INTERVENTIONAL PACKAGE ON KNOWLEDGE, PRACTICE
AND LABOUR OUTCOME AMONG HIGH RISK ANTENATAL
MOTHERS AT SELECTED HOSPITAL, CHENNAI.
THESIS
Submitted to
THE TAMILNADU Dr.M.G.R MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs. AMUTHA.T, M.Sc. (N)
INTERVENTIONAL PACKAGE ON KNOWLEDGE, PRACTICE
AND LABOUR OUTCOME AMONG HIGH RISK ANTENATAL
MOTHERS AT SELECTED HOSPITAL, CHENNAI.
THESIS
Submitted to
THE TAMILNADU Dr.M.G.R MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs. AMUTHA.T, M.Sc. (N)
Under the Guidance of
Dr. REVATHY VIJAYALAKSHMI, MD, Ph.D,
RESEARCH GUIDEOMAYAL ACHI COLLEGE OF NURSING
INTERVENTIONAL PACKAGE ON KNOWLEDGE, PRACTICE
AND LABOUR OUTCOME AMONG HIGH RISK ANTENATAL
MOTHERS AT SELECTED HOSPITAL, CHENNAI.
THESIS
Submitted to
THE TAMILNADU Dr.M.G.R MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs. AMUTHA. T, M.Sc (N)
Guided By
Dr. REVATHY VIJAYALAKSHMI, MD, Ph.D, RESEARCH GUIDE
OMAYAL ACHI COLLEGE OF NURSING
I hereby declare that this thesis entitled “EFFECTIVENESS OF NURSE DIRECTED HIGH RISK INTERVENTIONAL PACKAGE ON KNOWLEDGE, PRACTICE AND LABOUR OUTCOME AMONG HIGH RISK ANTENATAL MOTHERS AT SELECTED HOSPITAL, CHENNAI” is my own work carried out under the guideship Of Dr. REVATHY VIJAYALAKSHMI, MD, Ph.D, Research Guide, Omayal Achi College of Nursing which is approved by the Research Committee, The Tamil Nadu Dr.M.G.R.Medical University, Guindy, Chennai.
I further declare that to the best of my knowledge that the thesis does not contain any part of work which has been submitted for the award of any degree either in this
University or in any other University / Deemed University, without proper citation.
Mrs. AMUTHA. T RESEARCH SCHOLAR
This is to certify that this thesis entitled “EFFECTIVENESS OF NURSE
DIRECTED HIGH RISK INTERVENTIONAL PACKAGE ON
KNOWLEDGE, PRACTICE AND LABOUR OUTCOME AMONG HIGH RISK ANTENATAL MOTHERS AT SELECTED HOSPITAL, CHENNAI” submitted by Mrs.AMUTHA. T, M.Sc. (N) for the award of the Degree of Doctor of Philosophy in Nursing, is a bonafide record of research done by her during the period of study, under my supervision and guidance and that it has not formed the basis for the award of any other Degree, Diploma, Associateship, Fellowship or other similar title. I also certify that this thesis is her original independent work. I recommend that this thesis should be placed before the examiners for their consideration for the award of Ph.D. Degree in Nursing.
RESEARCH GUIDE,
Dr. REVATHY VIJAYALAKSHMI, MD, Ph D. RESEARCH GUIDE,
OMAYAL ACHI COLLEGE OF NURSING, 45, AMBATTUR ROAD,
PUZHAL, CHENNAI – 66.
This is to certify that the thesis entitled “EFFECTIVENESS OF NURSE DIRECTED HIGH RISK INTERVENTIONAL PACKAGE ON KNOWLEDGE,
PRACTICE AND LABOUR OUTCOME AMONG HIGH RISK
ANTENATAL MOTHERS AT SELECTED HOSPITAL, CHENNAI” submitted by Mrs. AMUTHA. T for the award of the Degree of Doctor of Philosophy in Nursing, is a bonafide record of research done by her during the period of study, under my supervision and Co-guidance and that it has not formed the basis for the award of any other Degree, Diploma, Associateship, Fellowship or other similar title. I also certify that this thesis is her original independent work. I recommend that this thesis should be placed before the examiners for their consideration for the award of Ph.D. Degree in Nursing.
RESEARCH CO-GUIDE, Prof. K.MANONMANI,
OMAYAL ACHI COLLEGE OF NURSING, 45, AMBATTUR ROAD,
PUZHAL, CHENNAI – 66.
I consider it my utmost privilege to offer my deep sense of gratitude to each and every individual who paved the way for making this research study a satisfying milestone in my Professional career.
I wish to express my deep sense of gratitude to the Vice Chancellor, Controller of Examination, Academic Officer, HOD’S and other officials of the Research Department of the Tamil Nadu Dr. M.G.R. Medical University, Guindy, Chennai, for giving me an opportunity to undertake my Ph.D. in Nursing at this esteemed University.
I express my sincere gratitude to Mrs. Valli Alagappan, Managing Trustee & Chairperson Governing Council, Mr.A.R. Kasiviswanathan, Member Trustee and Mrs. Seetha Subbiah, Member Trustee for offering me an opportunity to do my Ph.D at Omayal Achi College of Nursing, and also for extending their philosophical guidance and constant support which transformed my dream of completing the Ph D. into a reality.
This thesis has been executed under the diligent guidance of the subject expert Dr.K.R. Rajanarayanan, MBBS., FRSH.(Lond.), Research Co-ordinator, ICCR, and Governing Council Member, for providing ethical approval, and being a constant support for the study.
completing the thesis.
I offer my deepest gratitude to Dr. S. Kanchana, M.Sc (N), Ph D (N), Post Doc. Research, Research Director, ICCR and Principal, Omayal Achi College of Nursing, for providing a strong foundation in Nursing research. Her perpetual guidance, brain storming ideas, enthusiastic participation in research activities enabled me in sculpturing the manuscript and transforming it into a thesis.
My earnest gratitude to Prof. Manonmani M.Sc(N), Ph.D, Co guide, Omayal Achi College of Nursing for her constant motivation, timely suggestion and valuable guidance for the completion of the study.
I am deeply indebted to the Doctoral Advisory Committee Members Dr.Padmavathy, M.Sc(N), Ph.D., Vice Principal, MMM College of Nursing, Chennai and Dr. Vasanthakumari, M.Sc(N), Ph.D., for their efficient guidance, critical thoughts and untiring spirit which capacitated me to execute this study.
My whole hearted gratitude to Dr. D. Celina, M.Sc (N), Ph D (N), Vice Principal, Omayal Achi College of Nursing, for having been a constant source of motivation through her efficient guidance and valuable suggestions in each phase of the research study.
Hospitals, Vadapalani, Chennai who recommended the menu plan for the high risk mothers.
My deepest gratitude to Dr. Venkatesan Satish, PhD., Biostatistician, for his efficient guidance and assistance in transforming the numerical data into meaningful interpretations.
My heartfelt thanks to Dr. P. Jayanthi, M.Sc(N), PhD (N), PhD Co ordinator, and to Ms. P. Nandhini, M.Sc(N), Nurse researcher, the executive committee members, ICCR and the IEC Department of Omayal Achi College of Nursing for their support and contribution towards the successful completion of the study.
I extend my sincere gratitude to the Subject Experts who offered me their time and validated my data collection and intervention tool and suggested the necessary changes to refine the data collection instrument. My hearty thanks to the technical support who calibrated the instrument used for data collection and to Mr. Anand, HR Manager, Vijaya group of Hospitals, Vadapalani, Chennai, who facilitated this process.
