A CLINICAL STUDY OF 100 CASES OF
HERPES ZOSTER
Dissertation Submitted in
fulfillment of the university regulations for
MD DEGREE IN
DERMATOLOGY, VENEREOLOGY AND LEPROSY
(BRANCH XII A)
THE TAMILNADU DR.M.G.R.MEDICAL UNIVERSITY
CHENNAI
CERTIFICATE
Certified that this dissertation entitled
“A CLINICAL STUDY OF
100 CASES OF HERPES ZOSTER”
is a bonafide work done by
DR. C. CHANDRAKALA,
Post Graduate Student of the department of
Dermatology, Venereology and Leprosy, Madras Medical College,
Chennai – 600 003, during the academic year 2005 – 2008. This work has
not previously formed the basis for the award of any degree.
Prof. Dr. B. PARVEEN, MD. DD,
Professor
and
Head
of
the
Department,
Department
of
Dermatology
and
Leprology,
Madras
Medical
College,
Chennai-600003.
Prof.Dr.T.P.KALANITI , M.D.
Dean,
SPECIAL ACKNOWLEDGEMENT
My sincere thanks to
Prof. Dr. T.P. KALANITI M.D.,
the Dean
of Madras Medical College for allowing to do my dissertation and to utilize
ACKNOWLEDGEMENT
I am gratefully indebted to
Prof.Dr.B.PARVEEN, MD.DD,
Professor and Head, Department of Dermatology and Leprology for her
invaluable guidance, motivation and help throughout the study. I would
like to express my sincere and heartfelt gratitude to Professor
Dr.V.S.DORAIRAJ, M.D., D.V.,
and Director in charge, Institute of
Venereology.
I wish to thank
Dr.N.Gomathy M.D., D.D
., Former Professor,
Department of Dermatology and
Dr.N.Usman M.D., D.V., PhD
, Former
Director, Institute of Venereology for their constant support and motivation.
I am grateful to
Dr.S.Jayakumar M.D., D.D.
, Additional Professor,
Department of Dermatology for his invaluable guidance and help. I sincerely
thank
Dr.C.Janaki M.D.,D.D.
, Reader in Dermatology (Mycology) for her
priceless support. I thank Additional Professor
Dr.N.Kumar M.D., D.V.,
D.M.R.D
., Institute of Venereology for his guidelines.
I express my earnest gratitude to
Dr.D.Prabhavathy MD.DD,
Professor and Head, Department of Occupational Dermatology and
Dr.S.V.Somasundaram MD.DD,
Additional
Professor, Department of
Occupational Dermatology and Contact Dermatitis for his benevolent help
and support.
My sincere thanks go to
Dr.G.K.Tharini,M.D., Dr.V.Anandan
M.D.D.C.H.D.N.B.(Paediatrics), Dr.R. Priyavathani, M.D., D.D.,
D.N.B., Dr. N.Hema, M.D. and Dr.S.Anupama Roshan D.D.V.L
,
Assistant Professors, Department of Dermatology for their kind support and
encouragement.
I thank
Dr. A. Hameedullah, M.D., D.D., Dr.S. Kumaravelu, M.D.,
D.D., Dr. J. Manjula, M.D., DNB and Dr. Afthab Jameela Wahab M.D.,
D.D
., Assistant Professors for their support and help.
I am inclined to thank
Dr.V.Thirunavukarasu M.D.,D.V
.,
Dr.K.Venkateswaran M.D.,D.V., Dr.S.Thilagavathy M.D.,D.V.,
Dr.P.Mohan, M.D., D.V., Dr.S.Arunkumar M.D.. D.V., Dr.P.Prabahar,
M.D.D.V.L.,
and
Dr.S.Kalaivani M.D.D.V.,
Assistant Professors,
Department of Venereology, for their help and suggestions.
I express my sincere gratitude to
Dr.K.Rathinavelu MD., DD.,
I duly acknowledge the paramedical staff and my colleagues for their
help and favours. Last but not the least I am profoundly grateful to all
CONTENTS
S.No. Title
Page
No.
1. INTRODUCTION
1
2. REVIEW
OF
LITERATURE
3
3.
AIMS OF THE STUDY
42
4.
MATERIAL AND METHODS
43
5.
OBSERVATION AND RESULTS
46
6. DISCUSSION
62
7. CONCLUSION
68
BIBLIOGRAPHY
PROFORMA
MASTER
CHART
1
INTRODUCTION
Varicella-Zoster virus (VZV) is the etiologic agent of two
diseases, Varicella (Chicken pox) and Zoster (Shingles).
Varicella which occurs after the initial encounter with
Varicella Zoster virus, is a disease manifested by a pruritic rash
accompanied by fever and other systemic signs and symptoms that
are usually mild to moderate nature.
Most often Varicella is a self-limited infection of childhood.
Zoster is mainly a disease of adults. A prerequisite for
developing zoster is a prior episode of Varicella, which on occasion
may have been sub-clinical.
During Varicella, VZV establishes latent infection in sensory
nerve ganglion. Zoster results when the latent virus reactivates and
returns from the ganglion to infect the skin.
Most often VZV reactivates in the settings of relative
immunologic compromise, as occurs with aging, or following
disease or various therapies, such as steroids, cancer chemotherapy
2
The diagnosis is clinical: very few other diseases mimic
herpes zoster, especially in the localization of the rash, which is
otherwise quite similar in appearance and initial effect of that of
poison oak or poison ivy.
In case of doubt, diagnostic tests can be performed. Such lab
tests may be necessary because, depending on the affected sensory
nerve, the pain that is experienced before the onset of rash may be
misdiagnosed as pleurisy, myocardial infarction, appendicitis or
migraine headache.
A physician can take a viral culture of a fresh lesion, (or)
perform a microscopic examination of the blister base material
called a Tzanck preparation.
In a complete blood count, there may be an elevated number
of white blood cells, which is an indirect sign of infection. There
may also be a rise in the antibody to the virus, which could also give
indication to the virus.
Currently, there is no complete cure available for herpes
zoster, nor a treatment to effectively eliminate the virus from the
body. However, there are some treatments that can mitigate the
3
REVIEW OF LITERATURE
HISTORICAL OVERVIEW:
Varicella was distinguished clinically from small pox in the
mid 18th century. The origin of the name chickenpox is uncertain,
but it may have been derived from the French “pois chiche” or chick
pea or from the farmyard fowl (in old English cicen and Middle
High German kuchen). The name ‘shingles’ is derived from the
Latin word ‘cingulus’ meanings girdle (Zaia, 1981)
Herpes is derived from the Greek word meaning to “creep”.
Zoster is the Greek word meaning “girdle or belt”.
In 1875, Steiner successfully transmitted VZV by inoculation
of the vesicular fluid from a person suffering from chickenpox to -
“volunteer”1.
The delineation of the link between Varicella and zoster is of
virologic, medical and historical interest. A connection was
postulated in 1888 by Von Bokay2 who recognized that cases of
Varicella often occurred following exposure to a patient with zoster.
Kundratitz in 19253 showed that the inoculation of vesicular fluid
from patients with herpes zoster into susceptible person resulted in
4
In 1943 Garland4 suggested that herpes zoster was the
consequence of the reaction of latent VZV.
Since early in the 20th century, similarities in the
histo-pathologic feature of skin lesions and in epidemiologic and
immunologic studies indicated that Varicella and herpes zoster
were caused by the same agent5.
Tyzzer6 described the histo-pathologic features of skin lesions
resulting from VZV injections and noted the appearance of
intranuclear inclusions and multinucleated giant cells.
The histopathologic descriptions were amplified by Lipschutz
in 19217 for herpes zoster.
