Clinical Practice Guidelines
Urinary Incontinence
CareMore Quality Management
CareMore Health System adopts Clinical Practice Guidelines for the purpose of improving
health care and reducing unnecessary variations in care.
The guidelines are evidence-based, sourced from recognized organizations, approved by the
CareMore Quality Management Committee, disseminated to CareMore healthcare providers,
reviewed at least every two (2) years and updated as needed.
The Clinical Practice Guidelines in this document are considered essential to healthcare for the
member population served by CareMore.
April 15, 2013 ◆
Volume 87, Number 8
www.aafp.org/afp American Family Physician543
Diagnosis of Urinary Incontinence
CHRISTINE KHANDELWAL, DO, and CHRISTINE KISTLER, MD, MASc
University of North Carolina, Chapel Hill, North Carolina
U
rinary incontinence affects
mil-lions of persons, and the
preva-lence increases with age. Roughly
20 million American women and
6 million American men experience urinary
incontinence at some time in their lives.
1Although women report incontinence
more often than men,
2,3after 80 years of
age, both sexes are affected equally.
3Women
commonly experience stress or urge
incon-tinence (i.e., overactive bladder), or a
com-bination of the two, with approximately
equal frequency.
4In men, prostate problems,
which lead to overflow incontinence, and
their treatments, which lead to stress
incon-tinence, are the most common causes.
5Despite what many patients believe,
uri-nary incontinence is not a normal result of
aging. It is a pathologic condition that affects
quality of life. Patients who have incontinence
are more likely to have depression, limited
social and sexual function, and dependence
on caregivers.
3,6,7Guidelines for diagnosis
and treatment of urinary incontinence were
published in 2012 by the American Urological
Association.
8This article reviews the
diagno-sis; a separate article in an upcoming issue of
AFP reviews management options in women.
Classification
Incontinence can be classified as
tran-sient or chronic.
5,9Transient incontinence
is urinary leaking that spontaneously
reverses after the underlying cause is
resolved.
10Chronic urinary incontinence
does not typically resolve spontaneously,
and is classified into five types: stress, urge,
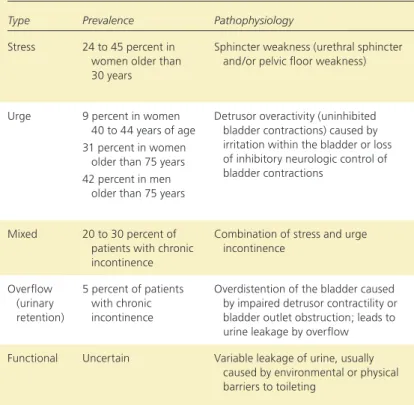
mixed, overflow, or functional.
2,11Character-istics of each type are shown in Table 1.
9,12-14Stress incontinence is caused by sphincter
weakness, which leads to ineffective
func-tion. It is the most common cause of urinary
incontinence in younger women and the
sec-ond most common cause in older women.
15It also occurs in men after prostate surgery.
Urge incontinence is a result of detrusor
overactivity, and can be further divided into
two subtypes: sensory (a result of local
irri-tation, inflammation, or infection within the
bladder) or neurologic (most often caused by
loss of cerebral inhibition of detrusor
con-tractions).
12Aging increases the prevalence
of urge and stress incontinence, and the two
often coexist, leading to mixed incontinence.
This occurs in about one-third of adults who
have incontinence.
9,15Overflow incontinence is caused by
impaired detrusor contractility, bladder
out-let obstruction, or both, resulting in
overdis-tension of the bladder.
2,5Chronic overflow
incontinence is common in men because
of prostatic hyperplasia, but it is
uncom-mon in women.
15Functional incontinence is
caused by cognitive, functional, or mobility
Urinary incontinence is common, increases in prevalence with age, and affects quality of life for men and women.
The initial evaluation occurs in the family physician’s office and generally does not require urologic or gynecologic
evaluation. The basic workup is aimed at identifying possible reversible causes. If no reversible cause is identified, then
the incontinence is considered chronic. The next step is to determine the type of incontinence (urge, stress, overflow,
mixed, or functional) and the urgency with which it should be treated. These determinations are made using a patient
questionnaire, such as the 3 Incontinence Questions, an assessment of other medical problems that may contribute to
incontinence, a discussion of the effect of symptoms on the patient’s quality of life, a review of the patient’s completed
voiding diary, a physical examination, and, if stress incontinence is suspected, a cough stress test. Other components
of the evaluation include laboratory tests and measurement of postvoid residual urine volume. If the type of urinary
incontinence is still not clear, or if red flags such as hematuria, obstructive symptoms, or recurrent urinary tract
infec-tions are present, referral to a urologist or urogynecologist should be considered. (
Am Fam Physician
.
2013;87(8):543-550. Copyright © 2013 American Academy of Family Physicians.)
More online at http://www. aafp.org/afp.
Downloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright © 2013 American Academy of Family Physicians. For the private, noncommercial use of one individual user of the Web site. All other rights reserved. Contact [email protected] for copyright questions and/or permission requests.
Urinary Incontinence: Diagnosis
544
American Family Physician www.aafp.org/afp Volume 87, Number 8 ◆April 15, 2013
difficulties that impair patients’ ability to use the toilet,
but without a failure of bladder function or neurologic
control of urination.
2,16This type of incontinence is also
referred to as toileting difficulty.
16Evaluation
Patients can be evaluated for urinary incontinence in a
family physician’s office. Although most incontinence
research excludes men and children, a standardized
approach is recommended for guiding the initial
evalua-tion.
17An algorithm for the diagnosis of
uri-nary incontinence is shown in Figure 1.
The patient history is often the most
important factor in identifying the type,
severity, and burden of incontinence for
patients.
6Generally, more than one office
visit is required to perform the physical
examination and necessary tests.
11Transient Urinary Incontinence
The first step in the evaluation is to
iden-tify transient or reversible causes of urinary
incontinence.
10,11,13Reversible incontinence
usually has a sudden onset and has been
present for less than six weeks at the time of
evaluation.
18The mnemonic DIAPPERS is
useful for recalling the common reversible
causes of urinary incontinence (Table 2).
19Physicians should take note of patients’
medications, especially those started recently.
Medication-induced incontinence often
can be reversed by stopping the medication.
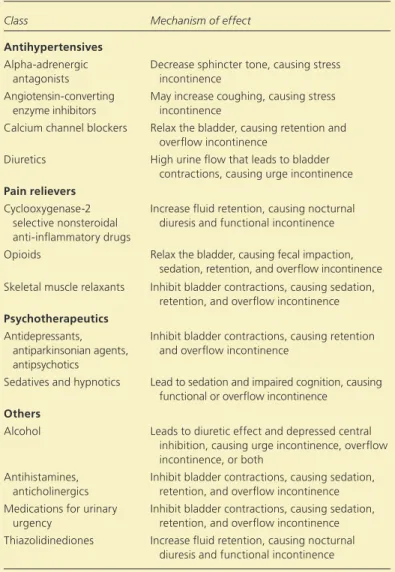
Table 3 lists the most important medications
to consider.
6,13Certain drugs (e.g., diuretics,
alcohol) have no pharmacologic action on
the lower urinary tract, but may contribute to
incontinence by increasing urine production
or impairing nervous system function.
9,11If the incontinence is determined to be related to an
acute condition, correcting the transient causes may
resolve the symptoms.
10,13However, if symptoms persist,
further evaluation is needed.
Chronic Urinary Incontinence
PATIENT QUESTIONNAIRESSeveral questionnaires are available to determine which
type of chronic urinary incontinence is present.
2The
3 Incontinence Questions is a reliable questionnaire
SORT: KEY RECOMMENDATIONS FOR PRACTICEClinical recommendation
Evidence
rating References Comments The 3 Incontinence Questions tool, which asks patients if, when, and
how often they experience urine leakage, should be used to help categorize the type of urinary incontinence.
C 20 Good-quality prospective cohort study with follow-up
A three-day voiding diary can be used as part of the initial assessment for urinary incontinence symptoms.
C 27 Systematic review of lower-quality studies
A positive cough stress test result is the most reliable clinical assessment for confirming the diagnosis of stress incontinence.
