by
STEPHEN PETER COLLINS
STATEMENT
The i n v e s t i g a t i o n s d e s c r i b e d i n t h i s t h e s i s are my own o r i g i n a l work.
I would l i k e to thank my supervisors Dr M.A. Denborough and Dr M.D.
White f o r t h e i r very he lp fu l advice, suggestions and discussions and
f o r t h e i r assistance in the preparation of t h is th e s is .
I also thank my departmental colleagues in c lu d in g Dr L. Marjanen, Dr
G. Galloway, Mr K. Hopkinson, Mr A. Sim and Mr P. Foster f o r t h e i r
h e lp fu l advice and discussions, and Mr K. Hopkinson f o r developing
the computer programs f o r data r e t r i e v a l . Thanks are also due to the
s t a f f of the l i b r a r y , the photography department and the animal
house.
I g r a t e f u l l y acknowledge the support o f an A.N.U. Ph.D Scholarship in
the Department o f Medicine and C lin ic a l Science, John C urtin School
of Medical Research.
F i n a l l y , I would l i k e to thank my fa m ily f o r t h e i r support and
ABSTRACT
The i n h e r i t e d a n a e s t h e t i c c o mp l i c a t i o n Mal i gnant Hyperpyrexi a (MH) i s
?+
t h o u g h t t o be due t o an a b n o r ma l i t y of s k e l e t a l muscle Ca
2+
r e g u l a t i o n . Because of t h i s t h e Ca -dependent r e g u l a t o r y p r o t e i n
2 +
c al modul i n was i n v e s t i g a t e d as a p o s s i b l e cause of abnormal Ca r e g u l a t i o n in MH s u s c e p t i b l e (MHS) p o r c i n e muscl e. Calmodulin i s
2+
known t o r e g u l a t e i n t r a c e l l u l ar Ca c o n c e n t r a t i o n s and t o modulate
2+
t h e e f f e c t s of Ca i n many t i s s u e s .
The cal modul i n a n t a g o n i s t drugs were shown t o a f f e c t t h e c o n t r a c t i l e c h a r a c t e r i s t i c s of bot h c o n t r o l and MHS p o r c i n e s k e l e t a l muscle in v i t r o . These drugs i nduced c o n t r a c t u r e in c o n t r o l and MHS muscl e. Cal modul i n a n t a g o n i s t s a l s o induced MH-like h y p e r c o n t r a c t i 1 i t y in c o n t r o l muscl e and p o t e n t i a t e d t he h y p e r c o n t r a c t i l i t y of MHS muscl e. These e f f e c t s were c o n s i s t e n t wi t h t h e cal modul i n a n t a g o n i s t drugs i nduc i ng an i n c r e a s e i n myoplasmic Ca ' c o n c e n t r a t i o n in both c o n t r o l and MHS muscl e. Da nt r ol e ne sodium was a bl e t o p a r t i a l l y r e v e r s e c o n t r a c t u r e s i nduced by cal modul i n a n t a g o n i s t drugs in bot h c o n t r o l and MHS p o r c i n e muscl e.
calmodulin
antagonist
drugs.
These
drugs
in h ib ite d
the
2+Ca -dependent ATPase a c tiv ity of isolated SR preparations in a
dose-dependent manner. The extent of th is in h ib itio n was the same in
both control and MHS SR.
Calmodulin antagonist drugs in h ib ite d the
2+
ATP-dependent Ca
uptake a c tiv ity of isolated SR preparations from
both control and MHS muscle to a sim ila r extent. Also, the e fflu x of
2+
Ca
from isolated SR preparations was accelerated by calmodulin
antagonist drugs.
The extent of th is acceleration was the same in
both control and MHS SR.
These effects of calmodulin antagonist
2+
drugs on SR Ca
transport functions were consistent with th e ir in
v itro pharmacological effects on control and MHS skeletal muscle.
That is ,
these drugs affected the co n tra ctile characteristies of
2+
control and MHS muscle by raising the myoplasmic Ca
concentration.
Dantrolene sodium was unable to reverse the effects of the calmodulin
antagonist drugs on brain calmodulin a c tiv ity or skeletal muscle SR
2+
Ca
transport functions of either control or MHS tissue.
However
dantrolene sodium did p a rtia lly reverse the contractures induced by
calmodulin antagonist drugs j_n v it r o .
Since dantrolene sodium is
thought to act on the excitation-contraction coupling mechanism,
these observations suggested that the calmodulin antagonist drugs
were acting,
in part,
on th is mechanism to induce the changes in
c o n tra c tile characteristics observed in both control and MHS muscle
in v it r o .
Many of the calmodulin
antagonist drugs
used in
the
present
investigation are c lin ic a lly useful antipsychotics.
The in v itro
2+concentrations,
may be involved in two in vivo side effects of
antipsychotic therapy.
Firstly, patients undergoing antipsychotic
therapy are
at risk from heat stroke in high environmental
temperatures.
Secondly, psychiatric patients may experience a rare
and dramatic side effect of antipsychotic therapy, the Neuroleptic
Malignant Syndrome (NMS).
The symptoms of NMS are similar to those
of MH. Diagnostic studies in the present investigation and elsewhere
have shown that NMS may be associated with MH.
The observations on the effects of calmodulin antagonist drugs on
control and MHS porcine skeletal muscle strengthen the hypothesis
2
+that MH may be due to an abnormally high myoplasmic Ca
2
+concentration.
Calmodulin antagonist drugs raised myoplasmic Ca
2
+concentrations by their effects on the SR Ca
transport functions
and
excitation-contraction coupling,
thereby
inducing MH-like
hypercontractility in control muscle in vitro.
An analysis of the
effects of individual calmodulin antagonist drugs on control and MHS
skeletal
muscle
implicated the excitation-contraction coupling
List of Figures
List of Tables
Abbreviations
Abstract
Page
C h a p t e r 1 I n t r o d u c t i o n
1.1
The Malignant Hyperpyrexia Syndrome
1
1.2
Clinical Features of Malignant Hyperpyrexia
1
1.3
Anaesthetic Triggers of Malignant Hyperpyrexia
2
1.4
Treatment of Malignant Hyperpyrexia
2
1.5
Genetics of Malignant Hyperpyrexia
3
1.6
Diagnosis of Malignant Hyperpyrexia
4
1.7
Syndromes Related to Malignant Hyperpyrexia
6
1.8
Malignant Hyperpyrexia in Animals
7
1.9
Aetiology of Malignant Hyperpyrexia
7
1.10
The Site of the Basic Abnormality in Malignant
Hyperpyrexia
9
1.10.1
Skeletal Muscle and Malignant Hyperpyrexia
