CLINICAL STUDY OF CUTANEOUS MANIFESTATIONS IN HIV POSITIVE PATIENTS IN CORRELATION WITH CD4 COUNT
Dissertation submitted to
THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI- 600032
APRIL 2017
In partial fulfilment of the requirements for the award of M.D. DEGREE IN
DERMATOLOGY, VENEREOLOGY AND LEPROLOGY (BRANCHXII)
COIMBATORE MEDICAL COLLEGE HOSPITAL, COIMBATORE. DEPARTMENT OF DERMATOLOGY, VENEREOLOGY
DECLARATION
I Dr. Meghana. M. J, solemnly declare that the dissertation
entitled “Clinical Study Of Cutaneous Manifestations In HIV Positive Patients in correlation with CD4 count” is a bonafide work done by me at Coimbatore Medical College Hospital during the year August 2015
to July 2016 under the guidance & supervision of Dr.P.P.Ramasamy
M.D.,D.D., Professor & Head of Department, Department of
Dermatology, Coimbatore Medical College & Hospital.
The dissertation is submitted to Dr.MGR Medical University
towards partial fulfilment of requirement for the award of MD degree
branch XII Dermatology, Venereology and Leprology.
PLACE: Dr. MEGHANA . M .J
CERTIFICATE
This is to certify that the dissertation entitled “CLINICAL STUDY OF CUTANEOUS MANIFESTATIONS IN HIV POSITIVE PATIENTS IN CORRELATION WITH CD4 COUNT” is a record of bonafide original work done by Dr. MEGHANA. M. J, Post graduate student in the Department of Dermatology, Venereology and Leprology, Coimbatore Medical College Hospital, Coimbatore under the guidance of
Dr.P.P.Ramasamy M.D.,D.D., Professor and HOD of Department, Department of Dermatology, Coimbatore Medical College Hospital, Coimbatore in partial fulfillment of the regulations for the Tamilnadu DR.M.G.R Medical University, Chennai towards the award of MD., degree (Branch XII.) in Dermatology, Venereology And Leprology.
Date: GUIDE
Dr. P.P.Ramasamy M.D., D.D.,
Professor& HOD, Department of Dermatology, Coimbatore Medical College & Hospital.
Date: HOD
Dr. P.P.Ramasamy M.D., D.D.,
Professor& HOD, Department of Dermatology, Coimbatore Medical College & Hospital.
Date: Dr. A. Edwin Joe M.D., B.L.,
COPYRIGHT
Declaration by the Candidate
I hereby declare that The Tamilnadu DR.M.G.R Medical University,
Chennai shall have the rights to preserve, use and disseminate this
dissertation / thesis in print or electronic format for academic / research
purpose.
PLACE: COIMBATORE Dr. MEGHANA. M. J.
ACKNOWLEDGEMENT
I solicit my humble thanks to the Dean Dr. A.Edwin Joe M.D.,B.L.,
Coimbatore Medical College Hospital, for allowing me to conduct the study
in this hospital.
I am also immensely thankful to my guide Dr. P.P.RAMASAMY
M.D., D.D., Professor & Head of the Department, Dermatology and
Leprology for his invaluable guidance, motivation and help throughout the
study. I would like to express my gratitude and indebtness to Dr.
P.MOHAN, M.D., D.V., Professor & Head of department, Department of
Venereology for his support.
I express my earnest gratitude to all the Assistant
Professors, Department of Dermatology Dr.R.Madhavan M.D.,
Dr.B.Eswaramoorthy M.D., Dr. S.Bharathi M.D., Dr. S Swarnalakshmi
M.D., Dr.Pradeepa M.D., and Dr.R.Revathy M.D., without their help and
guidance this work would not have been possible.
I owe great debt of gratitude to Dr.Ranjani Raju M.D., for her kind
support and encouragement.
I sincerely thank Dr. K. Mahadevan M.D., for being a great
I owe a lot to my parents, my husband Dr. Vivek N Savsani and other
family members who have always stood by me in my career and making me
what I am today.
My sincere thanks to all my post graduate colleagues Dr. R.Vithya,
Dr.A Amutha, Dr. M.S Krishna Meera, Dr. Divya and Dr. Dinesh who have
been of immense help throughout the study period.
I am very grateful to all patients for their co-operation and
TABLE OF CONTENTS
S. NO CONTENTS PAGE
1 INTRODUCTION 1
2 AIMS AND OBJECTIVES 3
3 REVIEW OF LITERATURE 4
4 MATERIALS &METHODS 47
5 OBSERVATION AND RESULTS 53
6 DISCUSSION 86
7 SUMMARY 96
8 CONCLUSION 99
9
ANNEXURES
BIBILOGRAPHY
PROFORMA
KEY TO MASTER CHART
MASTER CHART
LIST OF TABLES
SL. NO.
TABLE
PAGE NO.
1 Demographic characteristics of 100 HIV
infected patients
53
2 Marital status and HIV status of partners
54
3 Age – sex distribution of 100 HIV-infected
patients
56
4 Treatment status of 100 HIV-infected
patients
58
5 Classification of patients according to
WHO clinical staging of HIV
59
6 Classification of patients according to
WHO immunological staging of HIV
60
7 Number of mucocutaneous manifestation
per patient
61
8 Frequency of various mucocutaneous
manifestations in HIV individuals
62
9 Distribution of candidiasis
63
10 Morphological patterns of dermatophytosis
64
11 Distribution of HSV infection
65
12 Various presentation of HPV infection
66
13 CD4 cell count and Infectious dermatoses
72
14 CD4 cell count and Non-infectious
dermatoses
73
15 Prevalence of Infectious manifestations according to WHO Clinical stage of HIV infection
16 Prevalence of Non-infectious manifestations according to WHO Clinical stage of HIV infection
75
17 Prevalence of Infectious manifestations according to WHO immunological stage of HIV infection
76
18 Prevalence of Non- infectious manifestations according to WHO immunological stage of HIV infection
77
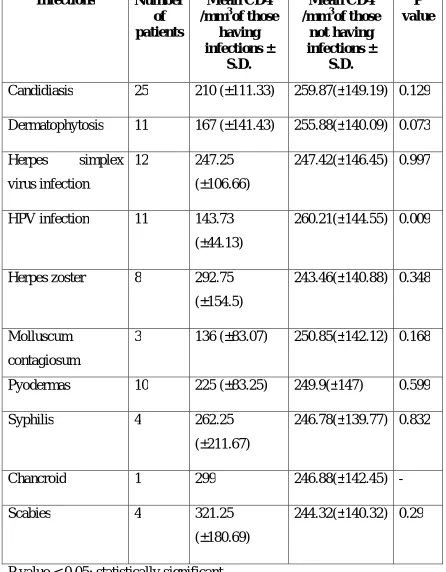
19 Mucocutaneous conditions (infectious dermatoses) stratified by CD4 cell count among HIV-infected patients
79
20 Mucocutaneous conditions (non-infectious dermatoses) stratified by CD4 cell count among HIV-infected patients
80
21 Mucocutaneous manifestations (infectious dermatoses) stratified by ART use among HIV-infected patients
82
22 Mucocutaneous manifestations
(non-infectious dermatoses) stratified by ART use among HIV-infected patients
83
LIST OF CHARTS
SL. NO.
