Maria Ganeva
1, A–F, Tanya Gancheva
2, B–F, Jeni Troeva
2, B, C,
Nataliya Kiriyak
2, B, C, Evgenya Hristakieva
2, C, EClinical Relevance of Drug-Drug Interactions
in Hospitalized Dermatology Patients*
Kliniczne znaczenie interakcji lekowych
u hospitalizowanych pacjentów leczonych dermatologicznie
1 Section of Pharmacology and Clinical Pharmacology, Faculty of Medicine, Thracian University, Stara Zagora, Bulgaria 2 Clinic of Dermatology and Venereology, University Hospital, Stara Zagora, Bulgaria
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Background. Potential drug-drug interactions (DDIs) are known to be a risk factor for the development of adverse drug reactions (ADRs). Data on the occurrence of ADRs related to DDIs is scarce and comes from different groups of patients.
Objectives. The aim of the study was to evaluate the frequency, nature and determinants of potential DDIs in hospitalized dermatology patients and assess their contribution for the development of ADRs.
Material andMethods. A prospective observational study comprising all consecutive inpatients admitted to the Clinic of Dermatology and Venereology, University Hospital, Stara Zagora for the period March 2009 – August 2011 was carried out.Systemic medication was screened for potential DDIs using an electronic drug interactions checker. DDIs were then verified with Stockley’s Drug Interactions and divided into “clinically important” and “clinically unimportant”. ADRs were classified by clinical manifestation, type and severity. Causality was scored according to Naranjo et al. (1981).
Results. The study included 674 patients, 513 (76.1%) of them with established comorbidities. Totally, 504 poten-tial DDIs were identified (441 “clinically important” and 63 “clinically unimportant”) in 236 patients. Hypotension was the most common expected clinical presentation of the potential DDIs. The strongest predictor for the devel-opment of DDIs was the number of systemic drugs (OR 2.25, 95% CI 1.97–2.58). Overall 43 ADRs were recorded, 53.5% “type B” and 46.5% “type A” reactions, most commonly with cutaneous and cardiovascular manifestations. The development of ADRs was attributed to 13 DDIs (2.6% of all detected potential DDIs) in 10 of these cases (23.25%).
Conclusions. Potential DDIs were frequent in hospitalized dermatology patients. The drug groups most com-monly involved were cardiovascular drugs. The proportion of DDIs associated with the occurrence of ADRs was relatively low, but close monitoring of patients on multiple drug regimens is essential because these reactions may be severe (Adv Clin Exp Med 2013, 22, 4, 555–563).
Key words: drug-drug interaction,adversedrug reaction, hospital, dermatology.
Streszczenie
Wprowadzenie. Potencjalne interakcje lekowe (DDIs) są znanym czynnikiem ryzyka rozwoju działań niepożą-danych leku (ADR). Dane na temat występowania działań niepożąniepożą-danych związanych z DDIs są ograniczone, a pochodzą z różnych grup pacjentów.
Cel pracy. Ocena częstości występowania, rodzaju i wyznaczników potencjalnych DDIs u hospitalizowanych pacjentów leczonych dermatologicznie oraz ocena ich wkładu do rozwoju działań niepożądanych leku.
Adv Clin Exp Med 2013, 22, 4, 555–563 ISSN 1899–5276
ORIGINAl PAPERS
© Copyright by Wroclaw Medical University
Drug-drug interactions (DDIs) are considered to be an important risk factor in the development of adverse drug reactions (ADRs) [1, 2]. The aging of the population, polymorbidity and polypharma-cy, and the introduction of new drugs are all as-sociated with a high probability of development of DDIs. The clinical outcome of DDIs may be either increased risk of adverse effects/toxicity or loss of efficacy. Since the clinical manifestation of DDIs is not always present they are often referred to as po-tential DDIs. A study of ADRs from the UK estimat-ed that 16.6% of ADRs leading to hospital admis-sion were associated with DDIs [3]. Although other studies have reported even higher proportions of DDIs underlying the development of ADRs, some authors question the clinical relevance of poten-tial DDIs [4, 5]. Data suggests that certain popula-tion groups like the elderly, patients from intensive care units and oncology patients are at high risk of drug-related morbidity due to DDIs [6, 7].