Isolation of VZV in 1958 permitted a definition of the biology
of this virus8.
By 1958, Weller and colleagues8 had been able to establish
that there were neither biologic nor immunologic differences
between the viral agents isolated from patients with chickenpox
and herpes zoster.
Viral DNA from a patient with chickenpox who subsequently
developed herpes zoster was examined by restriction endonuclease
analysis and the molecular identity of these two viruses was
5
Hope-Simpson10 was the first to recognize the importance of
the immune system in controlling manifestations of zoster. He
postulated that zoster resulted when humoral immunity to VZV
wanes in the years and decades after Varicella.
More recently the importance of declining cellular rather
than humoral immunity to VZV was recognized in the pathogenesis of
zoster10.
Cyto-diagnosis of herpes infection by smear taken from the base
of a blister reveals the characteristic cytopathic effects of herpetic
infection and multinucleated giant cells were introduced by Tzanck in
194711.
Before the availability of antiviral drug, oral pancreatic
enzyme therapy in shingles was used in some countries and later
subjected to clinical and scientific research12. A large scale study,
using an oral preparation of such enzymes has shown promising
results.
Antiviral drugs Acyclovir was discovered in 1974. Preclinical
investigation brought the drugs to clinical trials in 1977 and the
first form of drug (topical) was available in 198213.
A live attenuated vaccine using the same strain (Oka strain)
6
efficacy in terms of reducing shingles and post-herpetic neuralgia
incidences, of 51% and 67% respectively14. This vaccine received a
marketing authorization in France for adults more than 60 years of
age.
VIROLOGY:
Varicella – Zoster Virus
VZV is a member of the herpesviridae family and shares
structural characteristics with other members of the family. The
virus has icosapentahedral symmetry and contains DNA with a
surrounding envelope. The size of the virus is approximately 150
to 200nm.
The nucleo capsid has a diameter of approximately 90 to 95
nm15, consisting of 162 hexagonal capsomeres with central axial
hollow organised as an icosahedron with 5:3:2 axial symmetry16.
A biological important coat, the tegument, surrounds the
nucleocapsid, which in turn is surrounded by an envelope that is
derived in part from cellular membranes. The glycoproteins (gps)
are termed I through VI. These glycoproteins have been the subject
of intense investigative interest because they represent the primary
7
VZV replicates in the nuclei of infected cells, where the DNA
core and capsid are synthesized17.
EPIDEMIOLOGY:
Herpes zoster is a disease that occurs at all ages, but it afflicts
about 20% or more of the population overall, mainly the elderly9.
The highest incidence of disease varies between 5 and 10 cases per
1000 for persons older than 60 years18.
The incidence of zoster in children is low. Hope-Simpson29
reported a rate of 0.74 per 1000 subjects per year in the age group
9. Guess30 et al all noted that the rate increased from 20 cases per
1,00,000 person - years in the age group younger than 5 years to 63
cases per 1,00,000 person - years in the group aged 15 to 19 years.
Immunocompromised persons have a higher incidence of
both chickenpox and shingles19. Both sexes are equally affected.
Geographic and racial factors have been reported in studies of the
epidemiology of Varicella and herpes zoster. Non – Caucasian
racial group and tropical region people were each significantly
associated with younger age at Zoster onset in a study conducted by
Nagasako et al21. It is a sporadic disease occurring throughout the
year. Contagiousness of infection from zoster patient is low, as
secondary attack rate within household non-immune contacts is
8
PATHOGENESIS:
Primary viraemia of VZV:
Airborne droplets are the usual route of transmission of
primary Varicella (chickenpox). The incubation period ranges from
11 to 20 days. Varicella is extremely contagious with 80 to 90% of
susceptible household contacts developing clinical infection.
VZV enters individual by infection of mucosal epithelial cells
in the upper respiratory tract, oropharynx or conjunctiva. After
primary replication in the epithelium, the virus is disseminated by
the blood stream to the reticulo-endothelial system, where viral
replication leads to secondary viremia. Infection of capillary
endothelial cells allows spread of the virus to epithelial cells of the
epidermis, where focal cutaneous lesions of Varicella are formed.
Host immunity limits the acute disease but during spread
through the epidermal epithelium, the virus also infects sensory
nerve endings and is transported to sensory ganglia. Latent
infection is established in the ganglia, neurons and satellite cells23.
LATENCY AND REACTIVATION:
VZV evades the immune response to establish latency in an
9
there. It is believed that latent infection is established in a host cell
that is non permissive for viral gene transcription.
The configuration of VZV DNA in latently infected ganglia is
extra chromosomal and circular24. Herpes zoster appears upon
re-activation of VZV which may occur spontaneously or may be
induced by stress, fever, radiation therapy, surgery, tissue damage
or immune suppression25.
During herpes zoster reactivation, the virus continues to
replicate in the dorsal root ganglion and produces a painful
ganglionitis. Inflammation and neuronal necrosis can result in
severe neuralgia that intensifies as the virus spreads down the sensory
nerve. If the existing immune response cannot control the
re-activating virus, extensive viral replication can occur in the ganglia.
Virus also spreads to the periphery by axonal transport
through neurons innervating a specific dermatome or dermatomes.
There the virus productively infects the epithelium to cause the
10
HISTO - PATHOLOGY
SKIN LESIONS: I. Early stage:
The earliest changes involve the epidermal cell nuclei which
develop peripheral clumping of chromatin and a homogenous
ground glass appearance, combined with ballooning of nucleus26.
Vacuolization is the earliest cytoplasmic alteration. These
changes begin focally along the basal layer, but soon involve the
entire epidermis26.
II. Vesicular Stage:
Intra epidermal vesicle results from two types of degenerative
changes. 1). Ballooning degeneration & 2). Reticular degeneration.
Ballooning degeneration is peculiar to viral vesicles. The
affected cells swell and loose their attachment to adjacent cells,
thus separating from them (secondary acantholysis)25.
The cytoplasm of these cells becomes homogenous and
intensively eosinophilic and some are multinucleate (Tzanck cells)
11. At times the basal layer of the epidermis is also destroyed in this
11
Reticular degeneration25 is characterized by progressive
hydropic swelling of epidermal cells, which become large and clear
with only fine cytoplasmic strands remaining at the edge of the
cells. These eventually rupture contributing further to the
formation of a vesicle.
Whereas ballooning degeneration is found mainly at the base
of the vesicle, reticular degeneration is seen on its superficial
aspect and margin. Multinucleated giant cells containing upto 15
nuclei which are formed by fusion of epithelial cells containing
eosinophilic intranuclear inclusion bodies (Lipschutz bodies,
formerly Cowdry type A bodies)27 of 3 to 8 mm in diameter.
III. Late stage:
Eosinophilic intra nuclear inclusion bodies are found,
particularly in ballooned cells. Neutrophils are present within
established vesicles. Neutrophilic and lymphocytic infiltration is
also present in the underlying dermis. Marked inflammation and
vasculitis28 have been noted in some lesions. If the vasculitis is
severe, necrotizing lesions will be present. Eccrine duct
involvement has been reported. The chronic verrucous lesions show
hyperkeratosis, verruciform acanthosis and virus-induced
12
IMMUNOLOGY
Both humoral and cell mediated immune responses to VZV
develop within a few days after the onset of varicella.
Peak antibody levels are attained after 4 to 8 weeks; remain
high for about 6 months and then decline. IgG Ab to VZV can be
detected in healthy adults for decades after varicella30. After active
immunization against varicella antibody titers are lower than after
natural infection but persists for as long as 20 years in healthy
children. Serum IgG, IgA and IgM develop after both varicella and
zoster. Zoster occurs in the face of high levels of specific antibodies,
but significantly higher titers develop during convalescence,
reflecting an anamnestic response to this reactivation infection31.