Sir Ivan Stedford Hospital and her team for enabling the smooth conduct of the entire data collection process.
A sincere and whole hearted gratitude to all faculty and the Administrative staff of Omayal Achi College of Nursing, who anchored me in their hook of confidence and supported me throughout the study period.
I am extremely thankful to all the librarians Ms.F.S.Judith and Mr.T.M.Asokan, and Mr.N.Muthukumaran for their kindness and cooperation extended to me in retrieving the related literature and preparing the blue print.
I am grateful to all the High risk antenatal mothers who had accepted to participate in the research study.
I express my profound gratitude and heartfelt thanks to my friends Prof.R. Vijayalakshmi, Ms. Bhagavathy, Ms. Ruth Rani Princely, Ms. Beulah, Ms. Girija, Ms. Uthralakshmi, Ms. Umamaheswari and Ms. Durga for their kindness, helping hearts and mighty hands in successful conduct of this thesis.
My earnest gratitude to Mr.G.K.Venkataraman, Elite Computers, for his commitment and untiring spirit to convert this manuscript into a thesis.
Parents Late Mr. M. Thangavel and Mrs. T. Meenakshi who are always beside me during the happy and hard moments to push and gear me towards my aims and dreams.
My heartfelt thanks to my sister Mrs.T.Muthumari, and brother Mr. T. Rajanprabhu for extending their help and moral support.
My sincere thanks to my in-laws Mr. Pitchaiyah and Mrs. Palaniammal for offering their timely help and managing my children during my absence which enabled me progress smoothly throughout the study period.
At this moment of accomplishment I greatly appreciate my soulmate Mr.P.K. Samy. I successfully overcame many trials and tribulations, its only because of his zeal for passion, unflincting courage and conviction. I would never be able to share back the love and affection he showered upon me and my daughters Ms. Sankara Nivetha and Ms. Jeevitha Ragalakshmi for their moral support and patient acquiescence of the absence of their mother throughout the study period.
ANOVA – Analysis of Variance BMI – Body Mass Index
CDC – Centre for Disease Control and Prevention CPD – Cephalo Pelvic Disproportion
DBP – Diastolic Blood Pressure GDM – Gestational Diabetes Mellitus
Hb – Haemoglobin
HPR – High Risk Pregnancy
ICMR – Indian Council of Medical Research IUGR – Intra Uterine Growth Retardation K CAL – Kilo Calories
Kg – Kilogram
LBW – Low Birth Weight
LSCS – Lower Segmental Caesarean Section MDG – Millennium Development Goals MMR – Maternal Mortality Rate
NDHRIP – Nurse Directed High Risk Interventional Package NFHS – National Family Health Survey
SBR – Still Birth Rate SD – Standard Deviation SEAR – South East Asian Region
SPSS – Statistical Package of Social Science UK – United Kingdom
UNICEF – United Nations Children Emergency Fund US – United States
WHO – World Health Organization
CHAPTER
NO. TITLE PAGE NO.
1 INTRODUCTION 1
1.1 Background of the study 2
1.2 Significance and Need for the study 13
1.3 Conceptual framework 27
2 AIMS AND OBJECTIVES 39
2.1 Title 39
2.2 Statement of the Problem 39
2.3 Objectives of the Study 39
2.4 Null Hypothesis 40
2.5 Operational Definitions 40
2.6 Assumptions 44
2.7 Delimitations 44
3 REVIEW OF LITERATURE 45
3.1 Overview of high risk pregnancy 46
3.2 Research studies related to prevalence of high risk pregnancy 48 3.3 Research studies related to outcome of high risk pregnancy 52
3.4 Research studies related to knowledge about high risk
pregnancy 58
3.5
Research studies related to effectiveness of Nurse directed high risk interventional on knowledge, practice and labour outcome.
59
3.6 Summary, Gaps in the existing literature and new
information’s added by the present study to the literature. 62
4 MATERIALS AND METHODS 64
4.1 Research Approach 64
4.2 Research Design 65
4.3 Variables 65
4.4 Research Setting 66
4.5 Population 67
4.7 Sample selection criteria 68
4.8 Sampling technique 69
4.9 Data Collection tool 69
4.10 Interventions 72
4.11 Content validity 73
4.12 Reliability of the tool 74
4.13 Ethical considerations 74
4.14 Pilot Study 76
4.15 Data Collection procedure 78
4.16 Data Analysis procedure 82
5 RESULTS AND ANALYSIS 84
5.1 Identification of high risk pregnancy among antenatal
mothers in the experimental and control group. 87
5.2 Description of background variables of high risk antenatal
mothers in experimental and control group. 89
5.3
Assessment and comparison of pre and post test level of knowledge, practice and labour outcome among high risk antenatal mothers
96
5.4
Effectiveness of Nurse directed high risk interventional package on knowledge, practice and labour outcome among high risk antenatal mothers.
112
5.5
Correlation of mean differed level of knowledge with practice and labour outcome among high risk antenatal mothers in the experimental and control group.
118
5.6
Association of selected background variables with mean differed level of knowledge, practice and post test level of labour outcome among high risk antenatal mothers
122
6 DISCUSSION 130
7 SUMMARY, CONCLUSION, IMPLICATIONS,
RECOMMENDATIONS AND LIMITATIONS 149
8 REFERENCES 165
S. No. Title Page No. 1.1.1 Frequency and percentage distribution of high risk pregnancy
internationally. 3
1.1.2 Frequency and percentage distribution of elderly primi
internationally. 5
1.1.3 Maternal mortality ratio in India 11
1.1.4 Neonatal mortality rate in India 12
1.2.1 Risk for chromosomal abnormalities by maternal age 17
5.1.1(a) Frequency and percentage distribution of high risk pregnancy among antenatal mothers in experimental and control group. 87
5.1.1(b) Frequency and percentage distribution of high risk pregnancy among antenatal mothers in experimental and control group. 88
5.2.1(a)
Frequency and percentage distribution of demographic variables age education, residential area and religion of high risk antenatal mothers in the experimental and control group.
89
5.2.1(b)
Frequency and percentage distribution of demographic variables type of family, occupation and family monthly income of high risk antenatal mothers in the experimental and control group
90
5.2.1(c)
Frequency and percentage distribution of diet and habit of doing exercise among high risk antenatal mothers in the experimental and control group.
91
5.2.2 Frequency and percentage distribution of clinical variables of the high risk antenatal mothers in the experimental and control group. 92
5.2.3(a) Frequency and percentage distribution of obstetrical variables of the high risk antenatal mothers in experimental and control group. 93
5.2.3(b)
Frequency and percentage distribution of obstetrical variables, history of taking folic acid and of low birth weight among high risk antenatal mothers in the experimental and control group.
94
No. among high risk antenatal mothers in the experimental and control
group.
5.3.1(a) Frequency and percentage distribution of pre level of knowledge in
the experimental and control group. 96
5.3.1(b) Frequency and percentage distribution of post test level of knowledge in the experimental and control group. 97
5.3.1(c) Frequency and percentage distribution of knowledge dimension in the pre and post test of experimental group. 98
5.3.1(d) Frequency and percentage distribution of knowledge dimension in
the pre and post test of control group. 100
5.3.1(e) Frequency and percentage distribution of pre and post test level of
practice in the experimental group. 102
5.3.1(f) Frequency and percentage distribution of pre and post test level of
practice in the control group. 103
5.3.1(g) Frequency and percentage distribution of post test level of early to
labour outcome in the experimental group. 104
5.3.1(h) Frequency and percentage distribution of post test level of early to
labour outcome in the control group. 105
5.3.1(i) Frequency and percentage distribution of post test labour outcome
score in the experimental group. 106
5.3.1(j) Frequency and percentage distribution of post test labour outcome
score in the control group. 107
5.3.2(a) Comparison of pre and post test knowledge score among high risk
antenatal mothers in the experimental group. 108
5.3.2(b) Comparison of pre and post test knowledge score among high risk
antenatal mothers in the control group. 109
5.3.2(c) Comparison of pre and post test practice score among high risk
antenatal mothers in the experimental group. 110
5.3.2(d)
Comparison of pre and post test practice score among high risk
No.