C 2, 32 Systematic review of good-quality cohort studies
Postvoid residual urine measurement should be performed in select high-risk patients (e.g., those with overflow incontinence).
C 5, 15 Consensus opinion, no high-quality evidence is available to support the recommendation
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to http://www.aafp.org/afpsort.xml.
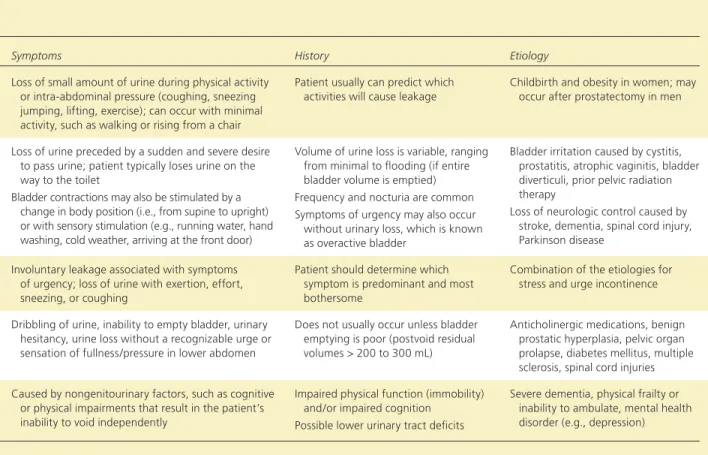
Table 1. Types of Chronic Urinary Incontinence
Type Prevalence Pathophysiology Symptoms History Etiology
Stress 24 to 45 percent in women older than 30 years
Sphincter weakness (urethral sphincter and/or pelvic floor weakness)
Loss of small amount of urine during physical activity or intra-abdominal pressure (coughing, sneezing jumping, lifting, exercise); can occur with minimal activity, such as walking or rising from a chair
Patient usually can predict which activities will cause leakage
Childbirth and obesity in women; may occur after prostatectomy in men
Urge 9 percent in women 40 to 44 years of age 31 percent in women
older than 75 years 42 percent in men
older than 75 years
Detrusor overactivity (uninhibited bladder contractions) caused by irritation within the bladder or loss of inhibitory neurologic control of bladder contractions
Loss of urine preceded by a sudden and severe desire to pass urine; patient typically loses urine on the way to the toilet
Bladder contractions may also be stimulated by a change in body position (i.e., from supine to upright) or with sensory stimulation (e.g., running water, hand washing, cold weather, arriving at the front door)
Volume of urine loss is variable, ranging from minimal to flooding (if entire bladder volume is emptied) Frequency and nocturia are common Symptoms of urgency may also occur
without urinary loss, which is known as overactive bladder
Bladder irritation caused by cystitis, prostatitis, atrophic vaginitis, bladder diverticuli, prior pelvic radiation therapy
Loss of neurologic control caused by stroke, dementia, spinal cord injury, Parkinson disease
Mixed 20 to 30 percent of patients with chronic incontinence
Combination of stress and urge incontinence
Involuntary leakage associated with symptoms of urgency; loss of urine with exertion, effort, sneezing, or coughing
Patient should determine which symptom is predominant and most bothersome
Combination of the etiologies for stress and urge incontinence Overflow (urinary retention) 5 percent of patients with chronic incontinence
Overdistention of the bladder caused by impaired detrusor contractility or bladder outlet obstruction; leads to urine leakage by overflow
Dribbling of urine, inability to empty bladder, urinary hesitancy, urine loss without a recognizable urge or sensation of fullness/pressure in lower abdomen
Does not usually occur unless bladder emptying is poor (postvoid residual volumes > 200 to 300 mL)
Anticholinergic medications, benign prostatic hyperplasia, pelvic organ prolapse, diabetes mellitus, multiple sclerosis, spinal cord injuries Functional Uncertain Variable leakage of urine, usually
caused by environmental or physical barriers to toileting
Caused by nongenitourinary factors, such as cognitive or physical impairments that result in the patient’s inability to void independently
Impaired physical function (immobility) and/or impaired cognition
Possible lower urinary tract deficits
Severe dementia, physical frailty or inability to ambulate, mental health disorder (e.g., depression)
Urinary Incontinence: Diagnosis
April 15, 2013 ◆
Volume 87, Number 8
www.aafp.org/afp American Family Physician545
available free of charge (Figure 2).
20It asks three
mul-tiple choice questions about if, when, and how often
patients experience urine leakage. This questionnaire
has been validated in studies that show it to be
reason-ably accurate in categorizing urinary incontinence in
middle-aged to older women.
20It has a sensitivity of 0.86
and 0.75, and a specificity of 0.60 and 0.77, for
classify-ing stress and urge incontinence, respectively.
20ASSESSMENT OF MEDICAL PROBLEMS
The patient history should include an assessment of other
medical conditions and symptoms, with their temporal
relationship to urinary incontinence.
15For example, a
history of bowel, back, gynecologic, or bladder surgery
could affect the anatomy and innervation of the lower
urinary tract, leading to incontinence.
6,15Gynecologic
history can assess estrogen status; estrogen deficiency
may result in atrophic vaginitis or atrophic urethritis, a
potentially reversible cause of urinary incontinence.
6Physicians should also inquire about other
comor-bidities, such as chronic obstructive pulmonary disease
(chronic cough can result in stress incontinence);
car-diovascular disease (volume status or diuretic therapy
can increase urine flow and cause incontinence in
patients with an overactive bladder); neurologic
condi-tions (central nervous system dysfunction can impair
inhibition of detrusor contractions, or lead to
denerva-tion of the detrusor muscle with resultant retendenerva-tion and
overflow incontinence); and musculoskeletal conditions
(impaired mobility can cause functional incontinence).
Treating these conditions may not eliminate
inconti-nence, but it may lessen the severity.
2,9,15ASSESSMENT OF QUALITY OF LIFE
The severity of symptoms and their effect on quality
of life determines the aggressiveness of treatment.
6,15Patients should be asked about the effects of
inconti-nence on work, activities of daily living, sleep, sexual
activity, social interactions, interpersonal relationships,
and general perception of health and quality of life.
6,15Identifying the most bothersome symptom will help
direct management. For example, one patient may be
most concerned about managing nocturia (often caused
by urge incontinence), whereas another patient may be
most concerned about incontinence that occurs during
exercise (typically caused by stress incontinence).
Table 1. Types of Chronic Urinary Incontinence
Type Prevalence Pathophysiology Symptoms History Etiology
Stress 24 to 45 percent in women older than 30 years
Sphincter weakness (urethral sphincter and/or pelvic floor weakness)
Loss of small amount of urine during physical activity or intra-abdominal pressure (coughing, sneezing jumping, lifting, exercise); can occur with minimal activity, such as walking or rising from a chair
Patient usually can predict which activities will cause leakage
Childbirth and obesity in women; may occur after prostatectomy in men
Urge 9 percent in women 40 to 44 years of age 31 percent in women
older than 75 years 42 percent in men
older than 75 years
Detrusor overactivity (uninhibited bladder contractions) caused by irritation within the bladder or loss of inhibitory neurologic control of bladder contractions
Loss of urine preceded by a sudden and severe desire to pass urine; patient typically loses urine on the way to the toilet
Bladder contractions may also be stimulated by a change in body position (i.e., from supine to upright) or with sensory stimulation (e.g., running water, hand washing, cold weather, arriving at the front door)
Volume of urine loss is variable, ranging from minimal to flooding (if entire bladder volume is emptied) Frequency and nocturia are common Symptoms of urgency may also occur
without urinary loss, which is known as overactive bladder
Bladder irritation caused by cystitis, prostatitis, atrophic vaginitis, bladder diverticuli, prior pelvic radiation therapy
Loss of neurologic control caused by stroke, dementia, spinal cord injury, Parkinson disease
Mixed 20 to 30 percent of patients with chronic incontinence
Combination of stress and urge incontinence
Involuntary leakage associated with symptoms of urgency; loss of urine with exertion, effort, sneezing, or coughing
Patient should determine which symptom is predominant and most bothersome
Combination of the etiologies for stress and urge incontinence Overflow (urinary retention) 5 percent of patients with chronic incontinence
Overdistention of the bladder caused by impaired detrusor contractility or bladder outlet obstruction; leads to urine leakage by overflow
Dribbling of urine, inability to empty bladder, urinary hesitancy, urine loss without a recognizable urge or sensation of fullness/pressure in lower abdomen
Does not usually occur unless bladder emptying is poor (postvoid residual volumes > 200 to 300 mL)
Anticholinergic medications, benign prostatic hyperplasia, pelvic organ prolapse, diabetes mellitus, multiple sclerosis, spinal cord injuries Functional Uncertain Variable leakage of urine, usually
caused by environmental or physical barriers to toileting
Caused by nongenitourinary factors, such as cognitive or physical impairments that result in the patient’s inability to void independently
Impaired physical function (immobility) and/or impaired cognition
Possible lower urinary tract deficits
Severe dementia, physical frailty or inability to ambulate, mental health disorder (e.g., depression)
Urinary Incontinence: Diagnosis
VOIDING DIARY
Because many patients provide an unclear voiding
his-tory, a voiding diary can be helpful (eFigure A). The
simplest voiding diaries ask patients to record the
fre-quency of incontinence episodes, but diaries also can
be used to assess the situations in which incontinence
occurs, which can help clarify the type of incontinence.