9
1.10.2
Structural Organization of Skeletal Muscle
10
1.10.2.1
Macroscopic Organization
10
1.10.2.2
Microscopic Organization
10
1.10.2.3
Molecular Organization
14
1.10.3
The Control of Contraction in Skeletal Muscle
15
1.10.4
The Source of Energy for Contraction in Skeletal Muscle
18
1.10.5
Dantrolene and Skeletal Muscle
18
1.11
Calmodulin
19
1.11.1
Introduction
19
1.11.2
Biological and Physicochemical Properties of Calmodulin
19
1.11.3
Calmodulin in Skeletal Muscle
24
1.11.4
Pharmacological Antagonism of Calmodulin Function
26
1.12
Pharmacological Findings in Malignant Hyperpyrexia
Page
1.13
Biochemical Findings in Malignant Hyperpyrexia
33
1.13.1
Skeletal Muscle
33
1.13.1.1
The Sarcoplasmic Reticulum
33
1.13.1.2
Muscle Proteins
36
1.13.1.3
Mitochondria
37
1.13.1.4
Electrophysiology
37
1.13.1.5
Muscle Energy Metabolism
38
1.13.1.6
Cyclic Nucleotides
39
1.13.2
Other Tissues
40
1.13.2.1
P latelets
40
1.13.2.2
Pancreas
40
1.13.2.3
Catecholamines
40
1.13.2.4
Erythrocytes
41
1.14
Summary
41
Chapter 2 The Pharmacology of Calmodulin Antagonists in
Control and Malignant Hyperpyrexia Susceptible
Porcine Skeletal Muscle
2.1
Introduction
42
2.2
Materials and Methods
44
2.2.1
Drugs and Reagents
44
2.2.2
Experimental Animals
44
2.2.3
Anaesthesia
44
2.2.4
Surgical Procedure
45
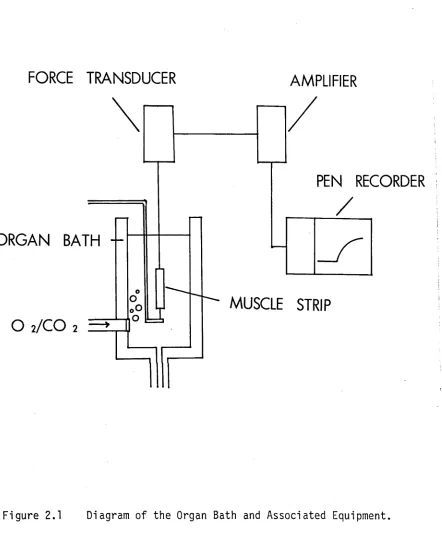
2.2.5
The Organ Bath Preparation
45
2.2.6
Data Storage and Analysis
47
2.3
Results
47
2.3.1
Id e n tific a tio n of Control and Malignant
Hyperpyrexia Susceptible Swine
47
2.3.2
Contracture Responses Induced by Calmodulin
Antagonists
50
2.3.3
The E ffect of Dantrolene on Contractures Induced by
and Potassium Chloride in Control Porcine Muscle
58
2.3.5
The Effects of Calmodulin Antagonists on Contractures
Induced by Halothane, Caffeine, Succinylcholine and
Potassium Chloride in Malignant Hyperpyrexia
Susceptible Porcine Muscle
72
2.4
Discussion
77
2.5
Summary
81
Chapter 3
Calmodulin in Porcine Malignant Hyperpyrexia
3.1
Introduction
83
3.2
Materials and Methods
84
3.2.1
Drugs and Reagents
84
3.2.2
I s o l a ti o n of Calmodulin from Control and
Malignant Hyperpyrexia Susceptible Porcine Brain
84
3.2.3
The Assay of Calmodulin Activity
85
3.2.4
The Assay of Porcine Skeletal Muscle Cyclic Adenosine
3 ' , 5' - monophosphate
86
3.2.5
U l t r a v i o l e t Absorption Spectrum of Calmodulin
86
3.2.6
Polyacrylamide Gel Electrophoresis of Proteins
87
3.2.7
Inorganic Phosphate Determinations
87
3.2.8
Protein Determinations
87
3.3
Results
87
3.3.1
I s o l a t i o n of Calmodulin from Control and Malignant
Hyperpyrexia Susceptible Porcine Brain
87
3.3.2
Sodium Dodecyl Sulphate Electrophoretic Comparison
of Calmodulins Isolated from Control and Malignant
Hyperpyrexia Susceptible Porcine Brain
88
3.3.3
Comparison of the U l t r a v i o l e t Absorption Spectra of
Calmodulin Isolated from Control and Malignant
Hyperpyrexia Susceptible Porcine Brain
93
3.3.4
Functional Studies of Calmodulin Isolated from Control
Page
3.3.4.1 A c ti va ti on of Phosphodiesterase 93
3.3 .4.2 I n h i b i t i o n of Calmodulin-Activated Phosphodiesterase
by Calmodulin Antagonists 96
3.3.5 Concentrations of Cyclic-Adenosine Monophosphate in
Control and Malignant Hyperpyrexia Susceptible Porcine
Skeletal Muscle 99
3.4 Discussion 102
3.5 Summary 107
Chapter 4 The E ffe c ts o f Calmodulin Antagonists on Is o la te d Sarcoplasmic Reticulum from Control and M alignant H yperpyrexia S u scep tib le Swine
4.1 Introd uctio n 109
4.2 Materials and Methods 110
4.2.1 Drugs and Reagents 110
4.2.2 Preparation of the Sarcoplasmic Reticulum Vesicles 110
4.2.3 Preparation of E th y l e n e g ly c o l - b i s - ( j ] -aminoethyl e t h e r )
- N ,N '- te tr a ac et a te Washed Sarcoplasmic Reticulum
Vesicles 111
4.2.4 The Calcium-Dependent Adenosine Triphosphatase Assays 111
4.2.5 The Adenosine Triphosphate-Dependent Calcium Uptake
Assay 112
4.2.6 Passively Loaded Sarcoplasmic Reticulum Calcium E f f l u x
Assay 112
4.2.7 U l t r a v i o l e t Light - Activated Binding of T r i t i a t e d
T r i fl uo p er a zi n e to Sarcoplasmic Reticulum Membrane
Proteins 113
4.2.8 Polyacryl amide Gel Electrophoresis 113
4.2.9 Inorganic Phosphate Determinations 114
4.2.10 Protein Determinations 114
4.2.11 S t a t i s t i c a l Methods 114
4.3 Results 114
4.3.1 Fragmented Sarcoplasmic Reticulum 114
2+
4.3.2 The E ff e c t of Tr if lu op er a z in e on the Ca -dependent
Adenosine Triphosphatase A c t i v i t y of Fragmented
4.3.3
4.3.4
4.3.5
4.3.6
4.4
4.5
Fragmented Sarcoplasmic Reticulum
122
The Ef fects of R24571, Penfluridol, Pimozide,
Fluphenazine, Chlorpromazine, Promethazine and
2+
Haloperidol on the Ca -dependent Adenosine
Triphosphatase of Fragmented Sarcoplasmic Reticulum
124
The Effects of Trifluoperazine, Haloperidol and
Penfluridol on the Adenosine Triphosphate-
2+
dependent Ca
Uptake by Fragmented Sarcoplasmic
Reticulum
126
The Effe cts of Trifluoperazine and Haloperidol on the
2+
Equilibrium Efflux of Ca
from Fragmented Sarcoplasmic
Reticulum
142
2+
The Effect of Caffeine on the Ca -dependent Adenosine
Triphosphatase Activity of Fragmented Sarcoplasmic
Reticulum
142
Discussion
149
Summary
153
Chapter 5
The Neuroleptic Malignant Syndrome and Malignant
Hyperpyrexia
5.1
Introduction
155
5.2
Report of a Case of Neuroleptic Malignant Syndrome
158
5.3
Discussion
161
5.4
Summary
165
Chapter 6
General Discussion
166
LIST OF FIGURES
Page
Figure
1.1 Schematic Diagram of the Muscle Cell Structure
12
Figure
1.2 Diagram of the Structure of the M yofibrils
13
Figure
1.3 Schematic Diagram of Thick and Thin Filament Structure
16
Figure
1.4 Structure of Trifluoperazine
28
Figure
2.1 Diagram of the Organ Bath and Associated Equipment
46
Figure
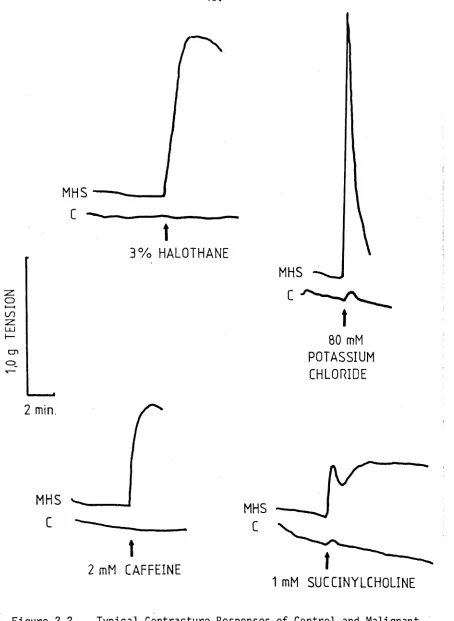
2.2 Typical
Contracture
Responses
of
Control
and
Malignant
Hyperpyrexia
Susceptible
Muscle
to
Halothane,
Caffeine,
Succinylcholine and Potassium
Chloride.
