Nursing Staff Knowledge of Cost and Perceptions of Cost-Conscious Practices: A Replication Study
Brannin E. St. Clair
Senior Honors Thesis School of Nursing
University of North Carolina at Chapel Hill March 22, 2019
Approved: Maureen J. Baker
1
Abstract
As principal users of bedside supplies and equipment, nurses are in an optimal position to positively impact cost-containment initiatives in the hospital setting. However, nurses’ ability to make cost-effective decisions in their daily clinical practice requires a solid foundation in, and working knowledge of, costs and cost-conscious practices. This replication study aimed to determine if knowledge of supply costs, attitudes toward cost-conscious practices, and interest in involvement in unit-level budgeting amongst UNC cardiac nurses had improved, diminished, or remained the same since the original parent-study conducted a decade ago. A total of 42 nurses working in the cardiac service of a single, academic healthcare center in Chapel Hill, North Carolina participated in the replication study. Data were gathered via an anonymous, online survey. Results of 2008 and 2018 survey data were compared using two proportion z-tests and Pearson’s chi square. Fewer than half of respondents correctly identified the cost of commonly used bedside supplies and equipment. Despite their limited awareness of costs, participants maintained a positive attitude towards cost-conscious practices and expressed interest in
budgetary issues. Results of the current study were largely consistent with the 2008 parent-study, which found a similar gap between nurse knowledge of cost-effective practices and their
willingness to learn and implement cost saving practices. This study, like its parent-study and its predecessors, highlights an opportunity for nurse leaders and educators to examine, address, and improve financial competencies among current and future nurses.
2 A Replication Study
Foreword
While progressing through the UNC nursing program, I have had a series of professors, nurse (RN) mentors, and fellow students who encouraged and deepened my natural sense of inquiry, empathy, and compassion for my patients. However, I consistently noticed a distinct lack of knowledge and capability in another key area of the profession: the economics of
healthcare. As a former owner of a construction company, I had trained myself to know the price points of every nut and bolt, and I expected the same cost-consciousness to be practiced during my clinical rotations. However, to my surprise, I found the financial literacy among the nurses with whom I was working to be limited.
As the United States healthcare system has moved from a volume-based to value-based reimbursement paradigm, an understanding of frontline nurses’ knowledge regarding health care costs and cost-efficient practices is essential for the delivery of efficient and effective patient care. My honors project is a first step towards understanding what nurses know, what they do not know, and if nurses’ knowledge of costs and cost-conscious nursing practice has changed in the past decade.
3 Rising healthcare costs spark debate everywhere from dinner tables to the United States Senate floor. An important tenet of the Triple Aim, a strategic framework for health care improvement, is to reduce per capita costs of healthcare (Berwick, 2008). Nurses make up the largest discipline in the hospital setting and are the primary users of hospital resources, and are therefore vital to ensuring that supplies and equipment are efficiently used at the bedside (Douglas, 2010; Hernu et al., 2018; Heydari et al., 2015). For nursing practice to be efficient, nurses must have a strong foundational working knowledge of supply costs and cost-effective practices, potentially leading to successful cost-containment efforts in hospitals (Caroselli, 1996; Douglas, 2010; Hernu et al., 2018; Heydari et al., 2015). However, historically, frontline
healthcare providers (HCP) have alarmingly poor awareness of supply costs and how their use of these resources may affect the overall hospital budget (Caroselli, 1996; Clancy and Murphy, 2014; Hadjipavlou & Bailey, 2010; Hernu et al., 2018; Heydari et al., 2015; Jackson et al., 2015; Kynaston et al., 2017).
Ten years ago, Christa Seaman, RN, DNP (2008) sought to gain insight into the financial competencies of nurses in the Cardiovascular service line at a large teaching hospital in the Southeastern United States. Seaman (2008) concluded that although nurses maintain a positive attitude towards cost-conscious practices, their knowledge of supply and equipment costs was lacking. Despite nurses financial literacy shortcomings, the majority of nurses indicated they wished to be more involved in the financial decision-making on their unit (Seaman, 2008). The purpose of this study was to replicate Seaman’s (2008) study and assess if nurses’ financial knowledge has changed since the 2008 study.
4 instruments, research questions, and hypothesis were nearly identical to Seaman’s 2008 study (Brandt et al., 2014). Due to the lack of published data prior to and since Seaman’s 2008 study, I aimed to answer the following research questions in order to determine if financial literacy (i.e. knowledge of supply costs, attitudes toward cost-conscious practices, and related budgetary concerns) amongst nurses had improved, diminished, or remained the same:
1. How familiar are nursing staff with the costs of common supplies and equipment used at the bedside?
2. How do nursing staff rate their overall knowledge of supply and equipment costs? 3. How do nurses apply their knowledge of supply and equipment costs?
4. What are nursing staff perceptions of the cost-conscious practices in their daily work and decision-making?
5. What are the differences between 2008 and 2018 nurse perceptions of costs and cost-effective practices?
Review of Literature
5 seven relevant articles, including five of international domain, were identified and reviewed. The articles reviewed centered on a few major themes: nurses’ economic awareness; cost-awareness of health providers; and nurse attitudes regarding cost-awareness and cost-conscious practices.
Economic Awareness
More than two decades have passed since Caroselli’s (1996) landmark research revealing severe deficits in the economic awareness and cost-consciousness of nurses. In her study,
orthopedic and cardiac surgical nurses from two urban academic medical centers were given the Wieseke-Bantz Economic Awareness Questionnaire to assess and calculate nurses’ Economic Awareness Scores (EAS) (Caroselli, 1996). Economic awareness was described as nurses’ knowledge of healthcare budgeting on a national and institutional level (Caroselli, 1996). Just over half of the 16 questions were answered correctly (mean EAS = 8.5) by the 68 nurses who responded to the survey, indicating poor budgetary awareness (Caroselli, 1996). Interestingly, demographic variations such as gender, level of education, and marital status had no effect on the mean EAS (Caroselli, 1996). Respondents’ budgetary or finance knowledge was reported as self-taught; however, the majority of respondents admitted having no budgetary or finance
knowledge (Caroselli, 1996). Caroselli (1996) concluded an overall lack of economic awareness existed among nurses.
Cost-Awareness
6 need for nurses’ alarmingly poor cost-awareness to be addressed and remedied (Hernu et al., 2018).
Another recent observational research study conducted in England evaluated operating room (OR) staff awareness of supply costs (Kynaston, Smith, & Batt, 2017). Physicians, nurses, and surgical technicians within a National Health Service (NHS) foundation trust completed a 13-item questionnaire. Respondents were asked to estimate the costs of various commonly used operating room supplies (Kynaston et al., 2017). Of the 48 individuals surveyed, only 22% were able to correctly estimate supply costs. No significant differences were found in cost-awareness between OR physicians and nurses. Results, consistent with the Hernu et al. (2018) findings, indicated that cost-related knowledge deficits could negatively impact the OR staff’s ability to make informed and efficient choices when using supplies and equipment (Kynaston et al., 2017).
Clancy and Murphy (2014) employed an eight-question survey in their quantitative observational study, which assessed staff attitudes and awareness of laboratory testing costs within a regional hospital in Ireland (Clancy & Murphy, 2014). The study revealed that both physicians (n=101) and nurses (n= 125) possessed knowledge deficits and reported having “little confidence” in their financial knowledge relating to laboratory costs (Clancy & Murphy, 2014). In fact, only 25% of the cost-assessment questions were correctly answered. And, since these questions only provided four multiple choice price options, even the correct answers may have reflected random chance more than educated responses. (Clancy & Murphy, 2014).