For example, the diary may reveal leakage during times
of increased abdominal pressure, suggestive of stress
incontinence, or dribbling that is indicative of overflow
incontinence.
21Patients with stress incontinence usually
wake once or not at all at night to void; patients with urge
incontinence usually wake more than twice and as often
as every hour.
21,22A voiding diary can also serve as a baseline for
com-paring the severity of incontinence after treatment,
thereby assessing the effectiveness of management.
23,24Table 2. Differential Diagnosis of Transient
Causes of Urinary Incontinence (DIAPPERS
Mnemonic)
Delirium
Infection (acute urinary tract infection) Atrophic vaginitis
Pharmaceuticals(Table 3)
Psychological disorder, especially depression Excessive urine output (e.g., hyperglycemia)
Reduced mobility (i.e., functional incontinence) or reversible (e.g., drug-induced) urinary retention
Stool impaction
Adapted with permission from Resnick NM, Yalla SV. Management of urinary incontinence in the elderly. N Engl J Med. 1985;313(13):801.
Diagnosis of Urinary Incontinence
Figure 1. Algorithm for the diagnosis of urinary incontinence. (PVR = postvoid residual.) Patient presents with urinary incontinence
Assess for transient incontinence: Apply DIAPPERS mnemonic (Table 2) Review medications (Table 3)
Assess for chronic incontinence:
Obtain history and give 3 Incontinence Questions questionnaire (Table 1 and Figure 2)
Review voiding diary (eFigure A)
Perform physical examination (Table 4); include cough stress test if stress incontinence is suspected Measure PVR urine
Obtain laboratory evaluation
Presumed type of incontinence after history, physical examination, and laboratory evaluation (may require return visit or referral if diagnosis is inconclusive or red flags are found)
Stress (only or predominantly) Symptoms with coughing,
sneezing, or exercise; no nocturia Voiding diary: small
volume leakage (5 to 10 mL) with activity Cough stress test: leakage
coincides with coughing PVR urine < 50 mL
Urge (only or predominantly) Symptoms of urgency Voiding diary: variable
volume loss; frequency and nocturia noted Cough stress test: may
show delayed leakage after cough PVR urine < 50 mL
Mixed
Symptoms equally as often with physical activity as with a sense of urgency Voiding diary: varies Cough stress test: may
show leakage with coughing PVR urine < 50 mL Overflow No symptoms with physical activity or urgency Voiding diary: varies Cough stress test: no
leakage PVR urine > 200 mL
No
Treat reversible causes
Incontinence resolved?
No further intervention Yes
Functional
Symptoms may include cognitive impairment and degree of immobility Voiding diary: may show
pattern in circumstances of incontinence Cough stress test: no
leakage PVR urine: varies
Urinary Incontinence: Diagnosis
April 15, 2013 ◆
Volume 87, Number 8
www.aafp.org/afp American Family Physician547
A three-day diary is as informative as a longer-term
assessment, has good reliability, and may be more
fea-sible than longer diaries in routine clinical settings.
25-27More sophisticated diaries, such as a frequency-
volume voiding diary for assessing bladder activity,
can also be used.
10,24A frequency-volume voiding diary
requires recording the amount of fluid intake, the volume
of urine voided (in mL) of each continent episode (using a
measuring cup or plastic hat placed below the toilet seat),
and an estimation of the volume of each incontinent
epi-sode.
28This approach can reliably discriminate between
urge and stress incontinence. Urge incontinence
typi-cally involves a large volume of urine loss, whereas stress
incontinence is often a smaller volume and is associated
with increased abdominal pressure.
29,30A
frequency-voiding diary can reveal whether the patient is
experi-encing frequent large volume voids, which are typically
associated with conditions causing polyuria
(e.g., excess fluid intake, diabetes mellitus).
PHYSICAL EXAMINATIONThe physical examination can identify
ana-tomic abnormalities or transient causes that
may not have been considered after
apply-ing the DIAPPERS mnemonic. Findapply-ings
associated with incontinence are listed in
Table 4.
6,11,16In particular, the cardiovascular
examination should look for evidence of
vol-ume overload (e.g., rales, pedal edema) that
might result in increased urine flow, which
aggravates urge incontinence. The abdomen
should be palpated for masses and tenderness,
and the bladder percussed for distention that
would indicate overflow.
11,17The extremities
should be examined for joint mobility and
function (impairment of which might
indi-cate functional incontinence), and peripheral
edema that might indicate volume overload.
In men, a prostate examination should be
included to identify prostate enlargement,
which may contribute to an outlet
obstruc-tion.
14,15In women, an external
gyneco-logic examination can assess for atrophic
vaginitis or other vulvar signs of irritation
caused by incontinence.
14,31Estrogen
defi-ciency may predispose women to urinary
frequency, urgency, or both, and can cause
or exaggerate sensory urge incontinence.
6,31Pelvic organ prolapse (with cystocele,
ure-thral polyps, or rectocele) may not lead to
incontinence, but it often accompanies
atro-phic vaginitis.
6,14,17,31A rectal examination is important
to assess for fecal impaction, which can exert pressure
on the urethra, impair bladder emptying, and
precipi-tate overflow incontinence caused by retention.
10,11In
select patients, primarily older adults, a cognitive and
functional assessment should be included to evaluate for
functional incontinence.
3,11,16COUGH STRESS TEST
If stress incontinence is suspected, the cough stress test
is the most reliable clinical assessment for confirming
the diagnosis.
2,28,32When compared with more
sophis-ticated multichannel urodynamic studies, the cough
stress test demonstrates good sensitivity and specificity
for stress incontinence,
32-34although it requires further
confirmatory urodynamic evaluation if the results are
inconclusive.
35Table 3. Common Medications and Substances That Can
Cause Urinary Incontinence
Class Mechanism of effect Antihypertensives
Alpha-adrenergic antagonists
Decrease sphincter tone, causing stress incontinence
Angiotensin-converting enzyme inhibitors
May increase coughing, causing stress incontinence
Calcium channel blockers Relax the bladder, causing retention and overflow incontinence
Diuretics High urine flow that leads to bladder contractions, causing urge incontinence
Pain relievers
Cyclooxygenase-2 selective nonsteroidal anti-inflammatory drugs
Increase fluid retention, causing nocturnal diuresis and functional incontinence Opioids Relax the bladder, causing fecal impaction,
sedation, retention, and overflow incontinence Skeletal muscle relaxants Inhibit bladder contractions, causing sedation,
retention, and overflow incontinence
Psychotherapeutics
Antidepressants, antiparkinsonian agents, antipsychotics
Inhibit bladder contractions, causing retention and overflow incontinence
Sedatives and hypnotics Lead to sedation and impaired cognition, causing functional or overflow incontinence
Others
Alcohol Leads to diuretic effect and depressed central inhibition, causing urge incontinence, overflow incontinence, or both
Antihistamines, anticholinergics
Inhibit bladder contractions, causing sedation, retention, and overflow incontinence Medications for urinary
urgency
Inhibit bladder contractions, causing sedation, retention, and overflow incontinence Thiazolidinediones Increase fluid retention, causing nocturnal
diuresis and functional incontinence
548
American Family Physician www.aafp.org/afp Volume 87, Number 8 ◆April 15, 2013
With a full bladder (although not to the point of
abrupt urination), the patient should be in the lithotomy
position. Women should separate the labia.