48
Figure
2.3 The
E ffect
of
Trifluoperazine
on
Control
and
Malignant Hyperpyrexia Susceptible Muscle.
(a) Typical Dose Responses to Trifluoperazine
(b)
P artial Reversal of Trifluoperazine Contracture
compared to Reversal of Haloperidol Contracture.
51
Figure 2.4
Dose Response of Contracture Induced by
Trifluoperazine in Control and Malignant Hyperpyrexia
Susceptible Muscle.
52
Figure 2.5
Dose Response of Contracture Induced by
Chlorpromazine in Control and Malignant
Hyperpyrexia Susceptible
Muscle.
53
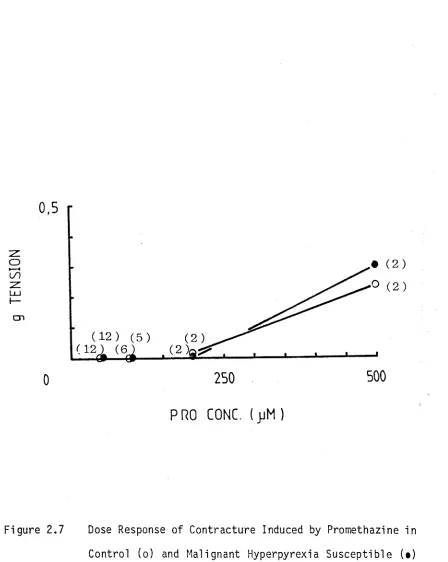
Figure 2.6
Dose Response of Contracture Induced by
Fluphenazine in Control and Malignant
Hyper pyr exi a S u s c e p t i b l e Muscle. 55
F i g u r e 2. 8 Dose Response of C o n t r a c t u r e Induced by Ha l o p e r i d o l in Cont rol and Mal i gnant
Hyper pyr exi a S u s c e p t i b l e Muscle. 56
F i g u r e 2. 9 Comparison of C o n t r a c t u r e Responses Induced by Chi or pr omazi ne, H a l o p e r i d o l , T r i f l u o p e r a z i n e , Fl u p h e n a z i n e and Pr omet hazi ne i n Cont rol and Mal i gnant Hyperpyrexi a S u s c e p t i b l e Muscle a t a
C o n c e n t r a t i o n of 50 jjM. 57
F i g u r e 2. 10 I n d u c t i o n of H y p e r c o n t r a c t i l i t y t o Hal ot hane,
C a f f e i n e and S u c c i n y l c h o l i n e by T r i f l u o p e r a z i n e in
Cont rol Por ci ne Muscle. 60
F i g u r e 2.11 Dose Response of T r i f l u o p e r a z i n e - I n d u c e d
H y p e r c o n t r a c t i l i t y t o 3% Hal ot hane in Cont rol Muscle. 63
F i g u r e 2. 12 Dose Response of T r i f l u o p e r a z i n e - I n d u c e d H y p e r c o n t r a c t i l i t y t o 2 mM Ca f f e i n e i n Control Muscle. 64
F i g u r e 2. 13 Dose Response of T r i f l u o p e r a z i n e - I n d u c e d H y p e r c o n t r a c t i l i t y t o 1 mM S u c c i n y l c h o l i n e i n Control Muscle. 65
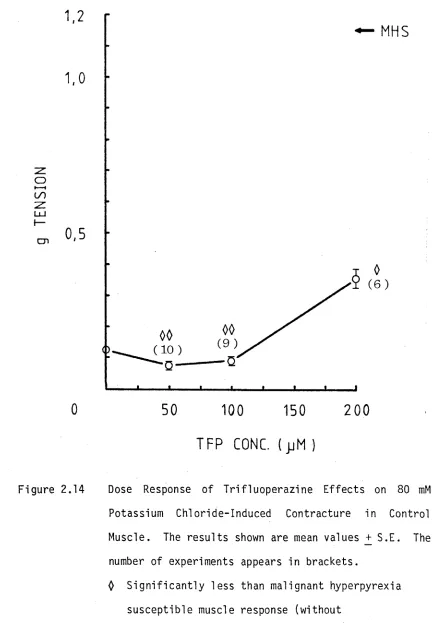
F i g u r e 2. 14 Dose Response of E f f e c t of T r i f l u o p e r a z i n e on 80 mM Pot as si um Ch l o r i d e - I n d u c e d C o n t r a c t u r e i n Cont rol
Muscl e. 66
Fi g u r e 2. 15 Comparison of 50 j jM T r i f l u o p e r a z i n e - I n d u c e d Hypercon t r a c t i l i t y t o Hal ot hane, Ca f f e i n e and S u c c i n y l c h o l i n e
Page F i gu re
Fi gu re
F i g u re
F i gu re
Fi gu re
Fi gu re
Fi gu re
F i gu re
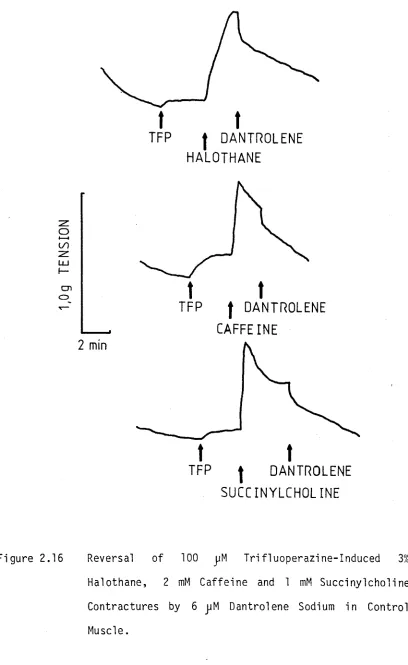
.16 Reversal o f 100 j jM T r i f l u o p e r a z i n e - I n d u c e d 3% Halothane, 2 mM C a f f e i n e and ImM S u c c i n y l c h o l i n e Cont r act ur es by 6 j jM Dantrolene i n Control Muscle.
.17 Dose Response o f T r i f l u o p e r a z i n e - I n d u c e d P o t e n t i a t i o n o f Halothane C on tr act ur e i n Malignant Hyperpyrexia S u sc e p t i b l e Muscle.
.18 Comparison o f 50jjM H a l o p e r i d o l - , 50jjM Chlorprom- a z i ne - and 50 j jM T r i f l u o p e r a z i n e - I n d u c e d P o t e n t i a t i o n o f Halothane, C a f f e i n e , and S u c c i n y l c h o l i n e C ont ract ur es i n Mali gnant Hyperpyrexia S u sce pt ib le Muscle.
.19 Reversal o f 50 jjM T r i f l u o p e r a z i n e - P o t e n t i a t e d 3% Hal othane, 2 mM C a f f e i n e and 1 mM S u c c i n y l c h o l i n e C ont ract ur es by 6 pM Dantrolene i n Malignant Hyperpyrexia S u s ce pt ib l e Muscle.
.1 E l u t i o n P r o f i l e o f P ro te i n and Calmodulin A c t i v i t y from the DEAE-Cellulose Column used i n the I s o l a t i o n o f Calmodulin from Mali gnant Hyperpyrexia S u sce pt ib le Porcine B ra in .
.2 E l u t i o n P r o f i l e o f P r o t e i n and Calmodulin A c t i v i t y from the A f f i n i t y Column used i n the I s o l a t i o n of Calmodulin from Mali gnant Hyperpyrexia S usce pt ib le Porcine B ra i n.
.3 Pol yacr yl amide Gel Patt er ns o f Various F r a c t i o n s obtained During the I s o l a t i o n o f Calmodulin from Ma li gnant Hyperpyrexia S u sce pt ib le Porcine Br ai n.
1.4 Comparison o f Pol yacryl amide Gel Pa tt er ns o f Calmodulins I s o l a t e d from Control and Malignant Hyperpyrexia Su s ce pt i bl e Porcine Br ai n.