Antibodies seem to have an incomplete protective effect. Cellular
immunity is thought to play the major role in host defense against VZV.
Natural killer cells and antibody dependent cellular cytotoxicity
against VZV have also been described. It is generally agreed that
CMI, presumable T cell cytotoxicity is more important than humoral
13
CLINICAL MANIFESTATIONS Pre - eruptive Stage:
The first manifestation of zoster is usually pain, which may be
severe and may be accompanied by fever, headache, malaise and
tenderness localized to areas of one or more dorsal roots.
The time between the start of the pain and the onset of
eruption averages 1.4 days in trigeminal zoster and 3.2 days in
thoracic disease33. The skin in the affected area becomes red and
papules soon develop34. Occasionally the pain is not followed by the
eruption (zoster sine eruptione, zoster signe herpete)35.
In the pre eruptive stage the pain simulates headache, eye
pain, dental pain, pleurisy, brachial neuritis, cardiac pain, intra
abdominal disease (especially gall bladder colic, appendicitis, renal
colic, etc.) or sciatic syndrome. Prodromal symptoms may be
absent, particularly in children36.
ERUPTIVE STAGE:
Closely grouped red papules, rapidly becoming vesicular and
then pustular develop in a continuous or interrupted band in the
area of one, occasionally two and rarely more contiguous dermatomes.
Mucous membranes within the affected dermatomes are also
14
and tender. Occasionally a few vesicles appear across the midline36.
Rarely eruption may be bilateral.
Dermatome involvement in Herpes zoster:
Thoracic - 53% (Commonest)
Cervical - 20%
Ophthalmic - 16%
Lumbosacral - 11%
Possibly because chicken pox is centripetal (located on the
trunk), the thoracic region is affected in two thirds of herpes zoster
cases36.
RESOLUTION STAGE:
The pain and constitutional symptoms subsides gradually as
the eruption subsides, vesicles either umblicate or rupture before
forming a crust, which falls off in 2 to 3 weeks.
In uncomplicated cases the recovery is complete in 2 to 3
weeks in children and young adults and 3 to 4 weeks in older
15
CEPHALIC ZOSTER:
This includes involvement of cranial nerves, such as
trigeminal nerve branches, facial nerve, auditory nerve,
glossopharyngeal and vagal nerves.
TRIGEMINAL NERVE ZOSTER
It is due to involvement of Gasserian ganglion of the
trigeminal nerve. Three branches of the trigeminal nerve such as
ophthalmic, maxillary and mandibular divisions are affected by
Herpes Zoster.
HERPES ZOSTER OPHTHALMICUS:
Herpes zoster ophthalmicus occurs when the recrudescence is
in the ophthalmic branch of the trigeminal nerve. The ophthalmic
involvement makes up to 10 to 15% of all cases of herpes zoster. V1
area involves forehead and upper eyelid. Infection involving the
cornea with keratitis and uveitis and may lead to permanent
damage. This presentation occurs when the nasociliary branch of
ophthalmic division is involved and accordingly presents with
cutaneous involvement of the nasal tip (Hutchinson’s sign)37.
Frontal sinusitis preceded 16% of all cases of ophthalmic
zoster38. Patients with ophthalmic herpes zoster who are HIV
16
than those who are HIV positive39.Herpes zoster ophthalmicus is a
known marker of HIV/AIDS in Africa40.
HERPES ZOSTER OF MAXILLARY DIVISION OF TRIGEMINAL NERVE:
Zoster of maxillary division of the trigeminal nerve produces
vesiculation of the tonsillar area, cheek, lower eyelid, side of the
nose, upper lip as well as mucosa of nose, nasopharynx, palate,
uvula and tonsillar area41.
HERPES ZOSTER OF MANDIBULAR BRANCH OF TRIGEMINAL NERVE:
The dermal and mucous membrane distribution of this
branch is to the side of the head, part of the external ear and
external ear canal, lower lip, anterior part of the tongue, floor of
the mouth and buccal mucous membrane. In oro facial zoster
toothache may be the presenting symptom.
HERPES ZOSTER OTICUS/ RAMSAY-HUNT SYNDROME:
The facial nerve, mainly a motor nerve, has vestigial sensory
fibres supplying the external ear (including pinna and meatus),
tonsillar fossa and adjacent soft palate. Classical sensory nerve
zoster in these fibres causes pain and vesicles in part or all of that
distribution, though the skin involvement may be minimal and
17
Swelling of infected sensory fibres in their course through the
confined spaces of the facial canal and the internal auditory
meatus, leading to compression of adjacent facial nerve motor
fibres resulting in facial palsy, which with the ear pain and
associated vesicle completes the classic triad of Ramsay-Hunt
syndrome42.
Auditory nerve involvement occurs in 37.2% of patients
resulting in hearing deficits and vertigo43.
GLOSSOPHARYNGEAL AND VAGAL ZOSTER (HERPES PHARYNGITIS AND HERPES LARYNGIS) 62:
This type involves the jugular and petrosal ganglia. Because
these two ganglia are adjacent, they are often involved in some
combination together but may be affected separately. The vesicular
rash is likely to be on the palate, back of the tongue, epiglottis or
faucial tonsils and occasionally in the external ear.
Palatal weakness, dysphonia, difficulty in swallowing,
hyperesthesia in pharynx, loss of gag reflex, etc may occur. There is
usually ear or deep pharyngeal or laryngeal pain.
HERPES OCCIPITOCOLLARIS (INVOLVEMENT OF C2 AND C3)44
The skin lesions seen over the back of scalp, back of neck,
part of the ear and part of the lower jaw and front of neck. C2 and
18
of C2 and C3 with VII and X cranial nerves. Combinations of C2 and
C3 with these cranial nerves are possible.
ZOSTER MENINGO ENCEPHALITIS:
This manifestation is most likely to be marked when cranial
nerves (especially Trigeminal Nerve) are involved. This is because
of a branch (recurrent nerve of Arnold) to the tentorium from
ophthalmic branch of Trigeminal Nerve. Hence meningeal reaction
(i.e. headache, changes in sensorium , fever, stiffness of neck , etc)
is most common with herpes zoster ophthalmicus.
SACRAL ZOSTER (S2, S3 AND S4 DERMATOMES):
A neurogenic bladder with urinary hesitancy or urinary
retention45 has reportedly been associated with zoster of the sacral
dermatomes S2, S3 and S4. Migration of virus to the adjacent
autonomic nerves is responsible for these symptoms.
BILATERAL HERPES ZOSTER46
Herpes zoster is almost always unilateral. The rarity of
bilateral cases is indicated by individual case reports in the
literature.
HERPES ZOSTER WITH MULTIPLE UNILATERAL LESIONS47
This type is quite rare and most likely to be noted in persons
19
metastatic cancer, HIV, etc. Such diseases should be looked for
when this dermal distribution is encountered.
RECURRENT HERPES ZOSTER48
Recurrent attacks are rare and zosteriform herpes simplex
should always be ruled out49.
ZOSTER IN MALIGNANCY:
Herpes zoster has been reported with Hodgkin’s, lymphomas,
leukemia, metastatic cancer and other neoplasm. The presence of
Herpes zoster especially in an older person indicates the need for
searching for these diseases as a causative background. Use of
cytotoxic immunosuppressant therapy altering immune response
may also be a factor.
HERPES ZOSTER IN HIV INFECTION
Herpes zoster is included in clinical stage - 2 of WHO staging
system for HIV infection.
