Declining
Frequency
of Circumcision:
Implications
for Changes
in the Absolute
Incidence
and Male
to Female
Sex Ratio
of
Urinary
Tract
Infections
in Early
Infancy
MAJ Thomas
E. Wiswell,
MC, USA,
MAJ
Robert
W. Enzenauer,
MC, USA,
Mark
E. Holton,
DO,
MAJ J. Devn
Cornish,
MC, USAF,
and
CPT Charles
T. Hankins,
MC, USA
From the Department of Pediatrics, Brooke Army Medical Center, Ft Sam Houston, Texas
ABSTRACT. The results of an investigation examining
the circumcision frequency rate and its effect on the
incidence of urinary tract infections in a large, widely dispersed population base during the 10-year period since the 1975 report of the American Academy of Pediatrics
Ad Hoc Task Force on Circumcision are reported. Our
study population included the 427,698 infants born in all
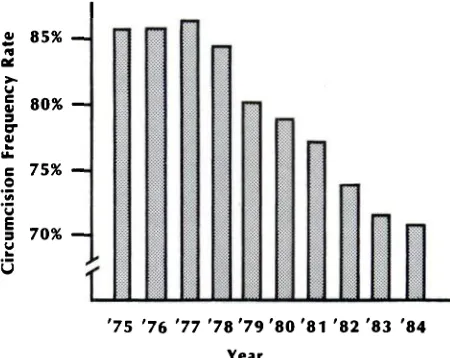
United States Army hospitals, worldwide, from Jan 1, 1975, through Dec 31, 1984. There was an initial plateau in the circumcision frequency rate at approximately 85%
during the first 4 years of the study period. In the
sub-sequent 6 years there was a steady, significant decrease
(P < .001) of 1.4% to 4.0% per year through 1984, when
the circumcision frequency rate reached its nadir of
70.5%. There was a concomitant increase in the total number of urinary tract infections among male infants (P < .02) as the circumcision rate declined. This increase was due to the increase in the overall number of
uncir-cumcised boys (who had a greater than 11-fold increased
infection rate compared with circumcised boys). During the first half of the study period, there was a female predominance for urinary tract infections from birth
onward. As the number of circumcised boys decreased
(with a resultant increase in the total number of boys
with infection), the male to female ratio of urinary tract
infections during the first 3 months of life reversed,
reflecting a movement toward a male predominance for
infection in early infancy. This is the first,
well-docu-mented report of a decreasing rate of circumcisions per-formed on the American male population. We conclude
that the number of urinary tract infections in male
in-fants, as well as the male to female sex ratio, is affected
Received for publication Jan 6, 1986; accepted May 23, 1986.
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as
reflecting the views of the Department of the Army or the
Department of Defense.
Reprint requests to (T.E.W.) Brooke Army Medical Center, Box
64, Ft Sam Houston, TX 78234-6200.
PEDIATRICS (ISSN 0031 4005). Copyright © 1987 by the American Academy of Pediatrics.
by the circumcision practices of the population examined.
Pediatrics 1987;79:338-342; circumcision, urinary tract
infection.
The 1975 report of the American Academy of
Pediatrics Ad Hoc Task Force on Circumcision
concluded, “There is no absolute medical indication
for routine circumcision of the newborn.”1 Most
investigators have failed to demonstrate any
sub-stantial decline in the percentage of males that are
circumcised since the dissemination of the
Amen-can Academy of Pediatrics policy statement.29 In
fact, there have been only two brief reports, both
from military facilities, that have found any
de-crease at all in the circumcision frequency rate.’#{176}”
We speculated that the circumcision frequency rate
in military hospitals involving a large, widely
dis-persed population base will have substantially
de-creased since the 1975 report of the American
Acad-emy of Pediatrics Ad Hoc Task Force.
Additionally, we recently reported evidence for
an increased risk of urinary tract infection in
un-circumcised boys compared with their circumcised counterparts.12”3 We believed that a significant de-dine in the circumcision frequency rate should
result in more uncircumcised boys and more total
urinary tract infections in the male population.