The recognition and management of potential DDIs is a matter of good prescribing practice and clinical care for which the use of drug informa-tion services is essential. Potential DDIs are usu-ally detected with various computerized screen-ing programs displayscreen-ing different sensitivity and specificity compared to the gold standard Stock-ley’s Drug Interactions, as a study from Switzer-land showed [8]. Thus the results from various studies on DDIs are difficult to be compared and interpreted. It is possible that many DDIs remain under-recognized [9].
Drug groups of particular significance for der-matologists considering their potential for DDIs are “general antiinfectives” and “antihistamines” [10]. A preliminary study of adverse DDIs in derma-tology patients showed that 25.5% of the inves-tigated cohort had a potential adverse DDI and
cardiovascular drugs were prevalently involved in these interactions [11].
The aim of the present study was to evaluate the frequency, nature and determinants of poten-tial DDIs in hospitalized dermatology patients and assess their contribution for the development of ADRs.
Material and Methods
Patient Population
The investigation is a part of a prospective pharmacovigilance study carried out among pa-tients admitted to the Clinic of Dermatology and Venereology at the University Hospital in Stara Za-gora. All consecutive adult and pediatric inpatients admitted to the Clinic for the period March 2009 – August 2011 were screened for potential DDIs. Information on systemic medication was collect-ed on the day of admission and the mcollect-edical charts were followed for further changes during the pe-riod of hospitalization. For each patient, addition-ally the following data was recorded: demograph-ic characteristdemograph-ics, primary diagnosis, concomitant diseases, history of previous ADRs, failure of ex-cretory organs. The International Classification of Diseases, version 10 (ICD-10) and the Anatomical Therapeutic Chemical (ATC) classification system were used to codify data [12, 13].
All ADRs including those resulting from DDIs were recorded in a structured form containing further information on drug history covering the last three months preceding hospitalization, clin-ical description of the adverse event, laboratory tests and reviews of consultants. The study was ap-proved by the local ethics committee.
Materiał i metody. Przeprowadzono prospektywne badanie obserwacyjne obejmujące wszystkich kolejnych pacjentów przyjętych do Kliniki Dermatologii i Wenerologii, Szpitala Uniwersyteckiego w Starej Zagorze w okresie marzec 2009 – listopad 2011. Podawanie leków układowych monitorowano pod kątem potencjalnych DDIs za pomocą elektronicznego urządzenia do sprawdzania interakcji. DDIs były następnie weryfikowane na podstawie „Stockley’s Drug Interactions” i podzielone na „klinicznie istotne” i „klinicznie nieistotne”. Działania niepożądane zostały sklasyfikowane według objawów klinicznych, rodzaju i stopnia nasilenia. Przyczynowość oceniano według Naranjo et al. (1981).
Wyniki. Do badania włączono 674 pacjentów, 513 (76,1%) z nich cierpiało na choroby współistniejące. W sumie zidentyfikowano 504 potencjalne DDIs (441 „klinicznie istotnych” i 63 „klinicznie nieistotne”) u 236 pacjentów. Niedociśnienie tętnicze było najczęściej oczekiwanym klinicznym objawem potencjalnych DDIs. Najsilniejszym predyktorem rozwoju DDIs była liczba leków układowych (OR 2,25, 95% CI 1.97–2.58). Ogólnie odnotowano 43 działania niepożądane leku; 53,5% reakcji „typu B” i 46,5% reakcji „typu A”, najczęściej były to objawy skórne i pochodzące z układu krążenia. Rozwój działań niepożądanych leku był związany z 13 DDIs (2,6% wszystkich wykrytych potencjalnych DDIs) w 10 przypadkach (23,25%).
Wnioski. Potencjalne DDIs występowały często u hospitalizowanych pacjentów leczonych dermatologicznie. Grupa leków, które najczęściej je wywoływały to leki sercowo-naczyniowe. Odsetek DDIs związanych z występowaniem działań niepożądanych był stosunkowo mały, ale ścisłe monitorowanie pacjentów poddanych wielolekowej terapii jest niezbędne, ponieważ reakcje te mogą być ciężkie (Adv Clin Exp Med 2013, 22, 4, 555–563).