Herpes zoster occurring in HIV disease is usually typical in
involving one or two adjacent dermatomes but uncommonly it may
be multidermatomal, recurrent within the same dermatome or
disseminated50. The eruption may be bulbous, hemorrhagic,
20
The majority of HIV infected patients with herpes zoster
experience an uneventful recovery; however atypical clinical course
of herpes zoster is not uncommon50. Lesions may persist for
months, either in localized or disseminated form, appearing as
hyperkeratotic, ulcerated, painful nodules, often with central
crusting or ulceration with a border of vesicles51. Systemic
dissemination of herpes zoster with hepatitis, encephalitis and
pneumonitis is common. HIV infected patients with herpes zoster
show increased neurologic and ophthalmic complications
particularly peripheral retinal necrosis52. Reactivation of varicella
zoster virus is the commonest cutaneous manifestation of immune
restoration disease53.
HERPES ZOSTER IN CHILDREN
Herpes zoster in neonates and children may represent the
result of an attenuated response to intra uterine or neonatal
infection. Baba et al54 reported that children who had varicella
before 2 months of age has lower varicella zoster antibody titers
and diminished skin test reactions; thus reactivation in these cases
may be secondary to an abnormal immune response to the primary
infection by varicella.
The development of herpes zoster is often preceded by
21
and fever may precede the rash, particularly in younger patients.
Resolution of lesion occur within 1 to 3 weeks.
Both normal and immunosuppressed patients may have
generalization of herpes zoster. Post herpetic neuralgia is
uncommon in children. Immunocompromised children with herpes
zoster may have more extensive involvement with a higher risk of
viremia and visceral dissemination.
HERPES ZOSTER IN PREGNANCY:
Herpes zoster during pregnancy, whether it occurs early or
late in the pregnancy, appears to have no deleterious effects on
either the mother or infant55. Maternal zoster in pregnancy is not
associated with intra uterine infection56. But maternal Varicella in
the first 20 weeks of pregnancy is associated with a approximate
2% risk of fetal damage57.
COMPLICATION
1. Acute complications of herpes zoster:
Acute complications occur during the course of illness and
are more common in immunocompromied individuals.
22
The common cutaneous complications are secondary bacterial
infections, cutaneous necrosis, scarring, dissemination and gangrene
formation.
ii. Ocular Complications58
Ocular complications include uveitis, keratitis,
conjunctivitis, conjunctival edema, ocular muscle palsies,
proptosis, scleretis, retinal vascular occlusion and ulceration,
scarring and even necrosis of the lid. Involvement of ciliary ganglion
may give rise to Argyl-Robertson pupil.
Acute retinal necrosis caused by Varicella-zoster virus
occasionally occurs in immuno-competent patients, although more
recent studies have focused on ocular disease in HIV infected patients59.
iii.
Neurological Complications:This includes cranial neuritis, motor neuropathy autonomic
neuropathy, aseptic meningitis, meningo-encephalitis,
transverse myelitis60, necrotizing myelopathy, Guillain-Barre
Syndrome, hemiplegia and granulomatous angiitis.
a) Cranial Neuritis:
Cranial neuritis includes trigeminal nerve zoster (Herpes
23
Ramsay-Hunt syndrome with involvement of facial nerve and 8th
cranial nerve, vagus and glossopharyngeal nerve zoster.
b) Motor Neuropathy:
This occurs overall in 5% of cases and is more common in
older patients and those with malignancy and in cranial when
compared with spinal nerve involvement. The motor weakness
usually follows the pain and the eruption by a few days to a few
weeks, but occasionally precedes or accompanies them. The
affected segment is usually but not always the same. Complete
recovery is expected in 55% and significant improvement in a
further 30% of cases. In ophthalmic zoster, ocular palsies occur in
13% and facial palsies in 7%61. An abdominal hernia followed zoster
involving thoracic 10th and 11th motor roots62. zoster of ano-genital
area may be associated with disturbances of defecation or
urination63. Herpes zoster oticus accounts for about 10% of cases
facial palsy64. Glossopharyngeal65 and vagal zoster66 produces
pharyngeal and palatal muscle weakness. Zoster of the second to
fourth cervical nerves may paralyze the ipsilateral diaphragm due
to involvement of the phrenic nerve.
24
Autonomic nervous system may also be affected. Autonomic
nerve involvement often presents as bladder dysfunction.
Gastro-intestinal tract involvement presents as spasm, hypotonia or ileus.
d) Herpes zoster Meningo - encephalis
Neurologic symptoms characteristically appear within the
first 2 weeks of onset of the skin lesions. Patients at risk are those
with trigeminal and disseminated zoster as well as the
immunosuppressed. Rarely manifestations of a
meningo-encephalitis may be significant and at times severe enough to cause
death.
e) Granulomatous angiitis67 (or) Delayed contra-lateral
hemiparesis:
By direct extension along the intracranial branches of the
trigeminal nerve, VZV gains access to the CNS and infects the
cerebral arteries. Patients present with headache and hemiplegia.
f) Herpes zoster Myelitis:
More rarely, the myelitis lesion predominates in zoster or is
the sole feature, so the clinical picture is one of acute onset of
paraplegia from a diffuse involvement of the spinal cord. The
25
iv. Visceral Complications:
Patients with lympho-proliferative malignancies are at risk
for cutaneous dissemination and visceral involvement, including
Varicella pneumonitis, hepatitis and meningo-encephalitis.
2. Complications occurring after resolution of Herpes
Zoster lesions:
i. Post Herpetic Neuralgia
The commonest and most intractable sequel of zoster is
Post-herpetic neuralgia, generally defined as persistence or recurrence of
pain for more than a month after the onset of zoster, but better
considered after 3 months. It occurs in about 30% of patients over
40 years of age and is most frequent when trigeminal nerve is
involved68.
The pain has two main forms, a continuous burning pain with
hyperaesthesia and spasmodic shooting type, although a pruritic
“crawling” paraesthesia may occur. Allodynia, pain caused by
normally innocuous stimuli, is often the most distressing symptom
and occurs in 90% of people with post herpetic neuralgia68.
26
A number of different overlapping mechanisms appear to be
involved in the pathogenesis of pain in herpes zoster and post
herpetic neuralgia68.
Injury to the peripheral nerves and to neurons in the ganglion
triggers afferent pain signals. Inflammation in the skin triggers
nociceptive signals that further amplify cutaneous pain. The
abundant release of excitatory aminoacids and neuro-peptides
induced by the sustained barrage of afferent impulses during the
prodrome and acute phase of herpes zoster may cause excito-toxic
injury and the loss of inhibitory inter-neurons in the spinal dorsal
horn.
ii. Post Herpetic Itch69:
Many patients with shingles experience neuropathic itch
accompanying pain or itch may be present instead of pain.
iii. Progressive multifocal leuko-encephalopathy
In addition to latent infection, VZV can produce prolonged
smouldering sub-clinical infection in patients lacking normal
defenses to eliminate the viral infected cells and resulting in cell to
cell spread of infection.
27
Elderly, malnourished, debilitated or immuno-suppressed
patients tent to have a more virulent and extensive course of
disease and Scarring. Sometimes keloidal or hypertrophic scars
28
v. Inflammatory skin lesions following a zoster infection
(Isotopic Response)
Following zoster, inflammatory skin lesions may rarely occur
within the affected dermatome. Lesions usually appear within a
month and rarely, longer than 3 months after zoster.