13,35The
patient should relax the pelvic muscles and forcibly
cough once.
13If the test is initially performed supine
and no leakage is observed, the test should be repeated
in the standing position. The patient stands while
wear-ing a pad or with his or her legs shoulder-width apart
over a cloth or paper sheet on the floor to see the
leak-age. If urine leaks with the onset of the cough and
ter-minates with its cessation, the test is positive for stress
incontinence.
35A negative test shows no leak or a delayed leak by five
to 15 seconds, and rules out most cases of stress
incon-tinence.
36False-negative results may occur if a patient’s
bladder is empty, if the cough is not forceful enough,
if the pelvic floor muscles contract to override urethral
sphincter incompetence, or if severe prolapse masks
the leakage.
35,36Furthermore, a delayed leak may
sug-gest a bladder spasm triggered by the cough, and not a
weakness of the sphincter. This indicates possible urge
incontinence.
13LABORATORY TESTS
Laboratory tests should include a serum
cre-atinine level, which may be elevated if there is
urinary retention (overflow bladder) caused
by bladder outlet obstruction or denervation
of the detrusor. If not already performed to
exclude acute urinary tract infection as a
cause of reversible incontinence, a
urinaly-sis should be obtained to rule out hematuria,
proteinuria, and glycosuria, any of which
require a diagnostic workup.
6POSTVOID RESIDUAL URINE
A measurement of postvoid residual (PVR)
urine is recommended to diagnose overflow
incontinence.
10Although overflow
incon-tinence is present in only a minority of
patients with incontinence, it is important
to exclude this diagnosis because chronic
failure of bladder emptying can lead to
hydronephrosis and irreversibly impaired
renal function. Overflow is more common
in older persons, but it can also occur in
young adults as a manifestation of
neu-rologic disorders, such as multiple
sclero-sis. Expert opinion recommends that PVR
urine always be measured in patients who
may have overflow incontinence, and some
experts recommend measuring PVR urine
when another cause is not obvious.
5,15To measure PVR urine, the patient empties the
bladder, and then the amount of urine remaining in
the bladder is measured. This can be performed with
a handheld ultrasound unit, which is the preferred
method if available. The alternative is in-and-out
ure-thral catheterization.
28In-and-out catheterization
requires training to decrease the risk of infection and
urethral trauma, which is important in men with
sig-nificant prostate enlargement.
11If PVR urine cannot be
measured in the office setting and if overflow
inconti-nence is strongly suspected, further urodynamic
evalu-ation is warranted.
10,12A PVR urine measurement less than 50 mL is negative
for overflow; 100 to 200 mL is considered indeterminate
(and the measurement should be repeated on another
occasion); and greater than 200 mL is suggestive of
over-flow as a main contributing factor of incontinence.
6Referral for Further Evaluation
If the cause of urinary incontinence is unclear after the
assessment, referral to a urologist or urogynecologist is
The 3 Incontinence Questions
1. During the past three months, have you leaked urine (even a small amount)?
❏ Yes
❏ No (questionnaire completed)
2. During the past three months, did you leak urine: (check all that apply)
❏ A. When you were performing some physical activity, such as coughing, sneezing, lifting, or exercising?
❏ B. When you had the urge or the feeling that you needed to empty your bladder, but you could not get to the toilet fast enough?
❏ C. Without physical activity and without a sense of urgency?
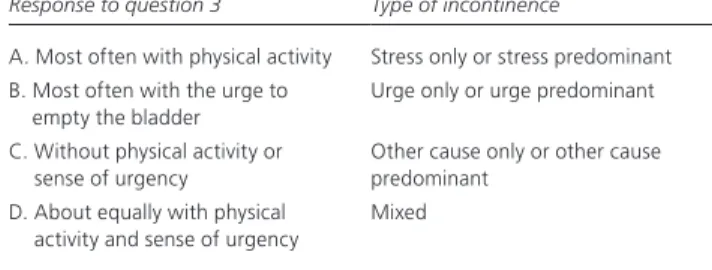
3. During the past three months, did you leak urine most often: (check only one)
❏ A. When you were performing some physical activity, such as coughing, sneezing, lifting, or exercising?
❏ B. When you had the urge or feeling that you needed to empty your bladder, but you could not get to the toilet fast enough?
❏ C. Without physical activity and without a sense of urgency?
❏ D. About equally as often with physical activity as with a sense of urgency? Definitions of type of urinary incontinence are based on responses to question 3:
Response to question 3 Type of incontinence
A. Most often with physical activity Stress only or stress predominant B. Most often with the urge to
empty the bladder
Urge only or urge predominant C. Without physical activity or
sense of urgency
Other cause only or other cause predominant
D. About equally with physical activity and sense of urgency
Mixed
Figure 2. Questionnaire for the evaluation of urinary incontinence. Adapted with permission from Brown JS, Bradley CS, Subak LL, et al.; Diagnostic Aspects of Incontinence Study (DAISy) Research Group. The sensitivity and specificity of a sim-ple test to distinguish between urge and stress urinary incontinence. Ann Intern Med. 2006;144(10):716.
Urinary Incontinence: Diagnosis
April 15, 2013 ◆
Volume 87, Number 8
www.aafp.org/afp American Family Physician549
recommended (Table 5
18,36)
. Patients with typical stress
or urge incontinence usually do not have any of the red
flags of hematuria, obstructive symptoms (straining to
void or sensation of incomplete bladder emptying), or
recurrent urinary tract infections. If any of these are
present, further evaluation is recommended.
36Routine referral for urodynamic testing is not
recom-mended, even if a patient is a candidate for surgical
treat-ment of stress incontinence. Studies show that routine
preoperative urodynamic testing in patients who have
uncomplicated stress incontinence does not result in
better surgical outcomes.
37The authors thank Anthony Viera, MD, MPH, assistant professor in the Department of Family Medicine, University of North Carolina at Chapel Hill, for his assistance with this article.
Data Sources: A literature search for scientific evidence supporting evaluation of urinary incontinence was performed in PubMed Clinical
Table 5. Indications for Urologic Referral
Incontinence associated with relapse or recurrent symptomatic urinary tract infections
Incontinence with new-onset neurologic symptoms, muscle weakness, or both
Marked prostate enlargement Pelvic organ prolapsed past the introitus Pelvic pain associated with incontinence Persistent hematuria
Persistent proteinuria
Postvoid residual volume > 200 mL Previous pelvic surgery or radiation Uncertain diagnosis
Information from references 18 and 36.