Definition of Drug-Drug
Interactions
DDIs were defined according to Ritter et al., as the modification of the action of one drug by another as a result of one or more of three differ-ent kinds of mechanisms: pharmaceutical, phar-macodynamic and pharmacokinetic[1]. Using the ePocrates® drug interactions checker, DDIs were classified into the following categories: “therapeu-tic advantage”, “caution advised”, “monitor/mod-ify therapy”, “avoid/use alternative” according to clinical management [14]. For each interaction, the DDI checker lists the expected or possible ef-fects of the drug combination, and the proposed mechanism of the interaction. DDIs were then ver-ified using the hard copy of Stockley’s Drug Inter-actions and classified into two groups: “clinical-ly important” and “clinical“clinical-ly unimportant”, when that was explicitly stated [15]. Drug preparations and DDIs not found in ePocrates® were added. DDIs not found in Stockley’s Drug Interactions were excluded.
Definition of Adverse Drug
Reactions
ADRs were defined according to the WHO [16]. Patients with non-skin ADRs recognized dur-ing hospitalization in the department were con-sulted by the respective specialists. The ADRs were classified by clinical manifestation using WHO-ART Adverse Reaction Terminology and by type as “type A” if related to the pharmacolog-ical properties of the suspected drug, and “type B” if otherwise[17, 18]. According to their severity, ADRs were assessed as “severe” (life-threatening or serious condition with progressive organ dys-function), “moderate” (fair condition, transitory organ dysfunction) and “mild” (good condition with minor/no organ dysfunction). The relation-ship between the drug and the reaction was scored as “definite”, “probable”, “possible” and “doubtful” following the method of Naranjo et al. [19].
Statistical Analysis
Continuous variables were tested for normal-ity using the Kolmogorov-Smirnov test. Because the study values were not normally distributed, the results were presented as median and interquartile range (25th–75th percentile). The non-parametric Mann-Whitney U test was applied to determine be-tween-group differences. logistic regression analy-sis was used to evaluate the relationship between the occurrence of DDIs and the factors age, female
sex, maximum number of systemic drugs used by the patients and the length of hospital stay. Ad-justment for possible confounders was made using multiple logistic regression. A value of p < 0.05 was considered statistically significant. Analyses were performed using SPSS for Windows version 9.0.
Results
Patient Characteristics
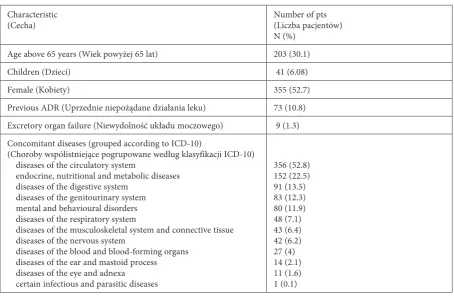
A total of 674 patients, 355 female and 319 male, with an age range 1–90 years (medi-an 54, interquartile r(medi-ange: 39–67) were included in the study. The demographic characteristics and the clinico-pharmacological risk factors are shown in Table 1.
The main causes for hospitalization by prima-ry diagnosis, coded by the ICD version 10, were infectious dermatoses “l00–l08” in 217 patients (32.2%) and eczema/dermatitis “l20–l30” in 200 patients (29.7%). Concomitant disease states were detected in 513 cases – 76.1% of the total study population (Table 1). Cardiovascular dis-eases were diagnosed in 356 patients (52.8%) and were the most frequent type of concomitant dis-eases. Cardiovascular drugs (ATC code C) and an-tihistamines (ATC code R) were the groups most commonly used in the study population (Table 2).
Hospital stay in the examined cohort of pa-tients was median 8 days (interquartile range: 7–10 days).
Drug-Drug Interactions
Initial online screening for DDIs with the ePocrates® drug interactions checker revealed 496 DDIs in 226 patients (Table 3). The prevalent type were DDIs which required careful monitoring and modifications in drug regimens – 304 DDIs (61.3%) in 152 patients. DDIs from the category “avoid/use alternative” numbered 59 (11.9%) and from the category “caution advised”, 112 (22.6%). More than one DDI was detected in 119 patients, the maximum number per patient being 9.
