STUDY OF LIPID PROFILE AND THYROID FUNCTION
ABNORMALITY IN CHILDREN OF NEPHROTIC
SYNDROME
Dissertation submitted in partial fulfilment of the
Requirement for the award of the Degree of
M.D. DEGREE
–
BRANCH VII
PAEDIATRICS
APRIL 2017
TIRUNELVELI MEDICAL COLLEGE HOSPITAL
THE TAMIL NADU DR.M.G.R. MEDICAL UNIVERSITY,
CHENNAI,
CERTIFICATE
This is to certify that the Dissertation entitled “
STUDY OF LIPID
PROFILE
AND
THYROID
FUNCTION
ABNORMALITY
IN
CHILDREN OF NEPHROTIC SYNDROME
”
submitted by Dr.J.DENNY
CLARIN, MBBS., DCH., to The Tamilnadu Dr.M.G.R. Medical University,
Chennai, in partial fulfilment for the award of M.D (Paediatrics) is a bonafide
work carried out by his under my guidance and supervision during the
academic year 2015-2017. This dissertation partially or fully has not been
submitted for any other degree or diploma of this university or other.
GUIDE
Prof.Dr.C.Krishnamurthy,MD.,
(Paediatrics).,
Department Paediatrics,
Tirunelveli Medical College,
Tirunelveli- 627011.
HOD
Prof.Dr.C.Krishnamurthy,MD.,
(Paediatrics).,
Department Paediatrics,
Tirunelveli Medical College,
Tirunelveli- 627011.
Dr.K.Sithy Athiya Munarvah,
THE DEAN,
DECLARATION
I, Dr.J.DENNY CLARIN, MBBS., DCH., solemnly declare that the
Dissertation titled
“
STUDY OF LIPID PROFILE AND THYROID
FUNCTION ABNORMALITY IN CHILDREN OF NEPHROTIC
SYNDROME
”
had been prepared by me under the expert guidance and
supervision of
Prof.Dr.C.Krishnamurthy,MD.,(Paediatrics).,Professor,
Department of Paediatrics, Tirunelveli Medical College Hospital, Tirunelveli.
The dissertation is submitted to The Tamilnadu Dr. M.G.R. Medical
University, Chennai in partial fulfilment of the regulation for the award of
M.D. Degree (Branch VII) in Paediatrics.
It was not submitted to the award of any degree/diploma to any
University either in part or in full previously.
Place: Tirunelveli.
Date:
Dr.J.DENNY CLARIN, MBBS.,DCH.,
POST GRADUATE,
M.D. (Paediatrics),
ACKNOWLEDGEMENT
I am very much thankful to the Dean Dr.K.Sithy Athiya Munarvah,
Triunelveli Medical College Hospital, Tirunelveli, who has granted
permission to do this study in this institution,
I take this opportunity to express my deepest sense of gratitude to
professor
Prof.Dr.C.Krishnamurthy,MD.,(Paediatrics).,
Head of the
Department of Paediatrics, Tirunelveli Medical College Hospital, Tirunelveli
for encouraging me and rendering timely suggestions and guiding me
throughout the course of this study. I will be forever indebted to his for his
constant support.
I sincerely thank my professors Dr.T.R.R. Ananthy Shri, M.D.,
(Paediatrics)., Prof.Dr. A.S.Babu Kandakumar, MD.,DCH., Prof. Dr.J.
Rukmani, M.D.,(Paediatrics)., Prof. Dr.C. Baskar, M.D.,(Paediatrics).,
for their support and guidance.
I
am
very
much
thankful
to
professor
Dr.V.Ramasubramanian,M.D.,DM., Head of Department of Nephrology
for providing valuable support and guiding throughout the study.
I
am
very
much
thankful
to
professor
Dr.Saradha,M.D.,(Biochemistry) Head of Department of Biochemistry for
I
am
extremely
thankful
to
my
guide.,
Prof.Dr.C.Krishnamurthy,MD.,(Paediatrics)., for guiding me throughout
the study.
I am extremely thankful to all my Assistant Professors of the
Department of Paediatrics for their guidance and support throughout my
study period in this institution.
I
thank
Dr.Rizwan,M.D.,(Community
Medicine),
Dr.Heber
Anandan,M.Pharm,PhD., Mr.Mohammed Ali,Pharm.D., for their useful
inputs regarding statistics.
I wish to express my gratitude to my parents, my brother, my wife and
my son & daughter for their support throughout my study.
I also like to express my gratitude to my friends and colleagues who
ABBREVIATIONS
ANP
Atrial naturetic peptide
ACE
Angiotensin converting enzyme
CBC
Complete blood count
CKD
Chronic kidney disease
CsA
Cyclosporine
ESRD
End stage renal disease
FSGS
Focal segmental glomerulosclerosis
FRNS
Frequently relapsing nephrotic syndrome
FGGS
Focal global glomerula sclerosis
FENA
Fractional excretion of sodium
GBM
Glomerular basement membrane
LDL
Low density lipoprotein
MCNS Minimal change nephrotic syndrome
MN
Membranous nephropathy
MPNS Membrano proliferativre nephrotic syndrome
RAAS
Rennin angiotensin aldosterone system
SSNS
Steroid sensitive nephrotic syndrome
SDNS
Steroid dependenet nephrotic syndrome
SRNS
Steroid resistant nephrotic syndrome
SLE
TSH
Systemic lupus erythematosus
Thyroid stimulating hormone
VLDL
Very low density lipoprotein
CONTENTS:
S.No
TITLE
PAGE NUMBER
1.
INTRODUCTION
1
2.
AIMS OF THE STUDY
3
3.
REVIEW OF LITERATURE
4
4.
MATERIALS AND METHODS
7
5.
OBSERVATIONS AND RESULTS
49
6.
DISCUSSION
72
7.
CONCLUSION
76
8.
BIBLIOGRAPHY
9.
PROFORMA
INTRODUCTION
Nephrotic syndrome is characterized by massive proteinuria, (>40mg/m2/hr (or)>100mg/m2/day (or) >3.5gm/day (or) spot protein
creatinine ratio of >2), will lead to hypoproteinemia (serum albumin <2.5gm/dl), generalized edema and hyperlipidemia (serum cholesterol >200mg/dl).1
1-3 per100000 children less than 16yrs affected with nephrotic syndrome. Most of them affected with primary or idiopathic type. Minimal change disease is the most common idiopathic type. One of the characteristic feature of nephrotic syndrome is 80% of them respond to corticosteroid therapy.
In nephrotic syndrome there will be elevated serum lipids and cholesterol level. During nephrosis there will be more loss of protein in urine this will lead to hypoalbuminemia. In addition to low serum albumin, more production of lipoproteins with impaired lipoprotein lipase activity will increase the lipoprotein level. Lipids are mainly transported by lipoproteins, so in nephrotic syndrome becoz of more lipoproteins there will high serum cholesterol, LDL cholesterol, VLDL cholesterol and Triglycerides.(2)
Thyroid hormones T3 and T4 binds with thyroid binding globulin ,pre albumin and albumin in circulation(3).During nephrosis due to loss of
production.(4)Afroz S et al in 2011 told that even though urinary losses of
thyroid hormones, T3 and T4 level were normal with compensatory rise in TSH level(5).so during proteinuria phase there will be mild or subclinical
hypothyroidism. Because it is a treatable condition in all cases of nephrotic syndrome always investigate for hypothyroidism.
Many studies were done in the past in nephrotic syndrome to evaluate lipid profile and thyroid function test both in active disease and in remission. In active disease that is in proteinuria phase there is hypercholesterolemia and mild (or) subclinical hypothyroidism. During remission after completion of 6 weeks of steroids there will be normalisation of serum cholesterol and thyroid function.so if the serum cholesterol level was high even during remission more risk for relapses. Serum albumin shows inverse relation with lipid profile and TSH. So more severe the hypoalbuminemia more will be serum cholesterol and TSH.
Aim of the Study
To study the correlation between lipid and thyroid Profile with different types of nephrotic syndrome in children between 1 to12yrs. And also study the association between serum albumin with lipid profile and TSH.