5.4.1 Comparison of pre and post test knowledge scores among high risk
antenatal mothers between experimental and control group. 112
5.4.2(a) Comparison of pre and post test practice scores among high risk
antenatal mothers between experimental and control group. 113
5.4.2(b) Comparison of pre and post test practice scores among high risk
antenatal mothers between experimental and control group. 114
5.4.3(a) Comparison of post test early to labour outcome scores among high
risk antenatal mothers between experimental and control group. 115
5.4.3(b) Comparison of post test early to labour outcome scores among high
risk antenatal mothers between experimental and control group. 116
5.4.3(c) Comparison of post test labour outcome scores among high risk
antenatal mothers between experimental and control group. 117
5.5.1(a) Correlation of mean differed knowledge with practice scores among
high risk antenatal mothers in the experimental group. 118
5.5.1(b)
Correlation of mean differed knowledge with practice and labour outcome scores among high risk antenatal mothers in the experimental group.
119
5.5.2(a) Correlation of mean differed knowledge with practice score among
high risk antenatal mothers in the control group. 120
5.5.2(b)
Correlation of mean differed knowledge with practice and labour outcome scores among high risk antenatal mothers in the control group.
121
5.6.1(a)
Association of selected demographic variables with mean differed knowledge scores among high risk antenatal mothers in the experimental and control group
122
5.6.1(b)
Association of selected obstetric variables with mean differed knowledge scores among high risk antenatal mothers in the experimental and control group.
123
5.6.2.1
Association of selected demographic variables with mean differed Kilocalorie intake scores among high risk antenatal mothers in the experimental and control group.
No.
5.6.2.2(a)
Association of selected obstetric variables with mean differed level of protein intake score among high risk antenatal mothers in the experimental and control group.
125
5.6.2.2(b)
Association of clinical variables with mean differed level of protein intake score among high risk antenatal mothers in the experimental and control group.
126
5.6.2.3
Association of obstetric variables with mean differed level of fat intake score among high risk antenatal mothers in the experimental and control group.
127
5.6.2.4
Association of demographic variables with mean differed level of iron intake score among high risk antenatal mothers in the experimental and control group.
128
5.6.3 Association of selected background variables with post test labour
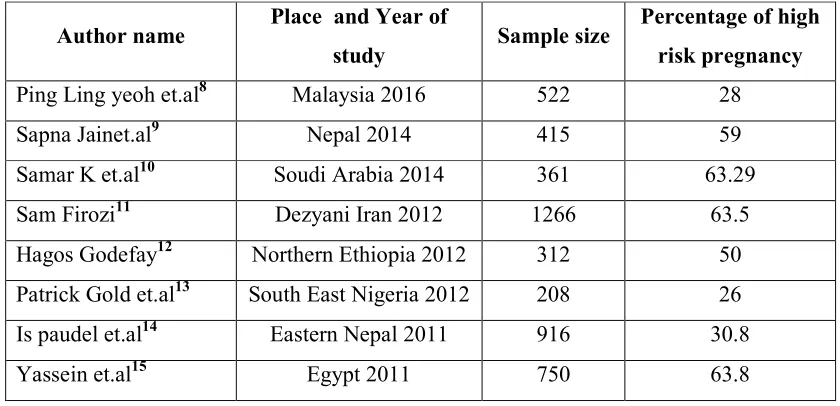
Fig. No Title 1.1.1 Birth rate of mother aged between 15-19 years. 1.1.2 Maternal mortality rate
1.1.3 Trends in maternal mortality rate
1.1.4 New born mortality rate among American women 1.3.1 Conceptual Framework Based on– General Concepts
1.3.2 Application of the Conceptual Framework Based On for the present study 4.15 Schematic Representation of Data Collection Process
5.1.2 Overall frequency and percentage distribution of level of risk in pregnancy among antenatal mothers in experimental and control group
5.4.2 Comparison of pre and post test level of knowledge among high risk antenatal mothers between experimental and control group.
S. No. Title
A Provisional Registration Certificate for the Award of Ph.D B Confirmation of Provisional Registration
C PhD Execution plan- Gantt Chart D Ethical Clearance Certificate E IEC Approval Certificate F Setting Permission Letter G Plagiarism Analysis Report H Certificates
I Research publications J Content Validity Certificate K List of Content Validity Experts
L Bio-physiological Tool Calibration Certificate M Certificates of English and Tamil Editing
N Informed Consent (English and Tamil) O Data Collection Tool (English and Tamil) P Intervention Tool (English and Tamil) Q Ph.D Synopsis Submission Application Form R Ph.D Thesis Submission Application Form S Photos
Effectiveness of nurse directed high risk interventional package on knowledge,
practice and labour outcome among high risk antenatal mothers in selected hospital,
Chennai.
Background: High risk pregnancies affect a significant number of women each year. Approximately 20- 30% of all pregnant women are classified as having high risk pregnancies. A relatively small percentage of high risk obstetric population gives rise to a disproportionately high maternal, perinatal mortality and morbidity. So early identification and appropriate management is the need of the hour to prevent adverse maternal and fetal outcomes.
Aim: To assess the effectiveness of Nurse directed high risk interventional package on knowledge, practice and labour outcome among high risk antenatal mothers.
Materials and Methods: The study was conducted using quantitative research approach with experimental design. A total of 298 high risk antenatal mothers who registered at Sir Ivan Stedford Hospital were the samples. Probability sampling technique with simple random sampling technique was undertaken to select the samples and day wise cluster randomization was used to categorize the experimental and control group. Structured interview schedule, 72 hours dietary recall and modified WHO Partograph were the data collection tools.
Results: The findings of the study revealed that regarding knowledge, the post test mean knowledge score was 20.11 whereas in the control group the score was 10.42 and the mean differed score for knowledge was 9.69 which inferred that there was a very high statistical significant difference in the experimental group. With regard to practice, the mean difference score was 463.44 for K Cal, 17.07 for protein, 5.95 for fat, 22.53 for carbohydrate, 0.16 for calcium and 7.07 for Iron. This inferred a very high level of statistical significant difference in the experimental group. With regard to labour outcome, the post test mean score for experimental group was 9.94 where as in the control group the score was 7.46 and inferred a very high level of statistical significant difference in the labour outcome among experimental group. Statistically significant correlation was observed between knowledge, practice and labour outcome. Statistically significant association of selected demographic, obstetric and clinical variables with mean differed level of knowledge, practice and with post test level of labour outcome score was identified in the experimental group.
Conclusion: The study concluded that the Nurse directed high risk interventional package devised by the investigator was an effective interventional strategy in enhancing the knowledge, practice and labour outcome among high risk antenatal mothers.
