Sonographic Detection of Thyroid
Pyramidal Lobes Before Thyroid Surgery
A Prospective Single-Center Study
thyroid pyramidal lobe is an accessory lobe of the thyroid gland that is reported at various frequencies, ranging from 15% to 75%, mostly as observed in cadaver studies.1–6 The preoperative detection of a thyroid pyramidal lobe may be nec-essary because residual thyroid tissue can be left after total thy-roidectomy because of the limited surgical field.2 In particular, remnant thyroid tissue in a patient with papillary thyroid carcinoma can influence the outcome of radioisotope ablation because the radioisotope preferentially targets remnant normal thyroid tissue over malignant thyroid cells.1,7
Recently, 2 studies in patients and healthy populations examin-ing the prevalence or size of thyroid pyramidal lobes usexamin-ing computed tomography (CT) have been reported.8,9However, CT has a radia-tion hazard, and its use is limited in patients with thyroid malignancy. Unlike CT, sonography has no radiation hazard and has been estab-lished as the first choice in the diagnosis of thyroid lesions. To the Dong Wook Kim, MD, Tae Kwun Ha, MD, Ha Kyoung Park, MD, Taewoo Kang, MD
Received May 2, 2013, from the Departments of Radiology (D.W.K.) and General Surgery (T.K.H., H.K.P.), Busan Paik Hospital, Inje University College of Medicine, Busan, Korea; and Depart-ment of Surgery, Busan Cancer Center, Pusan National University Hospital, Pusan National University College of Medicine, Busan, Korea (T.K.). Revision requested May 20, 2013. Revised manuscript accepted for publication June 1, 2013. This work was supported by the 2013 Inje University research grant.
Address correspondence to Tae Kwun Ha, MD, Department of General Surgery, Busan Paik Hospital, Inje University College of Medicine, 633-165 Gaegeum-dong, Busanjin-gu, Busan 614-734, Korea.
E-mail: [email protected] Abbreviations
CT, computed tomography
A
Objectives—This study aimed to assess the rate of preoperative sonographic detection of thyroid pyramidal lobes with subsequent surgical findings as the reference standard.
Methods—From January 2013 to March 2013, a single radiologist prospectively performed thyroid sonography to detect thyroid pyramidal lobes in consecutive patients who were scheduled for thyroid surgery on the same day. The location, anteroposterior and trans-verse diameters, length, and location of the upper end of each thyroid pyramidal lobe and its separation or contiguity with the main thyroid gland were investigated by thyroid sonography and surgery.
Results—The types of thyroid surgery included total thyroidectomy (n = 85), subtotal thyroidectomy (n = 4), and hemithyroidectomy (n = 43). The surgical incidence of thyroid pyramidal lobes was 59.8% (79 of 132), and the sensitivity, specificity, positive and negative predictive values, and accuracy of sonography for detection of thyroid pyramidal lobes were 81.0%, 79.2%, 85.3%, 73.7%, and 80.3%, respectively. The mean values for the anteroposterior diameter, transverse diameter, and length of the 79 thyroid pyramidal lobes at surgery were 2.2, 6.2, and 26.5 mm, respectively, but these meas-urements did not show statistically significant correlations with the sonographic detec-tion rate of thyroid pyramidal lobes.
Conclusions—Our study indicates that thyroid sonography may be helpful for identi-fying the presence and location of thyroid pyramidal lobes.
Key Words—general ultrasound; pyramidal lobe; sonography; surgery; thyroid
best of our knowledge, no study using thyroid sonography for detection of thyroid pyramidal lobes has been published. Therefore, the purpose of this study was to assess the rate of preoperative sonographic detection of thyroid pyramidal lobes using subsequent surgical findings as the reference standard in patients undergoing thyroidectomy.
Materials and Methods
PatientsFrom January 2013 to March 2013, consecutive patients who were scheduled for thyroid surgery on the same day underwent prospective preoperative thyroid sonography performed by a single radiologist to detect thyroid pyramidal lobes. Exclusion criteria for this study were previous thyroidectomy or other neck surgery, recent neck trauma, inflammatory neck lesions, and patient preference. Ultimately, 132 patients (115 women and 17 men; age range, 23–86 years; mean age ± SD, 47.1 ± 10.8 years) were included in this study. Patients had previous neck CT for the following reasons: suspicious thyroid malignancy at cytologic examination (n = 122), indeterminate cytologic findings (n = 2), and patient requests despite benign cyto-logic findings (n = 8). This study was approved by the Institutional Review Board before patient selection began (Institutional Review Board approval number 12-171), and written informed consent was provided by the study patients.