CHARTS
PAGE NO.
1
HIV status of sexual partners
54
2
Gender distribution of cases
55
3
Age – sex distribution of 100 HIV infected patients56
4
Mode of transmission of HIV
57
5
Treatment status of HIV-infected patients
58
6
Classification of patients according to WHO clinical staging of HIV59
7
Classification of patients according to
WHO immunological staging of HIV
60
8
Number of mucocutaneous manifestations
in 100 patients
COLOUR PLATES
SL. NO.
FIGURES
1. Fig. 1 Oral candidiasis – Pseudomembranous type
2. Fig. 2 Angular cheilitis
3. Fig. 3 Candida – KOH mount
4. Fig. 4 Vulvovaginal candidiasis with Buschke-Lowenstein
tumor
5. Fig. 5 Candidal balanoposthitis
6. Fig. 6a and 6b Extensive Dermatophytosis
Fig. 6c Dermatophytosis - KOH mount
7. Fig. 7 Atypical Herpes genitalis
8. Fig. 8 Herpes labialis
9. Fig. 9 Herpes genitalis in a male
10. Fig. 10 Herpes genitalis in a female
11. Fig. 11 Herpes simplex – Tzanck smear
12. Fig. 12 Herpes zoster ophthalmicus
13. Fig. 13 Herpes zoster
14. Fig. 14 Extensive genital wart
15. Fig. 15 Multiple cutaneous warts
16. Fig. 16 Genital Molluscum contagiosum
18. Fig. 18 Multiple furuncles over legs
19. Fig. 19 Furuncle over back
20. Fig. 20 Furuncle over labia majora
21. Fig. 21Carbuncle
22. Fig. 22 Secondary syphilis – Lichenoid lesions over palms
23. Fig. 23 Secondary syphilis – Papulosquamous skin lesions
24. Fig. 24 Chancroid
25. Fig. 25 Genital scabies
26. Fig. 26 Seborrhoeic Dermatitis
27. Fig. 27 Pruritic papular eruptions
28. Fig. 28 Fixed drug eruption
29. Fig. 29 Diffuse hyperpigmentation over hands
30. Fig. 30 Psoriasis
31. Fig. 31 Longitudinal melanonychia
32. Fig. 32 Acneiform eruption
LIST OF ABBREVIATIONS
HIV – Human Immunodeficiency Virus
AIDS – Acquired Immuno Deficiency Syndrome
CD4 – Cluster of Differentiation
RNA – Ribonucleic Acid
DNA – Deoxyribonucleic Acid
SIV – Simian Immunodeficiency Virus
NK cells – Natural Killer cells
gp120 – glycoprotein 120
gp41 – glycoprotein 41
CCR5 – CC Chemokine Receptor 5
CXCR4 – C-X-C chemokine Receptor type 4
ssRNA – single stranded Ribonucleic Acid
dsDNA – double stranded Deoxyribonucleic Acid
mRNA – messenger Ribonucleic Acid
ART – Anti-Retroviral Therapy
PCP – Pneumocystis carinii pneumonia
MAC – Mycobacterium Avium – Intracellulare
EDTA – Ethylenediaminetetraacetic Acid
CD4 mAb PE - Cluster of Differentiation monoclonal antibody
PhycoErythrin
HAART – Highly Active Anti-Retrovial Therapy
MRSA - Methicillin Resistant Staphylococcus aureus
TB – Tuberculosis
IRIS – Immune Reconstitution Inflammatory Syndrome
HSV – Herpes Simplex Virus
VZV – Varicella Zoster Virus
HZ – Herpes Zoster
HPV – Human Papilloma Virus
EDV – Epidermodysplasia verruciformis
MC – Molluscum contagiosum
CMV – Cytomegalovirus
EBV – Epstein-Barr Virus
OHL – Oral Hairy Leukoplakia
VVC – Vulvovaginal Candidiasis
GUD – Genital Ulcer Disease
CDC – Centers for Disease Control
EF – Eosinophilic folliculitis
ADR – Adverse cutaneous Drug Reaction
HLAB – Human Leucocyte Antigen
NHL – Non-Hodgkin’s Lymphoma
SCC – Squamous Cell Carcinoma
IL 1 - Interleukin 1
IL 4 - Interleukin 4
IL 5 - Interleukin 5
IL 6 - Interleukin 6
RANTES – Regulated on Activation, Normal T Cell Expressed and
Secreted
TNF - Tumour Necrosis Factor
MSH - Melanocyte Stimulating Hormone
IgA – Immunoglobulin A
IgM – Immunoglobulin M
IgG – Immunoglobulin G
SD – Standard Deviation
ABSTRACT
Title
Clinical Study Of Cutaneous Manifestations in HIV Positive Patients
in Correlation with CD4 Count.
Background and objectives
In HIV, mucocutaneous disorders are one of the common
presenting features. Common diseases may present atypically or rare
dermatoses may occur newly in the presence of HIV. Often, the
mucocutaneous manifestations correlates with the CD4 count and may
be used to assess the prognosis. Mucocutaneous manifestations in HIV
may vary from region to region, even within the same country. Since
many studies have not been conducted in our study area, it was
decided to take up this study.
Methodology
This was a descriptive study conducted from August 2015 to
July 2016 at the Outpatient Department of Dermatology &
Venereology, Coimbatore Medical College Hospital. Hundred
HIV-positive patients with age > 18 years and having one or more
CD4 count was recorded in all the patients. Other necessary
investigations like biopsy, KOH mount and Tzanck smear were done
in relevant cases. Patients were classified according to WHO clinical
stages and immunological classification.
Results
There were 100 patients with 143 dermatoses seen in the study. Male
: female ratio was 2.6: 1. Most cases belonged to the age group of
31- 40 years. Nearly 49% of all cases were in WHO clinical stage 2.
About 44% patients were in severe immunosuppression i.e CD4 count
< 200 cells/ mm3. Candidiasis was the most common dermatosis seen
in the study followed by herpes simplex virus infection, seborrheic
dermatitis and dermatophytosis.