Objectives
1. To study the correlation between lipid profile with different types of nephrotic syndrome.
2. To study the correlation between thyroid profile with different type of nephrotic syndrome.
REVIEW OF LITERATURE
Dnyanesh DG et al(6) conducted study on serum lipids in nephrotic
syndrome at Department of pediatrics KLE University Jawaharlal Nehru Medical CollegeBelgaum, Karnataka,India.Which includes 30 cases of nephrotic syndrome and 10 controls with normal renal and liver functions, age of less than 12yrs.Lipid profile was done during active disease and after one month of steroids. They found that there will be rise in serum cholesterol,LDL, VLDL and triglycerides when compared to controls. Compared to first episode serum cholesterol significantly elevated in relapse cases and in SRNS than in SDNS.In relapse cases even after 4 weeks of steroid therapy there will be no significant fall in serum cholesterol ,LDL,VLDL and triglycerides compared to significant fall in first episode of steroid responsive nephrotic syndrome.They also found the inverse relation between albumin and serum cholesterol.
P.Beck et al(7) done a study on lipid profile and its correlation with serum
Indumati.V et al(1) in 2011 done a study on serum proteins, intial and
follow-up lipid profile in children with nephrotic syndrome in department of Biochemistry,VIMS,Bellary,Karnataka,india.20 newly diagnosed cases of nephrotic syndrome in between 1 to12yrs selected for study and mean age of presentation 5.85 yrs. Two samples are taken one at the time of admission and another at discharge. They told at the time diagnosis there is hypoalbuminemia and hypercholesterolemia but during discharge that is after achieving remission statistically significant rise serum albumin and fall in serum cholesterol.
Vidhi shani et al(8) 2013 done a study on hypothyroidism in nephrotic
syndrome from June 2012 to December 2013 at dept. Of paediatrics,.B.D Sharma PGIMS, Rohtak.35 children of nephrotic syndrome between 1 to 8 yrs were included in study.2 samples of thyroid function test were taken one during the episode and another during remission. They found facial puffiness is the common presentation. They concluded that T3 and T4 were with in normal range both during active disease and in remission, but TSH value was high during the episode and produce a state of mild (or) sub clinical hypothyroidism but become normal during remission. They found inverse relation between albumin and TSH, with more severe the hypoalbuminemia more will be the TSH.They also concluded that thyroxine treatment not at all required during temporary hypothyroidism.
MATERIALS AND METHODS
Study Centre:
Study was conducted at Department of paediatrics, Tirunelveli Medical College, Hospital Tirunelveli.
Study group:
All cases of nephrotic syndrome which includes 1episode, relapse, sdns, srns and remission between age group of 1 to 12yrs.
Study design:
Cross sectional study
Study duration:
9months from December 2015 to august 2016
Sample size:
40 cases of nephrotic syndrome between 1 to12 yrs. Which include all type of nephrotic syndrome.
Collaborating department:
Inclusion criteria:
1. All cases of nephrotic syndrome between 1 to12 yrs.
2. New and old cases which include relapses, SDNS, SRNS and on remission.
Exclusion criteria:
1. Children with family history of hyperlipidemia
2. Children with previous history of thyroid dysfunction
3. Children with other causes of hypoproteinemia like liver disease and malnutrition.
4. Age less than 1yr and more than 12yr
ETHICAL APPROVAL AND INFORMED CONSENT:
Hospital ethics committee approved the study protocol. Informed consent was obtained from the parents of the study subjects after explaining to them in detail the nature of the study.
Methodology:
After history taking and clinical examination, blood samples were collected from the patients for lipid profile and thyroid function. Enzymatic method used for measurement of serum cholesterol and VLDL,enzymatic calorimetric method used for measurement of LDL and triglycerides,phosphotungstate method for HDL and photometric method used for measuring serum albumin.T3,T4and TSH level measured by ELIZA (Enzyme Linked Immunosorbent Assay).
Statistical Analysis:
The data collected from patients were entered in Microsoft excel sheet and analysed. For continuous variables mean and standard deviation were calculated. To compare the statistically significant association between the means of the two group student t test was used. Categorical variables were expressed as percentages or proportions. For categorical variable chi square test was used. P value of < .05considered as statistically significant.
NORMAL VALUES:
LIPID PROFILE
Desirable mg/dl Borderline mg/dl Elevated mg/dl
Cholesterol <170 170-199 >200
LDL <110 110-129 >130
HDL >45 35-45 <35
THYROID FUNCTION TEST
T3
:
0.5-2 ng/ml
T4 :
4.4-11.6microgr/dl
TSH :
0.5 -7.0 iu/ml
Nephrotic syndrome
The diagnosis of nephrotic syndrome requires 1. Edema
2. Massive proteinuria (> 40 mg/m2/h or Protein:creatinine ratio >2.0)
3. Hypoalbuminemia (<2.5 g/dl) 4. Hyperlipidemia10,11
Remission of nephrotic syndrome
Remission is defined as marked reduction in proteinuria (to < 4 mg/m2/h, or urine albumin dipstick of nil to trace for3 consecutive days) in
association with disapperance of previous edema.
Relapse of nephrotic syndrome
Relapse of nephrotic syndrome characterized by recurrence of massive proteinuria (> 40 mg/m2/h, or urine albumin ≥ 2 + on 3 consecutive
days), with recurrence of edema.
Steroid-sensitive nephrotic syndrome
Steroid-resistant nephrotic syndrome
Those who failed to develop remission after 8 weeks of corticosteroid treatment referred to as steroid-resistant nephrotic syndrome (SRNS). Some define this state as a failure to develop remission after 4 weeks of prednisone at a dose of 60 mg/m2/day, others define it as failure to develop remission
after 4 weeks of prednisone at a dose of 60 mg/m2/day followed by 4 weeks of alternate-day prednisone at a dose of 40 mg/m2/dose, or as 4 weeks of
prednisone at a dose of 60 mg/m2/day followed by three intravenous pulses of
methylprednisolone at a dose of 1000 mg/1.73m2/dose.12These patients are at
significantly higher risk for development of complications of the disease and also for progression to chronic kidney disease (CKD) orend-stage renal disease (ESRD).
Steroid-dependent nephrotic syndrome
Some respond to initial steroid treatment by developing complete remission, but develop a relapse either while still receiving steroids, or within 2 weeks of discontinuation of treatment following a steroid taper. Such patients require continued low-dose treatment with steroids to prevent this rapid development of relapse, and are therefore referred as steroid-dependent nephrotic syndrome (SDNS).
Frequently relapsing nephrotic syndrome
are at more risk of developing complications of nephrotic syndrome, and disease progression to CKD or ESRD. Need for prolonged or more frequent steroid treatment in these group of patients, places them at more risk for steroid-induced side effects when compared with other steroid-sensitive patients.
Pathogenesis of primary nephrotic syndrome
Most important function of kidney is blood filtration by glomeruli, allowing excretion of fluid and waste products, retaining all blood cells and the majority of blood proteins within the bloodstream. Each glomerulus is made of numerous capillaries which have developed to permit ultrafiltration of the fluid that forms urine. The capillary walls composed of an inner
endothelial cell cytoplasm, with pores known as ‘fenestrations’, the
glomerular basement membrane (GBM), and outer glomerular epithelial cells
(podocytes) whose distal ‘foot’ processes are attached to the GBM. Under
The podocyte
podocytes in glomerular function in renal disease and pathogenesis is evolving. Many morphologic changes been reported in podocytes in nephrotic syndrome. These changes include cell swelling; retraction and effacement of the podocyte foot processes, leading to formation of a diffuse cytoplasmic sheet along the GBM; vacuole formation; occurrence of occluding junctions with displacement of slit diaphragms; and detachment of podocyte from the GBM. These structural changes in podocytes, associated with detachment from the underlying GBM,will result in proteinuria.
1. Minimal change nephrotic syndrome
Many reports have told qualitative and quantitative abnormalities in both the humoral and cellular immune systems in MCNS. Low levels of immunoglobulin G (IgG) and highlevels of IgM been well documented in MCNS.21 Reduced levels of factor B and factor D also noted during
relapses.22Eventhough these observations indicate an abnormality of B-cell
function, in MCNS, their role in the pathogenesis was largely unknown.22Abnormalities in the cell-mediated immune system long been
implicated in the pathogenesis of MCNS. In 1974, Shalhoub first proposed that idiopathic nephrotic syndrome might be due to a disorder of T-lymphocyte function.23 His hypothesis suggest that a clonal T-cell population
• Disease responds to corticosteroids and alkylating agents
o Infections such as measles, which are known to depress cell-mediated immunity, often induced remission
• MCNS been associated with Hodgkin disease.