Finally, it is generally believed that there is an
increased incidence of urinary tract infections in
boys compared with girls in early infancy.14’7 Data supporting this contention were reported from
countries in which male infants are infrequently
circumcised.126 In the sole American investigation
ai 85% V 80% C 75% 0 70% Fig 1. 1984.
‘75 ‘76 ‘77 ‘78 ‘79 ‘80 ‘81 ‘82 ‘83 ‘84
Year V -! oc a,’,’ .a Eo z 0 90 85 80 75 70 65 60 55 50 45
Circumcision frequency rates for years 1975 to
[1
urinary tract infection, 95% of the infected male
infants were not circumcised, from a population
base in which fewer than 10% of the boys were
circumcised (G. H. McCracken, personal
commu-nication, February 1985).27 We conjectured that
there may not be a male predominance for urinary
tract infection in a population in which the majority
of male infants are circumcised.
This study was designed to test our hypotheses.
MATERIALS AND METHODS
The newborn medical records of all infants born
in US Army hospitals, worldwide, between Jan 1,
1975, and Dec 31, 1984, were reviewed to determine
the total number of births, the sex distribution, and the circumcision frequency rate. Additionally, in-formation concerning subsequent hospitalizations
of these infants during the first year of life was
evaluated. These data were obtained through the US Army Patient Administration Systems and Biostatistics Activity at Ft Sam Houston, TX. The
accessible data for each infant included: all
diag-noses made, duration of hospitalization, procedures
performed and the child’s age and sex. The records
of male infants were cross-referenced with the birth records to determine individual circumcision status. Because all diagnoses in the newborn records and
from subsequent hospitalizations were available,
infants with known congenital anomalies or other
conditions predisposing them to urinary tract
in-fection could be identified and excluded from the study. Further details concerning an individual
pa-tient’s hospital course were not readily accessible.
No information was available regarding
cincumci-sions performed in an out-of-hospital setting (eg, a
Jewish “bniss” at eight days of age) or after the
neonatal period.
Data were tested for significance using
x2
analy-sis.
RESULTS
During the study period, 427,698 infants were
born in Army hospitals. There was an initial
pla-teau in the circumcision frequency rate at
approx-imately 85% from 1975 through 1978. However,
during the subsequent 6 years (Fig 1) there was a
steady, significant decrease (P < .001) of 1.4% to
4.0% per year through 1984, when the circumcision
frequency rate reached its nadir of 70.5%. Of the
infants 1,661 (0.39%) were rehospitalized during
the first year of life with symptomatic urinary tract
infections. Infections were seen in 1,051 of 207,923
female infants (0.51%) and 610 of 219,775 male
infants (0.28%). Of the procedures performed for urine cultures in male infants, 92% were suprapubic
]
iflflfl
‘75 ‘76 ‘77 ‘78 ‘79 ‘80 ‘81 ‘82 ‘83 ‘84 Fig 2. Total number of urinary tract infections in male
infants for years 1975 to 1984.
bladder aspirations and 8% were bladder
catheter-izations. Similarly, 90% of the female urine cultures
had been obtained by suprapubic bladder aspiration
and 10% by catheterization.
Although only 21% of the male population was
not circumcised, 72% of the male urinary tract infections were in these infants. As the
circumci-sion frequency rate decreased, there was a
condom-itant significant increase in the total number of
male infants with urinary tract infections (Fig 2)
(P < .02). The yearly incidence of urinary tract
infections among both circumcised (0.07% to 0.13%
pen year) and uncircumcised (0.85% to 1.25% per
year) male infants remained relatively constant
during the entire study period. Thus, the increase
in the total number of male urinary tract infections was not due to an increased incidence of infection in either group, but due to the absolute increase in
TABLE 1. Comparison ofCircu and Number of Urinary Tract I
and Second Halves of Study
mcision Frequency Rate nfections During First
1975-1979 1980-1984
Male infants (No.)