71
73
74/75
76
89
90
91
Hyperpyrexia Susceptible Porcine Brain.
94
Figure 3.6
The Activation of Phosphodiesterase by Control and
Malignant
Hyperpyrexia
Susceptible
Porcine
Brain
Calmodulin.
95
Figure 3.7
The
Inh ibitio n
by
Trifluoperazine
of
Phosphodiesterase
Activity
Activated
by
Control
Porcine Brain Calmodulin.
97
Figure 3.8
The
I nh ib iti on
by
Trifluoperazine
of
Phosphodiesterase Activity Activated by Malignant
Hyperpyrexia Susceptible Porcine Brain Calmodulin.
98
Figure 3.9
The I n h i bi t i o n by Haloperidol of Phosphodiesterase
Activity
Activated
by
Control
Porcine
Brain
Calmodulin.
100
Figure 3.10
The I nh ib iti on
by Haloperidol of Phosphodiesterase
Act ivi ty
Activated
by
Malignant
Hyperpyrexia
Susceptible Porcine Brain Calmodulin.
101
Figure 4.1
Polyacrylamide
Gel
Patterns
of
Fragmented
Sarcoplasmic Reticulum Preparations Isol ate d from
Malignant
Hyperpyrexia
Susceptible
and
Control
Porcine Skeletal Muscle.
117
Figure 4.2
Comparison of Absorbance Scans of Polyacrylamide Gels
of Control
and Malignant Hyperpyrexia Susceptible
Fragmented Sarcoplasmic Reticulum Preparations.
118
Figure 4.3
I n h i b it i o n of Ca^+-Dependent ATPase A c t i v i t i e s of
Control
and
Malignant
Hyperpyrexia
Susceptible
Page
Figure 4.4
Efjjjct of Dantrolene Sodium
on the I n hi bit io n
of
Ca -Dependent
ATPase
A c t i v i t i e s
of
Control
and
Malignant
Hyperpyrexia
Susceptible
Fragmented
Sarcoplasmic Reticulum by Trifluoperazine.
120
Figure 4.5
Binding of U l t r a - v i o l e t Light-Activated T r i t i a t e d
Trifluoperazine to Control and Malignant Hyperpyrexia
Susceptible
Fragmented Sarcoplasmic
Reticulum
Prote ins.
122
2+
Figure 4.6
I n h i b it i o n of
Ca -Dependent ATPase A c t i v i t i e s
of
Control
and
Malignant Hyperpyrexia
Susceptible
Fragmented Sarcoplasmic Reticulum by Pe nfluridol.
127
Figure 4.7
I n h i b it i o n of
Ca^+-Dependent ATPase A c t i v i t i e s
of
Control
and
Malignant Hyperpyrexia
Susceptible
Fragmented Sarcoplasmic Reticulum by R24571.
128
Figure 4.8
I n h i b it i o n of
Ca^+-Dependent ATPase A c t i v i t i e s
of
Control
and
Malignant
Hyperpyrexia
Susceptible
Fragmented Sarcoplasmic Reticulum by Pimozide.
129
Figure 4.9
I n h i b it i o n of
Ca^+-Dependent ATPase A c t i v i t i e s
of
Control
and
Malignant
Hyperpyrexia
Susceptible
Fragmented Sarcoplasmic Reticulum by Fluphenazine.
130
Figure 4.10
I n h i b it i o n of
Ca^+-Dependent ATPase A c t i v i t i e s
of
Control
and
Malignant
Hyperpyrexia
Susceptible
Fragmented Sarcoplasmic Reticulum by Chlorpromazine.
131
2+
Figure 4.11
I n h i b it i o n of
Ca -Dependent ATPase A c t i v i t i e s
of
Control
and
Malignant
Hyperpyrexia
Susceptible
Fragmented Sarcoplasmic Reticulum by Haloperidol.
132
Figure 4.12
I n h i b it i o n of
Ca^+-Dependent ATPase A c t i v i t i e s
of
Control
and
Malignant
Hyperpyrexia
Susceptible
Malignant
Hyperpyrexia
Susceptible
Fragmented
Sarcoplasmic Reticulum by Haloperidol.
134
Figure 4.14
The
ATP-Dependent
Ca^+
Uptake
of
Control
and
Malignant
Hyperpyrexia
Susceptible
Fragmented
Sarcoplasmic Reticulum.
135
Figure 4.15
I n h ib iti on of
ATP-Dependent Cac+
Uptake of Control
Fragmented Sarcoplasmic Reticulum by T rifluo perazine .
136
Figure 4.16
I n h ib iti on of ATP-Dependent Ca^+ Uptake of Malignant
Hyperpyrexia
Susceptible
Fragmented
Sarcoplasmic
Reticulum by Trifluoperazine.
137
Figure 4.17
I n h i b it i o n of
ATP-Dependent Ca^+
Uptake of Control
Fragmented Sarcoplasmic Reticulum by Haloperidol.
138
Figure 4.18
I n h ib iti on of ATP-Dependent Ca“+ Uptake of Malignant
Hyperpyrexia
Susceptible
Fragmented
Sarcoplasmic
Reticulum by Haloperidol.
139
Figure 4.19
I n h i b it i o n of
ATP-Dependent Ca^+
Uptake of Control
Fragmented Sarcoplasmic Reticulum by Pe nf lu rid ol .
140
Figure 4.20
I n h i b it i o n of ATP-Dependent Ca^+ Uptake of Malignant
Hyperpyrexia
Susceptible
Fragmented
Sarcoplasmic
Reticulum by Penf lu rid ol .
141
Figure 4.21
Calcium
Efflux
from
Control and
Malignant
Hyperpyrexia
Susceptible
Fragmented
Sarcoplasmic
Reticulum.
143
2+
Figure 4.22
Acceleration of Ca
Efflux from Control Fragmented
Page F i g u r e 4. 23 A c c e l e r a t i o n of Ca 2+ Ef f l ux from Mal i gnant
Hyper pyr exi a S u s c e p t i b l e Fragmented Sarcopl asmi c
Ret i cul um by T r i f l u o p e r a z i n e . 145
F i g u r e 4. 24 A c c e l e r a t i o n of Ca 2+ Ef f l u x from Control Fragmented
Sa r c opl a s mi c Ret i cul um by Ha l o p e r i d o l . 146
Fi g u r e 4. 25 A c c e l e r a t i o n of Ca^+ Ef f l ux from Mal i gnant Hype r pyr exi a S u s c e p t i b l e Fragmented Sarcopl asmi c
Ret i cul um by H a l o p e r i d o l . 147
Fi g u r e 4. 26 E f f e c t of C a f f e i n e on Ca^+-Dependent ATPase A c t i v i t i e s of Cont rol and Mal i gnant Hyperpyrexi a
S u s c e p t i b l e Fragmented Sar copl asmi c Ret i cul um. 148
F i g u r e 5.1 D i a g n o s t i c Muscle C o n t r a c t u r e Te s t i ng of P a t i e n t R.M.
showing P o s i t i v e R e a c t i o n s . 160
F i g u r e 5. 2 H i s t o l o g i c a l Appearance of Vastus L a t e r a l i s Muscle of
Table 1.1
Cel l ul ar Functions
in which Calmodulin has
been
Implicated.
21
Table 1.2
Various
Compounds
which
Antagonize
Calmodulin
Act i vi t y.
27
2+
Table 1.3
Ca
Uptake by Malignant Hyperpyrexia Susceptible
Sarcoplasmic Reticulum Preparations in Relation to
Control Preparations.
35
Table 2.1
The Calmodulin Antagonist Drugs Used in the Present
Pharmacological Studies.
43
Table 2.2
Contracture
Responses
of
Control
and
Malignant
Hyperpyrexia Susceptible Swine Skeletal Muscle when
Exposed to Halothane,
Caffeine,
Succinylcholine and
Potassium Chloride.
49
Table 2.3
A Comparison of the Extent of Dantrolene Sodium
Reversal
and
Inhi bi t i on
of
Trifluoperazine
and
Haloperidol Contractures in Control and Malignant
Hyperpyrexia Susceptible Swine Muscle.