7 majority of both surgical trainees and fellows surveyed were unable to accurately estimate supply costs within 20% of the actual costs (Jackson et al., 2015).
In a different study, Hadjipavlou and Bailey (2010) surveyed 50 physicians within the Department of Anesthetics at Guy’s and St. Thomas’ NHS Foundation Trust in the United Kingdom, to evaluate the staff’s knowledge of commonly used medication and supply costs. Participants were instructed to estimate the cost of 20 medications and 13 disposable supplies listed on the questionnaire (Hadjipavlou & Bailey, 2010). The findings indicate that knowledge of costs and cost-conscious practices amongst anesthesia staff were lacking, as only 20% of the participants estimated costs within 25% of the actual cost (Hadjipavlou & Bailey, 2010). Hadjipavlou and Bailey (2010) claim this knowledge deficit has persisted, unchanged, over the past 15 years, indicating that interventions to improve cost-related knowledge, if any, were not working.
Attitudes Toward Nurse Involvement in Budgetary Issues
Nurse knowledge and application of cost-containment practices were studied in an Iranian cross-sectional study (Heydari, Mazloom, Najar, & Bakhshi, 2015). One hundred
8
Original Parent Study
An online survey conducted in 2008 within the cardiac service line at UNC Hospital assessed nursing staff awareness of supply and equipment costs and perceptions of
cost-conscious practices (Seaman, 2008). In the survey, Seaman (2008) employed a combination of multiple choice questions, open-ended questions, and rated answers using a Likert-type scale. Additionally, a modified version of the Blaney/Hobson Nursing Attitude Scale (BHNAS) was used to measure staff perceptions of cost-conscious practices in their daily practice and decision-making (Seaman, 2008).
Seventy-five participants took part in Seaman’s (2008) study. The results indicated nursing staff had very little knowledge of supply and equipment costs; only 34% of respondents identified the correct cost of only a few commonly used supplies (e.g. gauze, disposable
stethoscope, telemetry box) (Seaman, 2008). The mean score on the modified BHNAS was 45.7 out of a possible range of 15-60 (Seaman, 2008). Similar to findings by Heydari et al. (2015), the results from Seaman’s (2008) study found that participants lacked financial literacy yet held positive attitudes towards becoming more involved in financial decision-making on their unit.
Summary
9 in budgetary issues, and desire to be involved in budgetary issues has evolved over the past 10 years.
Further research has been recommended to identify baseline knowledge and attitudes of frontline HCPs in order to develop effective interventions to improve knowledge of supply costs, cost-effective practices, and cost-containment initiatives (Caroselli, 1996; Clancy and Murphy, 2014; Hadjipavlou & Bailey, 2010; Hernu et al., 2018; Heydari et al., 2015; Jackson et al., 2015; Kynaston et al., 2017; Seaman, 2008). To date, no replication studies on nurses’ financial
awareness have been conducted. The purpose of this study is to assess nurses’ financial literacy, as well as assess whether nurses’ financial literacy has evolved, devolved, or remained
unchanged over the past decade. Findings from this study will help determine if interventions implemented, if any, (e.g. nursing education, nursing orientation, nursing continuing education programs) have been effective at one academic hospital.
Methods
As a ‘close’ replication study, and to enhance fidelity, the research design was modeled to be nearly identical to Seaman’s 2008 study, “Nursing Staff Knowledge of Cost and Budgetary Control.” An online survey design was used to determine practicing nurses’ knowledge of supply and equipment costs as well as the extent to which they apply that knowledge in practice.
Nursing staff perceptions regarding cost-effective practices, cost-conscious decision-making processes, and participation in hospital budgeting were also examined.
Setting and Sample
10 Neurosciences Hospital, Women’s Hospital, Cancer Hospital, and Memorial Hospital. The UNC Health Care System (UNCHCS) currently has over 7,100 employees dedicated to providing quality, evidence-based treatment options to over 37,000 patients each year ("UNC Medical Center", 2019).
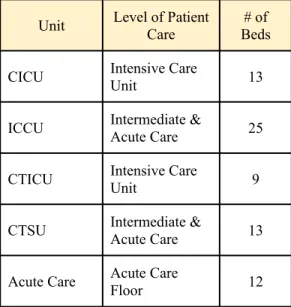
The present study was conducted in the Center for Heart and Vascular Care at UNCH (Cardiac Intensive Care Unit [CICU], 3 Anderson [ICCU], Cardiothoracic Intensive Care Unit [CTICU], Cardiothoracic Step-down Unit [CTSU], and 5 Anderson). The CICU is a 13-bed unit specializing in the management of an array of high-acuity, cardiac-related diagnoses. The Intermediate Coronary Care Unit (ICCU) has 19 acute care beds and six progressive care beds and manages care for patients with various coronary issues including myocardial infarction and heart failure. The 9-bed CTICU and the 13-bed CTSU host post-surgical cardiac and thoracic patients, including coronary artery bypass grafts (CABGs), heart valve repair/replacements, and heart and lung transplants. The last unit is a 12-bed, general acute care unit that specializes in the care of cardiology, thoracic and vascular patients. See Table 1 for unit breakdown.
Table 1. Description of Patient Care Units and Target Sample Personnel
Unit Level of PatientCare Beds# of
CICU Intensive Care Unit 13
ICCU Intermediate & Acute Care 25
CTICU Intensive Care Unit 9
CTSU Intermediate & Acute Care 13
11 Registered nurses from the five aforementioned patient care units were invited to take part in the online survey (estimated to be ~148 nurses). Fifty-three nurses consented to participating in the survey, however, several surveys were submitted as incomplete and were excluded from the data set, leaving 42 participants in the sample (n=42).
Variables and Their Measurement
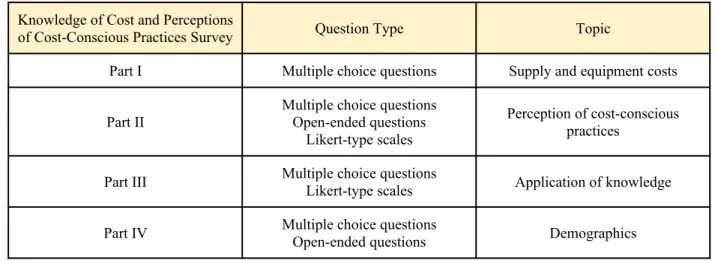
The study employed the same 4-part survey as Seaman used in 2008 to address the first four research questions. Part I of the survey included 10 multiple choice questions which were used to gain insight into participants’ knowledge of commonly used supply and equipment costs. Participants were asked to select the answer that most accurately represented the true cost of each item. The 10 items mirrored those on Seaman’s (2008) survey, however, costs were adjusted and scaled to reflect current pricing.
Part II included 15 multiple choice and two open-ended questions designed to measure the perception of cost-conscious practices in the daily work and decision-making amongst the nursing staff. Several multiple choice questions were derived from the Blaney/Hobson Nursing Attitude Scale (BHNAS) and were used with the permission of Dr. Charles J. Hobson (See AppendixA) (C. Hobson, personal communication, August 23, 2018). Participants were asked to indicate the degree to which they agreed or disagreed with nursing practice statements using a 4-point Likert-type scale. Possible scores on the BHNAS range from 15 to 60 4-points, with a higher score indicating a more positive attitude toward cost-effective nursing practices (C. Hobson, personal communication, August 23, 2018). Questions, added by Seaman’s (2008) included how the ever-changing economy, communication with management, and incentive programs affected participants’ attitudes.