Таble 1. Characteristics of the patient population
Tabela 1. Charakterystyka pacjentów
Characteristic
(Cecha) Number of pts (liczba pacjentów) N (%)
Age above 65 years (Wiek powyżej 65 lat) 203 (30.1)
Children (Dzieci) 41 (6.08)
Female (Kobiety) 355 (52.7)
Previous ADR (Uprzednie niepożądane działania leku) 73 (10.8) Excretory organ failure (Niewydolność układu moczowego) 9 (1.3) Concomitant diseases (grouped according to ICD-10)
(Choroby współistniejące pogrupowane według klasyfikacji ICD-10) diseases of the circulatory system
endocrine, nutritional and metabolic diseases diseases of the digestive system
diseases of the genitourinary system mental and behavioural disorders diseases of the respiratory system
diseases of the musculoskeletal system and connective tissue diseases of the nervous system
diseases of the blood and blood-forming organs diseases of the ear and mastoid process diseases of the eye and adnexa certain infectious and parasitic diseases
356 (52.8) 152 (22.5) 91 (13.5) 83 (12.3) 80 (11.9) 48 (7.1) 43 (6.4) 42 (6.2) 27 (4) 14 (2.1) 11 (1.6) 1 (0.1)
pts – patients; % – percent of total; ADR – adverse drug reaction; ICD-10 – International Classification of Diseases, version 10. pts – pacjent; % – procent wszystkich; ADR – niepożądane działanie leku, ICD-10 – Międzynarodowa Klasyfikacja Chorób, wersja 10.
Table 2. Systemic therapy according to the Anatomical Therapeutic Chemical (ATC) classification
Tabela 2. leczenie układowe według klasyfikacji „Anatomiczno-terapeutycznej związków chemicznych” (ATC)
ATC code
(Kod ATC) Main drug group (Główna grupa leków) N of pts (liczba pacjentów)
A alimentary tract and metabolism 150
B blood and blood forming organs 242
C cardiovascular system 324
G genitourinary system and sex hormones 5 H systemic hormonal preparations, excl. sex hormones and insulins 80
J anti-infectives for systemic use 311
l antineoplastic and immunomodulating agents 1
M musculo-skeletal system 24
N nervous system 178
R respiratory system 321
S sensory organs 1
DDI was present in 125 patients. The positive pre-dictive value of the ePocrates® drug interactions checker was estimated as 0.89.
Pharmacological groups like diuretics (187 DDIs), angiotensin-converting enzyme (ACE)-inhibitors (90 DDIs) and antidiabetic agents (80 DDIs) were commonly involved in DDIs (Table 4).
The prevalent clinical outcome of the detect-ed DDIs was increasdetect-ed toxicity or risk of adverse
effects, and only 73 DDIs (14.5%) of all 504 were associated with a possible decrease in drug effica-cy due to the antagonistic effects of the interacting drugs or pharmacokinetic mechanisms. Therapeu-tic advantage resulting from enhanced bactericid-al activity in the combinations of penicillins and aminoglycosides was the only beneficial DDI with no potential of adverse effects found in this study (14 DDIs or 2.8%). Risk of hypotension due to a combination of ACE-inhibitors or angiotensin2
-Table 3. Distribution of drug-drug interactions by type (ePocrates® and Stockley’s Drug Interactions)
Tabela 3. Rozkład interakcji lekowych według rodzaju (ePocrates®i Stockley’s Drug Interactions)
ePocrates® Stockley
N
(%) therapeutic advantage caution advised monitor/modify avoid/usealternative total clinically impor-tant clinically unimportant total Pts 21 (9.3%) 93 (41.2%) 152 (67.3%) 50 (22.1%) 226* 225 (95.3%) 54 (22.8%) 236** DDIs 21 (4.2%) 112 (22.6%) 304 (61.3%) 59 (11.9%) 496 379+62 (87.5%) 63 (12.5%) 504
pts – patients; *70 pts had more than 1 type of DDI (ePocrates); **43 pts had more than 1 type of DDI (Stockley’s). pts – pacjenci; * 70 pkt miał więcej niż 1 rodzaj DDI (ePocrates); ** 43 pkt miał więcej niż 1 rodzaj DDI (Stockley’s).