59
Table 2.4
Hyper cont r act i l i t y
Induced in
Control Muscle
and
Pot ent i at i on
Induced
in Malignant
Hyperpyrexia
Susceptible Muscle by 50
j jMTr i f l uoper azi ne.
62
Table
2.5Hypercontracti
1i t y
Induced in
Control Muscle
and
Pot ent i at i on
Induced
in Malignant
Hyperpyrexia
Susceptible Muscle by
50 jjMHaloperidol.
68Table 2.6
Hypercont ract i 1i t y
Induced in
Control Muscle
and
Pot ent i at i on
Induced
in Malignant
Hyperpyrexia
Page
Table 3.1
Table 4.1
Table 4.2
Table 4.3
Table 5.1
Concentration of Cyclic-Adenosine Monophosphate in
Control
and
Malignant
Hyperpyrexia
Susceptible
Porcine Skeletal Muscle.
103
2+
Ca -Dependent Adenosine Triphosphatase Activities of
Fragmented
Sarcoplasmic
Reticulum
Preparations
Isolated from Control
and Malignant Hyperpyrexia
Susceptible Porcine Skeletal Muscle.
115
The Effect of an Ethyleneglycol-bis-(p
-aminoethy-lether) -N,N'-tetraacetate Wash on the Inhibition of
2+
Fragmented
Sarcoplasmic
Reticulum
Ca -Dependent
Adenosine Triphosphatase Activity of Control and
Malignant
Hyperpyrexia
Susceptible
Muscle
by
Trifluoperazine.
121
2+
Calmodulin Antagonist Inhibition of Ca Dependent
Adenosine Triphosphatase Activity from Control and
Malignant Hyperpyrexia Susceptible Muscle Fragmented
Sarcoplasmic Reticulum.
125
Clinical
and
Biochemical
Similarities
Between
Malignant Hyperpyrexia and
Neuroleptic Malignant
AMP adenosine monophosphate ATP adenosine trip h o s p h a te ATPase adenosine trip h o s p h a ta s e
Ca2+ calcium
CPK c r e a tin e phosphokinase
CPM counts per minute
CPZ chlorpromazine
cyclic-AMP c y c lic -a d e n o s in e monophosphate DEAE-cellul ose d ie t h y l a m in o e t h y l - c e l l u l o s e DMSO dimethyl s u lf o x id e
E-C coupling e x c i t a t i o n - c o n t r a c t i o n coupling EDTA e th y le n e d ia m in e te tra a c e ta te
EGTA e t h y l e n e g ly c o l - b is - ( J3 - ami no-ethyl e th e r) -N ,N 1- t e t r a a c e t a t e
FPZ f 1uphenazine
FSR fragmented sarcoplasmic r e tic u lu m HPD h a lo p e rid o l
150 c o n c e n tra tio n producing 50% i n h i b i t i o n Kd d is s o c i a t i o n constant
ma mil 1iamperes
MH m alignant hyperpyrexia
MHS m alignant hyperpyrexia s u s c e p tib le
MW m olecular weight
PEN p e n f lu r i d o l
P. in o rg a n ic phosphate
PIM pimozide
PMSF phenyl m e t h y l s u l f o n y l f l u o r i d e
PRO promethazine
SDS-PAGE sodium dodecyl sulphate polyacrylam ide gel e le c tro p h o re s is
S.D. standard d e v ia tio n S.E. standard e r r o r
SR sarcoplasmic re tic u lu m TCA t r i c h l o r o a c e t i c acid
TFP t r i f 1uoperazine
CHAPTER 1 INTRODUCTION
1.1
The Malignant Hyperprexia Syndrome
Malignant Hyperpyrexia (MH) was first described in 1960 in a family
in which 10 members had died during general anaesthesia (Denborough
and Lovell, 1960).
The propositus had exhibited a drastic reaction
to anaesthesia given for the reduction of a compound fracture but had
survived.
Since that time MH has been recognized as an inherited
complication of general anaesthesia.
Susceptible individuals have a
skeletal muscle abnormality which is associated with at least three
clinically defined myopathies (King,
Denborough and Zapf,
1972;
Denborough,
Dennett and Anderson, 1973;
Moulds and Denborough,
1974d).
Estimates of the incidence of MH put it at approximately
1/14,000 general anaesthetics (McPherson and Taylor, 1982).
1.2
Clinical Features of Malignant Hyperpyrexia
The onset of a MH episode is often sudden, either during or a short
time after anaesthesia (Denborough, 1980).
The early signs may
include tachycardia,
a falling blood pressure,
arrhythmias,
tachypnoea, sweating and cyanosis of the skin (Nissen and Yonkers,
1982). Muscle rigidity is present in 70-80% of cases. Later a rapid
and sustained rise in body temperature is observed.
Serum
electrolyte estimations reveal a high potassium level and blood gas
analysis shows high carbon dioxide output.
Serum estimations show
massive increases
in muscle enzyme levels
such
as creatine
phosphokinase (CPK),
lactate dehydrogenase (LDH),
glutamic oxalic
transaminase (GOT) and hydroxybutyryl dehydrogenase (HBDH) (Britt,
coagulation, myoglobinuria and renal failu re.
A mortality rate of
60-70% is observed.
1.3
Anaesthetic Triggers of Malignant Hyperpyrexia
Most potent inhalational anaesthetics will induce MH in susceptible
individuals. These include halothane, methoxyflurane, diethyl ether,
ethylchloride, trichioroethylene,
cyclopropane and ethylene.
The
muscle relaxants succinylcholine and gallamine are also triggering
agents for MH.
Safe anaesthesia is possible in MH susceptible (MHS) patients by the
use of local, regional or spinal anaesthesia, or thiopentone, nitrous
oxide, d-tubocurarine, belladonna alkaloids and althesin (Denborough,
1980) .
1.4
Treatment of Malignant Hyperpyrexia
Fortunately,
there is a drug available which has the ab ility to
prevent or reverse a MH episode,
the muscle relaxant dantrolene
sodium (DANTRIUM, Norwich Pharmaceuticals) (Ellis and Bryant, 1972;
Kolb,
Horne and Martz,
1982).
When an MH episode occurs during
surgery,
anaesthesia should be discontinued and the operation
terminated. Dantrolene sodium should be given intravenously starting
with an i n i t i a l dose of 1-1.5 mg/kg, and repeated up to a cumulative
dose of 10 mg/kg as long as the symptoms of MH persist (Aldrete,
1981) .
3.
treatment of MH.
Cooling can be accomplished by immersion in ice and
water baths.
Metabolic acidosis can be tr eated with sodium
bicarbonate.
Di uretics such as mannitol help prevent hypernatremia
from large q u a n t i t i e s of sodium bicarbonate. Cardiac arrhythmias can
be con trolled by correction of f l u i d and e l e c t r o l y t e imbalances,
however
cardiac
a c t i v i t y
should
be
monitored
continuously.
Hyperkalemia may be reversed using 50% dextrose with soluble in su l in .
Coagulation studies should also be performed;
heparin can be used to
control coagulation i f i t develops.
Fin a lly ,
i t i s important to
monitor p a ti e n t s closely even a f t e r res olu tion of symptoms since
f a t a l recurrences of MH have been reported as occuring several hours
l a t e r (Nissen and Yonkers, 1982).
1.5
The Genetics of Malignant Hyperpyrexia
Three c l i n i c a l myopathies predisposing to MH have been defined.
The
Evans myopathy i s the most common myopathy predisposing to MH,
accounting for approximately 50% of MHS individuals (King, Denborough
and Zapf,
1972; B r i t t , Endrenyi, Pe ters, Kwong and Kadijevic, 1976).
I t i s usually sub -c lin ica l although some muscle wasting may occur,
and i s inher ite d as a Mendelian dominant c h a r a c t e r i s t i c (Denborough,
Ebeling,
King and Zapf, 1970; McPherson and Taylor, 1982).
Affected
individuals may display elevated serum CPK levels (Isaacs and Barlow,
1970).
