RIT Scholar Works
Theses
Thesis/Dissertation Collections
5-10-2002
How substance abuse affects sibling relationships:
A Qualitative study
Kellee Garney
Follow this and additional works at:
http://scholarworks.rit.edu/theses
This Thesis is brought to you for free and open access by the Thesis/Dissertation Collections at RIT Scholar Works. It has been accepted for inclusion
in Theses by an authorized administrator of RIT Scholar Works. For more information, please contact
Recommended Citation
Graduate Thesis
Submitted to the Faculty
Of the School Psychology Program
College of Liberal Arts
ROCHESTER INSTITUTE OF TECHNOLOGY
By
Kellee Gamey
In
Partial Fulfillment of the Requirements
For the Degree of
Master of Science and
Advanced Graduate Certificate
Rochester, New York
May 10,2002
Approved:
_
Brian Barry, Ph.D.
Jennifer Lukomski, Ph.D.
Dean:
-Permission to Reproduce Thesis
PERMISSION GRANTED
Title
~~esis
:\qH~~gJ~~Ah~~~:..-.--~
1100;
tri.6:biliQSG
~~~ue ~i
I
I
Lf'
\\ee
Cb.
(~
hereby grant permission to the
Wallace Memorial Ubrary oftthe Rochester Institute of Technology to reproduce my
thesis in whole or in part. Any reproduction will not be for commercial use or profit.
Date:
~
/ZOl62
Signature of Author:
PERMISSION FROM AUTHOR REQUIRED
Title of thesis
_
I
prefer to be contacted each time a
request for reproduction is made. I can be reached at the following address:
PHONE:
_
Date:
_
Signature of Author:
_
---PERMISSION DENIED
TITLE OF THESIS
_
I
hereby deny permission to theWallace
Memorial Ubrary of the Rochester Institute of Technology to reproduce my
thesis in whole or in part.
Running
Head:
Substance Abuse
andSibling
Relationships
How
Substance Abuse Affects
Sibling
Relationships:
A Qualitative
Study
Kellee
Garney
Abstract
The
purpose ofthis
research wasto
gain anunderstanding
ofthe
sibling
relationship
whenone
sibling
abusesdrugs
and/or alcohol.It
washypothesized
that
asibling
relationship
with asubstance-abusing
sibling
wouldhave lower levels
ofclosenessandtrust than
non-substanceabusing sibling
relationships.Nineteen young
adults aged19-47
were
interviewed
regarding
their
perceptions ofthe
sibling
relationship.Nine
participants
had
asibling
they
perceived asabusing drugs
oralcohol,
1
participant wasasubstance abuserwith a
non-abusing
sibling,
and9
participantshad
a non-substanceabusing
sibling.The
sample was notrandomly
selectedwith participants recruitedfrom
Rochester Institute
ofTechnology
psychology, sociology,
and socialworkclasses andthrough
acquaintances ofthe
researcher.Siblings
withasubstance-abusing brother
orsister were
found
to
have
moredistant
relationships,
less
trust toward
his/her
sibling,
andpoorer communication within
the
family. Both
the
participant andhis/her sibling
wereIntroduction
Statement
ofthe
Problem
The
authorinvestigated
what affect young-adultdrug
abuse(including
alcohol)
has
onthe
sibling
relationship.Specifically,
does
having
abrother
or sister whom usesdrugs
affectthe
relationship between
them?
Importance
ofthe
Study
Sibling
relationships areoneofthe
longest
lasting
relationships a person willhave
in his/her lifetime.
They
also canbe
one ofthe
first
socialsupportsachildhas growing
up.
Sibling
relationships areuniquein
that
they
canprovide sourcesofsupport, comfort,
companionship
and antagonism(Teti,
1992). The study
ofsibling
relationshipsis
ofparticular
importance
in
adolescenceandyoung
adulthood(Shortt &
Gottman,
1997).
While many
siblings growdistant because
of participationin different
peergroups,
many
stillretain a
strong
tie to their
sibling.Shortt
andGottman
(1997)
found
that
young
adultsibling
relationshipshave
more warmthandless
conflictandrivalry possibly due
to
trying
to
expressthemselves
andbecome
moreindependent from
their
family. This
search
for
anidentity
may
alsolead
to
substance use and abuse(Levine,
1985).