Table 4. Most common clinically important drug-drug interactions in hospitalized dermatology patients
Tabela 4. Najczęstsze klinicznie istotne interakcje lekowych u hospitalizowanych pacjentów leczonych dermatologicznie
I. General DDIs (Ogólne DDIs)
Drug groups (Grupy leków) DDIs (N) Potential effects (Potencjalne działania) ACE-inhibitors + Diuretics, thiazides/loop diuretics 65 first-dose hypotension
Antipsychotics + Benzodiazepines and related drugs 27 additive CNS depressant effects ARBs + Diuretics, thiazides 26 symptomatic hypotension Coumarins + Antibacterials 18 increased risk of bleeding Beta-blockers + Digoxin and related drugs 17 potential for additive bradycardia Digoxin and related drugs + Diuretics,
potassium-depleting 16 digitalis toxicity
Beta-blockers + Clonidine and related drugs 15 worsening the rebound hypertension following clonidine withdrawal, bradycardia
Penicillins + Aminoglycosides 14 enhanced bactericidal activity Antidiabetics + Diuretics, thiazides 12 impaired control of diabetes Thiazides + loop diuretics 12 hypokalemia, hypotension
Clonidine + Calcium-channel blockers 11 additive effects such as bradycardia and AV block
II. Dermatologic DDIs (Dermatologiczne DDIs)
Drug groups (Grupy leków) DDIs (N) Potential effects (Potencjalne działania) Antihistamines + Benzodiazepines and related drugs 16 sedation, additive CNS depressant effects Antihistamines + Antihistamines 15 additive CNS depressant effects
ACE – angiotensin-converting enzyme; ARBs – angiotensin2-receptor-blockers.
receptor-blockers (ARBs) plus diuretics was the most frequently encountered potential effect of DDIs in the study population.
Pharmacodynamic mechanisms were involved in 410 of the detected DDIs (81.35 %), pharmaco-kinetic in 49 DDIs (9.72%) and the rest were not well understood (e.g. increased effects of anticoag-ulants when combined with certain antibacterials, hypoglycemia following the combination of qui-nolones and antidiabetics).
Elderly patients (above 65 years) took a high-er numbhigh-er of drugs (median 5, inthigh-erquartile range: 4.0–7.0) than younger patients (median 3, inter-quartile range: 2.0 – 5.0), p = 0.0001. Patients with DDIs received significantly (p = 0.0001) more drugs (median 6, interquartile range: 5.0–8.0) than patients without DDIs (median 2, interquartile range: 1.0–4.0).
The logistic regression analysis showed that the development of DDIs was significantly associ-ated with a higher number of drugs (adjusted OR 2.23, 95% CI 1.96–2.55) and old age (adjusted OR 1.02, 95% CI 1.01–1.04). Female sex (adjusted OR 0.8, 95% CI 0.51–1.25) and the length of hospital stay (adjusted OR 0.99, 95% CI 0.89–1.09) were not found to be predictive of the occurrence of DDIs.
Adverse Drug Reactions
For the study period, 43 ADRs were recorded in 42 patients. The distribution of ADRs accord-ing to ADR type revealed 23 (53.5%) “type B” reac-tions and 20 (46.5%) “type A” reacreac-tions. Severe re-actions numbered 3, moderate 33, and mild 7. The causal relationship between the drug and the reac-tion were scored as „possible” in 24 ADRs and as „probable” in 19 ADRs.
Cutaneous ADRs (24 ADRs) presented with a variety of clinical manifestations, the prevalent clinical patterns being exanthematous and urti-carial. Cardiovascular ADRs (7ADRs) were in all cases hypotonia. Resistance mechanism disorders (3ADRs) were detected in patients with microbi-ological evidence for mucocutaneous or intestinal candidiasis after treatment with antibiotics or glu-cocorticosteroids. There were few cases of urinary system disorders, metabolic and nutritional disor-ders, vision disordisor-ders, etc.
The most common etiologic agents were anti-infectious drugs (15 ADRs). Other drug groups as-sociated with the development of ADRs were anal-gesics and non-steroidal antiinflammatory agents (5 ADRs), glucocorticosteroids (3 ADRs), thiazide diuretics (3 ADRs). In 10 cases, it was impossible to detect a single ADR-inducing drug due to the concomitant use of drugs capable of inducing the adverse event.
The development of ADRs was attributed to underlying DDIs in 10 of these cases (23.25%). The majority of them presented as hypotension (7 cas-es), the rest being single cases of melena, hypokale-mia and somnolence and dizziness (Table 5).