The King-Denborough syndrome i s usually found in boys and i s probably
i n her ite d as a reces sive c h a r a c t e r i s t i c (King and Denborough,
1973).
tho rac ic kyphosis,
lumbar l o r d o s i s ,
pectus carinatum,
low-set ears
and p t o s i s .
Central-core disease i s an uncommon myopathy and is often associated
with MH (Denborough, Dennett and Anderson,
1973).
This myopathy is
characterized
by
s t r i k i n g 'c o r e '
lesion s in muscle
f i b r e s on
hi st o lo g i c al examination.
Although MH episodes have been reported in p a tie nt s suffering from
congenital muscular dystrophy ( Fle tch er, Blennow, Olsson, Ranklev and
Tornebrant,
1982) and Duchenne's muscular dystrophy (Kelfer,
Singer
and Reynolds,
1983), pharmacological t e s t i n g of muscle from p a ti e n t s
with
these
and
other
muscle
diseases does
not
show
the
h yp e rc on tr ac ti1i t y which i s c h a r a c t e r i s t i c of MH s u s c e p t i b i l i t y
(Moulds and Denborough, 1974d).
1.6
The Diagnosis of Malignant Hyperpyrexia
The
most
widely accepted
and
r e l i a b l e method
of diagnosing
s u s c e p t i b i l i t y to MH i s the in v i t r o muscle contracture t e s t (Kalow,
B r i t t ,
Terreau and Haist,
1970;
E l l i s ,
Keaney,
Harriman, Sumner,
Kyei-Mensah,
T y r r e l l , Hargreaves, Parikh and Mulrooney, 1972; Moulds
and Denborough,
1974b).
This procedure n e ce ss i t at es the excision of
a muscle biopsy specimen,
usually from the vastus l a t e r a l i s .
Fibre
bundles are cut from the specimen and suspended in a physiological
so l u t io n ,
supplied with glucose and oxygen,
and maintained at body
temperature.
The muscle s t r i p s are then exposed to 3% halothane, 2mM
5.
80mM potassium c h lo r id e . Muscle s t r ip s from susceptible in d iv id u a ls
show increased co n tracture responses at these concentrations.
Other jn_ v i t r o methods f o r id e n t if y in g s u s c e p t ib ilit y to MH using
muscle biopsy specimens have been proposed. The ATP d e pletio n te s t
was based on the observation of a decrease in the ATP concentration
in MH muscle exposed to halothane (Harrison, Saunders, Biebuyck,
Hickman, Dent, Weaver and Torblanche, 1969). I t was found, however,
th a t t h i s te s t did not i d e n t i f y a l l of the MHS population ( B r i t t ,
Endrenyi, Kalow and Peters, 1976). An increase in myophosphorylase A
in MH muscle has been proposed as a d ia g n o s tic a lly useful te s t by
W ilin e r , Wood, Cerri and B r i t t (1980), but when t h is parameter was
studied by another group (Traynor, Van Dyke and Gronert, 1983) an
unacceptably high number o f fa ls e p o s itiv e responses were observed.
In the diagnosis of MH, muscle biopsy specimens are also taken f o r
hi stop athological and ele ctro n microscopic examination. Not a l l MHS
p a tie n ts show muscle pathology and the changes are not s p e c if ic . In
a reported series of 80 MH p a tie n ts 35 showed myopathic changes at
biopsy (Harriman, 1982). The most frequent myopathic change was
in te rn a l n u c le i, and others included fla tt e n e d f i b r e s , small angular
b a s o p h ilic f i b r e s , f i b r e s p l i t t i n g , moderate atrophy, moth-eaten and
c o re -ta rg e to id f i b r e s .
The disadvantage of the above d ia gno stic methods is t h e i r invasive
nature. A number o f studies have been reported in which blood c e lls
or serum enzymes have been in ve stig a te d f o r t h e i r d ia gno stic value in
(Rosenberg, F ish e r, Reed and Addonizio, 1981). Studies of
halothane-induced ATP de pletio n in p la te le ts have produced
c o n f l i c t i n g r e s u lt s . One study reported a s ig n if ic a n t decrease of
ATP in MHS p la t e le t s when compared w ith con tro ls (Solomons, McDermott
and Mahowald, 1980) but another study observed no d iffe re n c e (Giger
and Kaplan, 1983). The most commonly studied serum enzyme in MH was
CPK which was elevated in approximately 70% of MHS in d iv id u a ls (Blank
and Gruener, 1983). Evaluation o f CPK le v e ls as a screening method
f o r MH in an ambulatory surgical p a tie n t population showed a poor
c o r r e la t io n between high serum CPK and s u s c e p t i b i l i t y to MH
(Amaranath, Lavin, Trusso and Boutros, 1983). Typing of the human
leukocyte antigen in a sing le MHS fa m ily showed no d ia gno stic value
(Lutsky, Witkowski and Henschel, 1982).
Anthropometric studies ( th a t i s , h e ig h t, weight and s k in fo ld
thickness) have been shown to be of no dia gno stic value in MH
(Campbell, E l l i s , Hal sal 1 and Hogge, 1982).
1.7 Syndromes Related to Malignant Hyperpyrexia
Malignant hyperpyrexia usu a lly presents c l i n i c a l l y in susceptible
in d iv id u a ls when anaesthesia is induced with drugs which t r ig g e r MH.
I t may also present, however, as heat-stroke a f t e r severe physical
stress (Denborough, 1982) or rhabdomyolysis a f t e r serious in fe c tio n s
(Denborough, C o llin s and Hopkinson, 1984). In the case of
h e a t-s tro k e , dantrolene sodium has been shown to be an e f f e c t iv e
treatment (Denborough, 1982; L y d ia tt and H i l l , 1981). An association
between MH and the sudden in fa n t death syndrome (SIDS) has also been
7.
5 out of 15 parents whose children had died from SIDS were i d e n t i f i e d
as MHS.
1.8
Malignant Hyperpyrexia in Animals
Malignant hyperpyrexia has been i d e n t i f i e d in pigs (Hall,
Woolf,
Bradley and J o l l y ,
1966),
cats (De Jong,
Heavner and Amory, 1974),
dogs (Short and Paddleford,
1973) and horses (Williams,
1976).
Porcine MH has become the animal model of human MH with _in_ v i tr o
pharmacological
studi es
of
skeletal
muscle
showing
ide n ti ca l
behaviour in both species (Okumura, Crocker and Denborough, 1979).
The MH s u s c e p t i b i l i t y found in pigs i s associated with two other
conditions r e s u l t i n g from inte rbree ding .
These are the porcine
s t r e s s syndrome (PSS) and the pale,
s o f t ,
exudative pork syndrome
(PSEP).
Porcine s t r e s s syndrome i s induced by s t r e s s e s such as
f i g h ti n g or t r a n s p o r t a t i o n and i t s symptoms include shortness of
br eath,
increasing body temperature, patchy cyanosis of the skin and
collapse and death within a few minutes (Topel,
Bicknell,
Preston,
Christian and Matsushima, 1968).
Pale, s o f t , exudative pork syndrome
r e f e r s to poor meat qu a lit y post-mortem and i s a fe a t u r e of f a s t
glycolysing muscle which produces large q u a n ti t ie s of l a c t a t e before
the muscle can be cooled (Briskey,
1964).
I t appears t h a t MH,
PSS
and PSEP are d i f f e r e n t manifestations of the same syndrome in swine
(Nelson, 1973).
1.9
The Aetiology of Malignant Hyperpyrexia
The major p r e c i p i t a t i n g event when a MHS individual or MHS pig is
Ca^+ concentration (Britt,
1983;
Denborough,
1980).
The basic
abnormality in MH muscle accounting for this rise has yet to be
elucidated although a number of poss ibi lities have been suggested.