Lesions reported in herpes zoster scar include a keloid,
comedones, lichen planus, giant cell lichenoid dermatitis, urticaria,
granulomatous vasculitis, granulomatous folliculitis, sarcoidosis,
lichen sclerosis et atrophicus, morphoea, eosinophilic dermatosis,
fungal infections, pseudolymphoma, lymphoma, leukemia cutis,
Rosai-Dorfman disease, Kaposi’s sarcoma, various skin cancers and
29
DIAGNOSIS OF HERPES ZOSTER
CLINICAL DIAGNOSIS
The diagnosis is largely clinical. Grouped vesicles of varying
sizes on an oedematous and erythematous base with skipped areas
of normal skin in a dermatomal distribution makes the diagnosis of
herpes zoster, quiet obvious most of the times.
INVESTIGATIONS:
1. Morphological test
Tzanck Smear:
The initial test of choice is a cytological smear (Tzanck
smear). The test does not differentiate herpes simplex from
varicella. The base of an early lesion is scraped and stained with
haematoxylin and eosin, Giemsa, Wright’s stain, toluidine blue or
papanicolaou stain. Multinucleated giant epithelial cells and
epithelial cells containing acidophilic intranuclear inclusions are
seen.
2. Skin Biopsy:
Histo-pathological appearances of herpes simplex, varicella
and herpes zoster are very similar. Ballooning degeneration is
30
mainly at the base of the vesicle, reticular degeneration is seen on
its superficial aspect and margin.
3. Virological Investigations:
a) Viral Culture:
The most definitive test is a positive viral culture from
vesicular fluid, but a minimum of 48 to 72 hours is required to
produce the diagnostic cytopathic effects. Infective material is
inoculated into human amnion, human fibroblast, HeLa71 or Vero
cells.
b) Varicella zoster virus antigen detection:
VZV antigen may be demonstrated by immunoflourescence,
using a commercially available monoclonal antibody to VZV that is
conjugated to flourescin72.
c) Electron Microscopy:
The ultra-structural features of Varicella zoster virus are
similar to those of Herpes simplex virus. However colloidal gold
immuno-electron microscopy using monoclonal antibodies can
31
4. Serological Tests:
A number of sensitive serologic tests are available to measure
antibodies to VZV)
Serologic tests include
1. Fluorescent antibody to membrane antigens (FAMA)
2. Latex agglutination test
3. Enzyme linked immunosorbent assay (ELISA)
4. Enzyme Immuno assay (EIA)
5. Immune adherence haemagglutination assay (IAHA)
6. Radio Immuno assay (RIA)
7. Complement fixation test (CFT)
8. Varicella zoster virus neutralization tests.
5. Newer Techniques:
i. Nucleic acid probes
The nucleic acid hybridization test has also been described
for the detection of Varicella zoster virus DNA sequences in clinical
specimens. The spot hybridization assay used was comparable to
32
ii. Polymerase Chain Reaction:
PCR is more sensitive than viral culture or Tzanck smear for
detecting VZV infections. PCR was described as particularly useful
for the rapid and specific diagnosis of VZV infections without the
practical and technical limitations of conventional viral isolations
33
TREATMENT
The aim of treatment is the suppression of inflammation,
pain and infection.
TOPICAL TREATMENT:
During acute phase of herpes zoster, the application of wet
compresses, calamine lotion, Burrow’s solution cornstarch, or
baking soda may help to alleviate local symptoms and hasten the
drying of vesicular lesions.75
Topical Acyclovir
Topical treatment of herpes zoster rash with antiviral agents
is not effective75
Systemic Therapy
The major goals of therapy in patients with herpes zoster are
to limit the extent, duration and severity of pain and rash in the
primary dermatome and to prevent disease elsewhere and PHN.
SYSTEMIC ANTIVIRAL AGENTS 1. ACYCLOVIR
Oral acyclovir significantly reduced the healing time,
duration of viral shedding and acute pain in randomized controlled
34
72 hours of rash onset76. Aciclovir is a guanosine analogue and is
widely used for the treatment of HSV and VZV infections.
MECHANISM OF ACTION:
The active antiviral moiety aciclovir is aciclovir triphosphate,
which is a potent inhibitor of certain herpesvirus induced DNA
polymerases, but has relatively little effect on host cell DNA
polymerase.
INDICATIONS AND DOSAGE:
Varicella zoster virus is less sensitive to aciclovir than HSV,
higher doses of the drug should be used.
ORAL:
Indications:
1. Immunocompetent persons with age 50 years or
above25.
2. Immunocompetent patients with ophthalmic zoster.
3. Localised zoster (one or two dermatome) in asymptomatic
35
Dosage:
800 mg 5 times a day (in adults) or 20 mg/kg every 6 hours
(in children) for 7 days in immunocompetent individuals and 10
days for immunocompromised.
INTRAVENOUS ACICLOVIR:
1. Disseminated or localized zoster involving more than 3
dermatomes in immunocomprised patients.
2. Chronic, severe zoster in advanced AIDS patients77.
3. Zoster involving cranial nerves with complications such
as Ramsay - Hunt Syndrome25 or Ophthalmic zoster in
HIV patients77.
4. Visceral dissemination25.
5. Localised zoster in HIV positive patients with impaired
intestinal function (i.e. diarrhea or malabsorption)
where intravenous route is preferred to ensure adequate
drug level.
6. Herpes Zoster encephalitis
Dose: 500mg/m2 in children or 10mg/kg body weight in
36
2. VALACYCLOVIR:
It is the L-valine ester of aciclovir. It was developed to provide
increased oral bioavailability of aciclovir78. Valacyclovir may be more
effective in resolution of zoster associated pain79. Dose: 1 gm tds for 7 days.
3. FAMCICLOVIR AND PENCICLOVIR:
Famciclovir is a prodrug of pencilovir. Penciclovir is
phosphorylated to penciclovir triphosphate. Penciclovir
triphosphate inhibits viral DNA polymerases and also inhibits
extension of the nascent viral DNA chain80. Dose: Farmciclovir
500mg tid for 7 days.
4. FOSCARNET (TRISODIUM PHOSPHONOFORMATE)
It is a pyrophosphate containing compound that is active in
vitro against varicellar zoster virus. Forcarnet noncompetitively
inhibits viral DNA polymerases at the pyrophosphate binding81
sites.
Dosage:
Initial dosage of 40 to 60mg / kg administered intravenously, 8th
hourly for 14 to 21 days followed by a maintenance dose of
37
5. CIDOFOVIR:
It is a phosphonate nucleotide analogue. It has activity
against a broad range of herperviruses.
Cidofovir does not require initial phosphorylation by virus
induced kinases, but is converted by host cell enzymes to cidofovir
diphosphate which is a competitive inhibitor of viral DNA
polymerases and to a lesser extent of host cell DNA polymerases.
6. VIDARABINE (ADENINE ARABINOSIDE)
It is an adenosine analogue which is phrosphorylated
intracellularly by host enzymes and rapidly metabolised to
hypoxanthine arabinoside by adenosine deaminase, resulting in
markedly reduced antiviral activity within the cells. This instability
and systemic toxicity have limited its use82. Dose: 10mg/kg/day
infused over 12 hours for 5 days.
7. IDOXURUDINE
This synthetic nucleoside is effective against DNA viruses,
particularly the herpes group. Its use is now restricted to topical
application because of severe bone marrow and hepatic toxicity
38
RECENT DRUGS: (1) Sorivudine:
It is an uracil analogue with activity against VZV infections. It
requires viral thymidine kinase for phosphorylation.
(2) Brivudine:
It is a new uracil derivative with potent and specific activity
against VZV. It is effective in a single or twice daily dose orally
(50 to 200 mg) in immunocompetent adults and older patients 83.
In immunocompromised patients, it is as effective as iv aciclovir in
the dose of 125mg tablet every 6 hours.