A potentially important role of the cell-mediated immune system in nephrotic syndrome was further supported by depressed cell-mediate immunity during relapses of MCNS24, alterations in T-cell subsets during
relapses and more cell surface expression of interleukin-2 (IL-2) receptor on T cells, reflects T-cell activation. Alterations in numerous cytokines of T lymphocyte origin been reported in nephrotic syndrome. These abnormalities in cytokine expression include tumor necrosis factor α (TNF-α), vascular
permeability growth factor (VPGF), 1, 2, 4, 8, 10, 12, IL-13, and IL-1825,26.
Soluble immune response suppressor (SIRS) is another T-cell-derived cytokine isolated from the urine and serum of patients with SSNS.27,28
Although capable of suppressing both T-cell and B-cell function, it was not found to be present in the urine of patients with SRNS, and was unable to induce proteinuria following injection into animals. Evidence suggestive of T-cell involvement in MCNS has been recently described. Screening of genes express in peripheral blood mononuclear cells from patients during relapse revealed high levels of NF-κB DNA-binding activity, and reduced expression
of IκBα protein, and these abnormalities reversed during remission29 These
during MCNS, but do not clarify whether the changes were the cause or result of relapse of disease. Evidence had shown that corticosteroids may act directly on the podocytes, rather than through modulation of the immune system. Treatment of cultured podocytes with dexamethasone in
concentrations similar to that achieved in the patient’s serum during treatment
for nephrotic syndrome revealed a dramatic protection against, and enhanced recovery, from podocyte injury. Thesefindings shed an important light on the pathogenesis of MCNS, and need to further investigation.
Focal segmental glomerulosclerosis
FSGS occur either as a primary or a secondary disease associated with reflux nephropathy, hereditary nephropathies, sickle cell disease, HIV nephropathy, obesity, and nephropathy associated with heroin use. The pathogenesis of primary FSGS consist of
• podocyte injury
• genetic mutations
• soluble mediators
• Hemodynamic factors.
Podocyte injury
podocyturia31,32. Since podocytes are believes to be terminally differentiated
cells and are unable to replicate, their detachment from the GBM expose the GBM directly to the urinary space, where it adhere to the parietal epithelial cell of Bowman capsule led to the formation of a synechia, the earliest
‘committed’ lesion in the evolution of FSGS. Once synechiae formed, two
Genetic mutations
Mutations in numerous podocyte and podocyte-related proteins responsible for FSGS.
• The slit diaphragm protein nephrin (encoded by NPHS1), responsible development of congenital nephrotic syndrome of the Finnish type (CNF) in infants.35
• The podocyte protein podocin (encoded by NPHS2), will cause FSGS in young children.36
• The Wilms’ tumor suppressor gene WT1, will cause Denys–Drash syndrome in children.37,38
• The actin bundling protein α-actinin (encoded byαACTN4), producing
FSGS in adults.39
Soluble mediators
Soluble mediators play an important roles in some forms of FSGS.
Evidence includes:
• Isolation of a 30–50 kDa ‘FSGS factor’ from the serum of patients with FSGS which able to induce proteinuriafollowing injection into rats.40,41
Hemodynamic factors
Glomerular hypertension associated with development of FSGS. The mechanism by which glomerular hypertension leads to FSGS dueto the capillary stretch and mechanical stress on the podocytes induce by increased Trans glomerular pressure.43,44 Repeated or severe stress to podocytes will
lead to their detachment from the GBM and initiate the sequence of events that resut in the development of FSGS.
Pathophysiology of edema
Edema the most common clinical manifestation of nephrotic syndrome in children. Edema, due to total body water and sodium excess, the result of fluid accumulation in the interstitial space. The pathogenesis of edema in nephrotic syndrome been is due to hypoalbuminemia and an impaired sodium and water excretion.
Hypoalbuminemia
The pathogenesis of edema in nephrotic syndrome and the role of hypoalbuminemia explained by the Starling equation, which governs the movement of fluid in the peripheral tissue capillaries:
Net filtration = LpS (Δhydraulic pressure−Δoncotic pressure)
= LpS [(Pcap− Pif)− s (πcap−πif)] where Lp was the capillary permeability, S is
the surface area of the capillary wall, Pcap is the hydrostatic pressure of the
capillary, Pifis the interstitial fluid hydrostatic pressure, πcapwas the capillary
oncotic pressure and πif is the interstitial fluid oncotic pressure, s is the
complete impermeability). Formation of edema prevented in healthy individuals by a balance between forces that favor transcapillary passage of plasma fluid (capillary hydrostatic pressure – Pcap) and those opposing it
(capillary oncotic pressure – πcap). This favors the passage of fluid from
capillary lumen into the interstitial tissue, which wasreturned into the systemic circulation by the lymphatics. Hypoalbuminemia in nephrotic syndrome lead to low capillary oncotic pressure (πcap), and the capillary
hydrostatic pressure (Pcap) remains unopposed. This change in Starling forces
in the peripheral tissue capillary beds promotes development of edema.
Sodium and water excretion
Patients with nephrotic syndrome had an excess of total body sodium and water, there was major controversy regarding mechanisms involved in sodium and water retention, as well as the state of their intravascular volume.
The ‘under fill hypothesis’ proposes the presence of a decreased effective
circulating blood volume in nephrotic syndrome, whereas the ‘overfill
hypothesis’ proposed the existence of an expanded intravascular volume. Under fill hypothesis pointed the presence of clinical edema, urinary sodium excretion was low in nephrotic patients. It was told that low circulating intravascular volume stimulates the renin–angiotensin–aldosterone system (RAAS) will results in renal sodium retention under the influence of aldosterone. Inhibition of atrial natriuretic peptide (ANP) will also contributes to low urinary sodium excretion in these patients. 45Urinary
albumin infusion, or by head-out of water immersion, has been cited as the evidence pointing to sodium and water retention being the consequence of poor intravascular volume. This mechanism may be operative in patients withMCNS. The overfill hypothesis told that patients with nephrotic syndrome had inhibition of the RAAS associated with an increased circulatory blood volume, due to more sodium reabsorption from the distal convoluted tubule. This distal tubular sodium reabsorption due secondary to ANP resistance. Sodium excretion is not affected by albumin infusion or head-out of water immersion. Because the management of edema in children with nephrotic syndrome will differ if patients are deemed volume expanded as opposed to volume-contracted, establishing whether the patient is
‘overfilled’ versus ‘underfilled’ is clinically relevant. One group had told by measuring the fractional excretion of sodium (FENa) as well as the relative urinary potassium excretion [UK/(UK+UNa)]. Nephrotic patients with low FENa (< 1%) and high [UK/(UK+UNa)] (>60%) would fit the profile of a patient with a low intravascular volume, and these urinary tests had been shown to correlate with raised plasma renin, aldosterone, norepinephrine, and vasopressin levels.46
Clinical approach
syndrome. Proteinuria could be quantified by obtaining urine protein/creatinine ratio in a spot urine sample, and hypoalbuminemia and hypercholesterolemia must be confirmed.
Laboratory evaluation
The laboratory evaluation of children with nephrotic syndrome consist of confirming hypoalbuminemia, hypercholesterolemia, and assessment of renal function. Mild azotemia is not uncommon in childhood nephrotic syndrome. In the ISKDC study, they observed that serum creatinine elevation were noted in 32% of cases with MCNS, with 41% of children with FSGS and 50% of those with MPGN.47Macroscopic hematuria was un common in
of treatment for childhood nephrotic syndrome, Mantoux test to screen for previously undiagnosed tuberculosis is also recommended before institution of therapy. Renal ultrasound not needed in the evaluation of childhood nephrotic syndrome. However, in the setting of a child with nephrotic syndrome who presented with gross hematuria, a renal ultrasound should be done to look for the possible development of renal vein thrombosis.
Consideration of renal biopsy
In the ISKDC studies in the early 1970s, a renal biopsy was performed before starting of treatment, but the guidelines for a renal biopsy become less rigid since then. In current practice, some pediatric nephrologists took the decision to biopsy a child with nephrotic syndrome must be age-based, with those more than 10 years can undergoing a biopsy because of the higher risk of finding a histologic lesion other than MCNS.