These included an abnormality of excitation-contraction coupling (E-C
coupling) (Denborough, 1980; Okumura, Crocker and Denborough, 1980),
an abnormality of Ca
uptake by the sarcoplasmic reticulum (SR)
(Gronert, Heffron and Taylor, 1979; Blank, Gruener, Suffecool and
2+
Thompson,
1981), an abnormality of Ca
release by the SR (Nelson,
1983; Ohnishi, Taylor and Gronert, 1983), defective Ca^+ storage by
the mitochondria (Cheah and Cheah,
1978,
1979),
or an increased
adenylate cyclase activity with a resulting increase in cyclic-AMP
levels (Willner, Cerri and Wood, 1981).
2+
Whatever the basic cause,
a rise in myoplasmic Ca
will have
multiple heat-producing effects. Phosphorylase will become activated
leading to the breakdown of glycogen to lactic acid,
carbon dioxide
and heat.
Actomyosin ATPase will become activated and hydrolyze ATP
to ADP,
phosphate,
heat,
and energy which is utilized in muscle
2+
contraction.
Ca
will
also bind to troponin C in it ia t in g
2+
9.
and molecules d if f u s e in to and out of the muscle c e l l . Calcium ions
flo w in to the c e ll f u r t h e r exacerbating the s it u a t io n . Once the
sarcolemma has been breached, enzymes and myoglobin leak outward, and
myoglobin can o b s tru c t the renal tubules and cause renal f a i l u r e .
The changes produced in serum pH and e le c t r o ly t e balance can act on
body tissu e s and cause haemolysis, consumption coagulopathy, and
cardiac arrhythmias ( B r i t t , 1983; Denborough, 1980).
1.10 The S ite of the Basic Abnormality in Malignant Hyperpyrexia
1.10.1 Skeletal Muscle and Malignant Hyperpyrexia
I t is accepted th a t ske le ta l muscle is the s it e of the basic
abnormality in MHS in d iv id u a ls . This b e l ie f was based, in the f i r s t
insta nce, on a number o f c l i n i c a l observations of MH episodes.
During a MH c r i s i s the s ke le ta l musculature of many p a tie n ts displays
a generalized r i g i d i t y . The serum le v e ls of muscle s p e c ific enzymes
such as CPK show dramatic increases, in d ic a tin g muscle damage ( B r i t t ,
1979). Also the observation th a t in the face of generalized r i g i d i t y
during a MH episode a limb to which a tou rniq uet had been applied
e a rly in anaethesia remained f l a c c i d , ind ica ted th a t the anaesthetic
was a ffe c tin g s k e le ta l muscle (Drury and G ilbe rtson , 1970). I t was
also found th a t some MHS in d iv id u a ls showed c l i n i c a l l y discernable
myopathies (Denborough, Ebeling, King and Zapf, 1970; King,
Denborough and Zapf, 1972; Denborough, Dennett and Anderson, 1973;
Moulds and Denborough, 1974d) and th a t approximately 70% of
susceptible in d iv id u a ls have an elevated re s tin g serum CPK (Isaacs
and Barlow, 1970). Following these observations, in v i t r o
pharmacological studies of s ke le ta l muscle from MHS in d iv id u a ls have
and Hai s t, 1970; E l l i s , Keaney, Harriman, Sumner, Kyei-Mensah,
T y r r e l l , Hargreaves, Parikh and Mulrooney, 1972; Moulds and
Denborough, 1974a). Before going on to describe the pharmacological
and biochemical fin d in g s in MH muscle the s tru c tu re and biochemistry
of skele tal muscle w i l l be b r i e f l y reviewed.
1.10.2 S tru c tu ra l Organisation of Skeletal Muscle
1.10.2.1 Macroscopic Organization
Skeletal muscle accounts f o r 40-50% of t o t a l mammalian body weight,
and i t s spe cialized fu n c tio n is to convert chemical energy in to
c o n t r a c t ile fo r c e . The muscle consists of a large number of muscle
f i b r e s which are elongated, m u ltin u cle a te c e lls running from one end
of a muscle to the oth e r. These f ib r e s can be 10 cm or more in
length and t h e i r diameters range from 10-100 jjm. In d ivid u a l fib r e s
are separated from t h e i r neighbours by a f in e network of collagen
f i b r i l s ca lle d the endomysium. Groups of muscle f i b r e s , or
fa s c ic le s , are divided from one another by another collagen laye r
c a lle d the perimysium, and f i n a l l y the whole muscle is enclosed in a
strong collagen coat, the epimysium.
1.10.2.2 Microscopic Organization
The plasma membrane o f a muscle f i b r e is re fe rre d to as the
sarcolemma. The c o n t r a c t ile elements, the m y o f ib r ils , take up 85-90%
of the f i b r e volume. They are surrounded and bathed by the
sarcoplasm, the i n t r a c e l l u l a r f l u i d of muscle. The sarcoplasm
contains glycogen, g ly c o ly t ic enzymes, ATP, phosphocreatine and
inorganic e le c t r o ly t e s , as well as a number of amino acids and
muscles,
are regularly arranged along the myofibrils.
The muscle
fibre also contains a highly differentiated endoplasmic reticulum
known as the sarcoplasmic reticulum (SR) which functions in the
control of contraction as a store of Ca
(Figure 1.1).
The
t-tubules, invaginations of the sarcolemma, form junctions with the
terminal cisternae of the SR (triad junctions) (Figure 1.1).
The myofibrils are irregular polygons in cross-section with a mean
diameter of 1 pm and of indefinite length.
They are composed of
serially repeating segments, the sarcomeres, the lateral alignment of
which gives rise to the characteristic cross striations of the whole
fibre (Figure 1.2). The light bands are called isotropic or I bands,
and the dark bands are called anisotropic or A bands.
In resting
muscle,
the A bands are approximately 1.6 pm long and the I bands
approximately 1 pm long.
The I bands are bisected by a dense
o
transverse line about 800 A wide known as the Z line.
The central
portion of the A band, approximately 0.5 pm wide, called the H zone
and less dense than the rest of the A band,
is bisected by another
dense, transverse line, the M
line. The serially repeated unit, the
sarcomere, extends from Z line to Z line (Figure 1.2) (Landon, 1982).
12
.M yofibrils
S arcolem m a
Transverse tubule
M ito ch o n d rio n
Term inal cisternae T ria d o f the
reticulum
Z line
A band
I band
Transverse tubule
13
.SKELETAL MUSCLE
Muscle
L ig h t
t h i c k fila m e n ts extend throughout the A band, and the th in filam e nts
extend from the Z l i n e to the H zone boundary. The overlap of the
two fila m e n t types gives r is e to the denser parts of the A band. In
these denser regions re g u la r ly disposed cross-bridges between the
t h ic k fila m e n ts and adjacent t h in fila m e n ts have been observed.
These cross-bridges p ro je c t from the th ic k filam ents (Sjostrom and
S quire, 1977). During c o n tra c tio n the I band and H zone are
shortened w hile the A band length remains unchanged. Observations
such as these led to the fo rm ula tion of the s lid in g - fila m e n t theory
of muscle c o n tra c tio n (Huxley and Hansen, 1954; Huxley and
Niedergerke, 1954). In t h is th e o ry , changes in the length of a
muscle are due to the s lid in g of the th ic k and th in filam e nts past
each other due to t h e i r in te r a c tio n through the c ro ss-b rid g e s.