(3) Oral enzyme therapy:
Oral enzyme therapy is beneficial in diseases characterized in
part by TGF-β over production that included slingles patients84.
(4) Human Interferon-A
Interferons are synthesized by DNA recombinant technology.
Is nonspecific antiviral effects, involving synthesis of RNA and
additive protein, with immunomodulatory effects, help in preveting
39
ROLE OF STEROIDS IN HERPES ZOSTER MANAGEMENT:
Combination therapy of steroid and aciclovir resulted in an
improved quality of life, as measured by reductions in the use of
analgesics, the time to uninterrupted sleep, and the time to resumption
of usual activities85. However, neither study demonstrated any effect of
corticosteroids on the incidence or duration of post herpetic neuralgia.
Treatment of acute pain associated with herper zoster:
For acute pain scheduled short acting narcotic analgesics
should be prescribed. For persistent pain, long acting, controlled
-release opioids are preferred. If pain control remains inadequate
then regional or local anesthetic nerve blocks should be considered.
The effectiveness of carefully managed opiates, and tricyclic
antidepressants during the acute phase of herpes zoster in reducing
the incidence, duration of severity of PHN is not known.
Intradermal steroids, xylocaine and epinephrine can also be given.
TREATMENT OF POST HERPETIC NEURALGIA: TOPICAL THERAPY:
1. Topical lidocaine patch86
2. Topical EMLA cream
3. Topical Capsaicin (0.025%)cream
40 5. Doxepin cream (5%)88
SYSTEMIC TREATMENT
1) Anticonvulsants
For stabbing pain, sodium valproate, clonazepam,
carbamazepine and Gabapentin are effective.
2) Tricyclic antidepressants:
Desipramine. nortriptyline, maprotiline, Amitriptyline, are
effective in post herpetic neuralgia. They are thought to act
independent of their antidepressant actions.
(3) Oxycodone:
controlled release oxycodone (10mg every 12 hours) is an
effective analgesic for the management of steady pain, paroxysmal
spontaneous pain and allodynia.
(4) Analgesics:
Aspirin and other non steroidal anti inflammatory drugs
are commonly used in patients with post herpetic neuralgia, but
their value is limited. Tramodol87, a centrally acting analgesic
with opioid and non opioid activities also effective in post
41
(5) Anti psychotics
Fluphenazine, chlorprothixene, and perphenazines are used
with other drugs.
OTHER MODALITIES OF TREATMENT:
1. Intrathecal methyl Prednisolone
2. Intradermal steroids, xylocaine and epinephrine
injection.
3. Sympathetic blocks (stellate ganglion or epidural) with
0.25% bupivacaine prevents or relieves post herpetic
neuralgia. Epidural injection are made at or just above
the highest dermatome of the rash.
4. TENS (Transcutaneous electrical nerve stimulation)
may be helpful.
5. Acupuncture25
6. Spinalcord stimulators.
7. Bio feed back25
8. Jaipur block89
42
about 4 to 10 sites in one sitting. By this method, reported from India, 28% reported complete relief at 6 weeks, 57% after second injection and 11% after third injection89.
SURGICAL PROCEDURES
1. Division of dorsal root / tracotomy.
2. Rhizotomy (surgical separation of pain fibres)
3. Electrocoagulation of well defined area of dorsal root89.
4. Electrical stimulation of thalamus and spinal cord.
5. Anterolateral cordotomy89.
PREVENTION OF HERPES ZOSTER
(Zoster vaccine live (oka /merck)90
A subcutaneously administered live high titre (18,700 to
60,000 plaque -forming units per dose) varicella-zoster virus
vaccine (zoster vaccine) of the oka/ Merck strain has been
evaluated for the prevention of hesper zoster and the reduction of
43
AIMS OF THE STUDY
The study of herpes zoster was undertaken to findout:
1. Age incidence
2. Sex Incidence
3. Prevalence of prodromal symptoms
4. Predominant complaints given by patients.
5. Prevalence of constitutional symptoms.
6. Pattern of dermatomal involvement.
7. Prevalence of association with HIV.
8. Association with cutaneous disease, if any.
9. Association with systemic disease, if any.
10. Duration of time taken for resolution of lesions.
44
MATERIALS AND METHODS
The study was conducted between July 2005 and July 2007 at
the department of Dermatology, Madras Medical College, Chennai,
on hundred cases of herpes zoster. All cases of herpes zoster
attending skin out patient department and referred cases of zoster
from other departments were studied.
Patient’s age, sex, occupation, and address were noted. A
detailed history regarding the prodromal symptoms, skin lesions,
nature of pain, duration of illness at the time of presentation,
provocative factors were recorded. Associated cutaneous disease,
systemic disease and HIV infection were recorded. History of
chicken pox and previous attack of zoster were elicited and time
taken for complete resolution of lesions were noted. Complications
of herpes zoster and association with HIV were also recorded.
Each patient underwent detailed general physical and
systemic examinations. A thorough dermatological examination
was done in all cases and the following details were noted.
1. Site of lesion (segment involvement)
2. Morphology of lesions like grouped vesicles, scattered
45
3. Dermatomal distribution & the side of involvement.
4. Cutaneous dissemination.
5. Lymph node enlargement.
6. Mucosal lesions.
7. Motor zoster
8. Other cutaneous diseases.
The diagnosis of herpes zoster was made clinically on the
basis of characteristic presentation of vesicles in dermatomal or
disseminated pattern. Diagnosis was confirmed with Tzanck smear
and skin biopsy whenever required. A set of laboratory
investigation consisting of complete hemogram, blood sugar, renal
function test, urine analysis, ELISA for HIV antibody were done in
all cases. Whenever necessary, other specialist’s opinions like
ophthalmologist, physician, neurologist and diabetologist were
sought.
All patients were treated with oral aciclovir. Systemic
antibiotics were given for cases with secondary bacterial infection
and erosions. Patients with intractable zoster pain were given
carbamazepine or amitriptyline and analgesics. In addition to
46
calamine lotion, or topical antibiotic creams were given. These
patients were assessed with regards to the course of the disease,
resolution time, pain relief and complications.
All the patients were reviewed every 4 days, until the time of
complete healing. After that patients were followed once weekly or
more frequently depending upon the cases and complications
encountered till the resolution of problems.
During the follow up period the following complications were
noted.
1. Secondary bacterial infection.
2. Dissemination
3. Ulceration
4. Delayed healing
5. Post inflammatory hypo or hyperpigmentation.
6. Scarring
7. Post herpetic neuralgia.
47
OBSERVATIONS
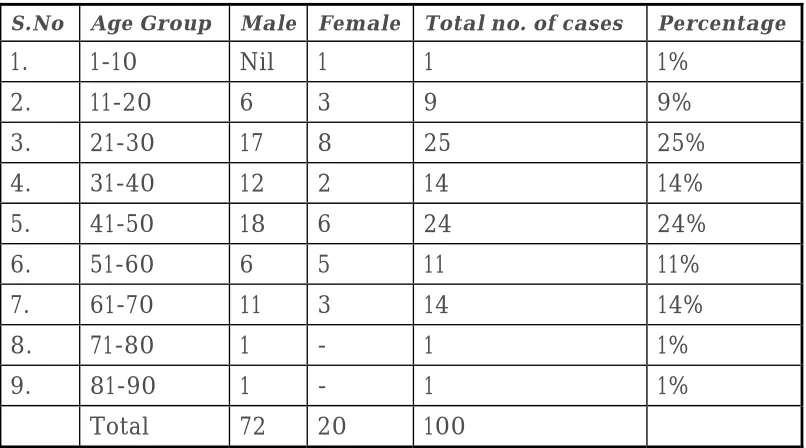
[image:54.612.119.522.196.420.2]AGE AND SEXWISE PREVALENCE OF ZOSTER
Table - I
S.No Age Group Male Female Total no. of cases Percentage
1. 1-10 Nil 1 1 1%
2. 11-20 6 3 9 9%
3. 21-30 17 8 25 25%
4. 31-40 12 2 14 14%
5. 41-50 18 6 24 24%
6. 51-60 6 5 11 11%
7. 61-70 11 3 14 14%
8. 71-80 1 - 1 1%
9. 81-90 1 - 1 1%
Total 72 20 100
Out of 100 cases 72 were males and 28 were females.