Some others suggested that a need for renal biopsy in only those with suspicion of underlying glomerulonephritis. Most pediatric nephrologists consider doing a diagnostic renal biopsy in all cases with SRNS. An additional indication for a biopsy is to find ‘a baseline’ histologic picture
Primary and secondary causes of nephritic syndrome in children
Primary causes
-Minimal change nephrotic syndrome (MCNS) -Focal segmental glomerulosclerosis (FSGS) -Mesangial proliferative glomerulonephritis
- Membranoproliferativeglomerulonephritis(MPGN) (mesangiocapillary glomerulonephritis)
• MPGN type I
• MPGN type II (dense deposit disease)
• MPGN type III
-Membranous nephropathy (MN) Secondary causes
Systemic diseases associated with nephrotic syndrome:
• Henoch–Schönlein purpura
• Systemic lupus erythematosus
• Diabetes mellitus
• Sarcoidosis
Infectious diseases associated with NS:
• Hepatitis B (usually associated with MN, rarely MPGN)
• Hepatitis C (usually associated with MPGN)
Hematology/oncology:
• Leukemia
• Lymphoma (Hodgkin disease usually MCNS) Sickle cell anemia
Drugs:
• Non-steroidal anti-inflammatory drugs
• Gold
• Penicillamine
• Captopril
Other:
• Bee stings (MCNS)
• Food allergies
• Obesity (usually with FSGS)
• Pregnancy–toxemia
HISTOLOGICAL CLASSIFICATION
The histologic lesions associated with childhood nephrotic syndrome divided into glomerulopathies that occur in isolation, primary glomerulopathies, and those occur in associated with systemic diseases, secondary glomerulopathies.
Primary glomerulopathies
Minimal change nephrotic syndrome
The old definition of minimal change nephrotic syndrome, also known as nil disease, is a renal biopsy specimen had no obvious glomerular or tubular abnormalities on light microscopy. This lesion, as defined by the ISKDC,permits a slight increase in mesangial matrix or cellularity, an occasional sclerosed glomerulus, or slight tubular atrophy, although the presence of a segmental scar or evidence of glomerularcollapse on light microscopy will exclude patients from this category.48 Important to note that
the some lesion of MCNS may precede the subsequent development of the sclerotic lesion of focal segmental glomerulosclerosis (FSGS). Minimal change disease is the most common histologic type seen in children with nephrotic syndrome who undergone renal biopsies at the outset of diagnosis. In the ISKDC study, out 127 children diagnosed as nephrotic syndrome who underwent a renal biopsy 77%had the histopathologic criteria of MCNS.49
untreated child with nephrotic syndrome was one of a young child, mostly male, with low likelihood of hypertension and hematuria. In most studies, nearly 80% of children with biopsy-proven MCNS were less than 6 years of age, 60% were male, 13–23% had microscopic hematuria, and 14% had systolic and 21% have diastolic hypertension.50 Whiteet al noted that due to
the more incidence of MCNS (77%), a child with new-onset nephrotic syndrome, even if associated hematuria and/or hypertension, was more likely to have MCNS than any other histologic lesion. They told steroid-responsiveness in 97% of patients, with relapse rates was as high as 94% in steroid-sensitive cases.51 Nowadays relapse rates are generally lower
compared to those early reports, due to the longer durations of initial steroid treatments course used.
Focal segmental glomerulosclerosis
.
Renal biopsy in a case of FSGS showing normal and sclerotic segment of glomeruli.
distribution). Furthermore, the glomerular scars when present are only seen in some portion of the involved glomeruli (segmental distribution) . In older reports, the incidence of FSGS among children with untreated nephrotic syndrome who underwent a renal biopsy ranged from 5 to 9%.among these 50% of these patients were less than 6 years of age, 70% were male, microscopic hematuria and systolic hypertension were seen in nearly 50% of these patients, and 33% exhibited diastolic hypertension. High occurrence of resistance to treatment with steroids is known to be associated with the diagnosis of FSGS. Classifying a glomerulopathy as FSGS appears to have some notable restrictions. McAdam et al done a retrospective study on analysis of 134 children with FSGS who presented with nephrotic syndrome or asymptomatic proteinuria. They told that the focal sclerosis lesion can be very nonspecific, and the appearance of the non-sclerotic glomeruli may indicate more regarding the disease prognosis. In their study, those children with FSGS and normal-appearing remaining glomeruli (defined as ‘primary FSGS’) present with either asymptomatic proteinuria or nephrotic syndrome. Those children with FSGS and generalized podocyte effacement in the non-sclerotic glomeruli were grouped in this study as ‘minimal change’ with
FSGS; whereas those with FSGS and mesangial proliferative changes in the non-sclerotic glomeruli were classified as ‘mesangial proliferation’ with
sclerosis affecting the entire glomerulus, rather than a segmental distribution as seen in FSGS. This lesion more benign than FSGS, if it occurs by itself and without associated interstitial changes.52,53 The collapsing variant of
FSGS, or collapsing glomerulopathy, was another glomerulopathy seen in children with nephrotic syndrome. Although the pathogenesis is unknown, this lesion is characterized by marked podocyte hyperplasia with compression of the glomerular tuft, often epithelial crescent formation. The FSGS
Working Group’s definition of the collapsing variant of FSGS needs at least 1 glomerulus to demonstrate segmental or global collapse and overlying podocyte hypertrophy and hyperplasia.54Collapsing glomerulopathy has been
associated in patients with HIV infection,55parvovirus B19 infection,56,57and also as an idiopathic disorder. Its prognosis in adults was worse than that of FSGS.58 Finally, FSGS can be either a primary or a secondary disorder. The secondary type of FSGS seen in reflux nephropathy, glycogen storage disease, sickle cell disease, and cyanotic congenital heart disease.59-62 This
lesion will also be seen in children with nephrotic-range proteinuria in the absence of nephrotic syndrome. Those patients with FSGS and absence of nephrotic syndrome tend to have a better prognosis compared to other types63.
Mesangial proliferative glomerulonephritis
but glomerular crescents and adhesions may sometimes be asociated. Immunofluorescence was usually negative, but sometimes show mesangial IgM deposition. The incidence of biopsy-proven MesPGN in untreated children with nephrotic syndrome was approximately 2–5%.64 Clinical
features of children with nephrotic syndrome and MesPGN were microscopic hematuria (100%) and hypertension (25%)65.Garin et al noted in a cohort of 23 patients with MesPGN 70% were steroid resistant.66
Membranoproliferative glomerulonephritis
Another less common histologic lesion associated with the childhood nephrotic syndrome was MPGN. Three types of MPGN have been described based on using immunofluorescence and electron microscopic observations, serology, and by their differing effects on the complement pathway.67,68On
light microscopy, all forms were characterized by more mesangial matrix and Electron microscopy of renal
biopsy in MPGN
glomeruli. Apparent duplication (railroad or tram track appearance) of the GBM as a result of mesangial interposition is also seen. Immunofluorescence staining is positive for C3 and IgG in MPGN types I and III, and C3 alone are seen in dense deposit disease (MPGN type II). Depend on the nature and location of the electron-dense deposits, MPGN is classified into three subtypes. MPGN type 1 Sub endothelial deposits,MPGN type II intramembranous electron-dense deposits characterize dense deposit disease , MPGN type III trans membranous (sub endothelial, intramembranous, andsub epithelial), par mesangial, and mesangial deposits have been described . MPGN in old reports accounted for 2–8% of children with new-onset nephrpotic syndrome. Characteristic clinical features of these children were older age at presentation, more in female, systolic hypertension in approximately 50% and diastolic hypertension in 25%. Nearly 60% had microscopic hematuria at onset, 75% had hlow C3, and 50% had azotemia. Often, the clinical presentation was one of nephritic syndrome (macroscopic hematuria, hypertension, and azotemia) in addition tofeatures nephrotic syndrome. These patients were poorly responds to corticosteroids.69 Three
associated with MPGN type I acts onthe classical complement pathway and results in low C3 and C4, with some degree of fall in C5. The antibody associated with type II stabilizes the C3 convertase (C3b, Bb), resulting in chronic activation of the alternative complement pathway and very low C3 levels, with normal C4 and C5 levels. The nephritogenic autoantibody associated with type III acts on the terminal pathway, lead to low C3 and C5 levels, with normal C4 levels.70MPGN has also been associated with hepatitis
B and hepatitis but these are less common in the pediatric age group. It may be associated with chronic bacterial infections, such as ventriculoatrial shunt infection (shunt nephritis) and deep-seated chronic abscesses. Circulating immune complexes were involved in the pathogenesis of MPGN types I and III, and had been seen in patients with shunt nephritis, as well as chronic hepatitis. The median age of onset was 7 years, with females being 4 times more affected than males.71The histologic subtype of MPGN associated with
acquired partial lipodystrophy was mostly dense deposit disease (MPGN type II) compared to other types.72
Membranous nephropathy
Primary membranous nephropathy or membranous glomerulonephritis (MGN) was the least common histologic lesion seen in childhood nephrotic syndrome. This type was more commonly seen in adults as a cause of nephrotic syndrome. Heymann nephritis was a rat model of human membranous glomerulonephritis. Antibodies directed against megalin, a membrane glycoprotein located at the base of the microvilli in the proximal tubular brush border and along the sides and bases of the podocyte foot processes, resulting in sub epithelial immune deposits .73,74 The pathogenesis
of MGN in humans was not known, most probably to an autoimmune disorder mediated by immune complexes . The antibody responsible for this lesion was directed against an antigen within the kidney, leading to formation of sub epithelial deposits. The renal biopsy features of MGN on light microscopy demonstrate mostly normal glomeruli with diffuse thickening of the glomerular capillary walls.