12 their involvement in budgeting and in budgetary training. Part IV included multiple choice and open-ended questions pertaining to participant demographics (i.e. number of years practicing as a nurse, number of years employed at the current institution, number of years employed on the unit, and current position held). Participants also indicated their highest level of education in nursing. See Appendix B for the survey used in this survey.
Table 2. Knowledge of Cost and Cost-Conscious Practices Survey Breakdown
Knowledge of Cost and Perceptions
of Cost-Conscious Practices Survey Question Type Topic
Part I Multiple choice questions Supply and equipment costs
Part II Multiple choice questionsOpen-ended questions Likert-type scales
Perception of cost-conscious practices
Part III Multiple choice questionsLikert-type scales Application of knowledge
Part IV Multiple choice questionsOpen-ended questions Demographics
Procedures
Study approval was obtained from both the IRB through the University of North Carolina at Chapel Hill (See AppendixC) and the UNCH Nursing Research Council (See Appendix D). Upon approval, an email invitation was sent to the nurse managers of the five inpatient care units on November 5, 2018 (See Appendix E). The managers then forwarded the email describing the purpose of the study, benefits, risks, anonymous participation, and instructions to all nurses employed on their unit. See Appendix E for the specific email sent to the nurse managers for distribution.
13 disagree was located at the bottom of the page. Upon clicking the Agree button, participants agreed to participate and the survey was immediately launched. The survey was accessible to respondents for three weeks, from November 5, 2018 through November 26, 2018, during which time a modified version of the Tailored Design Method (Dillman, Smyth, & Christian, 2009) was employed to maximize study response rates. Two reminder emails were sent (at the beginning of the second and third weeks) via the nurse managers of the five inpatient care units to remind those who may still be interested in participating of the time remaining. See Appendix F and G for follow up emails sent to the nurse managers for distribution.
Prospective respondents were informed that participation was voluntary and if they did not wish to participate they could simply disregard and delete all emails pertaining to the study. Participants were free to withdraw at any time by simply exiting out of the survey. Respondents could access the survey, which was expected to take 10-15 minutes to complete, from a
computer of their choice either when they were at home or during downtime at work. Upon completing the survey, respondents were instructed to record their responses by submitting the survey by clicking the “Finish Survey” button. Submission of their responses indicated their agreement to participate in the study.
Human Subjects
Data collected for this study was done so via anonymous, confidential web link requiring no login, password, or personally identifiable information. No anticipated costs or risks to participants were identified. In remaining consistent with Seaman’s (2008) study, all findings were combined and reported in groups. Potential participants were notified that participation status would have no effect on their current or future employment or benefits.
No direct benefits or compensation was offered for participation in this study.
14 on how the data was collected. Prospective participants were given the PIs contact information for any additional questions or concerns. Results of the study will be shared with nurse managers and staff.
Data Analysis
Using Qualtrics software, an advanced filter function was utilized to remove all incomplete survey responses from the data set. Descriptive statistics were then employed to summarize and analyze results for research questions one through four. For categorical variables, frequency counts and proportions were calculated. Data were then interpreted to determine patterns, relationships, or trends.
For the fifth research question, we compared survey results from the 2008 and 2018 studies using two different statistical operations. To compare nurses’ 2008 and 2018 overall financial knowledge and application of financial knowledge to practice, two-proportion z-tests were employed to test for statistically significant differences between the two data sets. We then utilized a Pearson’s chi square test to detect any significant differences between cost-conscious practice, current involvement, and desired involvement responses from 2008 and 2018.
Results
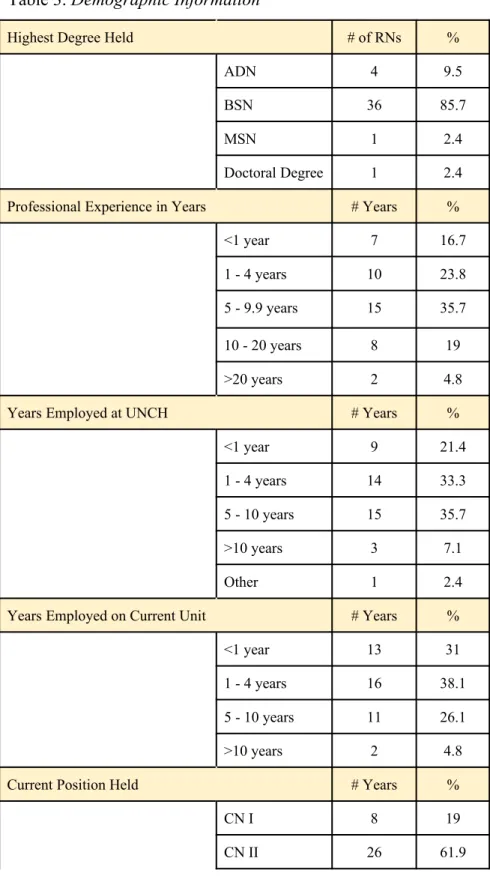
Of the estimated 148 nurses invited to participate in the survey, a total of 42 nurses completed the survey. The vast majority of respondents (85.7%) hold a Bachelor of Science in Nursing (BSN). Only 2.7% hold a Doctoral Degree in Nursing (e.g., Doctorate of Nursing Practice [DNP] or Doctor of Philosophy in Nursing [PhD]). All categories of Clinical Nurse (CN) I, CN II, CN III, and CN IV were represented, however the majority (80.9%) of
15 UNCH both ranged from four months to 38 years, and time employed on their current unit was reported to be anywhere from two months to 32 years. See Table 3for detailed demographic information.