In two patients, more than 1 DDI per patient that could contribute to the development of ADRs was detected. Overall 13 DDIs were found in 10 pa-tients who experienced an ADR.
Discussion
Potential DDIs were found in a significant part of the hospitalized dermatology patients – 35.5% (236 patients) of the study population (674 pa-tients). This frequency is similar to the results of Zwart-van Rijkom et al., who report 27.8% of hos-pitalized patients to have experienced at least one DDI, although many studies have identified high-er proportions of hospitalized patients with DDIs – 49.7% in the study of Cruciol-Souza and Thom-son,66% in the study of Blix et al. [20–22]. These differences can be attributed to variations in the morbidity and drug use in the examined patient cohorts, and also to the methods used for the de-tection of DDIs. It is also possible that the time of observation in this study was too short (medi-an 8 days) for the clinical or laboratory m(medi-anifesta- manifesta-tion of expected ADRs resulting from DDIs, and at least some of these events might have been evident after hospital discharge.
Consistent with findings from studies of po-tential DDIs in various patient populations, the number of prescribed drugs was significantly asso-ciated with DDIs [23, 24]. In this study it was the strongest predictor for the development of DDIs.
The drug groups most commonly involved in DDIs were cardiovascular drugs (diuretics, ACE- -inhibitors, ARBs, beta-blockers, etc.). High con-sumption of cardiovascular drugs due to the pres-ence of cardiovascular diseases in 52.8% of the patients included in the study provides the basis for such interactions.
In agreement with other studies, anticoagu-lants were also found to be frequently implicated in DDIs [20, 23, 24]. Since strict clinical and labo-ratory monitoring of hospitalized dermatology pa-tients on coumarins has been performed, no actual DDIs with these high risk drugs were detected dur-ing the study period.
Typical for this cohort of patients were DDIs including central nervous system (CNS) depres-sants like antihistamines, benzodiazepines and antipsychotics with potential additive CNS de-pressant effects (Table 4). Although second-gen-eration antihistamines (loratadine, desloratadine, cetirizine, levocetirizine, etc.) are designated as “non-sedating”, some studies show that they can also induce sedation, especially if used in higher doses [27]. Sleepiness and impaired psychomotor function are the expected clinical outcomes result-ing from DDIs between first- and second-gener-ation antihistamines as well as between antihis-tamines and benzodiazepines or antipsychotics. Sedation may not always be an unwanted effect in hospitalized dermatology patients with intensely pruritic dermatoses, but in outpatients it is always problematic.
Although a substantial part of the potential DDIs in this study (87.5%) were considered clini-cally significant, only 2.6% (13 DDIs) were impli-cated in the development of ADRs. These results are very similar to the results from a study evalu-ating admissions to medical hospital departments because of potential DDIs showing that 2.4% of
all patients with potential DDIs were admitted be-cause of an ADR be-caused by a DDI [28].
A higher incidence of DDI-related ADRs has been found in elderly hospitalized and outpa-tients [4, 7, 29]. Sixteen studies performed from 2000 to 2010 reported an elevated risk for hospi-talization in older adults associated with adverse drug interactions [30]. Alterations in physiologi-cal functions, polymorbidity and polypharmacy in elderly patients account for higher frequencies of DDIs in this age group. Age was not a strong pre-dictor of DDIs in this study compared to the factor “number of drugs used”. Polymorbidity and relat-ed consumption of multiple drugs but not age it-self seem to be more important predisposing fac-tors for the occurrence of DDIs.