No Mesangial proliferation which is diagnostic. Basement membrane stain
(silver stain) shows typical ‘spikes’ on the GBM. Sub epithelialand
infection.75 In children with hepatitis B-associated MGN,serologic evidence
of Hep B surface antigen (HepBsAg)was reported in 100%. Histologically, HepBeAg will be identified in all biopsies of hepatitisB-associated MGN, whereas HepBsAg was not detected consistently. Other common secondary causes of MGN include SLEand drugs such as penicillamine and gold.76
Secondary glomerulopathies
Glomerulonephritis associated with an underlying systemic disorder can lead to childhood nephrotic syndrome. These lesions were known as secondary glomerulopathies. The histopathology and pathogenesis of the secondary glomerulopathiesare variable, depending on the primary cause.
Systemic lupus erythematosus
Systemic lupus erythematosus, a multisystem autoimmune disorder, had been reported to be associated with kidney involvement in approximately 66% of newly diagnosed pediatric cases.77 The glomerulonephritis in SLE
can manifest as asymptomatic haematuria and/or proteinuria, acute glomerulonephritis, or nephrotic syndrome.78 It had been told that half of
with microscopic or gross hematuria, azotemia, and hypertension) was common in SLE nephritis, particularly in the diffuse proliferative disease.
Henoch–Schönlein purpura
Henoch–Schönlein purpura (HSP) is a vasculitis of the small vessel associated with renal involvement. The extra renal manifestations of HSP include a purpuric rash involving the buttocks and lower extremities, joint pain, or abdominal pain. The renal manifestations include microscopic hematuria, acute glomerulonephritis, with or without renal failure, and in some with nephrotic syndrome. Renal biopsies shows an IgA-associated mesangial glomerulonephritis..
Diabetes mellitus
Patients with diabetes mellitus were more risk for nephropathy. These patients can have other glomerular diseases that can accompany with diabetic nephropathy. Diabetic nephropathy typically occurs in patients with at least 10 years duration of diabetes mellitus, associated with poor glycemic control. Diabetic nephropathy correlate well with the presence of diabetic retinopathy.79 Steroid-sensitive MCNS, and immune complex
glomerulonephritis, had been associated with insulin-dependent(type I) diabetes.
Sarcoidosis
renal disease (granulomatous interstitial nephritis) may be the only manifestation of sarcoidosis– known as renal limited sarcoidosis.
Human immunodeficiency virus infection
Human immunodeficiency virus (HIV) infection can have nephrotic syndrome in both children and adults.81The histologic lesions associated with
HIV disease were range from mesangial proliferation to that of FSGS. HIV cases with FSGS often occur in the setting of nephrotic syndrome and had a worse prognosis. Another glomerular lesion associated with HIV nephropathy was collapsing glomerulopathy. Electron microscopy characteristically reveals tubuloreticular inclusions, which were not specific for HIV infection but diagnostic. Immunecomplex-mediated glomerulonephritis similar to SLE also been associated.
Hepatitis B
Hepatitis B nephrotic syndrome associated with either MGN or MPGN. The clinical picture of children with these were histologic lesions that include nephrotic syndrome, acute glomerulonephritis, or a combination of both. The MPGN histologic lesion appears to have a more prevalence in the pediatric age group.82.
Hepatitis C
had proven very good effect for hepatitis C-associated glomerulopathy, Ribavirin monotherapy had also used successful in inducing remission in a patient with hepatitis C-associated membranous nephropathy.83
Viral causes of collapsing glomerulopathy
HIV infection should be strongly suspected in a patients with collapsing glomerulopathy. Other viral infections have been associated with collapsing glomerulopathy were parvovirus B19, hepatitis C, and CMV infection.
Leukemia
Acute lymphoblastic leukemia (ALL) has also been associated with the childhood nephrotic syndrome. A few cases of ALL had been reported following treatment for nephrotic syndrome.MCNS had also been diagnosed following hematopoietic stem cell transplant for acute myelogenous leukemia.84
Lymphoma
Hodgkin lymphoma had been associated with nephritic syndrome, usually MCNS on renal biopsy. Remission of nephrotic syndrome in these cases usually the result oftreatment of the Hodgkin disease, in both adults and children.85
Non-steroidal anti-inflammatory drugs
to cause nephrotic syndrome, with renal biopsy was shows minimal change disease and interstitial nephritis.86
Angiotensin-converting enzyme inhibitors
Although angiotensin-converting enzyme inhibitors (ACEIs) were commonly used for their anti proteinuric effects in patients with nephrotic syndrome and refractory proteinuria, a number of reports had linked nephrotic syndrome to use of captopril in patients with hypertension. MGN was the usual histologic lesion in captopril-associated nephrotic syndrome.87
Miscellaneous drugs
Rheumatoid arthritis may require treatment of either gold or
penicillamine. Both of these drugs had been associated with glomerulopathies and proteinuria. MGN comprises accounts for 75% of the associated renal lesions. Most cases havd been reported in adults, but gold nephropathy had also been reported in a cases of juvenile rheumatoid arthritis of 2-year-old child .88
Sickle cell disease
Obesity
Obesity, defined as a body mass index (BMI) > 30 kg/m2, has been associated with a glomerulopathy that was FSGS associated with large glomeruli, or glomerulomegaly. This condition may present with either nephrotic syndrome, or isolated proteinuria. Adults with obesity-related glomerulopathy had been showed to have a slower progression of their renal disease compared with primary FSGS. Obesity-related glomerulopathy in adolescents associated marked proteinuria without nephrotic syndrome.90
Bee stings
Although rare, bee stings had been associated with nephrotic syndrome. Tasic reported a young child who developed SSNS following a bee sting, and the patient remained remission for 13 years of follow-up. Some others had reported patients with a known case of nephrotic syndrome on remission who relapses following a bee sting.91
Food allergies
Treatment
Symptomatic Treatment
Diet
Dietary therapy consist of more protein intake of around 130–140 % of the recommended daily allowance according to age. Salt restriction was advised for the prevention and the treatment of edema. A very low salt diet was indicated only in cases of massive edema. Moderate to severe hyponatremia (plasma sodium concentration less than 125meq/l) needs restriction of fluids. Diet low in saturated fat is recommended. Carbohydrates should be given preferably as starch or dextrin-maltose, sucrose to be avoided, which increases lipid abnormalities.
Hypovolemia
Hypovolemia occurs as a result of loss of protein and is sometimes complicated by the use of diuretics. This require emergency treatment by rapid infusion of plasma(20 ml/kg) or Human albumin 20%(1 g/kg) administrated carefully by monitoring of heart rate, respiratory rate, and blood pressure.
Diuretics
patients had developed respiratory distress with congestive heart failure. Refractory edema with massive effusions may require drainage of ascites and/or pleural effusions.
Thromboembolic complications
Antihypertensive Drugs
Hypertension to be carefully controlled, using either a β-blocker or a calcium channel blocker during acute episodes. In cases of permanent hypertension, an ACE inhibitor is preferred.
INFECTION AND IMMUNISATION
oral penicillin is often used in patients during the initial treatment with corticosteroids for prophylaxis against pneumococci . Pneumococcal vaccine was effective even in children receiving high doses of steroids, and not associated with an increased risk of relapse. In cases of suspected peritonitis, antibiotics against both S. pneumoniæ and gram-negative organisms were started after peritoneal sampling.Chicken pox is a serious disease in patients receiving immunosuppressive treatment or daily corticosteroids.. In cases of exposure, early acyclovir should be started. Varicella vaccination is safe and effective if the child was in remission (or) even if he/she is on low-dose alternate-day steroids [151, 152].
Hyperlipidemia
Miscellaneous
Calcium metabolism affected ,because of the urinary loss of 25-hydroxycholecalciferol and its carrier protein. Preventive treatment with vitamin D supplements can be useful, but not completely prevent bone loss Thyroxine sublimentation indicated only in patients with documented hypothyroidism.