Circumcised 89,975 83,688 Uncircumcised 16,648 29,464 Circumcision frequency rate (%) 84.3 74.0 Urinary tract infections in male
infants (No. [%])
Circumcised 94 (0.10) 57 (0.07)
Uncircumcised 172 (1.03) 287 (0.98)
Total female infants born (No.) 101,025 106,898
Total urinary tract infections in 527 (0.52) 524 (0.49)
female infants (No. [%])
TABLE 2. Relationship of Circumcision Frequency
Rate and Male to Female Ratio of Urinary Tract
Infec-tions
1975-1979 1980-1984
Circumcision frequency rate (%) 84.3 74.0 Male/female urinary tract
infec-tion ratio
During first month of life 1.0:1.2 1.7:1.0 During first 3 mo of life 1.0:1.6 1.0:1.0 During last 9 mo of first year 1.0:2.9 1.0:2.3
of life
During the last 5 years of the study period, there
was a significant decline in the circumcision
fre-quency rate from 84.3% during the first half of the study to 74.0% during the latter half (P < .001). As the number of circumcised boys decreased, there was a concomitant increase in the total number of
boys with urinary tract infections and in the male
to female ratio of infections, reflecting a movement toward a male predominance for urinary tract
in-fections during early infancy (Table 2).
DISCUSSION
Circumcision is the most commonly performed
surgical procedure in the United States.9’28’29 It is
estimated that 80% to 98% of all American male infants (>1,250,000 annually) are circumcised.9’28
In 1971 the American Academy of Pediatrics
Com-mittee on Fetus and Newborn concluded, “There
are no valid medical indications for routine
per-formance of the procedure in the neonatal period.”30
The American Academy of Pediatrics Ad Hoc Task
Force on Circumcision subsequently reaffirmed this
position statement in 1975.’ The position of the
American Academy of Pediatrics was endorsed by
the American College of Obstetricians and Gyne-cologists in 1978.
Several authors have noted that there has been
no apparent decrease in the percentage of male
infants circumcised since the position of the
Amen-ican Academy of Pediatrics was expressed.29 These
data are reported from relatively small populations
over a short period of time, making it impossible to
discern a trend.9 There have been only two reports
of reductions in the circumcision frequency rate.’#{176}” Gorske’#{176} reported a 30% decrease in the
circumci-sion frequency rate following a program of written and oral counseling. Enzenauer et al” reported a
20% decline with the use of videotape counseling. Interestingly, both of these reports originated from military hospitals.
There was no uniform method of circumcision counseling in our study population, nor were there
any “official” attempts to mandate more detailed
or extensive informed consent counseling during
this period. We conjecture that there may be several
possible reasons for the decrease in the
circumci-sion frequency rate that are, perhaps, unique to our
particular population.
The majority of military physicians performing the procedure (pediatricians, family practitioners, and obstetricians) are either in training or within 5 years of having completed residency training. As
such, these physicians may be more cognizant of
the changing philosophy in favor of noncircumci-sion. Younger physicians may be more willing to
“break” with the established tradition of
recom-mending routine circumcision.
Additionally, substantially more pediatricians
perform circumcisions in military compared with civilian hospitals (>50% v <10%). It is reasonable
to speculate that pediatricians are more aware of
the American Academy of Pediatrics position and, in their capacity as child advocates, influence the
decline in the circumcision frequency ratio by the
manner in which they counsel parents regarding
the procedure.
Finally, there is no additional financial remuner-ation to be gained by military physicians who
per-form circumcisions. Thus, these physicians may
counsel more vigorously “against” a procedure which is both time consuming and for which there
is no profit. In “private practice . . . noncircumci-sion is doubly costly: There is no fee, and there is
loss of time convincing parents not to have their
sons circumcised.”9 Wallerstein concludes, “If their
salary does not cover this ‘service’ (as in Britain), they tend to shy away from it.”3#{176}
We have previously reported a significant
in-crease in urinary tract infections in uncircumcised
boys compared with their circumcised
counter-parts.’2”3 Our present data indicate that as there
became a higher percentage of noncircumcised boys
in our population, there were more total infections.