Pregnancy and child birth is a natural and happiest event for every women, for
which she aspires and longs for with great expectation. It is a biological function which
remains the survival of the species. Pregnancy and child birth are considered as a normal
physiological process and the outcomes of such pregnancies are good, but some
pregnancies are complicated by problems with mother’s health, the health of the foetus
or complications unique to pregnancy. These pregnancies are at “high risk” for
developing problems and the likelihood of positive outcome is significantly reduced.
High-risk pregnancies affect a significant number of women each year.
Approximately 22% of all pregnant women are classified as having high-risk
pregnancies.A relatively small percentage of high risk obstetric population gives rise to
a disproportionately high maternal, perinatal mortality and morbidity. It is estimated that
globally, nearly 5 lakhs maternal deaths occur every year. About 99 percent of this
occurs in developing countries and hardly 1 percent in developed countries. It is
shockingly high in India, nearly 150 maternal deaths per day, one in every 10 minutes.
For every maternal death, there are 14 perinatal deaths and many women experience
serious complications.
Approximately 2.7 million newborn babies died in 2015, and an additional 2.6
million are stillborn. Nearly 30% of neonates, about 7.5 million are born with a low birth
weight (<2500 g) in India. This accounts for approximately 42% of the global burden.
About 60% of the low birth weight babies are born at term after fetal growth restriction,
whereas the other 40% babies are born as preterm babies. Each year, 3.5 million preterm
(<38 weeks of gestation) neonates are born in India with low birth weight. LBW infants
birth and LBW tend to repeat in families. The epidemiological evidence indicates an
increased risk of preterm/LBW births in a subsequent pregnancy for women with a
previous history of such outcomes. Good perinatal health is therefore important to
individuals, to society and to future generations (Barker et al., 2013).
Hence the investigator felt the need for undertaking a study to assess the
effectiveness of Nurse directed high risk interventional package on knowledge, practice
and labour outcome which is a major key factor for future health planning to manage
high risk pregnancy thereby preventing its complications and enhancing the maternal
perinatal outcome.
OBJECTIVES
1. To assess and compare pre and post test knowledge, practice scores among high
risk antenatal mothers in the experimental and control group.
2. To assess the post test level of labour outcome among high risk antenatal mothers
in the experimental and control group.
3. To assess the effectiveness of Nurse Directed High Risk Interventional Package
(NDHRIP) on knowledge, practice and labour outcome among high risk antenatal
mothers.
4. To correlate the mean differed level of knowledge with practice and labour
outcome among high risk antenatal mothers in the experimental and control
group.
5. To associate the selected background variables with mean differed knowledge,
practice and post test level of labour outcome score in the experimental group and
NH1: There is no significant difference between the mean differed level of knowledge, practice and labour outcome among high risk antenatal mothers in experimental
and control group at P<0.05 level.
NH2: There is no significant relationship between the mean differed level of knowledge, practice and labour outcome among high risk antenatal mothers in experimental
and control group at P<0.05 level.
NH3: There is no significant association of selected demographic variables with mean differed level of knowledge, practice and post test level of labor outcome among
high risk antenatal mothers in experimental and control group at P<0.05 level.
The research process for this study was based on the conceptual frame work
integrating the Wiedenbach’s prescriptive theory with Pender’s health promotion model.
MATERIALS AND METHODS
Experimental research design was undertaken for the study. The independent
variable for the study was Nurse directed high risk interventional package devised by the
investigator and the dependent variable was knowledge, practice and labour outcome.
The study was conducted at Sir Ivan Stedford Hospital, Chennai.
The samples for the study were the high risk antenatal mothers who registered
their pregnancy and planned to deliver in the selected hospital and the sample size was
298 (148 in the experimental group and 150 for control group). The sample size was
randomization was done to categorize experimental and control group.
The data collection instrument was structured knowledge questionnaire for
knowledge, 72 hours dietary recall for practice and modified WHO Partograph for labour
outcome. The Nurse directed high risk interventional package included the following
• Knowledge through Nurse directed education & group discussion - Power point teaching on general information about high risk pregnancy, physiological changes in
pregnancy, early pregnancy registration, diet, regular check-ups, weight gain,
investigations, exercises, antenatal advices( Hygiene, care of the breast, travel, drugs,
care of minor disorders of pregnancy, clothes) and warning signs regarding high risk
pregnancy for a group of (5-7) high risk antenatal mothers during the 1st visit for about 40 -45 min.
• Practice through Nurse directed Dietary programme - the investigator calculated BMI based on the pre pregnancy weight and devised a BMI specific dietary plan in
concurrence with a dietician and the same was recommended for high risk antenatal
mothers.
• Pictorial booklet for reinforcement
The data collection was processed with identifying the high risk antenatal
mothers by pregnancy risk assessment tool devised by the investigator based on the
concepts from Alberta pregnancy risk assessment tool. The background data pertaining
to demographic, obstetric and clinical variables was collected for both experimental and
control group. The pretest level of knowledge was assessed using structured interview
schedule and 72 hours dietary recall for dietary practice for both the groups. Nurse
knowledge, third, sixth and ninth month of pregnancy for practice, during and after
delivery for labour outcome. Reinforcement of information specific to the particular
trimester was given through pictorial booklet to the experimental group. Hospital routine
was followed for the control group. The obtained data was analyzed using descriptive
and inferential statistics.
RESULTS AND DISCUSSION
The pre test mean knowledge score among the experimental and control group
was 10.07 and 9.88 respectively representing very low awareness regarding the
management of high risk pregnancy. In the post test after intervention the mean
knowledge score was 20.11 and 10.42 among experimental and control group
respectively revealed there was a statistically significant difference at p≤0.001among
mothers in the experimental group.
With regard to practice, the mean difference score in the post test 4 was 463.44
for K Cal, 17.07 for protein, 5.95 for fat, 22.53 for carbohydrate, 0.16 for calcium and
for Iron the score was 7.07 respectively. This inferred a statistical significant difference
in the practice score among high risk mothers in the experimental group indicating the
Nurse directed high risk interventional package was effective in improving the dietary
practice.
In the experimental group the mean labour outcome score was 9.94 and in the
control group the score was 7.46. The mean difference score for labour outcome was
between knowledge, practice and labour outcome. Statistically significant association of
selected demographic, obstetric and clinical variables with mean differed level of
knowledge, practice and with post test level of labour outcome score was identified in
the experimental group. Nurse directed high risk interventional package was effective in
significantly enhancing the knowledge and thereby improving the dietary practice and
labour outcome of high risk antenatal mothers.
CONCLUSION
The study concluded that the Nurse directed high risk interventional package was
an effective interventional strategy in improving the level of knowledge, dietary practice
and labour outcome among high risk antenatal mothers. Hence, the study recommended
the utilization of Nurse directed high risk interventional package by the nurses working
in the hospital, community, Nurse educators and health care professionals to improve the
knowledge, practice and labour outcome of high risk antenatal mothers which in turn
CHAPTER – 1
INTRODUCTION
All Human life in this planet is born of women. In all cultures, giving birth to a child is considered as a vital and divine event. The joy and ecstasy of motherhood cannot be expressed in words. The formation of family is of central importance to most societies and indeed, to most of the people’s emotional lives. Pregnancy and motherhood is the most significant phase in the process of reproduction and in the life of every woman.1 It is a biological, emotional, spiritual and social function, which maintains the family continuum. Healthy mothers are important for families, communities and countries at large.
