95:e581–9.
[18]RousseauMA,BrussonA,LazennecJY.Assessmentoftheaxialrotationofthe pelviswiththeEOSimagingsystem:intra-andinter-observerreproducibility andaccuracystudy.EurJOrthopSurgTraumatol2013.
[19]LazennecJY,RiwanA,GravezF,RousseauMA,MoraN,GorinM,etal.Hipspine relationships:applicationtototalhiparthroplasty.HipInt2007;17(Suppl. 5):S91–104.
[20]PhilippotR,WegrzynJ,FarizonF,FessyMH.Pelvicbalanceinsagittaland Lewinnekreferenceplanesinthestanding,supineandsittingpositions.Orthop TraumatolSurgRes2009;95:70–6.
[21]MurrayDW.Thedefinitionandmeasurementofacetabularorientation.JBone JointSurgBr1993;75:228–32.
[22]LazennecJY,BoyerP,GorinM,CatonneY,RousseauMA.Acetabularanteversion withCTinsupine,simulatedstanding,andsittingpositionsinaTHApatient population.ClinOrthopRelatRes2011;469:1103–9.
[23]Lazennec JY, Rousseau MA, Rangel A, Gorin M, Belicourt C, Brusson A, etal.Pelvisandtotalhiparthroplastyacetabularcomponentorientationsin sittingandstandingpositions:measurementsreproductibilitywithEOS imag-ingsystemversusconventionalradiographies.OrthopTraumatolSurgRes 2011;97:373–80.
[24]LazennecJY,BrussonA,RousseauMA.Lumbar-pelvic-femoralbalanceon sit-tingandstandinglateralradiographs.OrthopTraumatolSurgRes2013;99(1 Suppl.):S87–103.
[25]ObeidI,BourghliA,VitalJM.Pediclesubtractionosteotomyforpostoperative flatbackandsagittalimbalance.EurSpineJ2012;21:1218–9.
[26]DebargeR,Demey G,RoussoulyP.Sagittal balanceanalysisafterpedicle subtractionosteotomyinankylosingspondylitis.EurSpineJ2011;20(Suppl. 5):619–25.
[27]RousseauMA,LazennecJY,TassinJL,FortD.Sagittalrebalancingofthepelvis andthethoracicspineafterpediclesubtractionosteotomyatthelumbarlevel. JSpinalDisordTech2014;27:166–73.
[28]McGraw KOWS. Forming inferences about some intraclass correlation coefficients.PsycholMethods1996.
[29]ShroutPE,FleissJL.Intraclasscorrelations:usesinassessingraterreliability. PsycholBull1979;86:420–8.
[30]McBride.Aproposalforstrength-of-agreementcriteriaforLin’sConcordance CorrelationCoefficient.NIWAClientReport;2005.
[31]DeMartinoI,TriantafyllopoulosGK,SculcoPK,SculcoTP.Dualmobilitycups intotalhiparthroplasty.WorldJOrthop2014;5:180–7.
[32]LafageV,SchwabF,PatelA,HawkinsonN,FarcyJP.Pelvictiltandtruncal incli-nation:twokeyradiographicparametersinthesettingofadultswithspinal deformity.Spine2009;34:E599–606.
[33]BoissiereL,BourghliA,VitalJM,GilleO,ObeidI.Thelumbarlordosisindex: anewratiotodetectspinalmalalignmentwith atherapeuticimpactfor sagittalbalancecorrectiondecisionsinadultscoliosissurgery.EurSpineJ 2013;22:1339–45.
[34]LewinnekGE,LewisJL,TarrR,CompereCL,ZimmermanJR.Dislocationsafter totalhip-replacementarthroplasties.JBoneJointSurgAm1978;60:217–20.