This increase was due solely to the fact that there
population (who have 10 to 20 times as many
infec-tions as circumcised boys’2”3).
The authors wish to emphasize that we do not
yet advocate routine neonatal circumcision for all
male infants because of the data we have
accumu-lated. As yet, there is no information regarding
whether or not the 1.0% to 4.1% of uncircumcised
male infants that have urinary tract infections will
subsequently have long-term urologic problems.
However, we emphatically believe that the
in-creased risk for infection should be conveyed to the parents as part of informed consent circumcision counseling.
There have been numerous reports on urinary
tract infections in newborns and older in-fants.12”3”827’31’32 Many of these are studies of asymptomatic bacteriuria detected by screen-ing.2”23’25’26’3’ In most of these reports, infections were more frequent in males during early infancy.
However, the majority of the studies that show a
male predominance for urinary tract infection were
performed in countries in which few boys are rou-tinely circumcised (Sweden,’8”9 England,20’2’ Aus-tralia,22 New Zealand,23’24 Switzerland,25 and Germany26). From the United States, Ginsburg and
McCracken27 reported a male predominance for
symptomatic urinary tract infection during the first 3 months of life. However, 95% of these infected boys were not circumcised. Additionally, the cir-cumcision frequency rate in their study population was less than 10%, far less than the 80% to 98% rate seen throughout the rest of the country (G. H. McCracken, personal communication, February 1985).28
Edelman et a!3’ screened full-term and premature infants for bacteriuria (in their hospital in New
York). They found no male predominance in the
infants they studied. A recent collaborative inves-tigation examined urinary tract infection in infants
with unexplained fever.32 The study involved 505
infants from various areas in the United States. All nine of the infants with urinary tract infection were girls. None of the 233 male infants investigated had such an infection. Presumably, the circumcision frequency rate of the broad population base was similar to that of the country as a whole.
Again, as the percentage of noncircumcised boys in our population rose, the total number of urinary
tract infections in male infants also increased. With
the decrease in the circumcision frequency rate, there was a change in the male to female ratio of symptomatic urinary tract infections, a male
pre-dominance in early infancy becoming evident as
fewer boys were circumcised. We speculate that in the United States there is no male predominance for urinary tract infections in early infancy. If there
is a nationwide increase in the number of uncircum-cised male infants, we may well see such a male
predominance.
We conclude that there has been a significant
decrease in the circumcision frequency rate of our study population since the 1975 American Academy of Pediatrics Ad Hoc Task Force report.
Addition-ally, the number of urinary tract infections in male infants is affected by the circumcision frequency rate of the population studied. As such, we found the male to female ratio of urinary tract infections in early infancy is affected by changes in the per-centage of male infants that are circumcised.