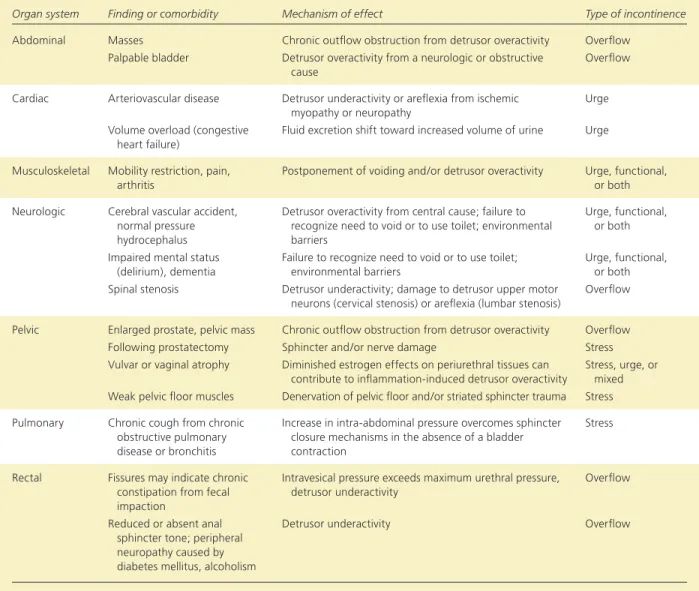
Table 4. Physical Examination Findings Associated with Urinary Incontinence
Organ system Finding or comorbidity Mechanism of effect Type of incontinence Abdominal Masses Chronic outflow obstruction from detrusor overactivity Overflow
Palpable bladder Detrusor overactivity from a neurologic or obstructive cause
Overflow Cardiac Arteriovascular disease Detrusor underactivity or areflexia from ischemic
myopathy or neuropathy
Urge Volume overload (congestive
heart failure)
Fluid excretion shift toward increased volume of urine Urge Musculoskeletal Mobility restriction, pain,
arthritis
Postponement of voiding and/or detrusor overactivity Urge, functional, or both Neurologic Cerebral vascular accident,
normal pressure hydrocephalus
Detrusor overactivity from central cause; failure to recognize need to void or to use toilet; environmental barriers
Urge, functional, or both Impaired mental status
(delirium), dementia
Failure to recognize need to void or to use toilet; environmental barriers
Urge, functional, or both Spinal stenosis Detrusor underactivity; damage to detrusor upper motor
neurons (cervical stenosis) or areflexia (lumbar stenosis)
Overflow Pelvic Enlarged prostate, pelvic mass Chronic outflow obstruction from detrusor overactivity Overflow
Following prostatectomy Sphincter and/or nerve damage Stress Vulvar or vaginal atrophy Diminished estrogen effects on periurethral tissues can
contribute to inflammation-induced detrusor overactivity
Stress, urge, or mixed Weak pelvic floor muscles Denervation of pelvic floor and/or striated sphincter trauma Stress Pulmonary Chronic cough from chronic
obstructive pulmonary disease or bronchitis
Increase in intra-abdominal pressure overcomes sphincter closure mechanisms in the absence of a bladder contraction
Stress
Rectal Fissures may indicate chronic constipation from fecal impaction
Intravesical pressure exceeds maximum urethral pressure, detrusor underactivity
Overflow
Reduced or absent anal sphincter tone; peripheral neuropathy caused by diabetes mellitus, alcoholism
Detrusor underactivity Overflow
Urinary Incontinence: Diagnosis
550
American Family Physician www.aafp.org/afp Volume 87, Number 8 ◆April 15, 2013
Queries using the key terms diagnosis, physical examination, urinaryincontinence, and causes. The search included meta-analyses, random-ized controlled trials, clinical trials, and reviews. We also searched the Agency for Healthcare Research and Quality evidence reports, Clinical Evidence, the Cochrane database, Essential Evidence Plus, and the National Guideline Clearinghouse database. Search date: June 6, 2012.
The Authors
CHRISTINE KHANDELWAL, DO, is a clinical assistant professor in the Department of Family Medicine at the University of North Carolina, Cha-pel Hill.
CHRISTINE KISTLER, MD, MASc, is an assistant professor in the Depart-ment of Family Medicine at the University of North Carolina.
Address correspondence to Christine Khandelwal, DO, University of North Carolina, 590 Manning Dr., Chapel Hill, NC 27599 (e-mail: [email protected]). Reprints are not available from the authors.
Author disclosure: No relevant financial affiliations. REFERENCES
1. Fantl AJ. Urinary incontinence in adults: acute and chronic manage-ment/urinary incontinence in adults. Guideline Panel Update. Rockville, Md.: U.S. Department of Health and Human Services, 1996; Agency for Health Care Policy and Research; Clinical Practice Guideline Number 2: AHCPR publication no. 96-0682.
2. Holroyd-Leduc JM, Tannenbaum C, Thorpe KE, Straus SE. What type of urinary incontinence does this woman have? JAMA. 2008;299(12): 1446-1456.
3. Gibbs CF, Johnson TM II, Ouslander JG. Office management of geriatric urinary incontinence. Am J Med. 2007;120(3):211-220.
4. Thom D. Variation in estimates of urinary incontinence prevalence in the community: effects of differences in definition, population characteris-tics, and study type. J Am Geriatr Soc. 1998;46(4):473-480.
5. DuBeau CE, Kuchel GA, Johnson T II, Palmer MH, Wagg A; Fourth International Consultation on Incontinence. Incontinence in the frail elderly: report from the 4th International Consultation on Incontinence. Neurourol Urodyn. 2010;29(1):165-178.
6. Weiss BD. Diagnostic evaluation of urinary incontinence in geriatric patients. Am Fam Physician. 1998;57(11):2675-2684, 2688-2690. 7. Coyne KS, Sexton CC, Irwin DE, Kopp ZS, Kelleher CJ, Milsom I. The
impact of overactive bladder, incontinence and other lower urinary tract symptoms on quality of life, work productivity, sexuality and emotional well-being in men and women: results from the EPIC study. BJU Int. 2008;101(11):1388-1395.
8. Gormley EA, Lightner DJ, Burgio KL, et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. J Urol. 2012;188(6 suppl):2455-2463.
9. McKertich K. Urinary incontinence-assessment in women: stress, urge or both? Aust Fam Physician. 2008;37(3):112-117.
10. Dowling-Castronovo A, Specht JK. How to try this: assessment of tran-sient urinary incontinence in older adults. Am J Nurs. 2009;109(2):62-71. 11. Frank C, Szlanta A. Office management of urinary incontinence among
older patients. Can Fam Physician. 2010;56(11):1115-1120.
12. Ouslander JG. Management of overactive bladder. N Engl J Med. 2004;350(8):786-799.
13. Imam KA. The role of the primary care physician in the management of bladder dysfunction. Rev Urol. 2004;6(suppl 1):S38-S44.
14. Chapple CR, Manassero F. Urinary incontinence in adults. Surgery (Oxford). 2005;23(3):101-107.
15. DuBeau CE. Clinical presentation and diagnosis of urinary incontinence. http://www.uptodate.com/contents/clinical-presentation-and-diagnosis-of-urinary-incontinence [subscription required]. Accessed January 31, 2012.
16. Yap P, Tan D. Urinary incontinence in dementia - a practical approach. Aust Fam Physician. 2006;35(4):237-241.
17. Goode PS, Burgio KL, Richter HE, Markland AD. Incontinence in older women. JAMA. 2010;303(21):2172-2181.
18. Cefalu CA. Urinary incontinence. In: Ham RJ, ed. Primary Care Geriatrics: A Case-Based Approach. 5th ed. Philadelphia, Pa.: Mosby Elsevier; 2007:306-323.
19. Resnick NM, Yalla SV. Management of urinary incontinence in the elderly. N Engl J Med. 1985;313(13):800-805.
20. Brown JS, Bradley CS, Subak LL, et al.; Diagnostic Aspects of Inconti-nence Study (DAISy) Research Group. The sensitivity and specificity of a simple test to distinguish between urge and stress urinary incontinence. Ann Intern Med. 2006;144(10):715-723.
21. Moore KN, Saltmarche B, Query A. Urinary incontinence. Non-surgical management by family physicians. Can Fam Physician. 2003;49:602-610. 22. Wyman JF, Choi SC, Harkins SW, Wilson MS, Fantl JA. The urinary diary in evaluation of incontinent women: a test-retest analysis. Obstet Gyne-col. 1988;71(6 pt 1):812-817.
23. Bryan NP, Chapple CR. Frequency volume charts in the assessment and evaluation of treatment: how should we use them? Eur Urol. 2004; 46(5):636-640.
24. Abrams P, Klevmark B. Frequency volume charts: an indispensable part of lower urinary tract assessment. Scand J Urol Nephrol Suppl. 1996; 179:47-53.
25. Homma Y, Ando T, Yoshida M, et al. Voiding and incontinence fre-quencies: variability of diary data and required diary length. Neurourol Urodyn. 2002;21(3):204-209.
26. Nygaard I, Holcomb R. Reproducibility of the seven-day voiding diary in women with stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 2000;11(1):15-17.
27. Yap TL, Cromwell DC, Emberton M. A systematic review of the reliability of frequency-volume charts in urological research and its implications for the optimum chart duration. BJU Int. 2007;99(1):9-16.