Conclusion
HIV infection produces a wide array of mucocutaneous manifestations.
This offers diagnostic clues pointing towards the early diagnosis of
the disease. CD4 count is an useful tool governing the occurrence of
certain dermatoses as well as treatment response.
Key words
INTRODUCTION
Human Immunodeficiency Virus is emerging as an epidemic of
gigantic proportion affecting not only the developed nations but also
the developing nations like India. Various systemic and cutaneous
manifestations can occur in HIV, of which mucocutaneous
manifestations has its own significance.
Around 36.7 million people worldwide are infected with Human
Immunodeficiency Virus (HIV).1 There are 2.1 million people living
with HIV in India making our country the third largest nation with
HIV population. India has HIV prevalence of 0.26% among adults
with 85,000 new HIV infections occurring annually. There are
1,43,000 people living with HIV in Tamil nadu.2
It has become evident over the past decade that cutaneous
disorders can occur in all stages of HIV-infection.3 In addition to
generalised immunosuppression seen in HIV / AIDS, localised
mucocutaneous immune dysregulation is noticed and is responsible for
the development of skin and mucosal infections.4
Few selected dermatoses serve as sensitive and useful clinical
dermatoses like herpes simplex virus infection are more severe,
chronic in nature and present with atypical manifestations.
CD4 count is helpful in monitoring HIV disease progression
in patients on anti-retroviral treatment. It predicts the degree of
immunosuppression and occurrence of specific dermatoses at specific
CD4 counts.
Our present study will attempt to find out the various
patterns and presentations of mucocutaneous conditions occurring in
AIMS AND OBJECTIVES
AIM
To study the various clinical patterns of mucocutaneous manifestations occurring in HIV positive patients and to
correlate with CD4 count.
OBJECTIVES
REVIEW OF LITERATURE
Origin of HIV
Human Immunodeficiency Virus belongs to Lentivirus group of
Retroviridae family. Retrovirus is a virus that attaches itself to the
host cell and transcribes viral RNA into cellular DNA. It was first
identified in the year 19815 by Robert Gallo and his colleagues.
HIV-1 virus is thought to have originated from Simian
Immunodeficiency Virus(SIV) of chimpanzees found in Central Africa.
HIV-2 is closely related to SIV of sooty Mangabey monkey found in
Western Africa.6
Types of HIV
Human Immunodeficiency Virus has been divided into two
types. HIV-1 and HIV-2. HIV-1 is the major cause of HIV disease
all over the world. It is further divided into 11 subtypes and subtype
‘C’ is prevalent in India. HIV-2 is prevalent in certain geographical
areas like West Africa. HIV-2 differs from HIV-1 in certain aspects
like lesser transmissibility, better prognosis and longer incubation
Pathogenesis of HIV infection
HIV is predominantly lymphotropic to CD4 (T-helper)
lymphocytes. Other cells bearing CD4 receptors are also infected (e.g,
macrophages, B cells, Langerhans cells, NK cells etc.,). HIV gains
entry into the cells by means of binding of gp120 to the CD4
receptor on host cell. This is followed by conformational changes in
gp120 which facilitates the binding of virion to CCR5 and CXCR4
molecules. This exposes gp41 which helps in entry of the viral RNA
and enzymes into the host cell.
The Reverse transcriptase enzyme is a RNA dependent
DNA polymerase which transcribes viral ssRNA into dsDNA and is
transported into host cell nucleus. The Integrase enzyme integrates the
viral DNA with the host cell nuclear DNA and forms provirus
(integrated virus).
Transcription of proviral DNA into genomic RNA or
mRNA occurs following host cell activation. HIV mRNA is translated
into protein which undergoes certain modifications to form viral
proteins. The viral proteins, enzymes and genomic RNA forms the
infectious viral particle and buds out of the host cell and further
CD4 cell count and HIV
It is the measurement of the number of CD4 T lymphocytes
present in the peripheral blood. CD4 stands for cluster of
differentiation 4.
CD4 is a glycoprotein which is expressed on a number of
immunologically important cells like T helper lymphocytes,
macrophages, monocytes and dendritic cells.
The characteristic feature of HIV infection is the progressive
destruction of CD4 cells. With severe immunosuppression,
opportunistic infections start manifesting in HIV-infected patients
causing significant morbidity and mortality. CD4 count is inversely
proportional to the degree of immunosuppression.
It serves as a guide to commence ART i.e when the CD4
count drops below 350 cells/µl ART is started. It is used to monitor
ART and also used as a guide for the commencement of prophylaxis
of some opportunistic infections like Pneumocystis pneumonia (CD4 <
200/ µl) and MAC (CD4 < 50 cells/ µl). It governs the progression of
HIV infection to clinical stage 3 infection – AIDS (CD4 < 200 cells/
µl).
The normal CD4 count ranges from 500 cells/ µl to 1600 cells/
i.e in the presence of infections, acute illness, vaccination, stress and
early in the morning, the count will be slightly lower. The count is
higher in the evenings and immediately after exercise. Therefore,
instead of a single CD4 count measurement and analysis, the analysis
of the trend of rise or fall in CD4 count is important.
CD4 count is measured by flow cytometry. Whole blood is
collected in an sterile EDTA tube by venepuncture under sterile and
universal precautions. 20 µl of blood is added into a Partec test tube.
To this, 20 µl of CD4 mAb PE is added. CD4 mAb PE is a
Phycoerythrin- conjugated monoclonal antibody to human CD4.
Contents of the tube is gently mixed and incubated at room
temperature away from sunlight for 15 minutes. 800 µl of buffer is
added and mixed. The tube is placed in the given slot and the
CD4-PE fluorescence is analysed in a flow cytometer with an excitation
light source of 488 nm or blue / green solid state laser source of 532
nm. Dilution factor is pre-set by the instrument. Counting results will
be displayed automatically as CD4 cells per µl of whole blood.
Mucocutaneous manifestations of HIV and AIDS
The dermatological manifestations are mostly the
course of HIV infection in all stages. WHO has divided the clinical
stages of HIV into Stage 1, Stage 2, Stage 3 and Stage 4.
In early stages, herpes zoster, seborrhoeic dermatitis, pruritic
papular eruptions, onychomycosis can occur. In late stages, oral hairy
leukoplakia, chronic herpes simplex virus infection, Kaposi’s sarcoma,
molluscum contagiosum etc. can occur which signifies advanced
immunosuppression.