REFERENCES
1. American Academy of Pediatrics Committee on Fetus and
Newborn: Report of the Ad Hoc Task Force on Circumci-sion. Pediatrics 1975;56:610-611
2. Bennett HJ, Weissman M: Circumcision: Knowledge isn’t enough. Pediatrics 1981;68:750
3. Herrera AJ, Hsu AS, Salcedo UT, et al: The role of parental information in the incidence of circumcision. Pediatrics
1982;70:597-598
4. Herrera AJ, Cochran B, Herrera A, et al: Parental infor-mation and circumcision in highly motivated couples with higher education. Pediatrics 1983;71:233-234
5. Maisels MJ, Hayes B, Conrad 5, et al: Circumcision: The effect of information on parental decision making. Pediatrics
1983;71:453-455
6. Land JA, Policastro AM: Parental information and circum-cision: Another look. Pediatrics 1983;71:142-143
7. Boyce WT: Care of the foreskin. Pediatr Rev 1983;5:26-30 8. Metcalf TJ, Osborn LM, Moriani EM: Circumcision: A
study of current practices. Clin Pediatr 1983;22:575-579 9. Wallerstein E: Circumcision: The uniquely American
medi-cal enigma. Urol Gun North Am 1985;12:123-132
10. Gorske AL: Circumcision and patient education. Am J Dis
Child 1980;134:521
11. Enzenauer RW, Powell JM, Wiswell TE, et al: Decreased circumcision rate with videotape counseling. South Med J
1986;79:717-720
12. Wiswell TE, Smith FR, Bass JW: Decreased incidence of
urinary tract infections in circumcised male infants. Pedi-atrics 1985;75:901-903
13. Wiswell TE, Roscelli JD: Corroborative evidence for the decreased incidence of urinary tract infections in circum-cised male infants. Pediatrics 1986;78:96-99
14. Stamey TA: Urinary infections in infancy and childhood, in Stamey TA: Pathogenesis and Treatment of Urinary Tract
Infections. Baltimore, Williams & Wilkins, 1980, pp 290-341
15. Belman AB: Genitourinary infections, in Kelalis PP, King LR, Belman AB (eds): Clinical Pediatric Urology.
Philadel-phia, WB Saunders Co, 1985, pp 238-239
16. Sidor TA, Resnick MI: Urinary tract infections in children.
Pediatr Clin North Am 1983;30:232-332
17. Durbin WA, Peter G: Management of urinary tract infec-tions in infants and children. Pediatr Infect Dis
1984;3:564-574
18. Winberg J, Andersen RI, Bergstrom T, et al: Epidemiology of symptomatic urinary tract infection in childhood. Acta
Pediatr Scand 1974; suppl 252:1-20
19. Bergstrom T, Larson H, Lincoln K, et al: Studies of urinary tract infections in infancy and childhood. XII. Eighty con-secutive patients with neonatal infection. J Pediatr
1972;80:858-866
radiological features of urinary tract infection in childhood.
Br Med J 1964;2:1222-1226
21. Littlewood JM, Kite P, Kite BA: Incidence of neonatal urinary tract infection. Arch Dis Child 1969;44:617-620 22. Drew JH, Acton CM: Radiological findings in newborn
infants with urinary infection. Arch Dis Child
1976;51:628-630
23. Abbott GD: Neonatal bacteriuria: A prospective study in
1,460 infants. Br Med J 1972;1:267-269
24. Bourchier D, Abbott GD, Maling TMJ: Radiological abnor-malities in infants with urinary tract infections. Arch Dis Child 1984;59:620-624
25. Maherzi M, Guignard J-P, Torrado A: Urinary tract infec-tion in high-risk newborn infants. Pediatrics
1978;62:521-523
26. Reindke B, Daschner F, Morgenroth H, et al: Value of
screening for bacteriuria in infants. Proc Eur Dial
Trans-plant Assoc 1975;111:132-139
27. Ginsburg CM, McCracken GH: Urinary tract infection in
young infants. Pediatrics 1982;69:409-412
28. Kaplan GW: Circumcision-An overview. Curr Prob Pediatr
1977;7:1-33
29. Wallerstein E: Circumcision: An American Health Fallacy.
New York, Springer Publishing Co, 1980, p 30
30. American Academy of Pediatrics, Committee on Fetus and Newborn: Hospital Care ofNewborn Infants, ed 5. Evanston,
IL, American Academy of Pediatrics, 1971, p 110
31. Edelmann CM, Ogwo JE, Fine BP, et al: The prevalence of
bacter,uria in full-term and premature newborn infants. J
Pediatr 1973;83:125-132
32. Roberts KB, Charney E, Sweren RJ, et al: Urinary tract
infection in infants with unexplained fever: A collaborative study. J Pediatr 1983;103:864-867
ERRATUM
Through an oversight that the editors are unable to explain, the names of
Drs Richard R. Brookman and John M. Pascoe were omitted from the list of
1986 reviewers published in the December 1986 issue of Pediatrics. We thank