Substance
abusemay
occuras away
to
diminish
or reducediscomfort
withthemselves
ortheir
family
and/orthey
may have
peerswhousedrugs
andintroduce it
to them.
The National Household
Survey (1999)
conductedby
the
U.S. Department
ofHealth
andHuman Services
andthe
Substance
Abuse
andMental Health
Administration
(SAMHA)
reportedthat
10.9
percent ofyouths,
aged12
to
17,
currently
useillicit drugs.
Among
young
adultsaged18-25,
16.1%
reportedusing illicit drugs in 1999. This
figure
and
increasingly
more common problemamong
adolescentsandyoung
adults.With
somany
ofour nation'syoung
adultsusing
drugs,
more andmorefamilies
are effected.While
researchershave
examinedsibling
effectsofdrug
and alcohol use onthe
othersibling's
behavior,
researchershave
not examinedhow
the
relationship
itself is
effected.Family
systemstheory
proposesthat
when a child/adolescentin
the
family
usesdrugs
allthe
relationshipsin
the
family
areimpacted in
someway (Bank &
Kahn, 1982;
Brooks
&
Rice, 1997; Kaufman, 1981; Levine,
1985).
Specifically,
the
theory
statesthat
siblingsofusers often either
become
enmeshed,
disengaged,
parentified,
orvery
successful.
The
useris
often consideredthe
scapegoatofthe
family
andtakes
onthe
entire system's
dysfunction. While
this
theory
is
important
to
ourunderstanding
offamily
dynamics,
it does
nottell
ushow
the
relationship is
changed;
ratherit
givesthe
rolespeople
play
in
the
family.
What
happens
whenoneofthe
personsin
the
sibling relationship
startsusing
orabusing drugs? When
this
important
social supportis
alteredby drug
use,
how does
this
impact
the relationship,
andin
turn the
adolescentoryoung
adultin
the
otherhalf
ofthe
dyad?
Dunn, Slomkowski,
andBeardsall
(1994)
found
negativelife
events such asmaternal
illness,
schoolproblemsor accidentsandillnesses brought
sibling
relationshipscloser,
withmorefriendly
and affectionatebehavior.
However,
Jenkins
(1992)
found
that
in families experiencing
maritaldisharmony
siblingshad
more conflict.Dunn
et al.(1994)
suggestedthat
negativelife
eventsshouldbe
examined more closely.In
particular,
different
categoriesoflife
events shouldbe
studied ratherthan
global scores oflife
eventthat
willhave
an adverse effect onthe
sibling relationship because
ofthe
stressand strain such
behaviors
causefor
everyone associated withthe
substance abuser.In
this
qualitativestudy
of young-adultsibling
relationshipsthe
effectsubstanceabuse
had
onsibling
relationships was examinedto
find
the
difference in
trust
andcloseness
between sibling
relationships withsubstance-abusing
siblings versusnon-substance
abusing
sibling.The
author alsoexaminedthe
difference
in
the
sibling
relationship based
on genderdifferences
andbirth
order ofthe
siblings.Order
ofPresentation
The
literature
offamily
systemstheory
with regardsto
addictionis
reviewed.Literature regarding
typical
sibling
relationshipsand what effecthaving
asibling
with achronic
illness,
mentalillness,
HIV
orsubstance-abusing sibling has
onthe
relationship is
then
critiqued.The
purpose andhypotheses
ofthe
following
study
willbe
described,
followed
by
the
methodsthat
willbe
utilizedandresults,
implications
andlimitations
ofthe
research.LITERATURE REVIEW
Family
Relationships
withinthe
Family
System
Family
relationshipsare animportant
aspectofevery
individual's
life. Almost
everyone
has
afamily
andhas
experiencedboth
negativeand positive emotions andevents
regarding his/ her
family
members.When
there
is
a substance abuserin
the
family,
the
relationshipsamong individuals
canbe
impacted
eithernegatively
orFamily
Systems
Theory
Brooks
andRice
(1997)
described
the
impact
addictionhas
onthe
family
in
the
book,
Families in
Recovery.