28. Culligan PJ, Heit M. Urinary incontinence in women: evaluation and management. Am Fam Physician. 2000;62(11):2433-2444, 2447, 2452. 29. Fink D, Perucchini D, Schaer GN, Haller U. The role of the frequency- volume chart in the differential diagnostic of female urinary inconti-nence. Acta Obstet Gynecol Scand. 1999;78(3):254-257.
30. Brown JS, et al. Measurement characteristics of a voiding diary for use by men and women with overactive bladder. Urology. 2003;61(4):802-809. 31. Bachmann GA, Nevadunsky NS. Diagnosis and treatment of atrophic
vaginitis. Am Fam Physician. 2000;61(10):3090-3096.
32. Videla FL, Wall LL. Stress incontinence diagnosed without multichannel urodynamic studies. Obstet Gynecol. 1998;91(6):965-968.
33. Scotti RJ, Myers DL. A comparison of the cough stress test and single-channel cystometry with multisingle-channel urodynamic evaluation in genu-ine stress incontgenu-inence. Obstet Gynecol. 1993;81(3):430-433. 34. Wall LL, Wiskind AK, Taylor PA. Simple bladder filling with a cough
stress test compared with subtracted cystometry for the diagnosis of urinary incontinence. Am J Obstet Gynecol. 1994;171(6):1472-1477. 35. Ghoniem G, Stanford E, Kenton K, et al. Evaluation and outcome
mea-sures in the treatment of female urinary stress incontinence: Interna-tional Urogynecological Association (IUGA) guidelines for research and clinical practice. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(1):5-33. 36. Weidner AC, Myers ER, Visco AG, Cundiff GW, Bump RC. Which
women with stress incontinence require urodynamic evaluation? Am J Obstet Gynecol. 2001;184(2):20-27.
37. Nager CW, Brubaker L, Litman HJ, et al.; Urinary Incontinence Treat-ment Network. A randomized trial of urodynamic testing before stress-incontinence surgery. N Engl J Med. 2012;366(21):1987-1997.
Nonsurgical Management of Urinary Incontinence in Women: A
Clinical Practice Guideline From the American College of Physicians
Amir Qaseem, MD, PhD, MHA; Paul Dallas, MD; Mary Ann Forciea, MD, MS; Melissa Starkey, PhD; Thomas D. Denberg, MD, PhD; and Paul Shekelle, MD, PhD, for the Clinical Guidelines Committee of the American College of Physicians*
Description:The American College of Physicians (ACP) developed this guideline to present the evidence and provide clinical recom-mendations on the nonsurgical management of urinary inconti-nence (UI) in women.
Methods: This guideline is based on published English-language literature on nonsurgical management of UI in women from 1990 through December 2013 that was identified using MEDLINE, the Cochrane Library, Scirus, and Google Scholar. The outcomes eval-uated for this guideline include continence, improvement in UI, quality of life, adverse effects, and discontinuation due to adverse effects. It grades the evidence and recommendations by using ACP’s guideline grading system. The target audience is all clinicians, and the target patient population is all women with UI.
Recommendation 1: ACP recommends first-line treatment with pelvic floor muscle training in women with stress UI. (Grade: strong recommendation, high-quality evidence)
Recommendation 2:ACP recommends bladder training in women with urgency UI. (Grade: weak recommendation, low-quality evi-dence)
Recommendation 3:ACP recommends pelvic floor muscle training with bladder training in women with mixed UI. (Grade: strong recommendation, high-quality evidence)
Recommendation 4:ACP recommends against treatment with sys-temic pharmacologic therapy for stress UI. (Grade: strong recom-mendation, low-quality evidence)
Recommendation 5:ACP recommends pharmacologic treatment in women with urgency UI if bladder training was unsuccessful. Cli-nicians should base the choice of pharmacologic agents on tolera-bility, adverse effect profile, ease of use, and cost of medication. (Grade: strong recommendation, high-quality evidence)
Recommendation 6: ACP recommends weight loss and exercise for obese women with UI. (Grade: strong recommendation, moderate-quality evidence)
Ann Intern Med.2014;161:429-440. doi:10.7326/M13-2410 www.annals.org
For author affiliations, see end of text.
U
rinary incontinence (UI), the involuntary loss of
urine, has a prevalence of approximately 25% in
young women (aged 14 to 21 years) (1), 44% to 57%
in middle-aged and postmenopausal women (aged 40 to 60
years) (2), and 75% in elderly women (aged
ⱖ
75 years)
(3). However, these statistics may be underestimated
be-cause one study showed that at least half of incontinent
women do not report the issue to their physicians (4). Risk
factors for UI include pregnancy, pelvic floor trauma after
vaginal delivery, menopause, hysterectomy, obesity,
uri-nary tract infection, functional and/or cognitive
impair-ment, chronic cough, and constipation (5). The effects of
UI range from slightly bothersome to debilitating. Urinary
incontinence also contributes to high medical spending—
approximately $19.5 billion was spent in the United States
in 2004 —and it accounts for 6% of nursing home
admis-sions for elderly women, costing approximately $3 billion
(6).
The 2 types of UI are based on the dysfunctional
mechanism: stress and urgency. However, the distinction is
not always clear, particularly for older women. Stress UI is
related to urethral sphincter failure associated with
intra-abdominal pressure and results in the inability to retain
urine when laughing, coughing, or sneezing (7). Urgency
UI is the involuntary loss of urine associated with a sudden
and compelling urge to void (7).
Mixed UI is a combination of stress and urgency UI.
Overactive bladder is a constellation of symptoms that
in-cludes urinary urgency (with or without UI), usually
ac-companied by frequency, and nocturia (5).
The primary goal of treatment is to achieve or improve
continence (8, 9). Clinically successful treatment has been
defined as that which reduces the frequency of UI episodes
by at least 50% (10). Treatments addressed in this
guide-line include lifestyle changes, pelvic floor muscle training
(PFMT), and various approved drugs (
Table 1
) (8).
Sur-gical treatments, available for women in whom
conserva-* This paper, written by Amir Qaseem, MD, PhD, MHA; Paul Dallas, MD; Mary Ann Forciea, MD, MS; Melissa Starkey, PhD; Thomas D. Denberg, MD, PhD; and Paul Shekelle, MD, PhD, was developed for the Clinical Guidelines Committee of the American College of Physicians. Individuals who served on the Clinical Guidelines Committee from initiation of the project until its approval were Paul Shekelle, MD, PhD (Chair); Michael J. Barry, MD; Roger Chou, MD; Molly Cooke, MD; Paul Dallas, MD; Thomas D. Denberg, MD, PhD; Nick Fitterman, MD; Mary Ann Forciea, MD, MS; Russell P. Harris, MD, MPH; Linda L. Humphrey, MD, MPH; Tanveer P. Mir, MD; Holger J. Schu¨nemann, MD, PhD; J. Sanford Schwartz, MD; Donna E. Sweet, MD; and Timothy Wilt, MD, MPH. Approved by the ACP Board of Regents on 25 September 2013.
See also:
Summary for Patients. . . I-34
Web-Only
Supplement CME quiz
Clinical Guideline
© 2014 American College of Physicians 429
This article has been corrected. The specific correction appears on the last page of this document. The original version (PDF) is available at www.annals.org. Downloaded From: http://annals.org/ on 07/30/2015
tive therapy has failed or who have anatomical
abnormali-ties, are not addressed in this guideline.
This guideline from the American College of
Physi-cians (ACP) presents the available evidence on the
nonsur-gical (pharmacologic and nonpharmacologic) treatment of
UI in women in the primary care setting. It does not fully
evaluate nonsurgical treatments, such as botulinum toxin
or percutaneous nerve, magnetic, or electrical stimulation,
because they are not typically used by or available to
pri-mary care physicians. The target audience includes all
cli-nicians, and the target patient population is all women
with UI. This guideline is based on a systematic evidence
review sponsored by the Agency for Healthcare Research
and Quality (11) and an updated literature search (
Supple-ment
, available at www.annals.org).
M
ETHODSThis guideline is based on a systematic evidence review
(11) that addressed the following key questions related to
the diagnosis and nonsurgical management of UI:
1. How effective is the nonpharmacologic treatment of
UI in women?
1a. How do nonpharmacologic treatments affect
in-continence, severity and frequency of UI, and quality of
life compared with no active treatment?