Thyroid Sonography
Thyroid sonography was performed with a high-resolution ultrasound instrument (iU22; Philips Healthcare, Andover, MA) equipped with a 5–12-MHz linear probe. On real-time sonography, a thyroid pyramidal lobe was defined as follows: (1) a longitudinally arranged accessory thyroid lobe protruding from the upper margin of the isthmus or the medial aspect of the right or left thyroid lobe, regardless of its contiguity with the main thyroid gland; and (2) the same echogenicity and vascularity as the main thyroid gland on grayscale and color Doppler images. Short pyramidal lobes less than 5 mm in length were excluded.
The location, anteroposterior and transverse diameters, length, position of the upper end, and separation or conti-guity of the thyroid pyramidal lobe with the main thyroid gland were recorded. The lobe location was classified in
lobe were measured directly. The pyramidal lobe was also classified into 1 of 4 categories in accordance with the loca-tion (or level) of its upper end: tongue base, hyoid bone, thy-rohyoid membrane, or thyroid cartilage. Separation of the pyramidal lobe was defined in the presence of a lack of com-munication from the main thyroid gland to the lobe. Thyroid Surgery
Thyroid surgery with a low-collar incision was performed after thyroid sonography by 2 independent surgeons (approximately 6700 thyroid surgeries for 34 years and 500 thyroid surgeries for 4 years, respectively), who were blinded to the thyroid sonographic findings. The surgeons directly recorded the locations, anteroposterior and transverse diameters, lengths, and positions of the upper ends of thy-roid pyramidal lobes identified at surgery and noted the separation or continuity of the lobes with the main thyroid gland. As with the sonographic evaluations, the antero-posterior diameter of the pyramidal lobe was calculated as the average of measurements from 3 sites (largest, smallest, and middle), whereas the largest transverse diameter and length were measured in the surgical field. As for thyroid sonography, short pyramidal lobes less than 5 mm in length were excluded.
Statistical Analysis
A conclusive finding of a thyroid pyramidal lobe was deter-mined on the basis of surgical observations, and diagnostic indices were calculated for sonographic diagnosis. The dif-ferences in the incidence of thyroid pyramidal lobes accord-ing to sex and age were evaluated by χ2and Student ttests, and differences in sonographic results for pyramidal lobes according to the anteroposterior diameter, transverse diameter, and length were compared by logistic regression analysis. The correspondence between thyroid sonogra-phy for detection of a thyroid pyramidal lobe and surgical findings was analyzed by a Fisher exact test, Wilcoxon rank sum test, or χ2test according to each item. Statistical analysis was performed with SPSS version 17.0.1 software (IBM Corporation, Armonk, NY). P< .05 was considered statistically significant.
Results
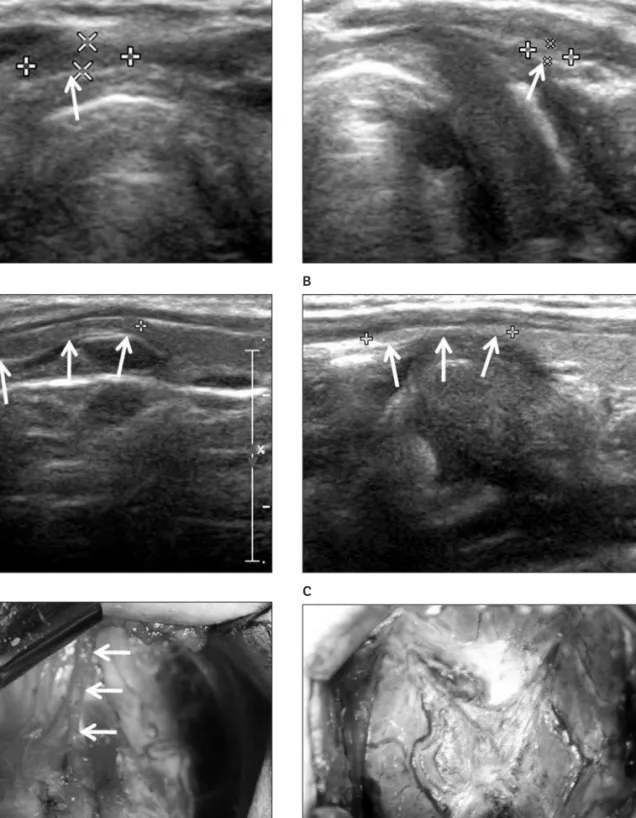
Figure 1. True-positive case: 38-year-old man with a right pyramidal lobe detected on thyroid sonography and at surgery. Transverse (A) and longitudinal (B) grayscale sonograms show the lobe (arrows; 1.6 × 5.7 × 15.4 mm). The lobe (C) was observed at thyroid surgery (arrows; 1.3 × 3.4 × 15.0 mm).