Table 3. Demographic Information
Highest Degree Held # of RNs %
ADN 4 9.5
BSN 36 85.7
MSN 1 2.4
Doctoral Degree 1 2.4
Professional Experience in Years # Years %
<1 year 7 16.7
1 - 4 years 10 23.8
5 - 9.9 years 15 35.7
10 - 20 years 8 19
>20 years 2 4.8
Years Employed at UNCH # Years %
<1 year 9 21.4
1 - 4 years 14 33.3
5 - 10 years 15 35.7
>10 years 3 7.1
Other 1 2.4
Years Employed on Current Unit # Years %
<1 year 13 31
1 - 4 years 16 38.1
5 - 10 years 11 26.1
>10 years 2 4.8
Current Position Held # Years %
CN I 8 19
16
CN III 4 9.5
CN IV 4 9.5
Research Question 1
Nursing staff familiarity with the costs of common supplies and equipment used at the bedside. A ten-item, multiple choice survey was used to assess nurse knowledge of
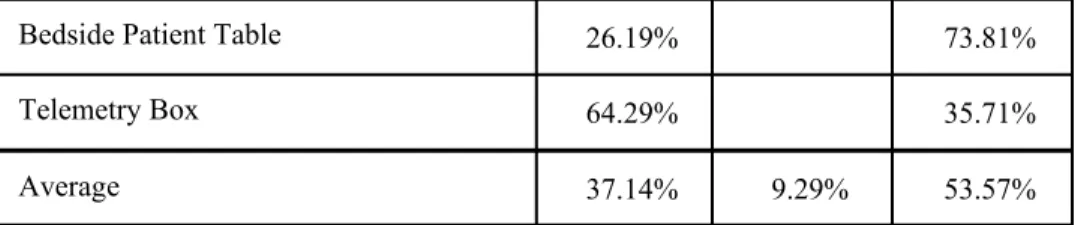
commonly used bedside supply and equipment costs. Respondents identified 37.14% of the answers pertaining to supply and equipment costs correctly. Incorrect responses were more likely to underestimate the costs of various supplies. Regarding specific supply costs, at least 50% of respondents selected the correct cost of cardiac-related supplies, such as disposable stethoscopes, EKG leads, and telemetry boxes. However, fewer than 30% of participants correctly identified the cost of more general supplies, such as 4x4 or 3x3 gauze, disposable SpO2 sensor, activity aprons, and bedside tables. Refer to Table 4 for detailed results from Part I of the survey. Table 4. Results - Part I of Survey
Question Percent
Correct
Percent High
Percent Low
“Boat” or Package of sterile 4x4 Gauze 11.9% 88.095%
Sterile 3x3 Gauze – 2 Gauze pads per
pack 28.57% 4.76% 66.66%
Blue Disposable Stethoscope 52.38% 47.62%
Disposable SpO2 Sensor 26.19% 73.81%
Busy Apron or Activity Apron 38.1% 61.9%
An IV pump (Baxter Sigma Spectrum
Pumps) 33.33% 66.66%
A SpO2 Cable that connects to bedside
Philips monitor 40.48% 59.52%
5-lead grabbers (EKG Leads) that
17
Bedside Patient Table 26.19% 73.81%
Telemetry Box 64.29% 35.71%
Average 37.14% 9.29% 53.57%
Research Question 2
Nursing staff perception of their overall knowledge of supply and equipment costs.
The next part of the survey required nurses to rate their overall knowledge of supply and
equipment costs. A 5-point Likert-type scale was used to rate their overall knowledge of supply and equipment costs from no or minimal knowledge to an expert level of knowledge. None of the 42 respondents rated their overall knowledge at an expert level, while 14% of respondents reported no knowledge or minimal knowledge of supply and equipment costs.
Research Question 3
Nurses’ application knowledge of supply and equipment costs. Here, participants were asked about the frequency with which they apply their financial knowledge in their everyday clinical practice. Approximately 45% of respondents reported applying their knowledge of cost-conscious practices into their clinical practice at least a few times a week. Thirty-three percent reported using this knowledge once to a few times per month, and nearly 12% of respondents indicated they never apply their knowledge into clinical nursing practice. See Table 5 for detailed response information.
Table 5. Results - Application of Financial Knowledge to Clinical Practice
Daily Few times aweek Few times amonth About once amonth Less than oncea month Never
Response
Percent 23.81% 21.42% 26.19% 7.14% 9.52% 11.9%
18
Nursing staff perceptions of cost-conscious practices in their daily work and
decision-making. Using a 4-point Likert scale, participants were prompted to indicate their level of agreement or disagreement with various cost-conscious nursing practice and decision-making practices statements. Possible scores range from 15 to 60, with 15 indicating a more negative attitude towards effectiveness and 60 indicating a positive attitude towards
cost-effectiveness. The average BHNAS for the current study was 41, indicating a slight trend towards a positive attitude of cost-conscious practices.
Most respondents (76%) agreed cost-effective nursing practices and procedures would benefit them personally and 90% of respondents agreed cost-effective nursing practices and procedures would benefit the nursing profession as a whole. All participants agreed cost-effective practices would benefit the hospital, and approximately 86% of respondents agreed hospitals should be concerned with making or losing money. Roughly half of respondents felt that cost-effectiveness should not influence the way in which nurses provide patient care, but more than 80% felt the implementation of cost-effective practices in the future would not
decrease the quality of patient care. It is interesting to note that 81% of respondents reported that rewards exist for nurses who use cost-effective practices on their unit. However, 64% of
participants reported that the unit manager failed to keep them up to date on unit finances, revealing a gap between incentives and the knowledge necessary to capitalize on them. Table 6 displays the statements included in Part II of the survey, the number of respondents who chose each response, and the percentage of participants that correlates with that number.
Table 6. Results - Part II of Survey
Strongly
19 Cost-effective nursing practices and
procedures will benefit me personally.* 2 or 4.76 % 8 or 19.05% 25 or 59.52 % 7 or 16.67%
Operating a nursing unit in order to
make a profit is wrong.* 8 or 19.05% 12 or 28.57% 15 or 35.71 % 7 or 16.67%
Cost-effective nursing practices and procedures will result in a decrease in
quality of patient care.* 13 or 31.0% 21 or 50.0% 5 or 11.90% 3 or 7.14%
Cost-effective nursing practices and procedures will benefit the nursing
profession as a whole.* 2 or 4.76% 2 or 4.76% 29 or 69.05% 9 or 21.43%
Cost-effectiveness should not influence the way in which nurses provide patient
care.* 2 or 4.76% 19 or 45.24% 10 or 23.81% 11 or 26.19%
Cost-effective nursing practices and
procedures will benefit patients.* 2 or 4.76% 9 or 21.43% 22 or 52.38% 9 or 21.43%
Hospitals should not be concerned with
making or losing money.* 15 or 35.71% 21 or 50.0% 6 or 14.29% 0 or 0%
Cost-effective nursing practices and
procedures will benefit the hospital. 0 or 0% 0 or 0% 24 or 57.14% 18 or 42.86%
The current economic climate has made me more conscious of the costs of
supplies and equipment on my unit. 2 or 4.76% 16 or 38.10% 18 or 42.86% 6 or 14.29%
The peaks and valleys of the economy have made me more aware of using cost-effective nursing practices on my unit.
2 or 4.76% 16 or 38.10% 18 or 42.86% 6 or 14.29%
Cost-effective nursing practices and
procedures will benefit my unit. 0 or 0% 5 or 11.90% 28 or 66.67% 9 or 21.43%
Knowledge of supply and equipment costs on my unit influences how I
practice. 1 or 2.38% 9 or 21.43% 26 or 61.90% 6 or 14.29%
There are rewards for nurses who use
cost-effective practices on my unit. 13 or 30.95% 21 or 50.0% 7 or 16.67% 1 or 2.38 %
My manager keeps me up to date on
20 Concerns about the peaks and valleys of
the economy have raised discussion of cost-effective nursing practices on my unit.
5 or 11.90% 19 or 45.24% 16 or 38.10% 2 or 4.76 %
Total 73 or 11.59% 199 or 31.59% 261 or 49.25% 97 or 15.40%
Question 21a and 21b of the survey assessed respondents’ perception of their current and desired involvement in unit-level budgetary issues. Participants were asked to rate their current and desired involvement in financial decision-making along a 4-point Likert-type scale.
Respondents selected from the following answer choices: not at all (1), a little (2), some (3), and a great deal (4).
Most (66%) of the nurses surveyed reported no current involvement in determining their unit's annual budget, although 74% report at least 'a little' desire to be involved in the process. Over half of respondents reported having no current involvement in formal or informal
discussions regarding cost-effective practices to consider or adopt on their current unit. Just over 59% of participants reported having no current involvement in providing input on staffing decisions that impact unit costs, however, 76% reported a least some desire for involvement. Almost all participants had a desire to be involved to some extent in discussing ways to minimize the waste of resources on their unit, but only half reported current active involvement in this process. Refer to Table 7 for more detailed information.