According
to
family
systemstheory,
whatever effectsoneperson will effect all people within
that
system.When
addictionoccursin
the
family,
it
is
considered afamily
disease
with each personin
the
family
playing
arolein
the
addiction.
This
addiction canleave
its
membersfeeling
angry,
sad and abandoned.Members
cantake
on various roles withinthe
systemthat
may
supportthe
substanceabuser and/or addiction.
These
roles areoften maladaptiveandunhealthy but
they
areused
to
help
the
individuals
survive and maintainthe
system(Brooks &
Rice,
1997).
This
interaction
ofthe
rolesto
maintainthe
addictionhas
several consequences.First,
trust
becomes
alifelong
issue for
the
members(Brooks &
Rice,
1997). Children
who grow
up in
ahome
with an addict asa parent oftenhave impaired
trust
anddo
notknow
whoto
trust,
or evenhow
to trust
their
ownfeelings
orintuitions. While Brooks
and
Rice
(1997)
discussed
trust
as anissue for
children whenaparent usesdrugs
the
samecould
be
extrapolatedto
apply
to
asibling
whousedrugs. Trust may be impaired
because
the
sibling may
confidein
the
addictedsibling
andhave his/her
secretstold,
money
couldbe borrowed
andnotrepaid,
feelings may be
hurt,
promisesmay be broken
and support
may falter.
Second,
angerandfear may
develop
in
the
memberstoward the
addictand
the
family
system(Brooks
&
Rice,
1997).
The
membersmay be
angeredthat
they
have
to take
on acertain role andthat
they
arein
afamily
with somany
problems.The
membersmay
develop
guilt overtheir
feelings
ofanger,
whichmay
impact
their
others will
find
out aboutthe
addiction.This
shameaboutthe
family
is
oftenfound
in
children of addicts
(Brooks
&
Rice,
1997).
The
roles eachfamily
membertakes
in
the
addictedfamily
andthe
consequencesof
these
roles areimportant
to
understand.However,
notmuch experimentalresearchhas
been done examining
these
roles.While Brooks
andRice
(1997)
discussed
the
family
system
in
terms
of when a parentis
an addictLevine
(1985)
discussed
the
rolessiblingsmay
take
when asibling
is
asubstance abuser.Levine
(1985)
described
the
possibleinteractional dynamics between
adolescent siblingswhen one adolescentis
a substanceabuser.
In
the
sibling dyad
whenone member abusessubstancesthe
other membermay
become
enmeshed andbecome
aco-addict.The
enmeshedrelationship may be
causedby
the
parents'
over-involvementwith each
other,
whichcausesthe
adolescentsto turn to
each other
for
nurturance and acceptance.Another interactional dynamic
that
may
occuris
that the
non-substanceabusing sibling becomes
parentifiedthereby
assuming
the
roleofcaretaker
for
the
substanceabusing sibling
(Kaufman,
1981).
Finally,
the
substance-abusing
adolescentmay
assumethe
scapegoat position withinthe
family
and usedrugs
in
order
to
avoidcompeting
withthe
"successful"sibling
(Levine,
1985).
While
these
aforementioned studiesdiscussed
theory,
Bank
andKahn
(1997,
originalpublication
1982)
attemptedto
describe
the
roles siblingstake
andtheir
relationships
to
their
siblings whenthere
is
a"disturbed"
and a
"well"
sibling using
casestudies
taken
from
clinical practice.They
(1997)
described how
siblings are effectedwhen one of
the
siblingsis
"disturbed"
(mentally
orphysically)
and whenoneis
"well"(not
sick)."Disturbed"
canmeanmental
illness,
chronicillnesses,
HIV
infection,
andsubstance abuse.
They
suggestedthat
a"well"
having
asibling
that
is disturbed
ordeviant
and vice versa.In
particular,
they
suggestedthat
parents reinforcethese
roles ofbeing
"well" and
"disturbed"
by
the
way
they
interact
with
their
children.Most
"well" siblingshad
to
balance
two
different
andcontradicting identities.