1b. How do combined methods of nonpharmacologic
treatments with drugs affect incontinence, severity and
fre-quency of UI, and quality of life compared with no active
treatment or monotherapy?
1c. What is the comparative effectiveness of different
nonpharmacologic treatments?
1d. What are the harms of nonpharmacologic
treat-ments compared with no active treatment?
1e. What are the comparative harms of different
non-pharmacologic treatments?
1f. Which patient characteristics, including age, type
and severity of UI, baseline disease that affects UI,
adher-ence to treatment recommendations, and comorbid
condi-tions, can modify the effects of nonpharmacologic
treat-ments on patient outcomes, such as continence, quality of
life, and harms?
2. How effective is the pharmacologic treatment of UI
in women?
2a. How do pharmacologic treatments affect
conti-nence, severity and frequency of UI, and quality of life
compared with no active treatment or combined treatment
methods?
2b. What is the effectiveness of pharmacologic
treat-ments compared with each other or with
nonpharmaco-logic treatments of UI?
2c. What are the harms of pharmacologic treatments
compared with no treatment?
2d. What are the harms of pharmacologic treatments
of UI compared with each other or with nonpharmacologic
tr
e
atments?
2e. Which patient characteristics, including age, type
and severity of UI, baseline disease that affects UI,
adher-ence to treatment recommendations, and comorbid
condi-tions, can modify the effects of pharmacologic treatments
on patient outcomes, such as continence, quality of life,
and harms?
The systematic evidence review was done by the
Minnesota Evidence-based Practice Center. The literature
search included English-language studies published
be-tween 1990 and December 2011 identified using
MEDLINE, the Cochrane Library, Scirus, and Google
Scholar as well as manual searches of reference lists from
systematic reviews. Literature was updated through
De-cember 2013, focusing on treatments most relevant to
pri-mary care (see the
Supplement
for details). Data were
ex-tracted using a standardized form, and study quality was
assessed according to the
Methods Guide for Effectiveness
and Comparative Effectiveness Reviews
(12). This guideline
focuses on treatments most relevant to primary care
clini-cians; the full report (11) and published article (13)
con-tain more details.
This guideline rates the evidence and
recommenda-tions by using ACP’s guideline grading system (
Table 2
).
Details of the guideline development process can be found
in the methods paper (14).
D
IAGNOSISBecause most women with UI do not report it to their
physicians (4), physicians should proactively ask female
pa-tients about bothersome UI symptoms as part of a routine
review of systems. Clinicians should take a focused history
and ask specific questions, such as the time of onset,
symp-toms, and frequency (4). Clinicians should also do a
fo-cused physical examination and evaluate neurologic
symp-toms. Asking such questions as “Do you have a problem
with urinary incontinence (of your bladder) that is
bother-some enough that you would like to know more about how
it could be treated?” as part of a quality improvement
in-tervention has been shown to increase appropriate care by
15% in patients aged 75 years or older (15).
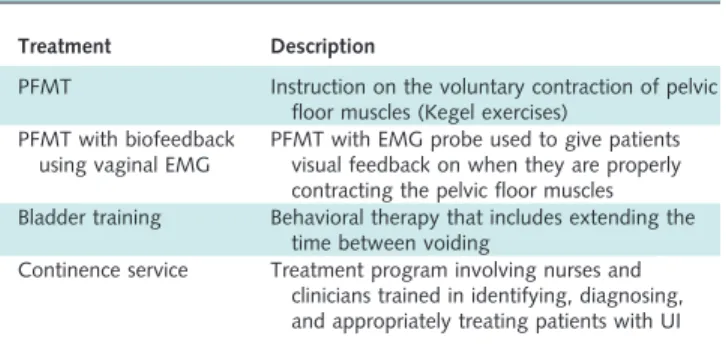
Table 1. Nonpharmacologic Treatments for UI
Treatment Description
PFMT Instruction on the voluntary contraction of pelvic floor muscles (Kegel exercises)
PFMT with biofeedback using vaginal EMG
PFMT with EMG probe used to give patients visual feedback on when they are properly contracting the pelvic floor muscles Bladder training Behavioral therapy that includes extending the
time between voiding
Continence service Treatment program involving nurses and clinicians trained in identifying, diagnosing, and appropriately treating patients with UI
EMG⫽electromyography; PFMT⫽pelvic floor muscle training; UI⫽urinary incontinence.
Clinical Guideline
Nonsurgical Management of Urinary Incontinence in Women43016 September 2014 Annals of Internal Medicine Volume 161 • Number 6 www.annals.org
T
REATMENTComplete continence, a clinically important
improve-ment in UI (defined as reducing UI frequency by
ⱖ
50%),
and quality of life were the primary outcomes assessed in
the systematic review to evaluate the effectiveness of
non-pharmacologic and non-pharmacologic treatments.
Nonpharmacologic Treatment
Appendix Table 1
(available at www.annals.org)
sum-marizes nonpharmacologic treatments.
Stress UI: Nonpharmacologic Treatment
PFMT Versus No Active Treatment.
High-quality
evi-dence showed that PFMT is an effective UI treatment
compared with no active treatment. Pooled data from
stud-ies that included women with stress UI (16 –18) showed
increased continence rates with PFMT compared with no
active treatment (number needed to treat for benefit
[NNT
B], 3 [95% CI, 2 to 5]). High-quality evidence
showed that PFMT was more than 5 times as effective as
no active treatment in improving UI (NNT
B, 2 [CI, 2 to
6]) (16, 19 –23). In addition, studies reported improved
quality of life (11).
PFMT With Biofeedback Using a Vaginal
Electromyog-raphy Probe Versus No Active Treatment.
Low-quality
evi-dence showed that PFMT with biofeedback using a vaginal
electromyography probe increased continence compared
with no active treatment (16, 20). High-quality evidence
showed that this treatment improved UI compared with
no active treatment (NNT
B, 3 [CI, 2 to 6]) (16, 19, 20,
24).
Other Treatments.
Evidence was insufficient to
deter-mine the effectiveness of vaginal cones and pessaries or of
intravaginal and intraurethral devices versus no active
treat-ment (11).
Urgency UI: Nonpharmacologic Treatment
Bladder Training Versus No Active Treatment.
Low-quality evidence showed that bladder training improved UI
compared with no active treatment (NNT
B, 2 [CI, 2 to 4])
(25, 26). However, evidence on bladder training for
achieving complete continence was insufficient (11).
Mixed UI: Nonpharmacologic TreatmentPFMT Versus No Active Treatment.
Pooled data from
studies that included women with mixed UI (18, 20, 27)
showed increased continence rates with PFMT compared
with no active treatment.
PFMT Plus Bladder Training Versus No Active
Treatment.
High-quality evidence showed that PFMT
combined with bladder training achieved continence
(NNT
B, 6 [CI, 4 to 16]) (28 –32) and improved UI
(NNT
B, 3 [CI, 2 to 6]) (28, 30 –32) compared with no
active treatment.
Continence Service Versus No Active Treatment.
Con-tinence service involves nurses and clinicians trained to
identify, diagnose, and appropriately treat patients with
UI. Moderate-quality evidence showed that this service
yielded no statistically significant improvement in
conti-nence compared with no active treatment (33–35).
Low-quality evidence showed no consistent statistically
signifi-cant improvement in UI (35, 36).
Weight Loss and Physical Activity Versus No Active
Treatment.
Moderate-quality evidence indicated that
weight loss and exercise improved UI in obese women
(NNT
B, 4 [CI, 2 to 18]) (37, 38).
Other Treatments.
Evidence was insufficient to
deter-mine the effectiveness of behavioral modification
pro-grams, a soy-enriched diet, or acupuncture for improving
UI in women with mixed UI (11).
Comparative Effectiveness of Nonpharmacologic Treatments
No evidence showed that one nonpharmacologic
treat-ment was superior to another in the various comparisons
assessed for stress, urgency, or mixed UI. Further details
are available in the full systematic review (11) and the
Supplement
.
Pharmacologic Treatment
Appendix Table 2
(available at www.annals.org)
sum-marizes pharmacologic treatments.
Stress UI: Pharmacologic Treatment
Nonsystemic Estrogen Therapy Versus Placebo.