A
B
C
Figure 2. False-positive case: 46-year-old woman with a left pyramidal lobe on thyroid sonography but no lobe at surgery. Transverse (A) and longitudinal (B) grayscale sonograms show a structure that appears as a small lobe (arrows; 1.1 × 2.8 × 13.0 mm). At thyroid surgery (C), no lobe was observed.
A
B
diameter, transverse diameter, and length of actual pyramidal lobes at surgery were 2.2 ± 0.7, 6.2 ± 2.6, and 26.5 ± 11.4 mm, respectively. The numbers of true-positive, false-positive, true-negative, and false-negative diagnoses by thyroid sonography were 64, 11, 42, and 15, respectively, and the diagnostic indices for sonographic diagnosis are shown in Table 1. There was no statistically significant difference in the sonographic detection rate of thyroid pyramidal lobes according to sex (P= .9264, χ2test), but there was a statistically significant difference in the sono-graphic detection rate of lobes according to age (P= .0041, Student ttest); the sonographic detection rate decreased with increasing age.
The rates of false-positive and -negative findings by thyroid sonography were 11 (8.3%) and 15 (11.4%) of 132 cases, respectively. The mean values for the anteroposterior diameter, transverse diameter, and length of the thyroid pyramidal lobes in the false-positive and -negative cases were 1.7 ± 0.59 and 2.0 ± 0.6, 5.8 ± 2.0 and 4.3 ± 1.8, and 25.8 ± 10.6 and 31.7 ± 9.8 mm, respectively. For the 64 true-positive cases (57 women and 7 men; age range, 30– 64 years; mean age, 45.0 ± 8.3 years), correspondence between thyroid sonographic and surgical findings for detection of thyroid pyramidal lobes was evaluated accord-ing to the location, anteroposterior diameter, transverse diameter, length, and upper end of the lobe and its separa-tion or contiguity with the main thyroid gland (Table 2). There were statistically significant differences in the antero-posterior diameter (P= .0035, Wilcoxon rank sum test), transverse diameter (P= .0072, Wilcoxon rank sum test), and upper end (P= .0003, Wilcoxon rank sum test) of the lobes between thyroid sonographic and surgical findings. However, by logistic regression analysis, the anteroposterior diameter (P= .3665), transverse diameter (P= .7717), and length (P= .9259) of the lobes were not statistically corre-lated with the sonographic findings.
Table 1. Diagnostic Indices for Sonographic Diagnosis of Thyroid Pyramidal Lobes
Parameter Value
Sensitivity, n (%) 64/79 (81.0)
Specificity, n (%) 42/53 (79.2)
PPV, n (%) 64/75 (85.3)
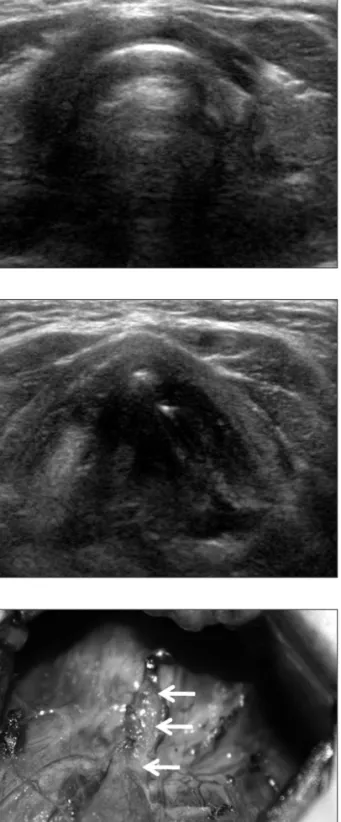
Figure 3. False-negative case: 52-year-old woman with no pyramidal lobe on thyroid sonography but a midline pyramidal lobe at surgery. Transverse grayscale sonograms at the lower (A) and upper (B) thyroid cartilage levels did not indicate a lobe. At thyroid surgery (C), a thin mid-line pyramidal lobe was observed (arrows; 1.1 × 4.8 × 16.5 mm).
