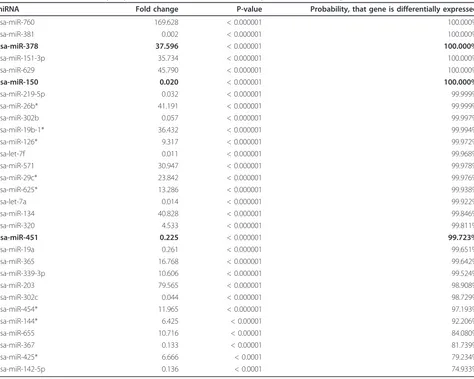
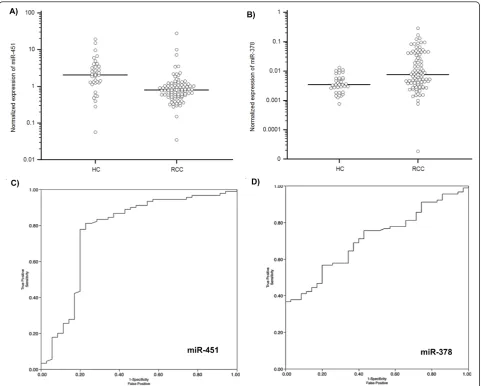
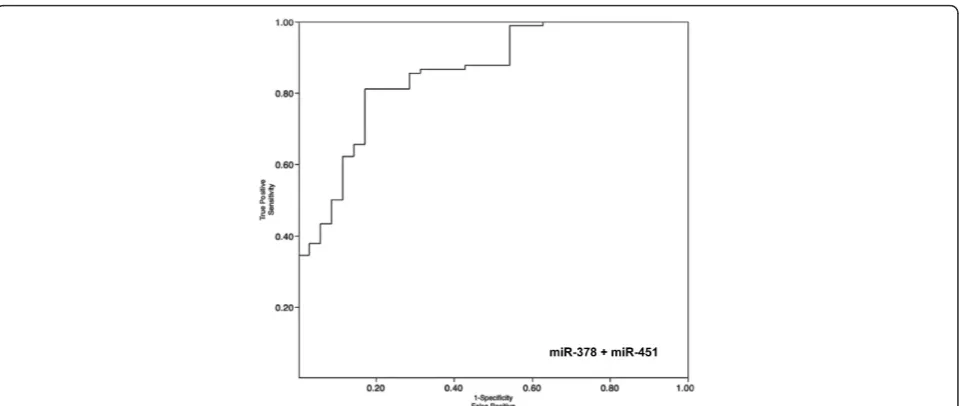
Circulating miR 378 and miR 451 in serum are potential biomarkers for renal cell carcinoma
Full text
Figure


Related documents
The pace of market implementation of technologies was estimated by considering inertia in the four phases of the roll-out trajectory: (1) policy decisions, laws and
The study is of significance as the recommendations based on the research findings would indeed be useful to (i) The stock market policy makers, a study on the
Abstract: This review summarizes important information on the ectoenzyme tissue-nonspecific al- kaline phosphatase (TNAP) and gives a brief insight into the symptoms, diagnostics,
The nucleotide sequences of ITS, D1/D2, and IGS1 regions for type strains of 16 Trichosporon human pathogen species available in GenBank as of 17 April 2018, and additional ITS
ported by the suppression of both viability and axon the Drosophila Abelson tyrosine kinase in nerves and muscles: defects of Ptp69D mutants by selective expression of
Addine a new Course to the BRI Research Database: When a new online course was added to the BRI Research Project database, it was seen that the course details also got added to the
The ascending branch, which is dominant in the vascularisation of the flap as a unique vessel, or its terminal branches which arise prior to the entrance into the muscle,
The largest part of indirect taxes is excise duty and there are significant loses in tax revenues from illegal trade of such goods as cigarettes due to the fact they are taxed with