For
example,
a"well"
sibling
identifying
withboth
the
"disturbed"sibling
andthe
parent(s) may
act asamediatorbetween
the
sibling
and parent(s).In
the
casestudy
ofPatrick,
he
tried to
buffer
the tensions
in
the
family by
talking
withhis
sister abouther
substanceabuse and
reassuring his
parentsthat
everything
would work out.His
parentswouldoftenpleadwith
him
to talk
withher because "she listens
to
you"
and
he
wouldtry
to
have his
sisterunderstandwhy his
parents were upset.Patrick's
workas a mediatorserved
the
family's function
andcreatedPatrick's
identity
in
the
family
asbeing
the
"competent
andsuccessful"
sibling (Bank &
Kahn,
1997). This
casestudy is
an exampleof
Brooks
andRice
(1997)
andLevine's
(1985)
description
offamily
memberstaking
the
roles of
hero
(overachiever),
enablerandparentified child.Other sibling
relationshipsmay form
sothe
"well"sibling completely
dis-identifies
withthe
disturbed sibling
andalignshis/herself
withthe
parents. Others' createrigid
boundaries
andcutthemselves
offfrom
their
family
andthe
conflictinvolved in
the
family
eitheremotionally
orby
physically
moving
away.One
suchbrother
movedto
adifferent country
to
getaway from
the
responsibilitiesofhaving
abrother
whowasmentally
retarded,
abrother
withschizophrenia,
and amother withdepression (Bank &
Kahn,
1997). On
occasion,
a"well"
sibling may become
arescuerofasibling
witha"disturbance"
these
disturbed
family
relationships can createdifferent
outcomesfor
the
sibling
whodoes
nothave
amental,
physical,
orsubstanceabuseproblem.Closeness
ofTypical
Sibling
Relationships
Before
examining
the
literature
ondisturbed
sibling
relationshipsit is
necessary
to
have
anunderstanding
oftypical
sibling
relationships.Dunn
et al.(1994)
conducted alongitudinal study
with39 sibling
pairsfrom early
childhoodto
adolescence.They
found
that
acrossthe
yearsindividual differences
between
the
siblingswere stableandthose
relationships
that
were characterized as closecontinuedto
be
sevenyearslater (Dunn
etal.
1994).
Similarly, Brody,
Stoneman
andMcCoy (1994)
found
that
69%
ofsibling
relationships classified as
harmonious in
middle childhood were reclassified asharmonious four
yearslater.
Dunn
et al.(1994)
alsofound
that
female-female
relationshipswerecloserthan
male-female relationships and children
from lower
socio-econonmic statustypically
had
more negative or conflictual relationships.
They
alsodiscovered
that
negativelife
events(such
asillness,
accidents) positively
correlatedwithgreaterintimacy
in
the
sibling
relationship.
However,
examination ofthe types
ofnegativelife
eventsis important. It is
possible
that
when asubstance-abusing
sibling
causes stressin
the
family
systemdifferent level
of affectionmay
existbetween
them.
Study
ofnegativelife
eventsis
particularly important
sinceJenkins
(1992)
found
that
maritaldiscord between
parentsresulted
in
anincrease
in
conflictin
the
sibling
relationship.Shortt
andGottman
(1997)
discovered
in
their
research onyoung
adultsibling
relationships
that
family
status variables suchasgender,
age,
andspacing
were notwhocharacterized
their
relationship
as closein young
adulthoodhad
more warmth withless
conflict, rivalry,
and power struggles.Family
statusvariables,
geographicaldistance
or amount of contact
between
the
siblings couldnotaccountfor
the
degree
of closenessin
the
sibling
relationships.Those
siblingswho arestillstruggling
withtheir
statusin
the
relationship
tend to
have
moredistant
andless
close relationships(Shortt &
Gottman,
1997).
Closeness
ofAtypical Siblings Relationships
Siblings
withChronic Illness
Other
researchhas
focused
onthe
reactions childrenhave
to their
chronically ill
sibling.