Table 7. Results - Questions 21a and 21b of Survey
Currently Involved Wish to be Involved
Not at all A little Some A greatdeal Not at all A little Some A great deal
Determining your unit’s annual budget (e.g. identifying supplies or equipment needed or wanted on the
28 or
21 unit) Acquiring staffing resources needed to provide care to patients
19 or
45.24% 23.81%10 or 16.67%7 or 16.67%7 or 26.19%11 or 14.29%6 or 40.48%17 or 9 or 21.43%
Evaluating supply and equipment costs, and/or the purchase of other items for my unit 11 or 26.19% 11 or 26.19% 14 or 33.33% 7 or 16.67% 11 or 26.19% 11 or 26.19% 14 or
33.33% 7 or 16.67%
Making unit-level financial decisions about hiring or bringing more staff onto the unit
27 or
64.29% 19.05%8 or 9.52%4 or 9.52%4 or 38.10%16 or 26.19%11 or 23.81%10 or 6 or 14.29%
Making unit-level financial decisions about purchasing supplies or equipment 26 or
61.90% 26.19%11 or 4.76%2 or 9.52%4 or 26.19%11 or 23.81%10 or 38.10%16 or 6 or 14.29%
Discussing cost-effective practices to consider or adopt (formally or informally) 22 or
52.38% 26.19%11 or 14.29%6 or 9.52%4 or 19.05%8 or 19.05%8 or 40.48%17 or 23.81%10 or
Providing input on staffing decisions that impact unit costs 25 or
59.52% 14.29%6 or 16.67%7 or 11.90%5 or 26.19%11 or 26.19%11 or 30.95%13 or 8 or 19.05%
Acquiring supplies, equipment, or other items needed to care for patients
15 or
35.71% 38.10%16 or 11.90%5 or 16.67%7 or 16.67%7 or 33.33%14 or 28.57%12 or 23.81%10 or
Discussing ways to minimize the waste of
21 or 50% 13 or
22 resources on
the unit
Research Question 5
Differences between 2008 and 2018 nurse perceptions of costs and cost-effective practices. Demographic data remained largely constant between both the 2008 and 2018 cohort. CN I and CN II categories accounted for 74% of participants in Seaman's (2008) study compared to 80.9% of the same categories in the current study. In addition, the current study only surveyed nurses, while Seaman (2008) also included Nursing Assistants as well as Clinical Support
Technicians.
Supply and equipment costs. Surprisingly, fifty-three percent of both cohorts underestimated supply and equipment costs. Beyond that, both cohorts had similar response scores, with the averages of the 2018 cohort (37%) slightly higher than that in 2008 (34%) (Seaman, 2008). Even with a slightly higher average of correct answers amongst the 2018 cohort, the difference in scores between the 2008 and 2018 cohorts (p = .72786) were non-significant (p > .05), underscoring an persistent knowledge deficit regarding supply and equipment costs.
Application of cost-conscious practices. A slightly higher percentage (54%) of Seaman’s (2008) respondents reported applying their knowledge of cost-conscious practices into their clinical practice at least a few times a week, versus 45% of the most recent cohort reporting the same. Only 7% of the 2008 cohort indicated they never apply their knowledge into practice, a slightly lower percentage than that reported by the 2018 cohort (~12%).
23 2008). Both scores indicate a more positive attitude towards cost-effective nursing practices, however, the attitudes of the nurses surveyed in 2008 was slightly more positive.
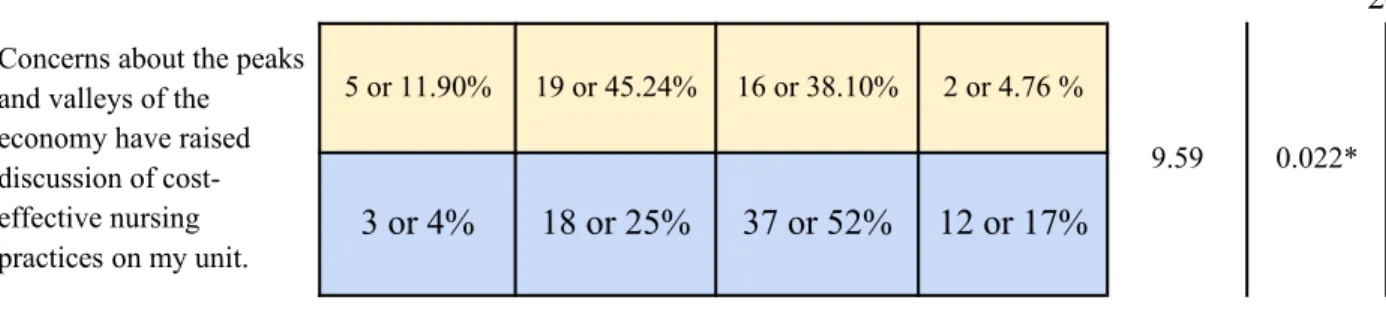
Only five the 15 items used to gauge participants’ perceptions of cost-effective practices in their daily work and decision-making yielded statistically significant differences between the 2008 and 2018 data. Over half (53%) of the 2018 cohort responded it was wrong to operate a nursing unit in order to make a profit, whereas only 27% the 2008 cohort responded the same (Seaman, 2008). The majority of nurses from both cohorts (2008 = 82%; 2018 = 57.15%) reported that the current economic climate made them more conscious of the costs of supplies and equipment on their units. Far more nurses in 2008 (66%) reported being kept up to date on unit finances by their manager versus only 36% in the 2018 cohort. Nurses in 2018 (57%) tended to disagree that the shifting economy raised discussion of cost-effective nursing practices, whereas 69% of nurses in 2008 reported that the economy did raise these discussions on their unit (Seaman, 2008). See Table 8 for significant findings.
Table 8. Significant Findings Between 2008 (blue) and 2018 (yellow) Responses
Strongly Disagree
Disagree Agree Strongly
Agree
Chi Square
p-value
Operating a nursing unit in order to make a profit is wrong.*
8 or 19.05% 12 or 28.57% 15 or 35.71 % 7 or 16.67%
10.3565 0.015* 13 or 18% 39 or 55% 16 or 23% 3 or 4%
Cost-effective nursing practices and procedures will benefit the nursing profession as a whole.*
2 or 4.76% 2 or 4.76% 29 or 69.05% 9 or 21.43%
7.877 .048* 2 or 3% 6 or 9% 42 or 59% 41 or 58%
The current economic climate has made me more conscious of the costs of supplies and equipment on my unit.
2 or 4.76% 16 or 38.10% 18 or 42.86% 6 or 14.29%
8.67 0.034*
1 or 1% 12 or 17% 48 or 68% 10 or 14%
My manager keeps me up to date on unit finances.
6 or 14.29% 21 or 50.0% 12 or 28.57% 3 or 7.14%
24 Concerns about the peaks
and valleys of the economy have raised discussion of cost-effective nursing practices on my unit.
5 or 11.90% 19 or 45.24% 16 or 38.10% 2 or 4.76 %
9.59 0.022*
3 or 4% 18 or 25% 37 or 52% 12 or 17%
Participants in both surveys were asked to indicate how they obtained their knowledge of cost-effective nursing practices. In 2008, staff meetings or other unit discussions were
overwhelmingly reported (93%) to be the primary knowledge sources (Seaman, 2008). Nearly 36% of the 2018 cohort reported gaining their knowledge of cost-effective practices in other ways, including formal and continuing education. See Table 9 for more in-depth information regarding the 2018 cohort’s sources of financial knowledge.