In general, pregnancy should be considered as a unique, physiologically normal episode in a woman’s life.2 Though most pregnancies have healthy, happy outcome, some pregnancies are complicated by problems with mother’s health, the health of the fetus or complications that are unique to pregnancy. These pregnancies are at “high risk” for developing health problems for both the mother and the baby are called high risk pregnancy.3 The health problems may range from delayed fetal or infant growth to preterm labour to maternal or infant death. So improving the maternal and child health is of critical importance in saving the lives of thousands of women and newborn who die due to complications from pregnancy and childbirth each year.4
availability of and access to quality health care service especially for those residing in rural areas, the poor, women and children is very much essential. The target of the Sustainable Development Goals is to reduce the global maternal mortality ratio to less than 70 per 1,00,000 live births between 2016 and 2030. The Government of India recently launched the National Rural Health Mission to improve the availability of quality care to the pregnant population to improve the best possible outcome for both mother and infant.5
1.1 BACKGROUND OF THE STUDY
Pregnancy is defined as a high risk when the probability of an adverse outcome for the mother or child is increased over and above the baseline risk of that outcome among the general pregnant population by the presence of one or more ascertainable risk factors or indicators.6 Risk is defined as a chance of harm or loss. Obviously risk does not necessarily mean a problem will occur, but indicates the need for extra vigilance.
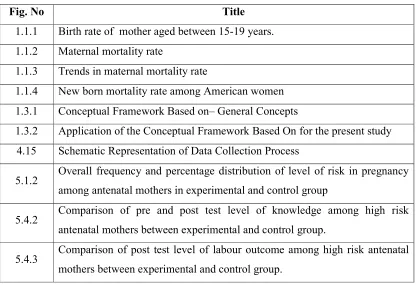
Table 1.1.1 Percentage distribution of high risk pregnancy Internationally
Author name Place and Year of
study Sample size
Percentage of high risk pregnancy
Ping Ling yeoh et.al8 Malaysia 2016 522 28
Sapna Jainet.al9 Nepal 2014 415 59
Samar K et.al10 Soudi Arabia 2014 361 63.29
Sam Firozi11 Dezyani Iran 2012 1266 63.5
Hagos Godefay12 Northern Ethiopia 2012 312 50
Patrick Gold et.al13 South East Nigeria 2012 208 26
Is paudel et.al14 Eastern Nepal 2011 916 30.8
Yassein et.al15 Egypt 2011 750 63.8
High-risk pregnancies occur for a variety of reasons. There are many risk factors that increase the risk for the pregnant woman and her developing fetus beyond the normal and complicate the pregnancy and labour outcome, some factors for high-risk pregnancies result from lifestyle choices that we can control to some degree, while others are out of our control. The risk factors may be pre - existing factors prior to or at the time of antenatal visit or may develop subsequently in the ongoing pregnancy. Some of these include:
Demographic risk factors, pre existing medical conditions complicating pregnancy such as diabetes, hypertension, medical conditions developed during pregnancy Eg Preeclampsia, previous pregnancy risk factors namely repeated miscarriage, preterm labour and baby with congenital anomaly and complications occurs in the current pregnancy and child birth such as premature labor.
world today, and about 350 millions live in SEAR countries. More than 30% of girls in low- and middle-income countries marry before they are 18; around 14% of the adolescents marry before they are 15. Teenage pregnancy almost accounts for 13% of all pregnancies. About 16 million women under age 20 give birth each year worldwide.
[image:33.612.126.524.425.652.2]The vast majority of births to adolescents occur in low and middle income countries. In SEAR alone 6 million adolescents are giving birth each year which is on an average 16% of all births. The average adolescent birth rate in middle income countries is more than twice as high as that in high-income countries. The proportion of births that take place during adolescence is about 2%. in China, 18% in Latin America and the Caribbean and more than 50% in sub-Saharan Africa. Every year, some 3 million girls aged 15 to 19 undergo unsafe abortions.17
The elderly pregnant mothers are often accompanied by a different set of health problems from those of the adolescent pregnancy. The elderly primigravida is generally believed to have decreased fertility and increased risk for adverse pregnancy outcomes like higher incidence of obstetric complications with adverse pregnancy outcomes like mal-presentations, malpositions, prolonged labour, pregnancy induced hypertension, diabetes mellitus, antepartum and postpartum haemorrhage, increased instrumental deliveries, increased caesarean section rate and induction of labour. The prevalence of pregnancy in advanced maternal age varies widely. The percentage distribution of elderly primi is given in the Table 1.1.2.
Table 1.1.2 Percentage distribution of elderly primi Internationally.
Author name Place /Year of study Sample size Percentage of elderly primi
Shapla et.al18 Dhaka 2015 206 19.9
Samar K et.al10 Soudi Arabia 2014 316 44.4
OJule et.al19 Nigeria 2013 471 16
Verma Amarin20 Jordan 2013 471 16
Minoorajajee et.al21 Iran 2011 2940 14.3
South East Asia region. Asian countries have the lowest prevalence of overweight and obesity, but it is increasing sharply. This epidemic also affects younger adults, including women of reproductive age. Currently, obesity prevalence rates among pregnant women are estimated to be as high as 30 %. In addition, approximately 40 % of women gain an excessive amount of weight during pregnancy in Western countries. Studies also show that 1 in every 5 pregnant women are obese in the United States.
Despite the current obesity epidemic, at the other end of the spectrum, maternal underweight is also common. For instance, 4.3% of pregnant women in the UK and 9.0% of women in China are underweight at the first antenatal visit according to the WHO’s classification. Moreover, 13.3% of Chilean women had a BMI <21 kg/m2, and a population-based Swedish study observed that 9.6% of women had a BMI in the range of 15–19.9 kg/m2.24
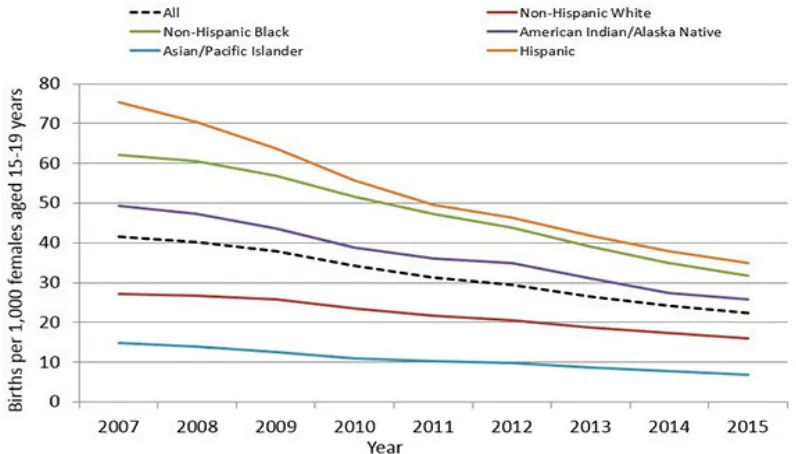
Fig.1.1.2: Maternal mortality rate SOURCE: WHO 2014 -201525
28/100,000 deliveries; incidence is 3 to 4 times higher in non white women. The maternal mortality rate is substantially higher in the US than western countries like Germany, Netherlands, Poland, Spain, Sweden, Switzerland, United Kingdom. 25