Bergmann
andWolfe
(1971)
used eight case studiesfrom
their
clinicalpracticeto
highlight
some ofthe
reactionshealthy
children,
ranging in
agefrom four
to
adolescence,
had
toward their
chronically ill
siblings.Overall it
was observedthat
younger children
(ages 4
to
6)
often usedbodily
meansto
expresstheir
feelings
such asbeing
hyperactive, drawing
anill sibling
withdistortions
andpunching
others.For
example,
onehealthy
sisteroften movedher hands
around and punched othersbecause
her
olderbrother
whohad
musculardystrophy (MD)
had
starteddoing
this
whenhis
muscle
deterioration began. To stop herself from
doing
this,
she sat onher hands. Her
anxieties about
developing
MD
andher identification
withher
older sickbrother
werethought
to
causeher hand
movements.School
agedchildren(6
to
12)
identified
withtheir
ill sibling
andoftendeveloped
neuroticpersonality traits
suchascrying
whensomeone else
helped
the
sicksibling
before
she/he could andhaving
disturbing
dreams
that
led
the
childto think
he/she
causedthe
sicksibling
to
be ill.
However,
by
the time
unidentified with
the
ill
sibling,
establishing
cleardifferences
between
themselves
andthe
chronically
ill
sibling
(Bergmann &
Wolfe,
1971).
Often
the
periodof adolescencehelps
in
this
dis-identification
by
having
the teenager
become
involved in
activitiesoutsidethe
home
(Bergmann &
Wolfe).
Thus,
it
is
apparentthat
growing
up
in
ahome
withachronically ill sibling
can causestress,
hysterical
symptomsand neurotic personalities.However,
the
small sample size and considerablepsychoanalyticinfluence
onthese
observations and subjective
interpretations
may bias
the
interpretations
andextrapolations
that
canbe
madefrom
this
research.Siblings
withMental Illness
Solomon
andDraine
(1995)
found
that
whenindividuals lived
withafamily
member who
is mentally ill
they
felt
more stress or moredisadvantaged because
they
had
an
ill
family
memberthat
neededtheir
supportandcare.Having
afamily
member whois
mentally
ill
placesmuch stress onallfamily
memberscausing
them to
feel
moreburdened. Deal
andMacLean's
(1995)
study
extendedthe
finding
ofBergmann
andWolf
(1971)
by
using
moreobjective measuresand aslightly larger
samplesize.They
sought
to
determine
the
impact
siblings with mentalillness have
on sibling'spsychological adjustmentand
sibling
relationships.Fifteen
younger siblings ofpsychologically
disturbed
siblingsand15
youngersiblings whodid
nothave
anolderbrother
orsister withmentally
illness
were recruitedfor
participation.The
controlsample was asampleofconvenience.
Using
established psychologicalmeasures and aninterview,
the
researchers soughtto
measureself-esteem,
personaladjustment,
Similar
to
Bergmann
andWolfs
(1971)
pilotstudy
with children of chronicillness,
Deal
andMacLean
(1995)
found
that
participants whohad
asibling
that
had been
hospitalized for
a psychoticdisorder
reported moreinternalizing
behaviors
orpsychological
distress
such aswithdrawal,
anxiety,
depression,
somaticcomplaints,
andsocial problems
than
siblingswhodid
nothave
adisturbed
sibling.However,
in
contrastto
Bergmann
andWolfe's
findings
that
siblingsidentify
withtheir
ill sibling Deal
andMcLean
found
that
children whohad
asibling
withmentally illness
identified
less
withthat
sibling
andthought
morenegatively
ofhim/her. In
particular,
siblings ofmentally ill
brothers/
sistersdescribed
themselves
as similarin
physical appearancebut
weredissimilar
in personality
andconduct,
whichmay have
contributedto the
siblings notidentifying
withthe
mentally ill
sibling.Similarly,
researchconductedonheroin
addictsand
their
non-addictedbrothers found
that
40%
ofnon-addictedbrothers
mentionedpersonality differences for
the
reasonwhy
they
did
not usedrugs
andwhy
their
brothers
did (Maddux &
Desmond,
1984).