Table 9. Sources of Financial Knowledge (2018)
Formal education programs 7 or 16.67%
Continuing education programs 3 or 7.14%
Informal educational offerings at work 11 or 26.19%
Unit staff meetings or other unit discussions 18 or 42.86%
Personal research 5 or 11.90%
Hospital/unit orientation 2 or 4.76%
Other (please specify) 2 or 4.76%
Discussion
25 central finding is that none of the three key elements studied as part of the survey has improved by any significant metric. None of the nurses surveyed considered themselves as experts in cost-awareness, and less than half found themselves applying financial knowledge to their clinical practice on a regular basis. Still, consistent with the 2008 findings, nurses continued to view cost-conscious practices positively, and agreed implementation would help themselves, the hospital, and the nursing profession as a whole without sacrificing quality of care (QOC). Finally, while most nurses reported no participation in annual budgeting, three out of four expressed a desire to be included. Little has changed in the decade since the 2008 study, thus, the most recent findings present a strong case for more action and education. Not only could steps be taken to address the lack of cost-awareness among nurses, but also to capitalize on nurse interest in learning and practicing cost-conscious behavior.
26 Just as this study indicates nurses who work at UNC in the cardiac service line continue to demonstrate largely poor cost-awareness, their positive attitudes towards cost-conscious practices have stood the test of time. Both the current and the parent-study showed a general amiability towards factoring costs into everyday nursing practice, despite a general lack of practice in implementation. As stated above, most nurses agreed that implementing more cost-effective practices would benefit themselves, the profession, and the hospital. In practice, though, nearly half of the 2018 cohort reported rarely or never using what financial knowledge they possess. In comparing the current cohort with the 2008 cohort, application of financial knowledge has not increased, so not only has cost-awareness not improved, but nurses have not applied what knowledge they have with any greater frequency. Despite both cohorts
overwhelmingly agreeing that effective practices would not decrease quality of care, cost-effective practices are rarely applied on a day-to-day basis. Further research should examine the disparity between nurses’ positive attitudes toward cost-effective practices and the frequency with which they apply their knowledge to clinical practice.
While most results remained consistent with those from the 2008 study, the current results do suggest one significant difference: Sources of nurses’ financial knowledge are more diverse today than they were ten years ago. Despite the shift in how nurses obtained their financial knowledge, though, initiatives to improve cost-awareness have not been effective as financial competencies continue to fall short.
Implications for Nursing
27 leaders to address existing financial knowledge gaps, develop cost-effectiveness education programs, and research the effectiveness of educational initiatives implemented. Additionally, the replication study design could aid other units within the UNCH institution in evaluating the financial literacy of their nursing staff. Future research should expand the study population to examine nurses’ financial literacy in different units, institutions, and in other areas of the country to better illuminate broader implications for the nursing profession. Additionally, financial literacy curriculum in existing nursing curricula should be examined to determine whether financial literacy education can be delivered more effectively.
In the current study, the vast majority of respondents report the belief that cost-effective practices would not result in a decrease in the QOC. Many nurses said incentives exist for cost-conscious nursing, but that unit managers do not always clarify for and update nurses on unit finances. Results of this study prompt a fundamental question: How can nurses demonstrate cost-effectiveness in their clinical practice if they lack the necessary financial competencies needed to make cost-conscious decisions? Furthermore, why, if most nurses have the desire to be involved in unit-level budgetary concerns, are they not engaging or have access to budgetary meeting information?
Limitations
28 Given the 10-year gap between studies and the fact that most respondents reported 10 or fewer years employed on their current unit, any bias due to prior exposure is unlikely.
Bias concerning healthcare costs should also be considered. Only three price options were listed for each item in the multiple choice portion of Part I of the survey, giving participants a 33% chance of guessing each answer correctly. Moreover, the highest cost option was the correct cost for eight of the ten items on that same portion of the survey. Therefore, respondents could have earned a score of 80% by intentionally - or arbitrarily - selecting the highest cost throughout that section. Additionally, limitations may have existed due to using secondary data as I did not have control over the accuracy of the data collection and reporting of that data from 2008.
Lastly, in error, one survey question was omitted in the 2018 survey. Question 21, seen in Table 6 above, should have included an additional question asking nurses to rate their current and desired involvement in discussing ways to minimize costs on the unit.
Conclusion
As the largest discipline in the hospital setting and the primary provider of patient bedside care, nurses have great potential to significantly impact cost-containment initiatives. The current study gives a glimpse into nurses’ subpar financial literacy, likely limiting the savings impact these nurses could have on this institution’s bottom line. Consistent with the results from cited studies, the findings of this research endorse the evaluation of educational programs, departmental guidelines, and the distribution of cost information to frontline HCPs in an effort to improve cost-awareness among this population.
29 Berwick D. M. (2008). The triple aim: care, health, and cost. Health affairs (Project Hope),
27(3), 759-769. Doi: 10.1377/hlthaff.27.3.759
Brandt, M. J., Ijzerman, H., Dijksterhuis, A., Farach, F. J., Geller, J., Giner-Sorolla, R.,…Veer, A. V. (2014). The Replication Recipe: What Makes for a Convincing Replication?
Journal of Experimental Social Psychology,50, 217-224. doi:10.1016/j.jesp.2013.10.005 Caroselli, C. (1996). Economic awareness of nurses: Relationship to budgetary control. Nursing
Economic$, 14(5), 292-298.
Clancy, M., Murphy, M. (2014). Laboratory test costs: attitudes and awareness among staff in a regional hospital. Irish Medical Journal, 107(1), 8-11. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/
Dillman, D.A., Smyth, J.D., & Christian, L.M. (2009). Internet, mail and mixed-mode surveys: The tailored design method (3rd ed.). New York: Wiley.
Douglas, K. (2010). Taking action to close the nursing-finance gap: Learning from success.
Nursing Economics, 28(4), 270-2. Retrieved from http://libproxy.lib.unc.edu/login?url= https://search-proquest-com.libproxy.lib.unc.edu/docview/746743021?accountid=14244 Gould, D. (2002). Using replication studies to enhance nursing research. Nursing Standard
(through 2013), 16(49), 33-6. Retrieved from http://libproxy.lib.unc.edu/login?url= https://search-proquest-com.libproxy.lib.unc.edu/docview/219795145?accountid=14244 Hadjipavlou, M., & Bailey, C. R. (2010). The price of everything and the value of nothing': Cost
30 Hernu, R., Cour, M., & Argaud, L. (2017). Are nurses ready to help improve cost-effectiveness?
A multicentric national survey on knowledge of costs among ICU paramedical staff.
Intensive Care Med, 44, 663-664. https://doi-org.libproxy.lib.unc.edu/10.1007/s00134-017-5032-5
Heydari, A., Mazloom, R., Najara, A.V., Bakhshi, M. (2015). Awareness and Performance of Iranian Nurses with Regard to Health Economics: A Cross-Sectional Study. North American Journal of Medical Sciences, 7(9), 384-389. Doi: 10.4103/1947-2714.166214 Kynaston, J.W.F, Smith, T., Batt, J. (2017). Cost awareness of disposable surgical equipment
and strategies for improvement: cross sectional survey and literature review. Journal of Perioperative Practice, 27(10) , 211-216. https://doi.org/10.1177/175045891702701002 Muma, J. R. (1993). The Need for Replication. Journal of Speech, Language, and Hearing
Research, 36(5), 927-930. doi:10.1044/jshr.3605.927
Owens, R., & Cronin, S. N. (1998). Nurses' attitudes towards cost-effectiveness and quality of care. Cost & Quality Quarterly Journal, 4(3), 18-22.