Specific Treatment
Steroid therapy was used in all cases of nephrotic syndrome even in patients with FSGS. The majority of patients are steroid responsive . Steroid responders may develop relapse, but the majority of them responding to steroids . Only 1–3 % of patients initially steroid-sensitivebut later become steroid-resistant and are defined as “late nonresponders” [
Initial Treatment
remission in small number of patients who responded quickly to the same dosage of prednisone. The intestinal absorption of prednisolone is less compared to that of prednisone, and this will explain a lesser efficacy in some children. The ISKDC regimen consists of prednisone, 60 mg/m2/day with a
maximum of 80 mg/day, in divided doses for 4 weeks followed by 40 mg/m2/day with a maximum of 60 mg/day in divided doses, on three consecutive days per week for 4 weeks. According to the International Study of Kidney Disease in Children, approximately 90 % of responders go for remission within 4 weeks after starting steroids, whereas < 10 % go into remission after 2–4 more weeks of a daily regimen. A few more patients go into remission after 8–12 weeks of daily steroids , but prolongation of daily steroid treatment beyond 4 or 5 weeks will increases the risk of side effects. An alternative for patients who not attain remission after 4 weeks is to administer 3 to 4 pulses of methylprednisolone (1 g/1.73 m2). This additional regimen associated with
lesser side effects than prolongation of daily high-dose steroids and producing remission more rapidly in the few patients who would have entered into remission during the second month of daily therapy .A working committee recently showed the following KDIGO guidelines . Initial prednisone therapy consists of 60 mg/m2 or 2 mg/kg administered as a single daily dose for 4–6 weeks (maximum dose of 60 mg/day), followed by alternate-day prednisone of 40 mg/m2 or 1.5 mg/kg (maximum dose of 40 mg/day) continued for 2–5
longer initial course of 6 weeks of daily prednisone at a dose of 60 mg/m2/day
followed by 6 weeks alternate-day prednisone at a dose of 40 mg/m2/ day . The
further relapse rate within 1yr following discontinuation of therapy was lower with the prolonged course of therapy compared to the standard course (36 % vs. 61 %). This study showed that extending initial prednisolone treatment from 3 to 6months without increasing cumulative dose did not benefit clinical outcome. Therefore, prolonged treatment regimens that decreases relapses mostly due to more cumulative dose rather than treatment duration.Another randomized control trial from India showed that extending the initial prednisolone treatment from 3 to 6 months will not influence the course of the disease . However, a study showed that an alternate-day regimen over a year will not reduce the rate of relapse compared to a 5-month alternate-day regimen . Although the studies were not aimed to analyze the side effects of glucocorticoids, the authors did not explain increased toxicity with longer duration of treatment. A slow tapering dose of steroid to avoid adrenal suppression responsible in maintain long-term remission as a study showed that moderate to severe adrenal suppression was associated with more chance for relapse . Another study also showed that adrenocortical suppression will increases the risk of relapse in children onlong-term alternate-day steroid therapy .
Treatment of Relapse
produce spontaneous remission, avoids the need for treatment with steroids. Prednisolone is administered at a dose of 2 mg/kg/day (single or divided doses) until remission. Followed by prednisolone is given in a single morning dose of 1.5 mg/kg on alternate days for 4 weeks, and then discontinued. The usual duration of treatment for relapse cases 5-6 weeks. In case the patient is not attain remission despite two weeks treatment with daily prednisolone, the treatment will be continued for two more weeks.If thePatients showing no
remission despite 4 weeks ‘treatment with daily prednisolone are labeled as
steroid resistant nephrotic syndrome.
Infrequent Relapses
Patients with infrequent relapses are managed using the regimen mentioned above for each relapse. Theses children were at a low risk for developing steroid toxicity.
Frequent Relapses and Steroid Dependence
Patients having frequent relapses or steroid dependence require prolonged courses of prednisolone will develop steroid toxicity, consist of cushingoid features (obesity, hirsutism, striae), hypertension, impaired glucose tolerance, posterior sub capsular cataract, emotional problems and growth retardation. Alternative regimens can be used in such patients are listed below:
i. Long-term alternate day prednisolone:
effective in maintaining a remission or reducing the number of relapses. Side effects were less and not interfere with growth. Breakthrough relapses during low dose maintainance therapy were treated with standard treatment of relapse. If the prednisolone threshold, to maintain remission, is more or if features of steroid toxicity develops additional use of the following immunomodulators were recommended.
ii. Levamisole:
Levamisole is useful in reducing relapse rates in patients with frequent relapses and steroid dependent nephrotic syndrome. It is given at a dose of2 mg/kg on alternate days for 12-24 months combine with
prednisolone at a dose of 1.5 mg/kg on alternate days is given for 2-4 weeks; its dose is gradually tappered by 0.25 mg/kg every 4 weeks to a maintenance dose of 0.5 mg/kg that is continued for 6 or more months. Some times, it may be possible to discontinue treatment with corticosteroids. The side effect of levamisole are leucopenia, flu-like symptoms, liver toxicity, seizures and skin rash are rare.
iii. Cyclophosphamide:
below4000/mm3. More fluid intake and frequent urination will help to prevent hemorrhagic cystitis. Other side effects are alopecia, nausea and vomiting.
iv. Calcineurin inhibitors:
Cyclosporine (CsA) causes specific and reverible Tcell suppression. The dose of CsA is 4 to 5 mg/kg per day (100-150 mg/m2 per day) and is given
for the prriod of 12-24 months. Prednisolone is combined at a dose of 1.5 mg/kg on alternate days for 2-4 weeks; its dose is gradually tapered by 0.25 mg/kg every4 weeks to a maintenance dose of 0.25-0.5 mg/kg that is continued for 6 or more months. Relapses can occur when therapy with CsA was discontinued. Side effects of therapy are hypertension, gum hypertrophy, hirsutism and nephrotoxicity; hypercholesterolemia and elevated transaminases rarely occur. Tacrolimus is an alternative agent because of lack of cosmetic side effects better used in adolescents.
v. Mycophenolate mofetil:
It is an inhibitor of purine metabolism, is found effective in reducing relapse rates in patients with frequent relapses and steroid dependent nephrotic syndrome. Main side effects are gastrointestinal discomfort and leucopenia.
INITIAL STEROID RESISTANCE
OBSERVATION AND RESULTS
[image:59.595.93.533.185.410.2]Total number of cases 40
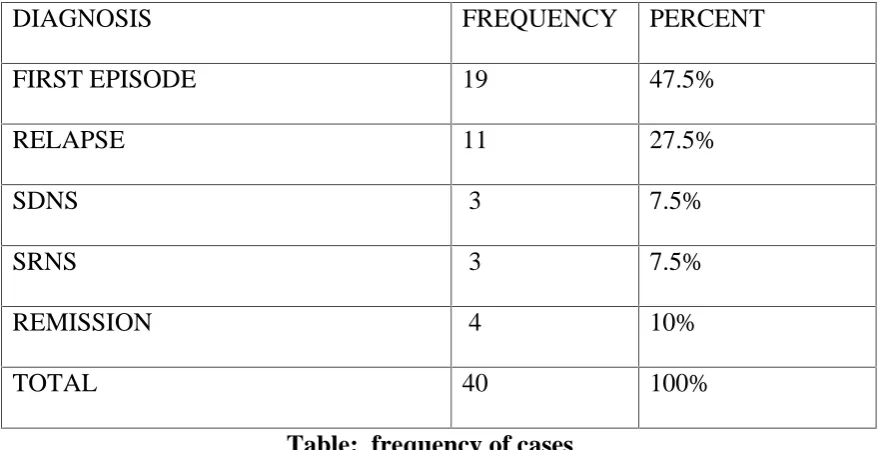
Table: frequency of cases
Among the 40 cases between 1 to 12 yrs. included in our study 19 cases were first episode (47.5%),11 cases were relapses (27.5%) which includes both frequent and infrequent relapses, 3 cases were steroid dependent nephrotic syndrome(SDNS 7.5%),3 cases were steroid resistant nephrotic syndrome(SRNS 7.5%) and 4 of them were included at the time of remission (10%).