Deal
andMacLean
(1995)
alsofound
that
the
sibling
ofthe
brother
or sister withamental
illness
perceivedhis/her relationship
asbeing
less
positivethan those
whodid
not
have
asibling
with mentalillness. In
particular, the
healthy
siblingsfelt
that
they
received
less
parental support and attentionfrom
their
parentswhenthey
had
abrother
orsister withapsychological
disorder
(Deal
&
MacLean,
1995). While Bergmann
andWolf
(1971)
did
not examinethese variables,
astudy
onsibling
relationships with anHIV infected sibling
did,
which willbe discussed
in
further detail below.
While
the
siblingswhosufferedfrom
mentalillness in
the
Deal
andMacLean
(1997)
studied adolescents with antisocialdisorders
and comorbiddisorders.
Utilizing
alarger, diverse,
and representative sample (N=698)
and standardizedmeasures, the
researchers were more confident
in
their
findings
and generalizations.Their
sampleconsistedof
698
adolescents who were groupedinto
treatment
categories ofhaving
asibling
with eitherOppositional
Defiant Disorder
(ODD)
orConduct Disorder
(CD)
orsome other
form
of a mentalillness
that
was notODD
orCD
asthe
control group.The
children who
had ODD
andCD
alsohad
comorbid presentations with alcohol abuse(19%),
emotionaldisorders
(25%),
and attentiondeficit disorder
(ADD)
(19%). The
control
group
consisted ofindividuals
whohad
asibling
that
had
emotionaldisorders
(43%),
ADD
(13%>)
andalcohol abuse(22%). The sibling relationship
was assessedusing
a self-report measuredesigned specifically
to
measure qualities of relationshipsentitled
the
Sibling Relationship
Questionnaire
(SRQ)
(Slomkowski, Cohen,
&
Brook,
1997).
It
wasfound
that
siblings whohad
an antisocialbrother
or sisterreported morenegatively
charged relationships withthat
sibling.Individuals
whohad
an antisocialsibling had less
warmthandclosenessin
their relationship,
more negativeinteractions
and morecompetition
than
adolescents whohad
asibling
with mentalillness.
However,
sibling
relationshipsthat
had
asibling
withODD
orCD
witha comorbid conditiondid
not result
in
anincrease
of negativerelationshipsfor
these
siblings.Overall,
siblings ofadolescentswith otherpsychological
disorders had relatively
normalrelationships withtheir
siblings(Slomkowski
etal., 1997).
Slomkowski
etal.'s(1997)
finding
that
siblingswithjust
emotionaldisorders,
MacLean's
(1995) finding
that
children whohave
asibling
with a mooddisorder have
less
positive relationships.This may
be due
to the
agedifferences
among
the
individuals
who participated.
In
Slomkowski
et al.'s(1997)
study
the
averageage ofthe
participants was16.2
years old.The
average ageofthe
participants ofDeal
andMacLean's study
was1 1.4
years old.As Bergmann
andWolfe
(1971)
found,
younger childrenexperience more psychologicaldistress
than
adolescents who werebetter
ableto
cope withthe
sibling
withchronicillness.
Thus,
the
coping
abilities ofthe
individuals
andthe
opportunitiesto
disengage
from
the
sibling
by
participating in
activities outsidethe
family
of originmay
mediatethe
impact
psychologicalillness
or chronicillness has
onthe
sibling
relationship.Further
researchis
neededto
examinethe
effectsof particulartypes
of psychologicaldisorders
have
onthe
sibling relationship
across ages.Young
adulthood
has
yetto
be
examinedin
the
literature
to
assessthe
impact
mental and chronicillnesses may have
onthe
sibling
relationship.Siblings
withHIV
While
the
above mentionedstudieshave discussed
the
effects onsibling
relationships when
there
is
amentally
ill
orchronically ill
sibling,
Daniel
(1998)
examined
the
effects ofhaving
anHIV+
sibling has
onthe
sibling
relationship.Eighteen
childrenwith anHIV infected
sibling
and18
childrenwithoutanHIV
infected
orchronically
ill
sibling
were recruitedfor
participation.The
meanage ofthe
siblings of children withHIV
was12.5
year withthe
mean ageofchildren withoutaninfected
It
wasfound
that
siblings of children withHIV
weremorelikely
to
have
rivalrousfeelings
toward their
sibling.In particular,
the
researcherfelt
that
parentspaidmoreattention
to
andhad
more concernfor
the
sibling
withHIV
(Daniel,
1998).