Overall
evidence was insufficient to determine the effectiveness of
topical estrogen therapies at improving UI. Evidence
showed increased continence and improved UI with
vagi-nal estrogen formulations, but transdermal patches were
associated with worsened UI. Studies used a range of
estro-gen applications.
Urinary incontinence improved with vaginal estrogen
tablets (39) and vaginal ovules (40) compared with
pla-cebo. Vaginal estrogen tablets increased continence
com-pared with placebo (NNT
B, 5 [CI, 3 to 12]) (39 – 42). An
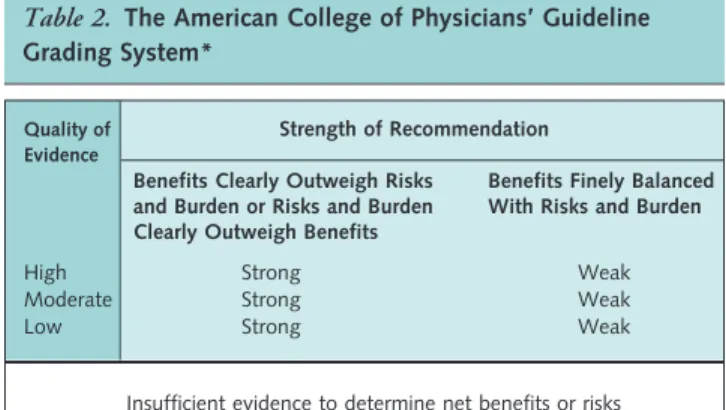
Table 2. The American College of Physicians’ Guideline Grading System*
Quality of Evidence
Strength of Recommendation Benefits Clearly Outweigh Risks
and Burden or Risks and Burden Clearly Outweigh Benefits
Benefits Finely Balanced With Risks and Burden
High Strong Weak
Moderate Strong Weak
Low Strong Weak
Insufficient evidence to determine net benefits or risks
*Adopted from the classification developed by the GRADE (Grading of Recom-mendations, Assessment, Development, and Evaluation) workgroup.
Clinical Guideline
Nonsurgical Management of Urinary Incontinence in Womenwww.annals.org 16 September 2014 Annals of Internal Medicine Volume 161 • Number 6 431 Downloaded From: http://annals.org/ on 07/30/2015
estradiol implant did not improve UI compared with
pla-cebo (41).
Intravaginal Estriol Plus PFMT Versus Intravaginal
Estriol.
Low-quality evidence from 1 study showed that a
combination of intravaginal estriol plus PFMT more
effec-tively achieved continence than intravaginal estriol alone
(NNT
B, 1 [CI, 1 to 2]) (43).
Duloxetine Versus Placebo.
Low-quality evidence
showed that continence was reduced less with duloxetine
than placebo (44, 45). High-quality evidence showed that
duloxetine did not statistically significantly improve UI
compared with placebo (NNT
B, 13 [CI, 7 to 143]) (44,
46 – 49). Low-quality evidence showed that duloxetine
im-proved quality of life (45, 49, 50). However, quality of life
did not improve in women with severe stress UI or
over-active bladder (46, 51).
Urgency UI: Pharmacologic Treatment With Antimuscarinics
Darifenacin Versus Placebo.
High-quality evidence
showed that darifenacin improved UI compared with
pla-cebo (NNT
B, 9 [CI, 6 to 18]) (52–54). Achieving
com-plete continence was not studied as an outcome with
dar-ifenacin treatment. High-quality evidence also showed that
darifenacin improved quality of life (11).
Fesoterodine Versus Placebo.
Moderate-quality evidence
showed that fesoterodine achieved continence more than
placebo (NNT
B, 8 [CI, 6 to 11]) (55–57). High-quality
evidence also showed an improvement in UI (NNT
B, 10
[CI, 7 to 18]) (56, 58 – 60). Low-quality evidence showed
that fesoterodine also improved quality of life (11).
Oxybutynin Versus Placebo.
High-quality evidence
showed that oxybutynin achieved continence more than
placebo (NNT
B, 9 [CI, 6 to 16]) (61– 65).
Moderate-quality evidence showed that this agent also improved UI
(NNT
B, 6 [CI, 4 to 11]) (24, 61, 62, 64, 66 –73).
Propiverine Versus Placebo.
Low-quality evidence
showed that propiverine achieved continence more than
placebo (NNT
B, 6 [CI, 4 to 12]) (74, 75), and
moderate-quality evidence showed that it improved UI (NNT
B, 5
[CI, 4 to 8]) (74 –76) compared with placebo.
Solifenacin Versus Placebo.
High-quality evidence
showed that solifenacin achieved continence more than
placebo (NNT
B, 9 [CI, 6 to 17]) (77– 81), and low-quality
evidence indicated that it resolved UI compared with
pla-cebo (NNT
B, 6 [CI, 4 to 10]) (81, 82). Low-quality
evi-dence from 1 study showed that higher doses of solifenacin
(10 mg/d vs. 5 mg/d) did not decrease the frequency of UI
episodes and were associated with increased risk for adverse
effects (83).
Tolterodine Versus Placebo.
High-quality evidence
showed that tolterodine achieved continence (NNT
B, 12
[CI, 8 to 25]) (55, 56, 84, 85) and improved UI (NNT
B,
10 [CI, 7 to 24]) (55, 56, 59, 86 –90) more than placebo.
Low-quality evidence showed that tolterodine improved
quality of life (11).
Trospium Versus Placebo.
High-quality evidence
showed that trospium achieved continence more than
pla-cebo (NNT
B, 9 [CI, 7 to 12]) (91–94). Low-quality
evi-dence did not show a statistically significant improvement
in UI compared with placebo (94, 95). Individual studies
showed that trospium improved quality of life (11).
Urgency UI: Pharmacologic Treatment With3-AdrenoceptorAgonists
Mirabegron Versus Placebo.
Moderate-quality evidence
showed that mirabegron achieved continence more than
placebo (NNT
B, 12 [CI, 7 to 29]) and improved UI
com-pared with placebo (NNT
B, 9 [CI, 6 to 17]) (96).
Low-quality evidence showed that higher doses of mirabegron
improved treatment satisfaction and quality of life
com-pared with lower doses (150 mg/d vs. 100 mg/d) (97).
Solabegron Versus Placebo.
Evidence was insufficient to
determine the effect of solabegron on continence or
im-proving UI, but low-quality evidence showed that it
de-creased the frequency of UI episodes in a dose-dependent
manner (98).
Urgency UI: Other Pharmacologic Treatments
Evidence was insufficient to determine the clinical
ef-fectiveness of resiniferatoxin or nimodipine compared with
placebo for treatment of UI (11).
Urgency UI: Comparative Effectiveness of Pharmacologic Treatments
Fesoterodine Versus Tolterodine.
Moderate-quality
evi-dence showed that fesoterodine achieved continence more
often than tolterodine (NNT
B, 18 [CI, 11 to 52]) (55, 56,
99). High-quality evidence showed that fesoterodine
im-proved UI more than tolterodine (NNT
B, 36 [CI, 17 to
1000]) (55, 56, 59, 90).
Oxybutynin Versus Tolterodine.
Low-quality evidence
showed no difference between oxybutynin and tolterodine
for achieving continence (100). Moderate-quality evidence
showed no difference for improving UI (66, 68, 100, 101).
Tolterodine Versus Trospium.
Low-quality evidence
from 1 study showed that tolterodine and trospium were
similarly effective at treating urgency UI (100).
Solifenacin Versus Tolterodine.
Evidence was
insuffi-cient to compare solifenacin with tolterodine for effects on
continence or improvement of UI (11).
Trospium Versus Oxybutynin.
Low-quality evidence
showed no differences between trospium and oxybutynin
for effects on continence or improvement of UI (100).
Other Comparisons.
Evidence was insufficient to
de-termine the comparative effectiveness on continence or
im-provement of UI for darifenacin, propiverine, solifenacin,
or
flavoxate
versus
oxybutynin;
solifenacin
versus
darifenacin; or tolterodine or solifenacin versus propiverine
(11).
Clinical Guideline
Nonsurgical Management of Urinary Incontinence in Women43216 September 2014 Annals of Internal Medicine Volume 161 • Number 6 www.annals.org