Decreased mucocutaneous immunity is often responsible for the
earliest clinical signs seen in HIV infected individuals. HIV produces
many atypical manifestations of known dermatological diseases and as
the disease progresses, these skin manifestations may become more
severe and diverse. In AIDS, opportunistic pathogens may present as
atypical cutaneous lesions.6
It is said that some cutaneous lesions reflect the progression of
HIV disease,7 but this relationship is still controversial. Infective
conditions such as oral candidiasis, herpes zoster and dermatophytoses
occur late in the disease compared to non-infective dermatoses.8
Atypical manifestations of cutaneous disorders may include: lesions
occuring at unusual anatomical locations, increased severity, treatment
Classification of Mucocutaneous manifestations of HIV disease
The mucocutaneous manifestations in HIV disease can be broadly
classified as10
1) Infectious manifestations
(a) Bacterial
(b) Viral
(c) Fungal
(d) Parasitic
2) Non - infectious dermatoses
(a) Papulosquamous disorders
(b) Pruritic eruptions of HIV
(c) Pigmentary disorders
(d) Neoplasms
(e) Miscellaneous
3) Cutaneous adverse drug reactions
4) Hair manifestations
6) Specific mucosal manifestations
1) Infectious dermatoses:
a) Bacterial infections
i) Staphylococcal infection
Staphylococcus aureus is the most common organism implicated
in cutaneous and systemic bacterial infections occurring in
HIV-positive patients.11The high frequency of Staphylococcus aureus skin
infection is attributable to high rates of chronic nasal carriage in HIV
patients.12, 13
Primary skin and soft tissue infections caused by Staph.aureus
are – folliculitis, furuncles, impetigo, bullous impetigo, ecthyma,
carbuncles, cellulitis, botryomycosis and pyomyositis. Secondary
staphylococcal infection commonly occurs in atopic dermatitis, scabies
and intertrigo. Subcutaneous abscesses due to staphylococci may
develop at intravenous-line or injection site. Hematogenous
dissemination occurs most commonly with intravenous catheter use.
Folliculitis is commonly seen in HIV patients not on HAART and
with CD4 <200 cells/µl.
The incidence of Methicillin-resistant Staphylococcal aureus in
HIV is 6 fold higher than non-HIV indiciduals. MRSA poses a
challenge to HIV patients. Risk factors for MRSA include: high-risk
HIV viral load copies/mL, absence of co-trimoxazole prophylaxis,
partners with skin infections, recent hospitalisation, prior MRSA
infection and recent β-lactam antibiotic use.14-18
ii) Streptococcal infection
Group A streptococcus is collectively referred to as
Streptococcus pyogenes. It causes primary skin and soft tissue
infections like impetigo, ecthyma, erysipelas, cellulitis, perianal
infection, ulcers and necrotizing fasciitis. Secondary infection occurs in
eczema, scabies and ulcers.
In HIV-positive patients, erysipelas and lymphadenitis commonly
occurs due to streptococci.19
iii) Pseudomonas infection
Pseudomonas aeruginosa causes periumbilical, periungual
infection, tropical immersion foot, gram negative folliculitis and hot
tub folliculitis. Secondary infection of burns ulcers can occur.
Septicemia, malignant otitis externa occurs in immunocompromised
individuals.
Ectyhma gangrenosum and panniculitis occurs in advanced HIV
iv) Bacillary angiomatosis
It is caused by the gram negative bacteria, Bartonella henselae
and Bartonella quintana. It is most commonly seen in late stage of
HIV disease (CD4 <100 cells/µl).24
The cutaneous manifestations are solitary or multiple red
coloured hemangioma like papules, nodules, hyperpigmented
hyperkeratotic plaques or large friable exophytic masses resembling
pyogenic granuloma. The lesions may develop ulceration with
discharge and crusting. Skin lesions must be regarded as a marker of
possible internal organ involvement.
Visceral involvement in the form of peliosis hepatitis presenting
as abdominal pain, jaundice and colonic angiomatosis causing
tenesmus and bloody diarrhoea may be seen.
v) Cutaneous Mycobacterium tuberculosis infection
Mycobacterium tuberculosis is a common agent of infection in
HIV but cutaneous lesions are rare. The cutaneous lesions include
scrofuloderma, scattered violaceous papules, nodules, acute miliary
tuberculosis of skin, keratotic papules and nodules, palmoplantar
In the perianal area, it can present as non-healing ulcers and
verrucous lesions. Tuberculosis cutis miliaris acuta generalisata is an
uncommon form of cutaneous tuberculosis reported in HIV patients.
Atypical mycobacterial infection
It is caused by Mycobacterium avium – intracellulare when CD4
count falls below 50 cells/µl. Skin lesions occur as violaceous papules,
nodules and ulcers over extremities, trunk, head and genitalia.26 In
HIV, sporotrichoid lesions can appear.
vi) Leprosy
The clinical features of leprosy is not significantly modified by
HIV except in IRIS.27-29 Type 1 reaction may develop in leprosy as a
part of IRIS after initiation of ART.
According to many studies, leprosy is not a risk factor for
developing HIV infection. Few studies suggests that there is higher
risk of erythema nodosum leprosum and recurrent reversal reactions.
But as such no effect on neuritis or reversal reactions overall.30
vii) Syphilis
It is a sexually transmitted disease caused by Treponema
pallidum, a gram negative spirochaete. The natural history of syphilis
could be altered in the presence of HIV. Syphilis and HIV both can
Because of immunological alterations induced by HIV, there is
rapid dissemination of treponemes from the primary lesion and the
early appearance of secondary lesions.31 In advanced HIV, syphilis may
have more atypical findings. Also, there is increased chances of
biological false positive reactions in syphilis serology.32
Primary syphilis – In HIV infected individuals, primary chancre
may be painful or may present as multiple chancres which are larger,
deeper and heal more slowly. Gangrenous, phagedenic and erosive
morphological forms are reported.33
Primary chancre may be concomitantly seen with lesions of
secondary syphilis. This could be due to rapid progression of the
disease or delayed healing of primary lesion or both.34 Mixed
infections with other STI’s like HSV, HPV are common.
Secondary syphilis – Signs of secondary syphilis may develop
sooner in HIV infected patients. The skin rash can be widespread and
lasts longer. The morphological lesions like papules, nodules, pustules,
ulcers and crusted forms can be present simultaneously. Condyloma
lata lesions are more common than in non-HIV-infected patients.
Lues maligna (malignant syphilis) is about 60 times more
frequent in HIV positive individuals.35 The likelihood of unusual
There is increased risk of relapse of secondary syphilis in HIV
co-infected patients.