This
finding
is
similarto
Deal
andMacLean's
(1995) finding
that
siblings of children with mooddisorders felt
that
they
receivedless
parental support andattention.Both
studiesusedchildrenwithsimilar
ages,
which provides strongersupportto the
finding
that
youngersiblings experience more
feelings
ofrivalry
whenthere
is
amentally ill
orchronically ill
sibling
present.Further
researchis
neededto
examinethis
effectwithdifferent
agegroups suchas adolescents and
young
adults.The sibling
relationshipswithHIV
infected
childrendid
notdiffer from
the
control
group
of siblingswithoutany
chronicillnesses in
terms
ofwarmth,
closeness orconflict
(Daniel,
1998). This
is
aninteresting finding
andmay be
an artifact ofthe
smallsample size.
Further
research shouldinvestigate
these
variables again withalarger
sample
to
seeif
the
resultshold
up.However,
childrenwhohave
anHIV
infected sibling
exhibited
less nurturing behavior
andweregenerally less
dominant
overtheir
infected
siblings.
The
type
ofquestionsthat
wereaskedto
define nurturing behavior may have
contributed
to this
finding. For
instance,
doing
extra chores aroundthe
house did
notqualify
as anurturing
behavior. These
siblingsmay have been
taking
care ofthe
household
to
free
the
parentsto
spendmoretime
caring for
the
infected
sibling.These
non-infected siblingsalso
held less
status and powerin
the
relationship
when comparedto the
control group.This
finding
may be due
to
the
sensitive nature ofHIV
infection
exclusion
from
caregiving for
the
infected
sibling resulting
in less
opportunity
to
exertdominance
(Daniel,
1998).
Siblings
withSubstance
Abuse
While
there
is
avast amount of researchthat
has
addressed whetherhaving
anolder
sibling
that
usesdrugs increases
the
riskfor
ayoungersibling
to use, there
has
been
very little
researchexamining
the
sibling relationship itself
whenonesibling
uses orabuses
drugs. This may be due
to the
relatively
recent(15
years)
focus
onsibling
relationships.
Also,
since substance abuseas afield
ofstudy is relatively
new,
very few
researchers
have begun
to
link
sibling
relationships and substance abusetogether.
Thus,
it has
notbegun
to
examine whatimpact
substance abuseonthe
partof asibling may
have
onthe
sibling
relationship.In
athorough
reviewofthe
literature only
onestudy
wasfound
examinedwhethersibling
relationships werelinked
to
substanceusethat
(Hall, Henggeler, Ferrerira,
andEast,
1992). In
this study,
37
female
adolescentswererecruitedfrom
the
Positive
Adolescent Life Skills
project(PALS). These
teenagers
wereathigh-risk for
developing
substance abuseproblems and/or were pregnant.
Most
camefrom
one-parent,
disadvantaged homes
withlow
educational attainmentby
the
parentsandhad
an averageage of
16.9
years.A
mixofHispanic
(16),
African-American
(14),
Caucasian
(4),
Asian
(2),
andAmerican Indian
(1)
female
adolescents were sampled(Hall, Henggeler,
Ferriera,
&
East,
1992).
Using
the
Sibling
Relationship
Questionnaire
(SRQ),
the
researchers soughtto
determine
if
substance abuse waslinked
to
sibling
relationships.It
wasfound
that
whenadolescent was more
likely
to
have
used alcoholand marijuanafor
atleast 1-year
orhad
alife
long history
ofdrug
use(Hall
etal.,
1992).