A
B
Discussion
A thyroid pyramidal lobe is an accessory lobe of the thyroid gland and an embryologic remnant of the thyroglossal duct that is formed during the descent of the thyroid diverticulum from the floor of the pharynx.10,11Based on studies using a limited number of cadavers, differing values for the preva-lence of pyramidal lobes have been reported, ranging from 15% to 75%.1–6Recent single-center and multicenter stud-ies focusing on the detection of thyroid pyramidal lobes by CT indicated that this variant is present in 41.3% (135 of 327) and 44.6% (981 of 2200) of study patients, respec-tively, and the results suggest that neck CT may be useful for detecting thyroid pyramidal lobes.8,9In this study, the prevalence rates for thyroid pyramidal lobes on sonogra-phy and at surgery were 56.8% (75 of 132) and 59.8% (79 of 132), respectively. The reason for this high prevalence is not clear, but we believe that a selection bias or the use of different diagnostic tools may have been a factor.
In this study, thyroid pyramidal lobes were found at surgery in various sizes and locations and at various levels. The lengths of the lobes assessed by thyroid sonography were similar to the surgical findings, but thyroid sonography tended to underestimate the anteroposterior and transverse diameters of the lobes compared with the actual values. We believe that this difference may have originated from a measurement bias, and in the 64 true-positive cases, thyroid sonographic and surgical findings showed corre-spondence in the lengths of the lobes, which ranged from 7.9 to 49.1 and 7.0 to 55.2 mm, respectively. On the other hand, there was a statistically significant difference between thyroid sonographic and surgical findings for the levels of the lobes, but it was common for sonographic reports to indicate lower levels than surgical findings, which may be related to the limited sonic window in the neck.
Regarding the rate of sonographic detection of thyroid pyramidal lobes by age and sex, this study showed a statis-tically significant difference for age only. This result corre-sponds to the fact that humans show a progressive decrease in the volume of the thyroid gland and thyroid pyramidal lobe with aging. The findings might suggest that it is pos-sible that the larger the anteroposterior diameter of a thyroid pyramidal lobe, the better the sonographic lobe detection rate, although in this study, the anteroposterior diameters of 79 lobes (mean, 2.2 mm) showed no statisti-cally significant correlation with the sonographic detection rate. Although the reason for this result is not clear, we believe that when the anteroposterior diameter of a thyroid pyramidal lobe is less than 3 mm, it may not influence the sonographic detection rate as strongly as the echogenicity, longitudinal arrangement, and contiguity will.
Among 132 cases, the number of false-positive and -negative cases on thyroid sonography were 11 (8.3%) and 15 (11.4%), respectively, and the mean anteroposterior diam-eters of the false-positive and -negative nodes were 1.7 and 2.0 mm, respectively. The reason for these findings is not fully understood, but a possible explanation is the limited sonographic differentiation of thyroid pyramidal lobes from longitudinally arranged small muscle fibers, fibrotic fatty tissues, or other structures. Because of this factor, we also believe that the thinner a thyroid pyramidal lobe is, the worse the sonographic detection rate will be.
This study had several limitations. It was a single-center study in which all sonographic examinations were per-formed by a single radiologist, with the confirmative diag-nosis of a thyroid pyramidal lobe made independently by 2 surgeons. Large-scale multicenter studies are recom-mended. Second, there were no patients younger than 22 years included in the study. Finally, pathologic results for the thyroid pyramidal lobe were not assessed.