Although limited to dermatology patients from one hospital, this study provides evidence that the DDI risk profile of this patient group does not dif-fer substantially from the profile of patients from other medicinal wards. It is well established that the number of medications and old age are predic-tors for DDIs, although other facpredic-tors like female sex, length of hospital stay and suffering from car-diovascular disease have also been mentioned in literature [21, 24, 25]. Variations in the report-ed prevalence rates of DDIs coming from diverse study populations are due not only to differences in patient characteristics and drug consumption, but also to the methods used to detect DDIs. The authors applied a two-step method using a quick on-line drug interactions checker followed by
Table 5. Adverse drug reactions related to drug-drug interactions
Tabela 5. Działania niepożądane związane z interakcjami lek–lek
Organ/system
(Układ) Symptom/laboratory abnormality (Objaw/zaburzenie laboratoryjne) DDIs* (N) Central nervous system disorders
(Zaburzenia układu nerwowego) somnolence and dizziness antihistamine + neuroleptic (1) Metabolic and nutritional disorders
(Zaburzenia metabolizmu i odżywiania) hypokalemia loop diuretic + thiazide (1) Cardiovascular disorders
(Zaburzenia sercowo-naczyniowe) hypotension ACE-inhibitor + thiazide (3)ACE-inhibitor + loop diuretic (2) thiazide + loop diuretic (1) ARB + thiazide (2) ARB + nitrate (1) Gastro-intestinal system disorders
(Zaburzenia żołądkowo-jelitowe) melena clopidogrel + aspirin (1)aspirin + glucocorticosteroid (1)
verification in Stockley’s Drug Interactions. This is a time-consuming procedure but it was necessary to accurately identify DDIs despite the differenc-es in drug nomenclature in thdifferenc-ese two information resources. ePocrates® demonstrated a satisfactory sensitivity to detect positive cases for DDIs.
The proportion of patients with DDI-related ADR amounted to 23.25% of all patients present-ing with ADRs for the study period. It is general-ly estimated that between 6 and 30% of all ADRs are due to DDIs [6]. The authors report one case of gastrointestinal bleeding due to DDIs between an-tiplatelet agents and glucocorticosteroids. Others investigating ADRs caused by DDIs have detected gastro-intestinal bleeding as a very common clin-ical manifestation of such ADRs, along with elec-trolyte disturbances, hyper- or hypotension and cardiac rhythm disorders [5, 29].
Potential DDIs were detected in one-third of hospitalized dermatology patients. The drug groups most commonly involved in DDIs were cardiovascular drugs. The present findings con-firm results from studies showing that the propor-tion of DDIs associated with potentially relevant clinical consequences appears to be relatively low.
No matter how rare these cases are, patients at risk for potential DDIs should be closely monitored in order to prevent the development of ADRs which may be severe and require specific treatment. Spe-cial attention should be paid to elderly patients and patients with chronic diseases on long term medi-cation, especially cardiovascular, and to those us-ing high-risk drugs like anticoagulants and anti-platelet agents.
References
[1] Ritter JM, Lewis LD, Mant TGK: A Textbook of Clinical Pharmacology. Arnold, london 1999, 4th ed., 97–107.
[2] McDonnell PJ, Jacobs MR: Hospital admissions resulting from preventable adverse drug reactions. Ann Pharmacother 2002, 36, 1331–1336.
[3] Pirmohamed M, James S, Meakin S, Green C, Scott AK, Walley TJ, Farrar K, Park BK, Breckenridge AM:
Adverse drug reactions as cause of admission to hospital: prospective analysis of 18820 patients. BMJ 2004, 329, 15–19.
[4] Bjorkman IK, Fastbom J, Schmidt IK, Bernsten CB: Drug-drug interactions in the elderly. Ann Pharmacother 2002, 36, 1675–1681.
[5] Becker ML, Kallewaard M, Caspers PW, Visser LE, Leufkens HG, Stricker BH: Hospitalisations and emergency department visits due to drug-drug interactions: a literature review. Pharmacoepidemiol Drug Saf 2007, 16, 641– 651.
[6] Pirmohamed M, Orme MLE: Drug interactions of clinical importance. In: Davies’s Textbook of Adverse Drug Reactions, Eds.: Davies D, Ferner R, de Glanville H, Chapman & Hall Medical, london 1998, 888–912.
[7] Becker ML, Visser LE, van Gelder T, Hofman A, Stricker BHCh: Increasing exposure to drug-drug interactions between 1992 and 2005 in people aged > or = 55 years. Drugs & aging 2008, 25, 145–152.
[8] Vonbach P, Dubied A, Krähenbühl S, Beer JH: Evaluation of frequently used drug interaction screening pro-grams. Pharm World Sci 2008, 30, 367–374.
[9] Mallet L, Spinewine A, Huang A: The challenge of managing drug interactions in elderly people. lancet 2007, 370, 185–191.