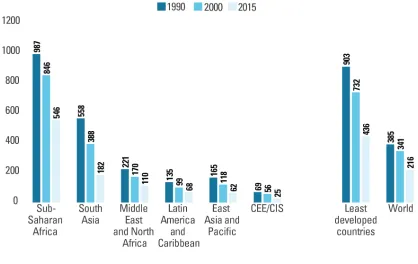
[image:37.612.114.532.350.614.2]Sub-Saharan Africans suffer from the highest maternal mortality ratio of 546 maternal deaths per 100,000 live births a year, which constitute 66 per cent of all maternal deaths per year worldwide. South Asia follows, with a maternal mortality ratio of 66,000 maternal deaths a year, accounting for 22 per cent of the global total. In 2015, the maternal mortality ratio in developing countries was 239 per 100 000 live births where as it was 12 per 100 000 live births in developed countries.26
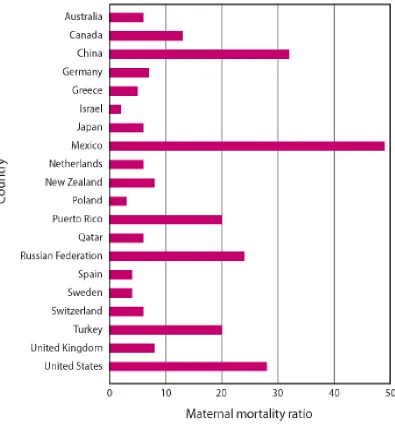
Fig. 1.1.3 Trends in maternal mortality rate Source: UNICEF 2015
weeks of gestation) and early neonatal death (first week of life) per 1,000 total births. In 2015 there were 2.6 million stillbirths globally, with more than 7178 deaths a day. Majority of these deaths occurred in developing countries. Ninety-eight percent occurred in low- and middle-income countries. Three-forths of the stillbirths occurred in South Asia and Sub-Saharan Africa and 60% occurred in rural families from these areas. The stillbirth rate in Sub-Saharan Africa was approximately 10 times that of developed countries (29 vs. 3 per 1000 births). About half of all stillbirths occured in the intrapartum period, representing the greatest time of risk. Estimated proportion of stillbirths that were intrapartum varied from 10% in developed regions to 59% in south Asia.27
Children face the highest risk of dying in their first month of life, at a global rate of 19 deaths per 1,000 live births. Globally, 2.6 million children died in the first month of life in 2016 approximately 7,000 newborn deaths every day most of which occurred in the first week, with about 1 million dying on the first day and close to 1 million dying within the next six days.28 Neonatal mortality was highest in sub-Saharan Africa and South Asia, which each reported 28 deaths per 1,000 live births. A child in sub-Saharan Africa or in South Asia is nine times more likely to die in the first month than a child in a high-income country.29 Across countries, neonatal mortality rates ranged from 46 deaths per 1,000 live births in Pakistan to 1 each in Iceland and Japan. The risk of dying for a newborn in the first month of life is about 50 times higher in Pakistan than in Japan.30
Karnataka. The prevalence of high risk pregnancy was found to be 31.4 % and 12.5% respectively.
Many maternal factors have been associated with an increased risk of spontaneous preterm birth, including young or advanced maternal age, short inter-pregnancy intervals and low maternal body mass index, maternal history of preterm birth. Among them maternal history is a strong risk factor and most likely driven by the interaction of genetic, epigenetic and environmental risk factors
Data of the National Family Health Survey (NFHS)-3 revealed that 16% of women in India, aged 15-19 years, have already started childbearing. This proportion is at the highest in the state of Jharkhand (28%), followed by West Bengal (25%) and Bihar (25%).33 The probability of lifetime risk of maternal death of a 15 year old woman who will eventually die from a maternal cause is 1 in 4900 in developed countries whereas it is 1 in 180 in developing countries. On the other hand there is definite increase in the incidence of elderly primi gravidae among women.34
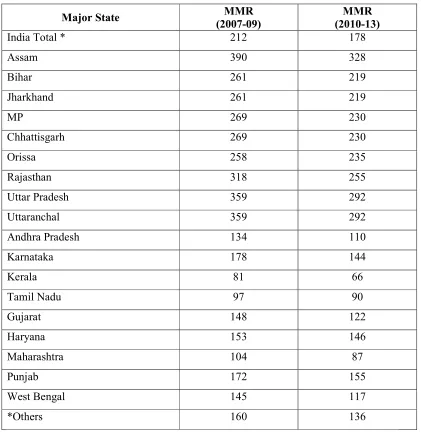
High-risk pregnancies are less common and are potentially serious occurrences. India accounts for the maximum number of maternal deaths in the world. 17 per cent or nearly 50,000 of the 2.89 lakh women died as a result of complications due to pregnancy or childbearing in 2013 and the MMR is 178 maternal deaths per 100,000 live births (Registrar General of India 2013). Almost 50 percentage of all maternal complications & 60 percentage of all primary caesarean section arise from high risk group of cases.38 Table 1.1.3: Maternal mortality ratio in India state wise
Major State (2007-09) MMR (2010-13) MMR
India Total * 212 178
Assam 390 328
Bihar 261 219
Jharkhand 261 219
MP 269 230
Chhattisgarh 269 230
Orissa 258 235
Rajasthan 318 255
Uttar Pradesh 359 292
Uttaranchal 359 292
Andhra Pradesh 134 110
Karnataka 178 144
Kerala 81 66
Tamil Nadu 97 90
Gujarat 148 122
Haryana 153 146
Maharashtra 104 87
Punjab 172 155
West Bengal 145 117
*Others 160 136
The most common causes of adverse perinatal outcomes are preterm birth, birth asphyxia, pneumonia, sepsis and infection. Babies born to mothers under 20 years of age face a greater risk of being still born or premature or low birth weight which increases the morbidity or mortality during their first few weeks of life as well as long-term effects and even death. The younger the mother, the greater the risk to the baby. About 10-20% of pregnancies may be terminated or complicated by abortion, stillbirth, fetal malformation, IUGR, preterm labor, preeclampsia, and GDM.
The current Perinatal Mortality Rate (PMR) in India (2013) is 26 per 1000 births. It ranges from 16 per 1000 births in urban areas to 28 per 1000 births in rural areas. PMR is not uniform across the country, the PMR of Kerala is only 9 per 1000 births, whereas that of Odisha is 35 per 1000 births. The Still Birth Rate (SBR) is estimated at four per 1000 births. India contributes to one-fifth of global live births and more than a quarter of neonatal deaths. About 0.75 million neonates die every year in India, the highest for any country in the world.40
Table 1.1.4: Neonatal mortality rate in India
S.No. State Neonatal mortality rate
India 28
1. Andhra Pradesh 25
2. Assam 27
3. Bihar 28
4. Chhattisgarh 31
5. Delhi 16
6. Gujarat 26
S.No. State Neonatal mortality rate
8. Himachal Pradesh 25
9. Jammu & Kashmir 29
10. Jharkhand 26
11. Karnataka 22
12. Kerala 6
13. Madhya Pradesh 36
14. Maharashtra 17
15. Orissa 37
16. Punjab 16
Source- Sample Registration System41 2013 – 2014
Perinatal outcome can be changed significantly by early detection followed by special intensive care of high risk pregnancies.42 Research has shown that small and affordable measures can significantly reduce the health risks that women face when they become pregnant. Most maternal morbidity and mortality could be prevented if women had access to appropriate and timely health care during pregnancy, childbirth, and immediately afterwards.