Tertiary syphilis – The ulcerative or nodular manifestations of
benign tertiary syphilis is known as gumma. Even though uncommon,
gumma represents an enhanced immune response or hypersensitivity to
T.pallidum. It has been suggested that Treponema pallidum persists in
a commensal state, with the potential to recover its virulence with
immunosuppression. It may also be seen in IRIS associated with
HAART.36
Cardiovascular syphilis – It is rarely seen nowadays. Some cases of
syphilitic aortitis have been reported.37
Neurosyphilis – Rapid progression of early syphilis to neurosyphilis is
seen in HIV co-infection, often despite appropriate treatment.38
viii) Chancroid
Chancroid is a genital ulcer disease caused by Haemophilus
ducreyi, a gram negative bacteria. Men are most commonly affected.
The typical clinical presentation is single or multiple, painful,
sharp-edged, non-indurated ulcers with yellowish grey necrotic exudate
covering the floor associated with unilateral inguinal lymphadenopathy.
It is the most common cause of genital ulcer in Africa.
The risk of HIV transmission is known to increase 4 – 10 times
- Increased HIV shedding into the genital tract from ulcer
exudates.
- Bleeding from genital ulcers during intercourse leading to
potential increase in HIV shedding
- Increased HIV viral concentration in seminal fluid of men with
GUD.
- Disruption of mucosal integrity provides a portal of entry for
HIV.
- The expression of CXCR4 and CCR5 are upregulated in the
chancroidal lesions by the macrophages.
The clinical presentation of chancroid in HIV appears to have only
minor differences compared to that in HIV-negative patients. The
differences reported include longer duration of ulcer, greater number
of ulcers, extragenital lesions 39 and slightly increased rate of
treatment failures in HIV-positive patients.40
ix) Granuloma inguinale
Granuloma inguinale, caused by Calymmatobacterium
granulomatis presents clinically as a chronic, destructive, beefy red,
non-tender granulomatous ulcer of the genitalia.
HIV-positive patients have ulcers that persist for longer duration,
produces greater tissue destruction 41 and necessitates intensive
x) Lymphogranuloma venereum (LGV)
Lymphogranuloma venereum is caused by the L1, L2 and L3
serovars of Chlamydia trachomatis. Its clinical course is characterised
by primary stage (papule or transient ulcer), secondary stage (inguinal
syndrome) and tertiary stage (ano-genito-rectal).43
Few studies have reported that HIV does not have any
significant effect on LGV.44 However, prolonged antibiotic therapy may
be required and resolution of the lesions may be delayed.
b) Viral infections
i) Herpes simplex virus (HSV) infection
HSV-1 and HSV-2 infections are very common in the course of
HIV disease. In normal immunocompetent individuals, HSV infection
is self-limiting and presents as multiple grouped vesicles filled with
clear fluid and erosions which heal within 2 weeks.
HIV and HSV are co-transmitters of each other, the co-infection
being termed as ‘double trouble’. HSV-2 infected persons have twice
the risk of developing HIV compared to non-HSV patients 45 due to
mucosal barrier disruption and the presence of activated T
lymphocytes in the ulcer base.46 HIV causes frequent recurrences of
HSV thus increasing the chances of its transmission.
HIV-infected patients experience an increased number and size
compared with HIV-uninfected patients. The vesicles and ulcers heal
slower and are more painful.47
Recurrent HSV infection may accelerate the progression of HIV
disease.48 According to CDC, any non-healing ulcer of HSV lasting
more than 1 month is an AIDS defining illness and indicates active
HIV.49
Atypical HSV presentation in HIV-infected patients –
- Deep progressive painful ulceration of genital, perianal area and
lip is the hallmark of HSV in HIV-infected patients.
- Hemorrhagic lesions, ecthyma like lesions and hyperkeratotic
verrucous lesions may be seen.
- Progressive herpetic whitlow may involve the entire digit with
painful ulceration.50
- Follicular facial lesions (herpetic folliculitis) may be seen but
often misdiagnosed as bacterial folliculitis.
- With progressing immunodeficiency, HSV infection becomes
chronic, persistant, progressive, recurrent and less responsive to
oral antiviral therapy.
- Prolonged viral shedding often necessitating suppressive antiviral
therapy.
HSV may also cause esophagitis, hepatitis, pneumonitis or
life-threatening disseminated infections in AIDS patients.
ii) Varicella zoster virus (VZV) infection
Varicella zoster virus causes varicella (chickenpox) as primary
infection and herpes zoster as reactivation of dormant infections. In
HIV disease, primary varicella may be severe and prolonged.
Complications like bacterial superinfection can occur and death can
ensue with systemic dissemination.
The occurence of herpes zoster is 7-15 times common in HIV
patients and may be the first sign of immunosuppression. In HIV, it
can occur in younger age patients. The eruption may be bullous,
hemorrhagic, necrotic and accompanied by excruciating pain. The
disease runs a longer course.
The lesions may persist as hyperkeratotic, ulcerated, painful
nodules with central crusting and/or ulceration with a border of
vesicles. The lesions may be multidermatomal with severe systemic
manifestations, recurrent within the same dermatome or disseminated.
Disseminated zoster is defined as involvement of more than
three contiguous dermatomes, more than 20 lesions scattered outside
the initial dermatome or presence of systemic manifestations (hepatitis,
HIV infected patients with zoster show increased neurological
and ophthalmic complications.52 Reactivation of VZV is the commonest
cutaneous manifestation of IRIS.53
iii) Human Papilloma Virus (HPV) infection
Human Papilloma Virus, a DNA virus, is the causative agent of
warts. Cutaneous warts are commonly caused by HPV types 1, 2, 3,
4, 5, 8, 27, 57. Out of these, plantar warts are caused by HPV-1, 2;
common warts (verruca vulgaris) by HPV-2, 1, 27, 57; Plane warts by
HPV-3, 10. The subtypes HPV-3, 5, 8 is involved in EDV. HPV -5
can cause a similar disease like EDV with extensive verruca plana,
pityriasis versicolor like lesions and cutaneous reddish plaques.51 Warts
are more numerous, extensive, exuberant and refractory to usual
treatment in HIV disease.54
Warts occur more commonly in HIV infected patients.55 HIV
positive women are 5 times more likely to have genital tract
neoplasia than HIV-negative women.56 Asymptomatic shedding is also
more common in women with HIV. Extensive warts are seen with
CD4 count < 200 cells/µl.57
The low risk HPV types – HPV 6 and HPV 11, are the most
specific types causing ano-genital warts. It causes condyloma
acuminata, Giant condyloma of Buschke and Lowenstein and low
- HPV 16 and HPV 18 are responsible for high grade SIL, bowenoid
papulosis and cervical cancer.