[10] Del Rosso JQ: Drug interactions of clinical significance to dermatologists: A primer and update. Curr Probl Dermatol 2000, 12, 63–68.
[11] Ganeva М, Gancheva T, Baldaranov I, Troeva J, Hristakieva E: Screening for adverse drug interactions in der-matology patients. TJS 2010, 8, 266–271.
[12] World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. http://apps.who.int/classifications/icd10/browse/2010/en
[13] ATC/DDD Index 2012. WHO Collaborating Centre for Drug Statistics Methodology. http://www.whocc.no/atc_ ddd_index/
[14] ePocrates®https://online.epocrates.com/home
[15] Stockley’s Drug Interactions. Ed.: Baxter K, Pharmaceutical Press, london, 2010, 9th ed.
[16] World Health Organization: International drug monitoring: The role of the hospital WHO Tech Rep Ser No. 425, 1969.
[17] Uppsala Monitoring Centre (UMC), the World Health Organization Collaborating Centre for International Drug Monitoring [http://www.umcproducts.com/graphics/3149.pdf]
[18] Rawlins MD, Thompson JW: Mechanisms of adverse drug reactions. In: Textbook of Adverse Drug Reactions. Ed.: Davies DM, Oxford University Press, Oxford 1991, 18–45.
[19] Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, Janecek E, Domecq C, Greenblatt DJ: A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther 1981, 30, 239–245.
[20] Zwart-van Rijkom JEF, Uijtendaal EV, ten Berg MJ, van Solinge WW, Egberts ACG: Frequency and nature of drug-drug interactions in a Dutch university hospital. Br J Clin Pharmacol 2009, 68, 187–193.
[22] Blix HS, Viktil KK, Moger TA, Reikvam A: Identification of drug interactions in hospitals –computerized screen-ing vs. bedside recordscreen-ing. J Clin Pharm Ther 2008, 33, 131–139.
[23] Bertoli R, Bissig M, Caronzolo D, Odorico M, Pons M, Bernasconi E: Assessment of potential drug-drug interactions at hospital discharge. Swiss Med Wkly 2010, 140, w13043.
[24] Mateti UV, Rajakannan T, Nekkanti H, Rajesh V, Mallaysamy SR, Ramachandran P: Drug-drug interactions in hospitalized cardiac patients. J Young Pharm 2011, 3, 329–333.
[25] Vonbach P, Dubied A, Krähenbühl S, Beer JH: Prevalence of drug-drug interactions at hospital entry and during hospital stay of patients in internal medicine. Eur J Intern Med 2008, 19, 413–420.
[26] Magro L, Conforti A, Del Zotti F, Leone R, Iorio ML, Meneghelli I, Massignani D, Visonà E, Moretti U:
Identification of severe potential drug-drug interactions using an Italian general-practitioner database. Eur J Clin Pharmacol 2008, 64, 303–309.
[27] Bender BG, Berning S, Dudden R, Milgrom H, Tran ZV: Sedation and performance impairment of diphenhydr-amine and second-generation antihistdiphenhydr-amines: a meta-analysis. J Allergy Clin Immunol 2003, 111, 770–776.
[28] Fokter N, Mozina M, Brvar M: Potential drug-drug interactions and admissions due to drug-drug interactions in patients treated in medical departments. Wien Klin Wochenschr 2010, 122, 81–88.
[29] Obreli-Neto PR, Nobili A, de Oliveira Baldoni A, Guidoni CM, de Lyra Júnior DP, Pilger D, Duzanski J, Tettamanti M, Cruciol-Souza JM, Gaeti WP, Cuman RK: Adverse drug reactions caused by drug-drug interactions in elderly outpatients: a prospective cohort study. Eur J Clin Pharmacol 2012 [Epub ahead of print] PMID:22644345.
[30] Hines LE, Murphy JE: Potentially harmful drug–drug interactions in the elderly: a review. Am J Geriatr Pharmacother 2011, 9, 364–377.
Address for correspondence:
Maria Ganeva
Section of Pharmacology and Clinical Pharmacology Faculty of Medicine
Thracian University 11 Armeiska St 6000 Stara Zagora Bulgaria
Tel.: 00359 42664/310
E-mail: [email protected] Conflict of interest: None declared Received: 31.08.2012