1.2 SIGNIFICANCE AND NEED FOR THE STUDY
The world population was estimated to have reached 7.6 billion as of October
2017. The United Nations estimates will further increase to 11.2 billion by the year
2100.42 India is the second most populated country in the world with nearly a fifth of
population of the developing countries. In India, women of child bearing age constitute 22.2% and children under 15 years of age are about 35.3% of total population. Together 57.5% of population consists of mother and children.43
Pregnancy and child birth is a natural and happiest event for every woman, for which she aspires and longs for with great expectation.3 It is a biological function which remains the survival of the species. Pregnancy and child birth are special events for the women and her family. Becoming a mother is one of the most exciting time in a woman's life.A number of biological and social factors during pregnancy influence the outcome. Age, parity, social class and past obstetric history are only some of the factors that should be taken into account while assessing the risk for any pregnant woman.44
A high-risk pregnancy is the one in which the maternal environment or past reproductive performance presents a significant risk to fetal well-being, such as premature birth, small for date infant, full term with low reservoir or still births and early neonatal death. A woman with one or more of the risk factors has an increased risk of delivering a baby with health issues. Approximately 10- 30% of all pregnant women are classified as having high-risk pregnancies in the world.3 The prevalence is more in under developed countries. In India, the prevalence of high risk pregnancy varies in the states. The prevalence is high in Assam, Uttar Pradesh, Uthrangal and Rajasthan and less in Kerala and Tamilnadu.45
obesity is one common condition that classifies a mother for a high risk pregnancy. More than half of all pregnant women in the United States are overweight or obese. High pre pregnancy BMI and excessive gestational weight gain have been reported to have several risks to the mother. Obese patients have a higher prevalence of infertility. Once they conceive, they have higher rate of early miscarriage and congenital anomalies, including neural tube defects and also obesity increases the risk for high blood pressure, preeclampsia, gestational diabetes, stillbirth, neural tube defects, and caesarean delivery.46 National Institute of Child Health and Development has found that obesity can raise infants risk of heart problems at birth by15%.
Anir dasgupta., Harichandrakumar K.T., Syed habeebullah48 (2011) Conducted a prospective cohort study to assess the obesity related adverse outcome in pregnancy, labour and immediate effects on the newborn among 199 pregnant women using new Asian Indian guidelines for obesity in a tertiary care hospital in southern India. The pregnant women were categorized into non-obese, obese and morbidly obese (BMI <35 Kg/m). Hypertensive disorders in pregnancy and gestational diabetes were main outcomes while total LSCS, instrumental deliveries, induction rates, macrosomia, Post partum hemorrhage, shoulder dystocia, birth asphyxia and wound sepsis were also studied. The study results revealed that there was a significant increase in gestational diabetes among morbidly obese (26%) and obese (17%) compared to non-obese (4%)(p = 0.0023). There was a significant increase in LSCS as well as instrumental deliveries. Macrosomia, PPH, birth asphyxia and puerperal wound sepsis were also significantly higher among obese. The study concluded the Obesity is associated with adverse outcomes in pregnancy, in labour and on the fetus at odds comparable to western studies with obesity taken as BMI ≥30 Kg/m.
Teenage pregnancies represent a high-risk group in reproductive terms because of the double burden of reproduction and growth. Complications of pregnancy and childbirth are the leading cause of mortality among girls aged 15-19 years in developing countries. Recent preliminary data from the Centre for Disease Control and Prevention (CDC) indicate that in 2016, for the first time in three decades, birth rates among women aged 30 to 34 surpassed those among women aged 25 to 29 in the United States.50 Currently, the average age of women having their first child is at around 30 years of age. Young and advanced maternal age continues to be associated with a range of adverse outcomes such as increased risk for prematurity pregnancy-induced hypertension and congenital and genetic anomalies. The risk goes up every year. If women get pregnant at the age of 25, the risk of having a baby with Down syndrome, is about 1 in 1,250, there
after the risk is increases with every subsequent year.51
Table 1.2.1 Risks for Chromosomal Abnormalities by Maternal Age
Maternal age Down syndrome Other chromosomal abnormality Under 30 years Less than 1/1,000 Less than 1/385
35 years 1/400 1/192
40 years 1/105 1/66
45 years About 1/25 1/21
Source: National Institute of Health 2016
Verma Amarin20 (2013) Conducted a case review method survey to evaluate the
obstetric intervention, pregnancy complications and outcome. The older women had a significantly higher rate of medical complications like hypertension and diabetes mellitus. There was also a significant increase in the incidence of fetal complication; large babies, trisomy 21, twin pregnancy, Caesarean section rate, incidence of placental abruption, preterm delivery, and neonatal intensive care unit admission. The study concluded that the older women are more prone for maternal and fetal complications and managed by modern obstetric methods, quality healthcare, their pregnancy outcome may be improved.
Short stature of the mother (less than 5 ft) has been associated with increased perinatal morbidity and mortality. Maternal short stature may be a reflection of adverse environmental conditions and poor nutrition as a child. Short women have a higher incidence of operative delivery, including caesarean section because of cephalo pelvic disproportion. Antenatal mothers in the South East Asia and Thai are typically shorter than those in western countries. In developing countries, a significant number of maternal deaths are attributable to the complications of obstructed labour leading to birth canal trauma, postpartum hemorrhage, and genital infections, etc.
special skills, has been investigated extensively especially in developing countries for predicting obstructed labor.52
Samiran Bisai53 (2013) Conducted a hospital based cross-sectional study to assess the influence of maternal height on Neonatal Size among 72 adolescent mother baby pairs in Government general hospital in south Kolkata, India. Weight and height, head circumference, mid upper arm circumference, biceps and triceps skin fold thickness of the mother were recorded using Salter digital weighing scale and anthropometer rod non-stretchable fibre tape respectively. Maternal BMI was calculated using standard formula and also newborn birth weight and length were measured by using triple beam balance and locally made neonatometer. The study findings revealed that the maternal height alone accounted for 12.9% and 16.1% variation in neonate weight and length, respectively and the study concluded that the height of the mother is a well-known predictive index of perinatal mortality and morbidity.
In women who have the past history of obstetric complication or a perinatal loss, there is a tendency for the problem to be repeated in a subsequent pregnancy. A history of previous stillbirth or neonatal death, especially if the cause is unknown, is an indication of high-risk status.54 A woman who has had a previous premature labor has a significantly higher chance of delivering prematurely with a subsequent pregnancy. The risk of recurrence is 25 to 50 percent, and the risk increases with each subsequent preterm birth. (Creasy, 1990).
pregnancy and adverse pregnancy outcomes in previous pregnancies in Uttar Pradesh, India. The results of this study showed that the hazard ratio of having stillbirths were significantly higher among women with obstetric complications compared to women with no obstetric complications.
A relatively small percentage of high risk obstetric population gives rise to a disproportionately high maternal, perinatal mortality and morbidity.55 It is estimated that globally, nearly 5 lakhs maternal deaths occur every year. About 99 percent of this occurs in developing countries and hardly 1 percent in developed countries. It is shockingly high in India, nearly 150 maternal deaths per day, one every 10 minutes. For every maternal death, there are 14 perinatal deaths and many women experience serious complications.56
According to World Bank in 2016, every day, 15 000 children died before their fifth birthday, 46% of them or 7000 babies died in the first 28 days of life. At current trends, 60 million children will die before their fifth birthday between 2017 and 2030. 50% of newborn death will be contributing for the above statement. Approximately 2.7 million newborn babies died in 2015, and an additional 2.6 million were stillborn. Stillbirth is a major obstetric catastrophe and it can occur at any gestational age.
contributed by developing nations like India, Pakistan, Nigeria, China, Demographic Republic of Congo, Ethiopia, Bangladesh, Indonesia, Tanzania and Afghanistan. A number of social and demographic factors are known to be associated with stillbirth, the degree of which varies from country to country. The major causes of still birth are child birth complications, post term pregnancy, maternal infections, and maternal disorders like hypertension, diabetes, obesity, foetal growth restriction and congenital anomalies.57
Nearly 30% of neonates, about 7.5 million are born with a low birth weight (<2500 g) in India. This accounts for approximately 42% of the global burden. About 60% of the low birth weight babies are born at term after fetal growth restriction, whereas the other 40% babies are born as preterm babies. Each year, 3.5 million preterm (<38 weeks of gestation) neonates are born in India with low birth weight. Low birth weight infants are at 11–13 times increased risk of dying than Normal birth weight infants. Indeed, >80% of total neonatal deaths occur among Low birth weight/preterm neonates. Preterm birth and low birth weight tend to repeat in families. The epidemiological evidence indicates an increased risk of preterm/low birth weight births in a subsequent pregnancy for women with a previous history of such outcomes.
six percent samples belonged to 18 or less than 18 years of age; 79.7% were19-34 years; and 14.3% were 35 years or older. Preterm labor and placenta previa were significantly higher in less-than 18 years of age.