In our study cases are diagnosed and categorized in to different types and blood samples were collected within 48 hrs of admission in our hospital and in 1 episode cases before starting steroids. Among 4 remission cases sample taken after one month of daily steroids and 3 consecutive early
DIAGNOSIS FREQUENCY PERCENT
FIRST EPISODE 19 47.5%
RELAPSE 11 27.5%
SDNS 3 7.5%
SRNS 3 7.5%
REMISSION 4 10%
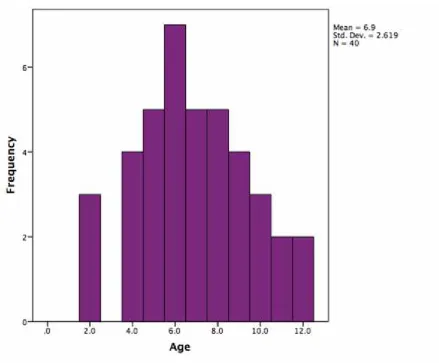
1. Age of presentation
FIGURE 1 Age of presentation
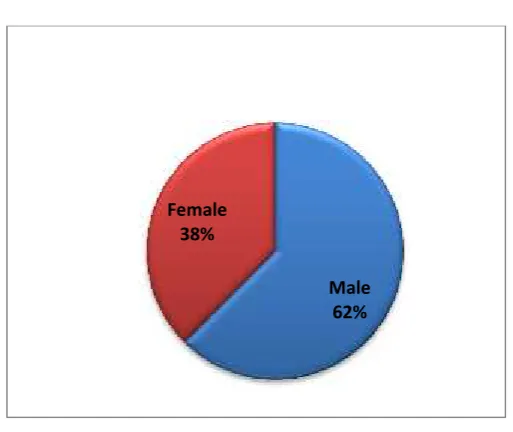
2.Gender distribution
FIGURE. 2 Gender distribution
Among the 40 cases of nephrotic syndrome in our study males (62%) affected more than females (38%).
Male 62% Female
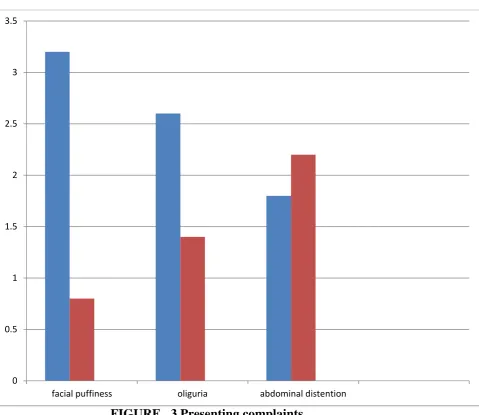
3 .Common presentation
FIGURE 3 Presenting complaints
Among 40 cases of nephrotic syndrome 32 children presented with facial puffiness (80%), 26 children presented with decreased urine output (65%) and 22 cases with abdominal distention (45%). In our study most common presenting complaint is facial puffiness.
0 0.5 1 1.5 2 2.5 3 3.5
4.Distribution of various parameters
N Minimum Maximum Mean Std. Deviation
Age 40 2.0 12.0 6.900 2.6195
Protein 40 3.4 6.6 4.615 .7560
Albumin 40 1.2 4.0 2.212 .5694
Cholesterol 40 109.0 657.0 344.300 117.4793
TG 40 101.0 775.0 304.025 161.2228
LDL 40 52.0 476.0 234.650 88.6094
HDL 40 30.0 81.0 46.07 13.8944
VLDL 40 20.0 155.0 61.625 32.0134
T3 40 .5 1.7 .923 .3190
T4 40 3.4 11.0 6.105 1.9104
TSH 40 .80 8.24 4.2925 1.88614
TABLE 1 distribution of age, serumalbumin, lipid and thyroid
profile in nephrotic syndrome.
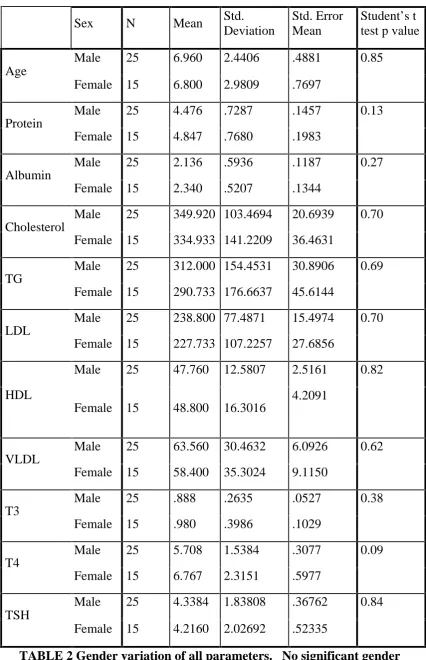
TABLE 2 Gender variation of all parameters. No significant gender
variation of all parameters. p value >0.05 insignificant. 5.Gender variation of all parameters
Sex N Mean Std. Deviation
Std. Error Mean
Student’s t
test p value
Age
Male 25 6.960 2.4406 .4881 0.85 Female 15 6.800 2.9809 .7697
Protein
Male 25 4.476 .7287 .1457 0.13 Female 15 4.847 .7680 .1983
Albumin
Male 25 2.136 .5936 .1187 0.27 Female 15 2.340 .5207 .1344
Cholesterol
Male 25 349.920 103.4694 20.6939 0.70 Female 15 334.933 141.2209 36.4631
TG
Male 25 312.000 154.4531 30.8906 0.69 Female 15 290.733 176.6637 45.6144
LDL
Male 25 238.800 77.4871 15.4974 0.70 Female 15 227.733 107.2257 27.6856
HDL
Male 25 47.760 12.5807 2.5161 0.82
Female 15 48.800 16.3016
4.2091
VLDL
Male 25 63.560 30.4632 6.0926 0.62 Female 15 58.400 35.3024 9.1150
T3
Male 25 .888 .2635 .0527 0.38 Female 15 .980 .3986 .1029
T4
Male 25 5.708 1.5384 .3077 0.09 Female 15 6.767 2.3151 .5977
TSH
6.Serum albumin level in all types
SERUM ALBUMIN MEAN SD
FIRST EPISODE 2.08 0.33
RELAPSE 1.96 0.29
SDNS 2.23 0.29
SRNS 2.03 0.21
[image:65.595.94.523.111.247.2]REMISSION 3.65 0.25
TABLE 3 Mean albumin level in different types of nephrotic syndrome.
FIGURE 4 Bar chart showing serum albumin level in different type of
nephrotic syndrome.
During relapse mean albumin (mean=1.96gm %) level less than that of first episode (mean=2.08gm %)and SRNS (mean2.03gm %) but the mean difference is statistically insignificant. (p value >0.05)
In SRNS mean albumin level (mean=2.03gm %) lower than that of SDNS (mean=2.23mg %) and 1 episode (mean=2.08gm %). But the difference
2.08 1.96 2.23 2.03
3.65
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50
[image:65.595.103.467.289.506.2]statistically insignificant .In remission albumin level (mean=3.65gm %)was statistically significant from all other types (p value less than<0.05)
7.Serum cholesterol level in all types
SERUM CHOLESTEROL MEAN SD
FIRST EPISODE 348.63 83.88
RELAPSE 363.00 83.35
SDNS 290.00 67.56
SRNS 543.00 182.93
[image:66.595.95.523.183.383.2]REMISSION 164.00 39.00
TABLE 4 Mean cholesterol level in different type of nephrotic syndrome.
FIGURE 5 Bar chart showing mean cholesterol level in all types of cases.
In our study compared to 1 episode (mean=348.63mg/dl) mean cholesterol level was elevated in relapse cases (mean363.00mg/dl) but the
348.63 363.00
290.00
543.00
164.00 0.00
100.00 200.00 300.00 400.00 500.00 600.00 700.00 800.00
[image:66.595.100.463.404.623.2]SDNS (mean=290mg/dl) is less than that of 1 episode and relapse cases, but again statistically insignificant (P value >0.05).
Serum cholesterol in SRNS VS Other types
SRNS Diagnosis MD P VA
episode 1 194.37 0.012
Relapse 180.00 0.037
Sdns 253.00 0.013
Remission 379.00 0.000
TABLE 4.1 Compare the cholesterol level of SRNS with other types.
MD–Mean Difference P VA - P value.
Mean Serum cholesterol level in SRNS (mean 543mg/dl) compared to all other types very much elevated.
Mean difference between cholesterol values of SRNS with 1episode (md=194.37) and the P value 0.012. (<0.05 Significant) With relapse cases the mean difference (md=180.00) and p value was 0.037 .(<0.05 significant) Mean difference between cholesterol value of SRNS with SDNS ( md=253) and P value 0.013 (<0.05 significant).