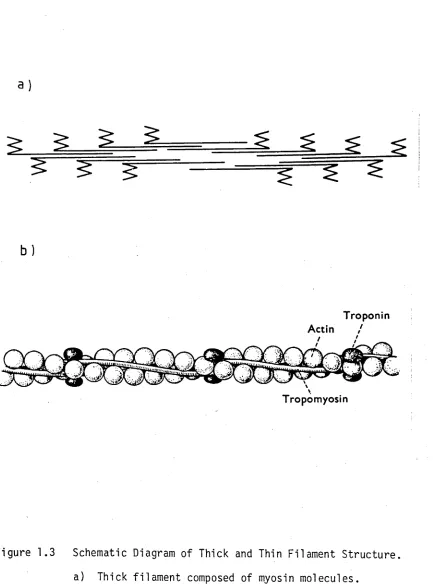
1 .1 0 .2 .3 Molecular Organization
The t h ic k fila m e n ts are composed almost e n t ir e ly of the p ro te in
myosin. The myosin molecule is rod shaped (approximately 150 nm
long) with a molecular weight (MW) o f 470,000. I t is made up of two
strands forming an a lp h a -h e lix and bears two pear-shaped heads at one
end ( E l l i o t and O ffe r, 1978). The shafts of the myosin molecules
stack together to form the sha ft o f the th ic k fila m e n t in such a
manner th a t the paired heads l i e on i t s surface, and the myosin
molecules in each h a lf of each th ic k fila m e n t are arrayed with
opposite p o l a r i t i e s (Figure 1.3a) (Huxley, 1963). The myosin heads
correspond to the crossbridges seen between the th ic k and the th in
fila m e n ts . The th in filam e nts are composed mainly of a c tin . The
a c tin monomer (G a c tin ) is a g lo b u la r molecule (diameter 5.46 nm)
1 5
.
actin), a right handed, two stranded helix (diameter 6-7 nm) twisted
so that there are 13-15 6 actin molecules for every full rotation of
the helix (Huxley and Brown, 1967). A second thin filament protein,
tropomyosin, lies in the grooves on either side of the two chains of
actin molecules (Figure 1.3b).
Tropomyosin is a rod shaped,
left-handed alpha-helix 38.5 nm long with a MW of 63,000.
These
molecules lie head to tail along the length of the thin filament
(Cohen, Caspar, Parry and Lucas, 1971; Ebashi, 1980). The third thin
filament protein is troponin.
This structure is globular with a MW
of about 80,000 (Ebashi, Kodama and Ebashi, 1968). One troponin unit
is attached to each tropomyosin molecule to give a periodicity of
38.5 nm along the thin filament (Ohtsuki, 1975). Troponin itself is
made up of three subunits, I, C and T. Troponin T binds the structure
to tropomyosin,
troponin I inhibits the interaction of the thick
filament cross-bridges with the thin filament, and troponin C confers
Ca“+ sensitivity on this inhibition (Potter and Gergely, 1974). The
2
+binding of Ca
to troponin C allows interaction between the thick
and thin filaments, and thus allows contraction to proceed (assuming
energy is avai 1 able).
1.10.3 The Control of Contraction in Skeletal Muscle
2
+In resting muscle the Ca
concentration in the sarcoplasm is in the
range 10~^-10"^ M (Ashley,
1978),
intracellul ar Ca^+ being
sequestered by the SR. This concentration gradient is upheld by a
2+ 2+
Ca -dependent transport ATPase present in the SR membrane. The Ca
2+
is stored within the SR bound to a high capacity, low affinity Ca
b )
Troponin
Tropomyosin
Figure 1.3 Schematic Diagram o f Thick and Thin Filament S tru c tu re .
a) Thick fila m e n t composed of myosin molecules.
b) Thin fila m e n t composed of a c tin , tropomyosin and
tr o p o n in .
[image:39.541.71.504.46.630.2]1 7.
the in n e rv a tin g motor-neuron stim ulates the muscle c e ll to co n tract
( th a t i s , - releases a ce tylch o lin e at the motor endplate) the
sarcolemma becomes depolarized. This tra n s ie n t d e p o la riza tio n (from
a re s tin g le ve l of -90 mV to -50 mV), re s u ltin g from a voltage and
time-dependent increase in sodium conductance, spreads over the
sarcolemma and t-t u b u le s in to the i n t e r i o r of the f i b r e (Nastuk and
Hodgkin, 1950). Here the t- tu b u le s form t h e i r t r i a d i c ju n c tio n s w ith
the SR (Figure 1.1) and through an unknown coupling mechanism
stim u la te the SR to release i t s stored Ca (Costantin, 1975). When
2+
the nervous s tim u la tio n ceases, release ceases, the Ca -dependent
2+
tra n s p o rt ATPase can again reduce the sarcoplasmic Ca concentration
and the f i b r e relaxes (Martonosi, 1982).
The nature o f the coupling between the t - t u b u le and the SR at the
t r i a d ju n c tio n ( e x c it a tio n - c o n tr a c t io n or E-C coupling) has received
o
much in v e s tig a tio n . I t is known th a t the ju n c tio n a l gap (100-200 A
wide) is bridged by re g u la rly disposed d e n s itie s termed SR fe e t
(Franzini-Armstrong, 1980). Schneider and Chandler (1973) proposed
th a t charge movement w ith in the t- t u b u le membrane d i r e c t l y e ffe c ts
2+
the SR membrane p e rm e a b ility to Ca , the fe e t acting as the l i n k
between the two. Mathias, Levis and Eixenberg (1980), on the other
hand, envisaged a p e rm e a b ility channel spanning the e n tir e ju n c tio n a l
gap. The t - t u b u le d e p o la riz a tio n led to i t s t r a n s it o r y opening and
subsequently to the i n i t i a t i o n of a voltage-dependent increase in
2+
p e rm e a b ility to Ca o f the SR membrane. Other the o rie s of E-C
coupling in s k e le ta l muscle provide no e x p l i c i t ro le f o r the SR f e e t .
The most important among these is the ' t r i g g e r ' Ca theory (Endo,
2+
release of a small amount of Ca from the t- t u b u le , e ith e r bound to
the membrane surface or w ith in the tu b u le , leads to the release of
2+
la rg e r amounts o f Ca from the SR i t s e l f , thus i n i t i a t i n g
c o n tr a c t io n .
1.10.4 The Source of Energy f o r Contraction in Skeletal Muscle
The energy required by skele tal muscle to generate c o n t r a c t ile fo rc e
i s provided by ATP. The s lid in g of the th ic k and th in fila m e n ts past
one another is accomplished by the c y c lic a l attachment and release o f
the cross-bridges and is driven by an ATPase enzyme w ith in the myosin
molecule (Huxley, 1962). The amount of ATP stored in muscle can
sustain c o n tra c tio n f o r only a f r a c t io n of a second. High energy
phosphoryl groups are stored in the form of phosphocreatine. This
compound replenishes the ATP supply through the action of CPK.
Phosphocreatine + ADP ^ ATP + cre atine
As phosphocreatine stores are depleted the level of ATP f a l l s and the
le v e ls of ADP and P.. r i s e . The level of AMP also ris e s through the
action of adenylate kinase.
2 ADP 5=* ATP + AMP
The re s u ltin g f a l l in the muscle c e ll energy charge stim ulates
g ly c o ly s is , the c i t r i c acid cycle and o x id a tiv e phosphorylation. The
r e la t i v e c o n trib u tio n of these pathways to ATP generation depends on
the type of muscle examined.
1.10.5 Dantrolene Sodium and Skeletal Muscle
Dantrolene sodium (DANTRIUM, Norwich Pharmaceuticals) is a l i p i d
1 9.
1967).
I t is a skeletal muscle relaxant which acts directly on
muscle (Ellis, Castellion, Honkomp, Wessels, Carpenter and Halliday,
1973) and is thought to inhibit E-C coupling (Ellis and Bryant,
1972).
Dantrolene sodium has been shown to lower resting myoplasmic
2+ 2+
Ca
concentrations and to inhibit the release of Ca
from the SR in
intact ce lls,
(Desmedt and Hainaut,
1977,
1979),
but i t did not
2+ 2+
stimulate the Ca -dependent ATPase of isolated SR or affect Ca
exchange or efflux rates of isolated SR (White,
Collins and
Denborough, 1983).
1.11
Calmoduli n
1.11.1
Introduction
2+
Over 40 years ago Heilbrunn (1943) considered that Ca
played a
central role in almost every physiological process.
Although today
2+
i t -is known that Ca
does not play as universal a role as Heilbrunn
2+
suggested,
Ca
exerts a profound influence on many biological
processes such as cell motility, muscle contraction,
axonal flow,
cytoplasmic streaming, chromosome movement, neurotransmitter release,
endocytosis and exocytosis. Since 1970 i t has become clear that many
2+
of the cellular effects of Ca
are mediated through a primary
2+