Shapla, Islamma, Shahida, Parveen18(2015). Conducted an observational study to identify the various types of high risk pregnancy and to determine the maternal and foetal outcome among 206 high risk pregnant women in the Gynecology and Obstetrics department of Border Guard Hospital, Dhaka. High risk pregnant women were grouped into three. Group A and Group B included pregnant women having medical condition before and during pregnancy respectively. Group C consisted of pregnant women who had pregnancy related high risk issues. The study findings revealed that the majority 43.68% of high risk pregnant patients were in age group of 30-35 years, 19.90% pregnant women were in age group of >35 years and 19.40% were in age group of upto 20 years. Among 206 study population, 60.19% high risk pregnant women were at term at the time of delivery and 39.8% women delivered their babies preterm. Caesarean section was done in 69.41% of high risk pregnant women. 49% neonates had low birth weight and premature 39.80%. During the study period no maternal and neonatal death were observed.
status. The risk assessment and classification of pregnant women into low risk and high risk group helps to mitigate problems early in pregnancy.58
Sapna Jain, SwetaAnand, RupaAherwar9 (2014) conducted a prospective study to detect high risk factors in pregnancy to predict neonatal outcome by prospective multifactorial analysis of high risk factors. Totally 415 antenatal mothers were selected. The ante partum, intra partum and neonatal parameters were integrated into the clinical records and the relationship of risk score to outcome was evaluated for over a period of 1 year. The study findings revealed that out of 415 women, 96 (59%) were high risk, 191 (46%) were low risk and 128 (31%) were no risk. In High risk group there were 59 perinatal deaths and perinatal mortality rate was very high (614 per 1000 live births).
Prenatal care is recognized as an important public health intervention to prevent adverse pregnancy outcomes. A thorough understanding of the physiology of pregnancy, the interrelationships between the mother and fetus, the impact of medical conditions on pregnancy, and pregnancy outcomes on the long term health of both mother and child will help us to manage a high-risk pregnancy. For most women, early and regular prenatal care promotes a healthy pregnancy and delivery without complications. Women going through high-risk pregnancies may require multidisciplinary care and comprehensive evaluation, involving lifestyle modifications, pharmacological and technical support and even hospitalization to ensure that their pregnancies are healthy and that they can carry their babies safely till term.59
Considering the important role of mother’s health, fifth Millennium Development Goal (MDG5) aims at improving maternal health with the targets of reducing maternal mortality ratio (MMR) by 75% of 2009 rate by 2015 and achieving universal access to
reproductive health services
.
To improve the maternal health, barriers that limit access toPonnose Reshmi, Karki Samundra61 (2015) conducted a quasi-experimental study to evaluate the effectiveness of planned teaching programme on knowledge about high risk pregnancy among Muslim women. Totally 60 samples were selected using purposive sampling technique. Structured interview schedule was used to collect the data. A planned teaching programme was administered for the samples after the pretest. The post test was conducted 7 days after the intervention. The study findings showed that there was a significant difference between the pre-test and post-test knowledge scores, which was statistically tested using paired ‘t’ test and was found to be highly significant (t(59) =25.20). The study concluded that the planned teaching programme was highly
effective in improving the knowledge of women.
Thangaratinam S., Rogozińska E., Jolly. K62 (2014) conducted a systematic review to evaluate the effects of dietary and lifestyle interventions in pregnancy on maternal and fetal weight and to quantify the effects of these interventions on obstetric outcomes. 44 randomised controlled trials that evaluated any dietary or lifestyle interventions (diet, physical activity and mixed approach) with potential to influence maternal weight during pregnancy and outcomes of pregnancy were selected. Overall, there was 1.42 kg reduction in gestational weight gain with any intervention compared with control. Interventions were associated with a reduced risk of pre-eclampsia and shoulder dystocia. Dietary intervention resulted in the largest reduction in maternal gestational weight gain, with improved pregnancy outcomes compared with other interventions.
The above stated studies and the researcher’s experience in the obstetrics and gynaecology, reflects that the high risk antenatal mothers are prone for preterm labour, and preterm birth increases the vulnerability to both maternal and neonatal mortality and morbidity. So early identification of the pregnancy with risk factors which cause adverse maternal and perinatal outcomes and sensitizing the high risk mothers on care during high risk pregnancy are considered as a vital role of nurses and midwives.
1.3 CONCEPTUAL FRAMEWORK
1.3.1 CONCEPTUAL FRAMEWORK – GENERAL CONCEPTS (WIEDENBACH’S PRESCRIPTIVE THEORY AND PENDERS HEALTH PROMOTION MODEL)
PENDER’S HEALTH PROMOTION MODEL
The health promotion model guide to nursing care in relation to assisting the
recipients of nursing care in choosing and carrying out behaviors to increase well being.
INDIVIDUAL CHARACTERISTICS AND EXPERIENCES:
The combination of individual characteristics and experiences is unique to each
person and the importance of any characteristic, experience or combination of them
varies with the behavior.
Prior related behaviors are best predictor of future behavior. The indirect effects of prior related behaviors are associated with perception of self efficacy, perceived benefits
and barriers and positive or negative activity related effect, which indicate that the nurse
can help the client more toward health. Promoting behavior by focusing on the benefits.
Personal Factors are described as biological, psychological, psychosocial, sociocultural.
BEHAVIOR SPECIFIC COGNITIONS AND AFFECT:
Behavior specific cognitions and affect are viewed as of major motivational
importance and are considered the core for intervention since they are most amenable to
change through nursing intervention.
Perceived benefits of actions may be intrinsic (feeling better) or extrinsic(time to socialize with practicing the target behavior). Perceived benefits may influence the
observations of others with such outcomes, increases the motivational importance of the
target behavior and relates to the expectation of positive or negative outcomes. Perceived barriers to action
Perceived barriers may influence action directly by blocking that action or
indirectly by decreasing any commitment to act. A key in this construct is that the
barriers are perceived- they may be real as seen by others, or they may be imagined by
the person. It is the perception of the barrier that influences the decision making about
participating in the target behavior. Barriers may relate to degree of availability of access
or resources, costs in money and time, and degree of perceived difficulty. Perceived
barriers are more likely to lead to avoidance of a behavior. With low readiness and
perceptions that barriers are high, change in behavior is not likely; with high readiness to
act and perception of low levels of barriers, action is more likely.
Perceived self- efficacy
Perceived self efficacy or one’s judgement of one’s ability to carryout an
identified action, relates not to a person’s skills but to that person’s judgement about
what can be accomplished with those skills. It is the perception of whether the person