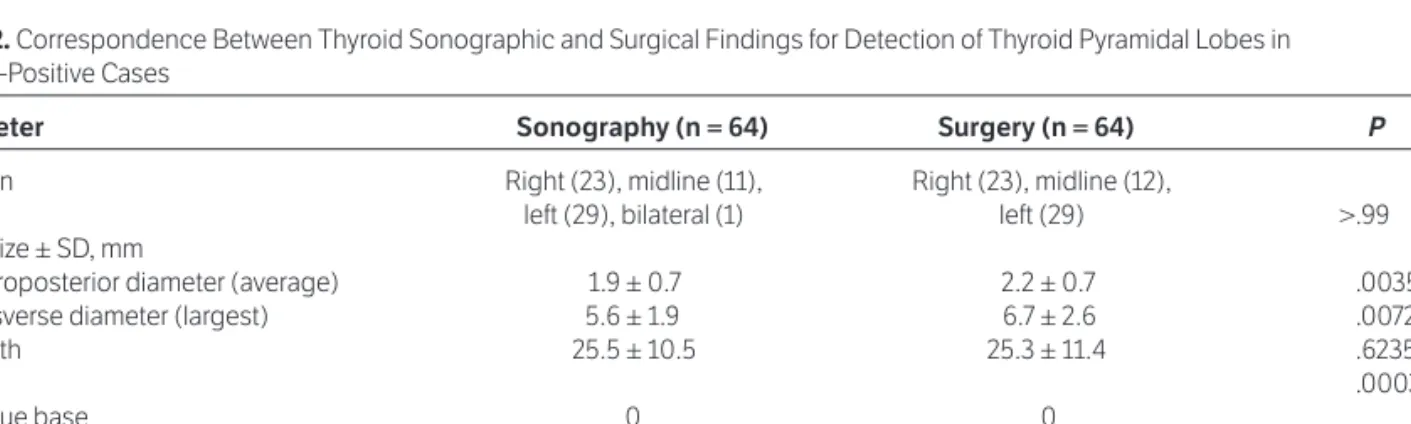
Table 2. Correspondence Between Thyroid Sonographic and Surgical Findings for Detection of Thyroid Pyramidal Lobes in 64 True-Positive Cases
Parameter Sonography (n = 64) Surgery (n = 64) P
Location Right (23), midline (11), Right (23), midline (12),
left (29), bilateral (1) left (29) >.99
Mean size ± SD, mm
Anteroposterior diameter (average) 1.9 ± 0.7 2.2 ± 0.7 .0035
Transverse diameter (largest) 5.6 ± 1.9 6.7 ± 2.6 .0072
Length 25.5 ± 10.5 25.3 ± 11.4 .6235 Level .0003 Tongue base 0 0 Hyoid bone 6 12 Thyrohyoid membrane 5 20 Thyroid cartilage 53 32 Separation 4 5 <.99
In conclusion, our study indicates that thyroid sonog-raphy may be helpful for identifying the presence and loca-tion of thyroid pyramidal lobes.
References
1. Marshall CF. Variations in the form of the thyroid gland in man. J Anat
1895; 29:234–239.
2. Braun EM, Windisch G, Wolf G, Hausleitner L, Anderhuber F. The pyramidal lobe: clinical anatomy and its importance in thyroid surgery.
Surg Radiol Anat2007; 29:21–27.
3. Sultana SZ, Mannan S, Ahmed MS, Rahman MM, Khan MK, Khalil M. An anatomical study on pyramidal lobe of thyroid gland in Bangladeshi people. Mymensingh Med J2008; 17:8–13.
4. Joshi SD, Joshi SS, Daimi SR, Athavale SA. The thyroid gland and its vari-ations: a cadveric study. Folia Morphol (Warsz)2010; 69:47–50. 5. Ozgur Z, Celik S, Govsa F, Ozgur T. Anatomical and surgical aspects of
the lobes of the thyroid glands. Eur Arch Otorhinolaryngol2011; 268:1357– 1363.
6. Prakash, Rajini T, Ramachandran A, Savalgi GB, Venkata SP, Mokhasi V. Variations in the anatomy of the thyroid gland: clinical implications of a cadaver study. Anat Sci Int2012; 87:45–49.
7. Pacini F, Schlumberger M, Harmer C, et al. Post-surgical use of radioio-dine (131I) in patients with papillary and follicular thyroid cancer and the issue of remnant ablation: a consensus report. Eur J Endocrinol 2005; 153:651–659.
8. Park JY, Kim DW, Park JS, Kang T, Kim YW. The prevalence and fea-tures of thyroid pyramidal lobes as assessed by computed tomography.
Thyroid2012; 22:173–177.
9. Kim DW, Jung SL, Baek JH, et al. The prevalence and features of thyroid pyramidal lobe, accessory thyroid, and ectopic thyroid as assessed by com-puted tomography: a multicenter study. Thyroid 2013; 23:84–91. 10. O’Rahilly R, Müller F. Human Embryology and Teratology. New York, NY:
Wiley-Liss; 1992.
11. Moore KL, Persaud TVN. The developing human. In: Moore KL, Dalley AF, Agur AMR (eds). Clinically Oriented Embryology.2nd ed. Philadelphia, PA: WB Saunders Co; 1993:200–203.