HIV infected patients are more likely to harbour the high risk
HPV types 16 and 18. Other strains seen in HIV are HPV 7, 72, 73.
Genital warts are florid, disseminated, refractory to treatment with
chances of frequent recurrences after treatment. Squamous cell
carcinoma also arises more frequently from these lesions.
HIV-positive patients have higher rates of SIL as well as
cervical, anal and other genital cancers.58 Since, 70% of genital HPV
infection is subclinical, HIV-positive women should be regularly
screened by routine cervical examination. Invasive cervical cancer is
an AIDS defining condition and is aggressive.59
iv) Molluscum Contagiosum Virus infection
Molluscum contagiosum (MC) is caused by molluscipox virus.
Multiple facial molluscum contagiosum is a sign of advanced HIV
disease.60 It signifies CD4 count below 100 cells/µl.
The morphology of MC in HIV disease includes giant and large
(up to 2cm) or numerous (up to hundreds), disfiguring 61 endophytic,
aggregated or inflamed nodules which lack the characteristic central
The lesions persist and respond poorly to treatment. The clinical
presentation of MC in HIV must be differentiated from lesions of
cutaneous cryptococcosis, histoplasmosis and penicilliosis.62
v) Cytomegalovirus (CMV) infection
Cytomegalovirus infection occurs as an opportunistic infection in
HIV at CD4 counts below 50 cells/µl. CMV usually causes retinitis,
encephalitis and esophageal ulcers in HIV-positive patients. The
cutaneous lesions rarely occur in the form of perianal ulcerations,63
keratotic skin lesions, purpura, indurated pigmented nodules and
plaques. Concomitant HSV and CMV skin involvement may be seen.
vi) Epstein-Barr Virus
Epstein-Barr Virus is a member of the Herpesviridae family.
Following primary infection, EBV establishes lifelong latency in the
B-lymphocytes of the host. It is the causative agent of Oral Hairy
Leukoplakia (OHL) .
Occurence of OHL is thought to signal a rapid progression to
clinical AIDS.64 It presents asymptomatically with vertically arranged
parallel rows of corrugated plaques situated along the lateral borders
of the tongue. The lesion disappears on commencement of HAART
c) Fungal infections :
They may be superficial or deep.
- Superficial fungal infections:
(i) Candidiasis
It is the most common opportunistic infection,66 occurring
almost in all HIV-infected patients at some stage of the disease.67 It is
caused by the yeast Candida albicans in most of the cases. However,
other species of Candida like C.glabrata, C.dublinensis, C.tropicalis,
C.parapsilosis, C.krusei have also been described as etiological agents.
Oropharyngeal candidiasis -
Majority of patients (90%) with AIDS develop candidiasis
of the oropharynx.68 Its incidence correlates with lower CD4
counts. It has a higher prevalence in HIV patients with CD4
count < 200 cells/µl.69
Clinical types -
- Pseudo membranous candidiasis – acute and chronic types
- Atrophic (erythematous) candidiasis – acute and chronic types
- Hyperplastic candidiasis
- Median rhomboid glossitis
Pseudo membranous candidiasis is the commonest type of OPC.
It presents with creamy white plaques on the tongue, palate, buccal
mucosa and oropharynx which can be easily removed to leave an
erythematous surface. Perleche with painful fissures at the oral
commissures may also be seen.70
From the oral mucosa, candidiasis extends into the posterior
pharynx and down the oesophagus and / or tracheobronchial tree.
Oesophageal candidiasis is the most common cause of dysphagia in
HIV-infected individuals and is considered the second most common
AIDS defining disease after PCP.71 Oral candidiasis predicts AIDS in
a median of 2 years and is an indication for institution of PCP
prophylaxis and HAART.
Vulvovaginal candidiasis (VVC) –
The incidence of VVC is increased in HIV and it occurs early in
HIV infection.8 Clinically the manifestations are similar to that seen in
HIV-negative women. It presents as thick curdy white vaginal
discharge and erythema of vaginal walls with pruritus, edema, erosions
and soddening resembling ‘cottage-cheese’. Vulval infection presents as
a morbilliform rash which may extend up to thighs with satellite
Cutaneous candidiasis
Cutaneous involvement is uncommon. Candidal paronychia,
onychodystrophy and intertrigo may be seen.72 A generalised
cutaneous eruptions of papules and nodules has also been described.73
(ii) Dermatophytosis
Dermatophytosis refers to superficial fungal infection of skin, hair and
nails caused by Trichophyton, Epidermophyton or Microsporum
groups. Trichophyton rubrum is the most common agent responsible
for dermatophytosis. The infections are named depending on the sites
of involvement.
Tinea cruris
It is the dermatophytic infection of the groin. Predisposing
factors are humidity, warm climate, obesity, usage of tightly fit
undergarments leading to retention of moisture and in turn favors
fungal growth.
Tinea corporis
It is the dermatophytic infection of non-hairy areas of the body.
In HIV, it is the extension of tinea cruris beyond the groin onto the
The typical lesion in normal individuals is well defined
annular, erythematous, scaly plaque with central clearing and
peripheral spreading edges.
In HIV patients, dermatophytosis is more varied and extensive.
The lesions may lack the typical active edge and central clearing. The
penis and scrotum may also be involved.74 Other atypical
manifestations include pseudoimbricata, purpuric lesions, Majocchi’s
granuloma etc.,
Tinea capitis
It is the dermatophytic infection of the scalp. It is commonly
seen in children and not in adults. This is because, the free fatty acid
in the sebum secreted from sebaceous gland (which becomes active
from puberty onwards) plays a protective role in adults. But when it
occurs in an adult, immunocompromised status has to be always ruled
out.
T.capitis is of 2 types – Inflammatory and Non-inflammatory.
Inflammatory types include – kerion, favus, agminate folliculitis type
and abscess type. Non-inflammatory types include - black dot, grey
patch, alopecia areata like and adult glabrous type.
The typical lesion in normal individuals depends upon the type
of T. capitis varying from few broken hairs, itchy scaly patch to
characteristic feature is patchy partial hair loss with some amount of
inflammation.
In HIV-infected patients, severe tinea capitis with significant
hair loss can occur.75
Tinea pedis
It is the dermatophytic infection of the feet or toes. Constant
wearing of tight shoes causing occlusion of toe spaces is the main
predisposing factor.
T.pedis is of 4 types
– Intertriginous type – most common
- Chronic Hyperkeratotic type or Moccasin type
- Vesiculobullous type
- Acute ulcerative type
The typical lesion in normal individuals depends upon the type
of T. pedis varying from interdigital erythema, scaling and maceration
to thick plaques or tense vesicles and ulcers in toe clefts and feet.