Seaman, C. (2008). Nursing Staff Knowledge of Cost and Budgetary Control (Unpublished masters research paper). University of North Carolina, Chapel Hill.
UNC Medical Center. (n.d.). Retrieved January 30, 2019, from
https://www.uncmedicalcenter.org/uncmc/hospitals-locations/profile/unc-medical-center/
31
From: Hobson, Charles J <[email protected]>
Sent: Thursday, August 23, 2018 6:36 PM
To: St.Clair, Brannin
Subject: Re: Permission Request
Good Evening Ms. St. Clair,
Please consider this email as permission to use the Blaney/Hobson Nursing Attitude Scale. Good luck with your research.
Regards, Charlie
Charles J. Hobson, Ph.D. Professor, School of Business Indiana University Northwest (219) 980-6903
Appendix B
32 I am writing to invite you to participate in a research study that I am conducting as part of my bachelor’s honors project at the University of North Carolina at Chapel Hill, in the School of Nursing. Your participation in this study would involve completing a short survey. The study is about nursing staff knowledge of cost and budgetary issues. Please read this form carefully and ask any questions you may have before agreeing to take part in the study.
What the study is about: The purpose of this study is to gain insight into how familiar nursing staff members are with the cost of supplies and equipment commonly used at the bedside. The study uses an online survey to gather your views on general supply and equipment costs, your perceptions of cost-effective practices, the degree to which you are and want to be involved in budget-related decisions, and any education you may have received about your unit-level costs and budgets.
What we will ask you to do: You will be asked to answer a series of questions, including multiple choice and short answer questions.
Risks and benefits: We do not anticipate any risks to you participating in this study. There are no benefits or compensation to participating in this study.
Your answers will be confidential. The records of this study will be kept private. There is no way your name can be associated with your answers. All information you provide will be combined with others, and be reported only in groups. In any report we make public we will not include any information that will make it possible to identify you. Research records will be kept on a password protected computer; only the researchers will have access to the records.
Taking part is voluntary: Taking part in this study is completely voluntary. If you decide not to complete the survey, it will not affect your current or future employment. If you start the survey but decide not to complete it, you are free to withdraw at any time.
If you have questions: The researchers conducting this study are Brannin St. Clair, Dr. Maureen Baker, PhD, RN and Cheryl Jones, PhD, RN, FAAN. You may contact Brannin at 303-717-7175 or [email protected], Dr. Maureen Baker at [email protected], or Dr. Cheryl Jones at [email protected] with any questions you may have.
33 Directions: Please select the answer that you believe best represents the cost of each item listed below. Here, “cost” is defined as the price per unit that the nursing unit is charged by central distribution for a particular item.
1. “Boat” or Package of sterile 4x4 Gauze (i.e., the cost per “boat” or package) a. 43 cents
b. $1.08 c. $1.88
2. Sterile 3x3 Gauze (2 gauze pads per pack) a. 51 cents
b. $1.22 c. $2.03
3. Blue Disposable Stethoscope a. $1.07
b. $2.14 c. $2.78
4. Disposable SpO2 Sensor a. $3.06
b. $5.26 c. $7.30
5. Busy Apron or Activity Apron a. $6.35
b. $11.83 c. $19.11
Directions: Please select the answer that you believe best represents the cost of each item listed below. Here, “cost” is defined as the price per unit that the nursing unit or hospital pays the company to purchase each of these items.
34 a. $1,236
b. $2,250 c. $5,000
2. A SpO2 Cable that connects to bedside Philips Monitor a. $79
b. $116 c. $180
3. 5-lead grabbers (EKG Leads) that connect a patient to a telemetry box a. $54
b. $80 c. $112
4. Bedside Patient Table a. $343
b. $521 c. $646 5. Telemetry Box
a. $1,636 b. $2,147 c. $3,067
Part II
Directions: Please indicate how much you agree or disagree with the following statements about the use of cost-effective nursing practices.
Strongly Disagree Disagree Agree Strongly Agree
Cost-effective nursing practices and procedures will benefit me personally.*
35 make a profit is wrong.*
Cost-effective nursing practices and procedures will result in a decrease in quality of patient care.*
Cost-effective nursing practices and procedures will benefit the nursing profession as a whole.*
Cost-effectiveness should not influence the way in which nurses provide patient care.*
Cost-effective nursing practices and procedures will benefit patients.*
Hospitals should not be concerned with making or losing money.*
Cost-effective nursing practices and procedures will benefit the hospital.
The peaks and valleys of the economy have made me more conscious of the costs of supplies and equipment on my unit.
The peaks and valleys of the economy have made me more aware of using cost-effective nursing practices on my unit.
Cost-effective nursing practices and procedures will benefit my unit.
Knowledge of supply and equipment costs on my unit influences how I practice.
There are rewards for nurses who use cost-effective practices on my unit.
My manager keeps me up to date on unit finances.
36 * These statements were taken directly from the Blaney/Hobson Nursing Attitude Scale.
Permission to use this survey was granted by Dr. Charles J. Hobson (C. Hobson, personal communication, August 23, 2018).
Please identify any factors that encourage or facilitate the use of cost-effective practices on your unit:
______________________________________________________________________________ Please identify any factors that discourage or put up barriers to the use of cost-effective practices on your unit:
______________________________________________________________________________
Part III
1. On a scale of 0-4 please rate your overall knowledge of supply and equipment costs commonly used on your unit.
No/minimal knowledge A great deal/expert knowledge 0 1 2 3 4
2. Please rate the frequency with which you apply your knowledge of supply and equipment costs commonly used on your unit:
a. Daily
b. A few times a week c. A few times a month d. About once a month e. Less than once a month f. Never
For each item in the table below, please indicate: A) the extent to which you are currently involved in various budgeting related activities; and B) the extent to which you would like to be involved in various budgeting-related activities.
Currently Involved Wish to be Involved
A great deal
Some A
little Not at all
A great deal
Some A
37 Determining your unit’s annual budget (e.g. identifying supplies or equipment needed or wanted on the unit)
Acquiring staffing resources needed to provide care to patients
38 Providing input
on staffing decisions that impact unit costs
Acquiring supplies, equipment, or other items needed to care for patients
Discussing ways to minimize the waste of resources on the unit
From the list below please indicate how you gained your knowledge of cost effective nursing practice. Please select all that apply.
a. Formal education program b. Continuing education program
c. Informal educational offerings offered at work d. Unit staff meetings or other unit discussions e. Personal research
f. Hospital/unit orientation
g. Other (please specify) __________________________________
Part IV
Demographics. Please answer the following questions to help us better understand the context of nursing practice and the practice environment.
