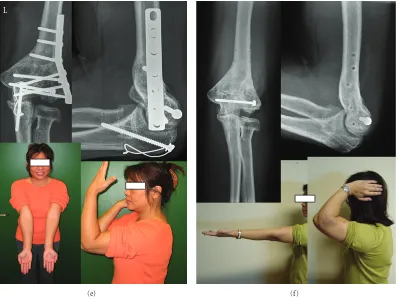
Intra-Articular Osteotomy for Distal Humerus Malunion
Full text
Figure
Related documents
In discussions on the spread and prospects of democracy in the global south, Africa and Middle East are often depicted as less democratic, indeed undemocratic,
Verificando que os sistemas de bike-sharing, ainda apresentam vários problemas, nomeada- mente em termos de redistribuição de bicicletas pela cidade, de segurança e de otimização
Solid waste from the different source from may come in contact with the surface, subsurface, wells, water table, lineaments/fracture and drainage network and which lead to
Conclusions: Accurately measuring the physical availability of alcohol is critical for understanding the causes and consequences of its distribution and for developing
In order to examine the profitability of futures spread trading, we propose a profit model to analyze the potential of this trading strategy, focusing on how the convergence
l Lateral approach to the elbow is usually sufficient to address fractures limited to the capitellum and con- comitant radial head fractures if present.. l Alternative approaches
Instead of changing the zoning ordinance, the planning commission agreed to change its admini- strative rules to allow a streamlined approval process for hoop houses, as long as
Ig allotype and the H-2 genotype are given on the right side. a) Mice of DBA/2 and DBA/l strains have only cross-reacting or even slightly heteroclitic IgM. b) The