It is common in HIV-positive homosexual men and
dermatophytes can be isolated even from the normal toe clefts in
around 7% homosexual men.76
Onychomycosis
It is the fungal infection of the nail plate. It can be caused by
by dermatophytes, it is called Tinea unguium. Trichophyton rubrum is
the commonest dermatophyte implicated in onychomycosis.
Onychomycoses can be classified into the following types
- Distal lateral subungual onychomycosis (DLSO) – most common
- Proximal subungual onychomycosis (PSO)
- Superficial white onychomycosis (SWO)
- Total dystrophic onychomycosis (TDO)
- Endonyx
Proximal subungual onychomycosis is considered as a sign of
HIV disease. The fungal infection extends from posterior nail fold to
invade the undersurface of the nail plate and gives rise to whitish
discoloration of the proximal nail plate. HAART improves
onychomycosis even in the absence of specific antifungal treatment in
some cases.77
- Deep fungal infections
(i) Cryptococcosis
Cryptococcosis is an opportunistic infection caused by the
encapsulated yeast Cryptococcus neoformans. It predominantly affects
immunocompromised hosts. They develop cryptococcosis when CD4 <
50 cells/µl. Lung is the most common portal of entry and patients
present with pleurisy, pneumonia. Cutaneous dissemination occurs in
The lesions are most commonly located on head and neck.
They present as multiple, discrete, flesh colored to red painless
papules sometimes progressing to pustules or ulcerated nodules.
Biopsy should be done to differentiate it from MC.
(ii) Penicilliosis (Talaromycosis)
It is caused by a dimorphic fungi – Penicillium (Talaromyces)
marneffei. It is an AIDS defining opportunistic infection.79-83 It
commonly occurs with CD4 < 100 cells/µl.
Clinical features include fever, anemia, weight loss, cough but
skin lesions are seen in the majority.
Cutaneous features include a generalised papular eruption with
central umbilication. Necrotic papules, nodules, folliculitis, macular
rash and mouth ulcers have also been reported.84
(iii) Histoplasmosis
It is caused by Histoplasma capsulatum, a dimorphic fungi and
is seen with advanced immunodeficiency. Disseminated histoplasmosis
is an AIDS defining illness.85, 86 It produces skin lesions in 10% cases
and the lesions resemble molluscum contagiosum, folliculitis,
(iv) Aspergillosis
Aspergillosis is caused by Aspergillus flavus and usually
presents as primary cutaneous infection occurring under adhesive tape
near central venous catheters or as disseminated infection.88
Skin lesions appear as skin-colored to pink umblicated
papules resembling molluscum contagiosum.
d) Parasitic infestations
(i) Scabies
Scabies is caused by the mite Sarcoptes scabiei var hominis.
Normally, it is characterised by nocturnal itching, positive family
history, typical lesions of papules and burrows over typical sites like
webspaces of fingers, anterior axillary fold, periumbilical area and
genitalia. In adults it spares scalp and neck. In classical scabies there
are few mites around 12-20 because most of them are destroyed by
scratching.
In HIV-infected patients, Crusted/Norwegian scabies is the
common presentation. In crusted scabies, the host's response to mites
is modified allowing them to multiply and millions of mites may be
present. Itching is often absent or minimal.
Crusted scabies presents as thick, crusted plaques over hands,
be present over face, neck, trunk and progresses to erythroderma.
Longitudinal splitting of nails may also be seen.
Other atypical clinical features include involvement of skin of
head and neck. Crusted scabies localised to soles and genitals have
been reported.89, 90
Crusted scabies is extremely contagious and difficult to eradicate
and may require repeated applications of topical scabicides along with
keratolytic agents and oral ivermectin.
(ii) Demodicosis
Demodex folliculorum is a saprophytic mite colonizing
pilosebaceous unit. It causes pustular folliculitis, blepharitis and
granulomatous rosacea.91
It occurs in HIV infection when CD4 count falls below 200
cells/µl. It presents as a pruritic, papulonodular folliculitic eruption on
face, neck and trunk.92 Demodex folliculitis can also occur as part of
IRIS.93
2) Non – infectious disorders:
a) Papulosquamous disorders
(i) Psoriasis
Psoriasis is an inflammatory papulosquamous disorder
characterised by eryhthematous plaques with thick, silvery white
of new onset psoriasis is 4-5% in HIV compared to 2% in normal
population.94
HIV associated psoriasis is paradoxical, the paradox being
psoriasis which is a T cell mediated disease occurring in HIV – a T
cell depleting disease. HIV tat protein or some viral protein acting as
superantigen and recurrent infections, could account for exacerbation of
psoriasis in HIV positive patients.95
Some of the factors hypothesized to be responsible for the
worsening of psoriasis in HIV include – immune dysregulation,
increase in viral and bacterial antigens in the skin, genetic
susceptibility and direct effects of HIV proteins on keratinocytes.96
In psoriasis developing after HIV seroconversion, palmoplantar
and flexural disease are more common than in HIV-negative patients.
Patients with psoriasis have higher prevalence of psoriatic arthritis.97
and higher frequency of guttate, inverse and erythrodermic types of
psoriasis. Erythrodermic type of psoriasis in HIV-infected patients may
be a sign of S.aureus septicaemia, resolving only after appropriate
intravenous antibiotics.98
(ii) Reactive arthritis (Reiter’s syndrome )
It consists of a triad of nongonococcal urethritis, conjunctivitis and
causes are Immune dysfunction, cellular lymphokines, arthritogenic
pathogens and the direct effect of HIV .
The classic cutaneous lesions of reactive arthritis include
hyperkeratotic plaques over palms and soles (keratoderma
blenorrhagicum) and also circinate balanitis. Geographic tongue,
asymptomatic oral erosions may be present. Nails may show Beau’s
line, horizontal ridging, subungual debris or dystrophic. Arthritis is
inflammatory and affects 1 to 5 large joints. Small joint involvement is
uncommon.
In HIV-infected patients, the association of HLA-B27 is high
99
which presents with severe arthritis. Reactive arthritis with AIDS
shows rapid progression and is often refractory to treatment.100
(iii) Seborrhoeic dermatitis
Seborrhoeic dermatitis is a type of endogenous eczema
affecting up to 80% of HIV-infected individuals. It is observed in the
early stage of HIV infection when CD4 >500 cells/µl.101 It is one of
the earliest clinical markers of HIV infection.102
The host-organism relationship is altered by the cutaneous
immune dysfunction caused by HIV leading to increased yeast
density.102,103 HIV infection itself is associated with skin surface lipid
The classical seborrhoeic dermatitis represents an aberrant
cutaneous reaction to Malassezia yeast species in the form of itchy,
scaly patches found in seborrhoeic distribution. In HIV patients,
seborrhoeic dermatitis is extensive and may even progress to
erythroderma. The severity of seborrhoeic dermatitis is increased at
CD4 < 100 cells/µl.
b) Pruritic eruptions
- Follicular eruptions
(i) Eosinophilic folliculitis
It is an idiopathic dermatitis that occurs in HIV-infected
individuals with different clinical manifestations. The etiology is
unknown, but Th2 cytokines (IL-4, IL-5), eotaxin, RANTES are increased
in lesional skin.