Age wise distribution (Table-1) shows that 73 cases were
below the age of 50 and 27 were above the age of 50 years.
Maximum number of cases were seen between the age group
of 21 to 30 years (25%) and 41 to 50 years (24%) which was
followed by 31 to 40 years (14%) and 61 to 70 years (14%).
Minimum number of cases were observed in the age group of 1 to 10
years (1%), 71 to 80 years (1%) and 81 to 90 years (1%).
48
Out of 100 cases, 72 were males and 28 were females and the
sex ratio is 2.5: 1 (male: female) approximately.
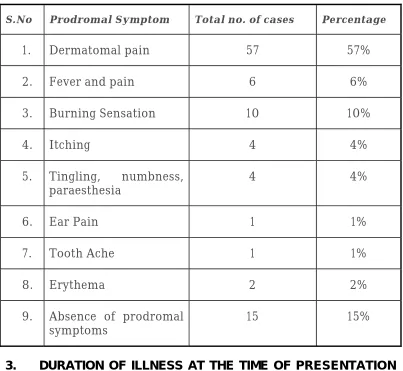
2. PREVALENCE OF PRODROMAL SYMPTOMS
The following prodromal symptoms were recorded.
1. Fever and pain
2. Dermatomal pain
3. Burning sensation
4. Itching
5. Tingling, numbness, paraesthesia
6. Ear pain
7. Tooth ache
8. Erythema
Prodromal symptoms were present in 85 cases and absent in
15 cases. Dermatomal pain prior to the onset of lesions was the
commonest prodromal symptom (57%). The next common
prodromal symptom seen was burning sensation (10%). Fever and
pain was present in 6% of cases. Itching was present in 4% of cases.
Ear pain and tooth ache were present in one case of herpes zoster
49
Table -2 : Prevalence of prodromal symptoms
S.No Prodromal Symptom Total no. of cases Percentage
1. Dermatomal pain 57 57%
2. Fever and pain 6 6%
3. Burning Sensation 10 10%
4. Itching 4 4%
5. Tingling, numbness,
paraesthesia 4 4%
6. Ear Pain 1 1%
7. Tooth Ache 1 1%
8. Erythema 2 2%
9. Absence of prodromal
symptoms 15 15%
3. DURATION OF ILLNESS AT THE TIME OF PRESENTATION TO THE HOSPITAL:
Out of 100 cases, 74% of cases presented with vesicular
lesions within 5 days of onset of lesions. The remaining 26% of
cases were presented after 6 days and above to the hospital. The
complications like secondary infection and PHN were maximum in
those cases came for treatment late in the course of the disease.
Table - 3: Duration of illness at the time of presentation
50
1. 2 days 18 18%
2. 3 days 20 20%
3. 4 days 26 26%
4. 5 days 10 10%
5. 6 days 4 4%
6. 7 days 12 12%
7. 8 days & above 10 10%
100
4. PREVALENCE OF PRESENTING COMPLAINTS AND CONSTITUTIONAL SYMPTOMS
Most common presenting complaint was pain in 99% of cases.
In 57% of cases pain was present prior to the onset of lesions and
the remaining 42% of cases developed pain during evolution of
vesicles.
Vesicular lesion was the next common presenting complaint
in 98% of cases and it was present in association with pain in
almost all cases.
Other presenting complaints were erosions, crusting, itching
and burning sensation in very few cases (1 to 2 %). Headache and
watering in the eye were present in 6 % of cases of ophthalmic
51
Fever was the most common constitutional symptoms present
in 45% of cases other constitutional symptoms present with fever
were myalgia (18%), headache (12%) and joint pain (2%).
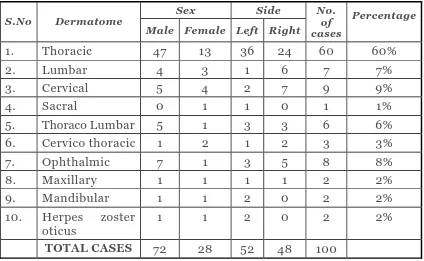
5. MORPHOLOGY OF LESION AND PATTERN DERMATOME INVOLVEMENT:
Grouped vesicles with erythematous background in
dermatomal distribution were present in 97% of cases. The
remaining 3% of cases had crusting and erosion alone. Other
lesions presented with grouped vesicles were pustules, erosions and
crusting. Oral erosions were seen in 2% of cases of maxillary and
mandibular nerve zoster.
Redness of eyes and eyelid edema were present in 6% of cases
of ophthalmic zoster.
Thoracic dermatome was the most common dermatome
involved (60%) followed by cervical in 9% of cases, ophthalmic
zoster in 8% of cases and lumber segment in 7% of cases.
The prevalence of maxillary, mandibular and herpes zoster
oticus was 2% each.
Thoracolumbar and cervicothroracic involvement was 6% and
3% respectively. The least common dermatome involved was sacral
52
The pattern of dermatome involvement was almost similar in
both sexes.
Dermatome involvement was predominantly on the left side
(52%) when compared to right side (48%). But in lumbar, cervical
[image:59.612.119.543.263.524.2]and opthalmic zoster right side was commonly involved.
Table-4 : Pattern of dermatome involvement:
Sex Side S.No Dermatome
Male Female Left Right No.
of cases
Percentage
1. Thoracic 47 13 36 24 60 60%
2. Lumbar 4 3 1 6 7 7%
3. Cervical 5 4 2 7 9 9%
4. Sacral 0 1 1 0 1 1%
5. Thoraco Lumbar 5 1 3 3 6 6% 6. Cervico thoracic 1 2 1 2 3 3% 7. Ophthalmic 7 1 3 5 8 8%
8. Maxillary 1 1 1 1 2 2%
9. Mandibular 1 1 2 0 2 2%
10. Herpes zoster
oticus 1 1 2 0 2 2%
TOTAL CASES 72 28 52 48 100
6. MULTIDERMATOMAL INVOLVEMENT AND DISSEMINATION
Multidermatomal involvement was noted in a case of herpes
zoster oticus. The affected patient was an elderly man (70 years)
with carcinoma prostate. He had involvement of C2, C3 and C4
segment in addition to herpes zoster oticus with facial palsy on the
53
Cutaneous dissemination was noted in 2 cases in addition to
the classical dermatomal distribution of grouped vesicles. One
patient was a 36 year old male with HIV infection and another
patient was a 65 year old male with no underlying
immunosuppression or malignancy.
No recurrence of herpes zoster was observed in any case.
7. LYMPH NODE ENLARGEMENT:
Regional lymph node enlargement was noted in 95% of cases.
Nodes were tender in 80% of cases and non tender in 15% of cases
and are firm in consistency. Generalised lymphadenopathy (PGL)
was present in twelve HIV positive cases.
8. PROVOCATIVE FACTORS:
Out of 100 cases, 36 cases were having one or more suspected
provocative factors. Among the 36 cases, 16 cases (44.4%) were
having HIV, 7 cases (19.4%) were having diabetes and 5 cases
(13.8%) were on steroid therapy for SLE (3 cases) and bronchial
[image:60.612.118.523.650.710.2]asthma (2 cases).