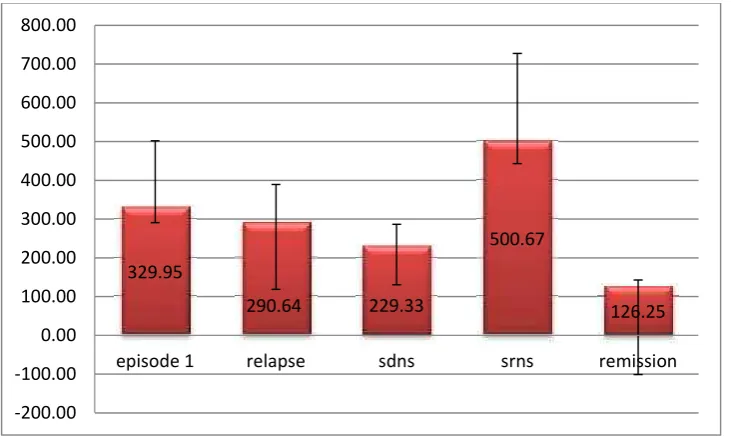
8.Serum Triglycerides level in all types
TRIGLYCERIDES MEAN SD
FIRST EPISODE 329.95 171.93
RELAPSE 290.64 98.63
SDNS 229.33 57.07
SRNS 500.67 227.01
[image:68.595.94.522.111.297.2]REMISSION 126.25 17.02
TABLE 5 Mean TRIGLYCERIDES level in all type of cases
FIGURE 6 Bar chart showing mean TRIGLYCERIDES in all cases.
Mean Triglycerides level in 1 episode (mean=329.95mg/dl) higher than relapse (mean=290.64mg/dl) and SDNS (mean=229.33mg/dl)cases. In SRNS cases TG level (mean=500.57mg/dl) highly elevated compared to 1
329.95
290.64 229.33
500.67
126.25
-200.00 -100.00 0.00 100.00 200.00 300.00 400.00 500.00 600.00 700.00 800.00
[image:68.595.100.466.373.593.2]Episode, relapse and SDNS cases but the mean difference was statistically insignificant.
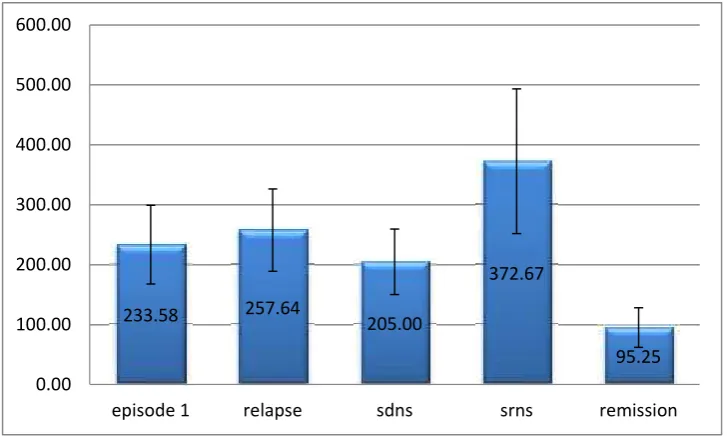
9.Serum LDL level in all type of cases
LDL MEAN SD
FIRST EPISODE 233.58 65.51
RELAPSE 257.64 68.72
SDNS 205.00 54.56
SRNS 372.67 120.70
[image:69.595.127.491.443.662.2]REMISSION 92.25 33.14
TABLE 6 Mean LDL level in all cases
FIGURE 7 Bar chart showing mean LDL level in all type of cases. 233.58 257.64 205.00
372.67
95.25 0.00
100.00 200.00 300.00 400.00 500.00 600.00
Mean serum LDL level in relapse cases (mean=257.64mg/dl) higher than 1 episode, (mean=233.58mg/dl) and SDNS (mean=205.00mg/dl) cases but statistically insignificant (p value >0.05).In SRNS cases mean serum LDL(mean=372.67mg/dl) highly elevated compared to other types but statistically significant when compared to SDNS (P value 0.048) and 1 episode cases (p value 0.023).
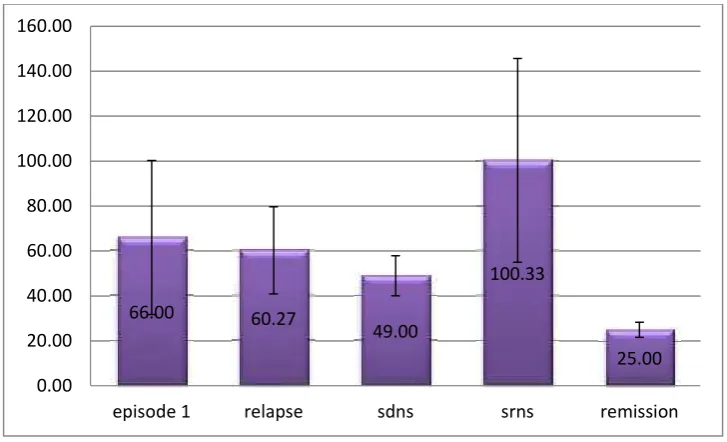
10.Serum VLDL level in all type of cases
VLDL MEAN SD
FIRST EPISODE 66.00 34.31
RELAPSE 60.27 19.37
SDNS 49.00 8.89
SRNS 100.33 45.35
REMISSION 25.00 3.37
FIGURE 8 Bar chart showing mean VLDL level in all type of cases.
In our study mean serum VLDL level in 1 episode (mean=66mg/dl) higher than relapse (mean 60.27mg/dl) andSDNS (mean=49.00mg/dl) cases but statistically insignificant (P value >0.05).
In SRNS cases VLDL level (mean= 100.33mg/dl) higher than other types but insignificant statistically. Compared to remission (mean=25mg/dl) cases
VLDL in SRNS cases statistically significantly elevated. (p value 0.016).
66.00 60.27
49.00
100.33
25.00 0.00
20.00 40.00 60.00 80.00 100.00 120.00 140.00 160.00
11.Serum HDL in all type of cases
HDL MEAN SD
FIRST EPISODE 49.05 12.18
RELAPSE 45.55 8.84
SDNS 36.00 6.0
SRNS 42.33 29.05
[image:72.595.92.522.119.349.2]REMISSION 43.75 9.60
TABLE 8 Mean HDL in all type of nephrotic syndrome.
FIGURE 9 Bar chart showing mean HDL variation in different type of
cases.
Mean serum HDL in 1 episode (mean=49.05mg/dl) higher than relapse (mean 45.55mg/dl) and SDNS (mean 36.00mg/dl) cases. Mean HDL in SRNS (mean42.33mg/dl) cases lower than 1 episode and relapse cases.
49.05 45.54
36.00 42.33 43.75
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00 80.00
[image:72.595.100.464.331.518.2]12.Serum T3 level in all type of cases
T3 MEAN SD
FIRST EPISODE 0.89 0.29
RELAPSE 0.93 0.35
SDNS 0.87 0.15
SRNS 0.83 0.32
[image:73.595.105.526.110.293.2]REMISSION 1.15 0.49
TABLE 9 Mean T3 Level in all type of cases
FIGURE 10 Bar chart showing mean variation serum T3 in all type of
nephrotic syndrome.
Serum T3 level was with in normal limit in all of the 40 cases included in our study. Mean serum T3 level in 1 episode (mean= 0.89ng/ml),relapse (mean =0.93ng/ml) cases, SDNS (mean= 0.87ng/ml) cases, SRNS cases (mean=0.83ng/ml) and in remission cases (mean 1.15ng/ml).
0.89 0.93 0.87 0.83 1.15
0.00 0.20 0.40 0.60 0.80 1.00 1.20 1.40 1.60 1.80
[image:73.595.102.462.332.552.2]13.Serum T4 level in all type of cases
T4 MEAN SD
FIRST EPISODE 5.73 1.66
RELAPSE 6.71 2.21
SDNS 5.33 0.23
SRNS 6.87 2.47
[image:74.595.95.521.113.543.2]REMISSION 6.25 2.68
TABLE 10 mean Serum T4 level in all type of cases.
FIGURE 11 bar chart showing variation of mean T4 in all type of
nephrotic syndrome.
Mean serum T4 in 1 episode (mean=5.73 microgr/dl) less than that of relapse (mean = 6.71microgr/dl) cases and higher than SDNS (mean=5.33microgr/dl) cases. Mean T4 in SRNS (mean=6.87microgr/dl) cases. Compared to all other types shows statistically insignificant elevation. (P value .0.05)
5.73 6.71 5.33 6.87 6.25
0.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00 8.00 9.00 10.00