It presents as intensely pruritic erythematous urticarial papules,
pustules with pinpoint vesicles on the face, neck, upper chest, back,
eyelids or scalp. It can co-exist with acne vulgaris.105 The histologic
feature of EF is characterized by predominant eosinophilic infiltrate in
the follicular infundibula.106
EF is more common with CD4 < 250 cells/µl. It serves as a
marker to identify patients at immediate risk of developing
(ii) Pityrosporum folliculitis
It is caused by Malassezia furfur invading into the hair follicle.
It commonly occurs in immunosuppressed individuals.
It presents as itchy follicular papulopustules arising in crops on
the upper back, shoulders, chest and scalp. In HIV-infected patients,
follicles affected with eosinophilic folliculitis may also show increased
colonization with Malassezia yeasts.107
- Non-follicular eruptions
Pruritic papular eruption (PPE)
Pruritic papular eruptions are one of the commonest
non-infectious manifestations of HIV-AIDS. Although no etiological agent
has been documented, an exaggerated response to arthropod bites may
underlie its occurence. It is often the diagnosis of exculsion.
It presents as severely itchy, symmetrical, non-follicular papular
eruptions with excoriations on the trunk and extremities. Lichenified
plaques and patches, prurigo nodules may be seen. It follows a
waxing and waning course.10
It is seen with CD4 cell count < 100-200 cells/µl and is
regarded as a marker of advanced HIV disease.108
c) Pigmentary changes
Progessive pigmentation of skin, nails and mucosa occurs in
hyperpigmentation as seen with zidovudine and ketaconazole or due to
Addison’s disease because of opportunistic infection of adrenal cortex.
136
Due to immune system dysregulation seen in HIV, there is rise
in IL-1, IL-6 and TNF- α which leads to release of α-MSH from
anterior pituitary gland.
Hyperpigmentation can be considered a marker of immune
suppression as it is associated with low CD4 counts usually < 200
cells/µl. 106
The hyperpigmentation presents as diffuse, grey or brown
multifocal patches over skin, oral mucosa and / or nails. On
histopathological examination, there is no evident melanocyte
proliferation.
d) Neoplasms
Cancers that commonly occur in the setting of HIV are
non-Hodgkin disease, oral, anal, penile, vulvar and cutaneous squamous
cell carcinoma and basal cell carcinomas. Since the introduction of
ART, some malignancies like Kaposi sarcoma and non-Hodgkin
lymphoma have declined dramatically. 126
i) Non-Hodgkin’s lymphoma
HIV-infected patients are at an increased risk of developing
AIDS patients develop lymphomas at some point. HAART has no
effect on the incidence of NHL.
Extranodal NHL commonly occurs in gastrointestinal tract.
Primary cutaneous lymphomas comprise in 5-10% of extranodal
NHL.127 It presents as single or multiple subcutaneous nodules or
infiltrative and ulcerative lesions. Cutaneous NHL indicates advanced
NHL.
(ii) Kaposi's sarcoma
Kaposi's sarcoma is caused by Human herpes virus 8 acquired
through sexual transmission. It has been the first neoplasm to be
reported in HIV disease. It is recognized as an AIDS defining illness.
The lesion begins as multifocal pink, red, brown or purple
macules that progress to violaceous plaques or nodules which may
ulcerate. Common sites involved are legs and feet.
Kaposi’s sarcoma can occur at all stages of HIV disease.
HIV-related Kaposi’s sarcoma is known as epidemic Kaposi’s sarcoma.128
The severity of the disease does not correlate with the degree of
immunosuppression. Oral mucosal involvement of hard palate, gums
and lips and internal involvement commonly of gastrointestinal system
may be seen in HIV. As a rule, the affected patient has
In homosexuals, KS – AIDS has an aggressive course.128
AIDS-related Kaposi’s sarcoma may disseminate to involve lymph node,
viscera, skin and mucosa.129 With the advent of HAART, the
incidence of Kaposi’s sarcoma has fallen in recent times.
iii) Squamous cell carcinoma
AIDS patients have a 3 to 5 fold increased risk of developing
a nonmelanoma skin cancer. The ratio of SCC to BCC in
HIV-infected patients is approximately 1:7.130
SCC is associated with HPV infection in anogenital, cervical
and oral cancer and in epidermodysplasia verruciformis. Uncommonly,
the behavior of SCCs may be quite aggressive, with rapid growth of
primary lesions, extensive local recurrences and distant metastasis.131
Response to therapy is almost the same as in the general population.
(iv) Basal cell carcinoma
More aggressive basal cell carcinomas have been reported in
HIV patients, including metastatic BCC and multiple infundibulocystic
BCC. 132 The most common clinical and histological presentation of
BCC is the superficial type, which tends to occur on the trunk and
may be multiple.
v) Malignant melanoma
Malignant melanoma has an increased incidence in patients with
melanoma as normal naevi, benign macules or multiple nevoid lesions
have also been reported.
HIV-infected patients with malignant melanoma are more likely
to develop metastases and have a more aggressive course and worse
outcomes.134
e) Miscellaneous
Xerosis
Xerosis or generalized dryness of skin presents as polygonal
brown or skin colored scales over legs and trunk. It has been thought
to occur due to alterations in microcirculation and nutrient supply of
skin and also due to changes in the production of sweat and oil in
the skin. 135
Xerosis corresponds to declining CD4 count and can be considered as
a marker of HIV disease progression. 136
3) Adverse cutaneous drug reactions
The incidence of adverse cutaneous drug eruptions is high in
HIV disease, especially to antibacterial agents. These drug eruptions
tend to be more severe in HI-infected individuals than in non-HIV
infected individuals.109
The commonest drugs causing reactions in HIV disease are
an exanthematous eruption with fever, 1-2 weeks after starting
sulphonamide therapy.
The patterns of cutaneous eruptions seen are morbilliform
rashes, fixed drug eruptions, erythema multiforme major, Stevens –
Johnson syndrome and toxic epidermal necrolysis. Most patients with
Stevens - Johnson syndrome survive but the mortality in t