Table - 5
PREVALENCE of provocative factors
S.No. Provocatve Factors Male Female Total %
1. HIV 14 2 16 44%
54
3. Diabetes 6 1 7 19.4%
4. Renal transplantation 1 0 1 2.7% 5. Steroid therapy 2 3 5 13.8% 6. Hansen’s disease 1 0 1 2.7% 7. Pulmonary Tuberculosis 1 0 1 2.7%
8. Pregnancy 0 1 1 2.7%
9. Radiotherapy 0 2 2 5.5% 10. Malignancy
(Prostate cancer) 1 0 1 2.7%
TOTAL 26 10 36
Hansen’s disease and tuberculosis were also present in 2
cases of herpes zoster. Physical stress of parturition was suspected
as a provocative factor of zoster in a case of postpartum female.
Immunosuppression of pregnancy was the probable cause for zoster
in an antenatal case (2.7%).
A renal transplant patient (2.7%) on azathioprine therapy
developed herpes zoster. Two female patients on radiotherapy for
carcinoma breast and carcinoma cervix had herpes zoster (5.5%).
One male patient (2.7%) with carcinoma prostate developed
multidermatomal herpes zoster with herpes zoster oticus.
55
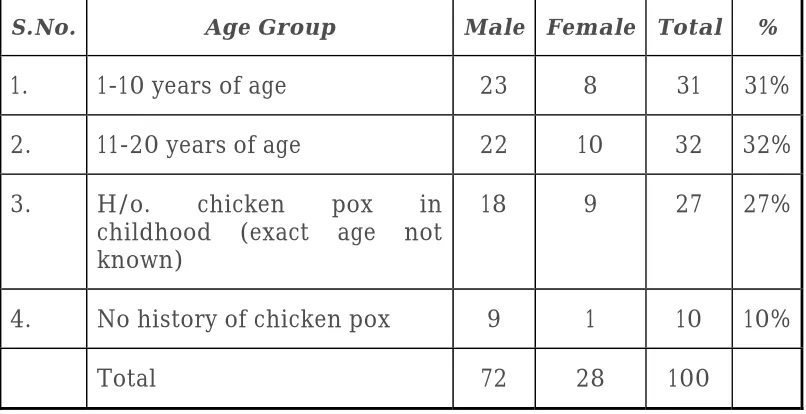
[image:62.612.119.522.137.344.2]9. PAST HISTORY OF CHICKEN POX:
Table-6 : Age group - wise past history of Chicken Pox
S.No. Age Group Male Female Total %
1. 1-10 years of age 23 8 31 31%
2. 11-20 years of age 22 10 32 32%
3. H/o. chicken pox in childhood (exact age not known)
18 9 27 27%
4. No history of chicken pox 9 1 10 10%
Total 72 28 100
Out of 100 cases, 90% gave definite history of occurrence of
chicken pox out of 90 cases. 27% of patient did not give the exact
age of occurrence of chicken pox. 32% of cases gave history of
chicken pox between 11 to 20 years of age and 31% of cases gave
history of vericella between 1 to 10 years. The remaining 10% of
cases were either not aware of or not had chicken pox at all.
10. ASSOCIATED CUTANEOUS AND SYSTEMIC DISEASES:
Cutaneous diseases seen in association with herpes zoster
were acne 1 case, seborrhoeic dermatitis two cases, tinea versicolor
2 cases, SLE 3 cases, Hansen‘s disease 1 case, insect bite allergy 2
cases, wart 1 case, cellulitis 1 case, oral candidiasis 1 case, tinea
cruris 1 case and intertrigo 1 case. Most of these cases were seen in
56
Diabetes (7 cases) was the most common systemic disease
seen in association with herpes zoster. The next common systemic
disease seen with zoster was hpertension (6 cases). Other systemic
diseases seen with herpes zoster were SLE (3 cases), bronchial
asthma (2 cases), tuberculosis (1 case), Hepatitis B (1 case) and
chronic renal failure (1 case).
11. TIME TAKEN FOR RESOLUTION OF LESIONS:
Most cases (50%) showed complete resolution of lesions
between 15 to 21 days (3rd week). All patients were given T. aciclovir
800mg 5 times a day for 8 days except for immunocompromised
patients and they were given aciclovir for 10 days. The response to
aciclovir was good and resolution was rapid unless there was
[image:63.612.119.524.490.641.2]secondary bacterial infection or underlying immunosuppression.
Table - 7 : Resolution time of zoster lesions
S.No. Duration No. of cases %
1. 8 to 14 days 35 35%
2. 15 to 21 days 50 50%
3. 22 to 28 days 14 14%
4. 29 days and above 1 1%
Resolution of lesions occurred within 8 to 14 days (2 weeks)
57
in 14% of cases. One case with underlying immunosuppression and
necrotic lesion resolved at 29 days.
12. INVESTIGATIONS:
Complete hemogram was within normal limits except for
increasecd eosinophil count in 6 patients, increased ESR in 20
patients, increased neutrophil count in 6 patients, decreased
haemoglobin value in 4 patients.
Blood sugar was elevated above the normal valve in 7
patients. Urine routine examination was normal in almost all
patients (98%). Urine examination showed reducing sugar in 2
patients with elevated blood glucose value.
ELISA test for HIV antibody was done in all patients. Positive
ELISA test result was obtained in 6 cases. 10 patients were already
diagnosed as HIV Positive and presented with zoster during the course
of HIV disease
ECG was taken for patients with zoster involving left thoracic
segment and it was found to be normal.
One patient with SLE had elevated blood urea and serum
creatinine values and nephrologist opinion obtained for her and
58
Diabetologist opinion for 3 patients, neurologist opinion for
13 patients, ophthalmologist opinion for 8 patients and ENT
surgeon opinion for one case of herpes zoster oticus were obtained.
Tzanck smear was positive in 95% of cases and negative in 5% of
cases who presented late and those with ulcerations, erosions and
crusting.
Skin biopsy was done in 2 patients with erythematous
plaques studded with very few grouped papules in a dermatomal
pattern, in the pre eruptive stage, which under light microscope in
haematoxylin and eosin staining showed intraepidermal
uniloculated to multiloculated bullae with ballooned epithelial cells
and multinucleated giant cells. Reticular degeneration seen in some
areas. The upper dermis showed inflammatory infiltration.
13. COMPLICATIONS:
a. Secondary bacterial infection:
Secondary bacterial infection was reported in 15 cases
(37.5%). In 2% of patients with secondary infection scarring
occurred in affected dermatome. Cases were treated with topical silver
sulphadiazine cream and systemic antibiotics in addition to aciclovir.
59
Scarring was noted in 5 cases (12.5%) out of 5 cases, 3 cases
had erosions and ulcerations of the lesion and 2 cases were
associated with secondary bacterial infection and later developed
ulceration.
c. Motor Zoster:
Facial palsy was seen in a patient (2.5%) with Ramsay Hunt
60
Table - 8
PREVALENCE OF COMPLICATIONS
Complication M F T Percentage
Scarring 5 0 5 12.5%
Secondary bacterial infection 12 3 15 37.5%
Post herpetic neuralgia 14 5 19 47.5%
Motor Zoster 1 0 1 2.5%
TOTAL 32 8 40
d) Post herpetic neuralgia:
PHN is the most feared complication in immunocompetent
patients. Both the incidence and duration of post herpetic neuralgia
are directly correlated with the patient’s age. Out of 40 patients
with complications of zoster, 19 cases (47.5%) developed post
herpetic neuralgia.
Among the 19 cases of post herpetic neuralgia, 14 were male