39 4. Please indicate your current position:
a. Clinical Nurse (CN) I b. Clinical Nurse (CN) II c. Clinical Nurse (CN) III d. Clinical Nurse (CN) IV
5. Please indicate your highest level of education in nursing: a. Diploma in Nursing
b. Associate Degree in Nursing
c. Bachelor of Science in Nursing (BSN) d. Master of Science in Nursing (MSN)
40
Appendix C IRB Approval To: Brannin St. Clair, Dr. Maureen Baker
School of Nursing
From: Office of Human Research Ethics Date: 10/18/2018
RE: Notice of IRB Exemption
Exemption Category: 2.Survey, interview, public observation Study #: 18-2213
Study Title: Nursing Staff Knowledge of Cost and Budgetary Control: A Replication Study This submission has been reviewed by the Office of Human Research Ethics and was determined to be exempt from further review according to the regulatory category cited above under 45 CFR 46.101(b).
Study Description:
Purpose: The purpose of this study is to examine and compare nursing staff knowledge of supply and equipment costs, as well as nursing staff perceptions of budgetary control practices and concerns between 2008 and 2018.
Participants: Registered nurses employed within the Center for Heart and Vascular Care at UNC Hospitals. The Center for Heart and Vascular Care department includes five inpatient units: Cardiac Intensive Care Unit, Cardiothoracic Intensive Care Unit, 3 Anderson, 4 CTSU, and 5 Anderson.
41
Investigator’s Responsibilities:
If your study protocol changes in such a way that exempt status would no longer apply, you should contact the above IRB before making the changes. There is no need to inform the IRB about changes in study personnel. However, be aware that you are responsible for ensuring that all members of the research team who interact with subjects or their identifiable data complete the required human subjects training, typically completing the relevant CITI modules.
The IRB will maintain records for this study for 3 years, at which time you will be contacted about the status of the study.
The current data security level determination is Level I. Any changes in the data security level need to be discussed with the relevant IT official. If data security level II and III, consult with your IT official to develop a data security plan. Data security is ultimately the responsibility of the Principal Investigator.
Please be aware that approval may still be required from other relevant authorities or
"gatekeepers" (e.g., school principals, facility directors, custodians of records), even though the project has determined to be exempt. .
CC:
Cheryl Jones, School of Nursing IRB Informational Message - please do not use email REPLY to this address
42
Appendix D
NRC Approval
October 11, 2018 To: Brannin St. Clair
Dear Brannin,
Thank you for submitting your proposal to the Nursing Research Council (NRC) at UNCH. Congratulations, the NRC has approved your proposal, Nursing Staff Knowledge of Cost and Budgetary Control, a Replication Study. Dr. Cheryl Jones will be the NRC contact to assist you. You may reach her at [email protected]. If you have any questions, please do not hesitate to contact either Dr. Jones or Rebecca Shaw, the Chair of the NRC.
Thank you for the opportunity to review and be the site for your project. We look forward to hearing back from you with results at the completion of your project. Please submit the Final Report Form to [email protected] when your work is concluded. We would also enjoy having you present at an NRC meeting to share your findings.
We wish you the best.
Kind Regards,
Rebecca Shaw, MA, BSW, BSN, RN-BC| CN III Chair, Nursing Research Council
[email protected] Mary Kime RN, MSN
43
Appendix E
Subject: Nursing Research Study – Nursing Staff Knowledge of Cost & Budgetary Control: A Replication Study
Hi all,
First, allow me to introduce myself to those of you who may not know me. My name is Brannin St. Clair and I am a fourth year nursing student. I am currently finishing my BSN and am working on my senior honors thesis. My research is focused on nursing staff knowledge of cost and budgetary control. With the assistance of Dr. Maureen Baker and Dr. Cheryl Jones, I have replicated a survey in initially conducted in 2008 by Christa Seaman DNP, RN, NE-BC, CCRN to assess the knowledge of registered nurses (RNs) regarding unit-level costs and supplies, and the perceptions of RNs about cost-effective practices. I am writing now to ask each registered nurse member of the Center for Heart and Vascular Care (CICU, CTICU, 3 Anderson, CTSU, and 5 Anderson) to take a moment to take part in this research study by completing the online survey.
Your participation in this research study is voluntary. The survey is online and your answers will be kept confidential. There is no user ID or password to access this survey therefore your
answers cannot be directly linked to you. We do not anticipate any risks to you for participating in this study. Any information you provide will be combined with the responses provided by others, and reported only in groups. There are no benefits or compensation to participating in this study. Taking part in this study is completely voluntary. If you decide not to take part in this study it will not affect your current or future employment and you may delete this email and any subsequent emails regarding this study. If you decide to take part in this study but decide later that you do not want to continue, you are free to withdraw at any time.
To access the survey, please point your web browser to the secure website at
44 This study has been approved by the Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill. If you have questions about your rights as a study participant, you may contact the IRB at 919-966-3113 or by email at [email protected]. If you have any questions about the research study, please feel free to contact me, Brannin St. Clair, at 303-717-7175 or [email protected]. You may also contact my faculty advisor, Dr. Dr. Maureen Baker at [email protected], Dr. Cheryl Jones, at [email protected], or Christa Seaman DNP, RN, NE-BC, CCRN, at [email protected].
The results of this study will provide information regarding your knowledge of costs, perceptions of cost and budgetary control, and current or desired involvement in unit-level financial decision making. The results of this study may be used to develop future educational offerings and guide future study interventions to increase nursing staffs’ awareness of cost.
Thank you!
Brannin St. Clair, UNC-Chapel Hill, BSN | Class of 2019
Appendix F
45 Hi all,
I just wanted to send out a quick email to thank everyone who has participated in the research study (Nursing Staffs’ Knowledge of Cost and Budgetary Control: A Replication Study). If you have not yet had a chance to complete the survey, I just wanted to let you know that the survey will remain open until November 26, 2018. If you are interested in participating in the survey, you may access the survey by pointing your web browser to
https://unc.az1.qualtrics.com/jfe/form/SV_d0CarJJbBaPJpJz. If you are not interested in participating in the survey, please feel free to delete this email.
Please remember that any information you provide will be confidential, and your identity will be protected at all times.
This study has been approved by the Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill. If you have questions about your rights as a study participant, you may contact the IRB at 919-966-3113 or by email at [email protected]. Please feel free to contact me at [email protected] or 303-717-7175. You can also contact my faculty advisor, Dr. Maureen Baker at [email protected], Dr. Cheryl Jones, at
[email protected], or Christa Seaman DNP, RN, NE-BC, CCRN at [email protected].
Thank you!
Brannin St. Clair, UNC-Chapel Hill, BSN | Class of 2019
Appendix G
46 Hi all,
I just wanted to send out a quick email to thank everyone who has participated in the research study (Nursing Staffs’ Knowledge of Cost and Budgetary Control: A Replication Study). If you have not yet had a chance to complete the survey, I just wanted to let you know that the survey will remain open until November 26, 2018. If you are interested in participating in the survey, you may access the survey by pointing your web browser to
https://unc.az1.qualtrics.com/jfe/form/SV_d0CarJJbBaPJpJz. If you are not interested in participating in the survey, please feel free to delete this email.
Please remember that any information you provide will be confidential, and your identity will be protected at all times.
This study has been approved by the Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill. If you have questions about your rights as a study participant, you may contact the IRB at 919-966-3113 or by email at [email protected]. Please feel free to contact me at [email protected] or 303-717-7175. You can also contact my faculty advisor, Dr. Maureen Baker at [email protected], Dr. Cheryl Jones, at
[email protected], or Christa Seaman DNP, RN, NE-BC, CCRN at [email protected].
Thank you!