Thus,
those
adolescentswho used alcoholand marijuana
for
an extended period oftime
ratedtheir
sibling relationship
asfilled
withmore conflict and
rivalry
andthe
sibling relationship had
moreimpact
onwhetherthe
participants used
drugs
than
other relationshipswithinthe
family. It may be
that these
relationships are
indeed filled
withthese emotions,
however,
it may
alsobe
adistorted
view of
the
relationship
causedby
the
drug
use.These feelings
of conflict andrivalry
may
resultfrom viewing
his/herself
asdifferent
from his/her
drug
abusing sibling in
terms
ofpersonality
andbehavioral
conduct.As
reportedearlier,
Maddux
andDesmond's
(1984)
found
that
40%
ofnon-substanceabusing
siblingsreportedto
have
different
personalities and conductthan their
drug-abusing
siblings whichdisuaded
them
from using heroin.
Unfortunately,
Hall
et al.(1992)
did
notdetermine
the
rate ofdrug
usefor
the
other
sibling in
the relationship,
whichmay be
animportant
variableto
considerin light
of
family
systemstheory
that
suggeststhat
siblings often areco-addicts or enablersofthe
drug
use(Levine
1985; Kaufman,
1981).
Hall
et al. alsodid
notutilize a controlgroup
therefore
it is
unknownif
these
conflictualrelationshipsare normativefor
at-risk,
economically impoverished
adolescentsin
whichthe
sibling relationship may already be
strained
due
to their
circumstances.It
is
alsounknownwhatthe
sibling relationship
waslike before
the
drug
usebegan.
Further
research needsto
examinehow non-using
adolescents
feel
abouttheir
sibling relationship
withthe
drug-using
sibling
in
orderto
Summary
andCritique
ofAtypical
Sibling
Relationships
Taken
together,
the
studiesindicate
that
having
asibling
whois
"atypical"
may
cause psychological
distress
andanxiety
for
the
healthy
sibling (Bergmann &
Wolf,
1971;
Deal
&
MacLean, 1995;
Solomon &
Drain,
1995). The
qualities ofthe
sibling
relationships
differed according
to the
age ofthe siblings, the
particularillnesses
the
siblings
had
andthe
amount ofidentification
that
took
place withthe
ill
sibling.In
particular,
siblingswhohad
an antisocialbrother
orsister experiencedless
positive andmorenegativerelationships with a
higher level
of competition when comparedto
siblingswith otherpsychological
illnesses (Slomkowski
etal.,
1997).
However,
children whohad
siblingswith
HIV
experienced morerivalry
andhad
comparablelevels
ofwarmth,
closeness,
and conflict asthose
whohad
siblingsthat
did
nothave
chronicillnesses
(Daniel,
1998).
Heightened rivalry
wasalso shownfor
school aged children whohad
asibling
withamooddisorder (Deal
andMacLean, 1995)
andfor female
adolescentswhohad
used alcohol andmarijuanafor
atleast
one year(Hall
etal.,
1992).
Rivalry
orcompetitiveness was
found
across alldisorders
and all agesfor
the
empirically
conductedresearch
(Daniel, 1998;
Deal
&
MacLean, 1998;
Hall
etal.,
1992;
Slomkowski
etal.,
1997).
However,
discrepancies
werefound
in
the
level
ofpositive(warmth)
in
the
relationship
andthe
level
of negative(or conflict) in
the
relationships.Deal
andMacLean
(1995)
found
that the
sibling
relationshipsof childrenwithmooddisorders
were
less
positivethan those
without.In
contrast,
Slomkowski
et al.(1997)
found
that
siblings of children withpsychological
disorders
otherthan
ODD
andCD
weresimilarto
positive.
Daniel
(1998)
found
nodifference
between
the
warmth/ closeness andconflictof
sibling
relationships whenthere
was asibling
withHIV
or without asibling
with chronicillness.
Thus,
further
researchis
neededto
determine
whatthe
effects ofdifferent
pathologiesmay
have
onsibling
relationshipswith a child withoutany
pathology.These
differences
should alsobe
examinedin
terms
ofthe
developmental
stage of childrenandtheir
ablity
to
cope withthe
stressesofliving
with anindividual
whois
atypical.As
Bergmann
andWolfe
(1971)
pointedout,
as childrenage, their
coping
strategies andthe
resources available
to them
improve.
In
addition,
many
children(63%)
whohave
asibling
with adisability
may
wishto talk to
someone abouttheir
experienceandfeelings
(Bischoff &
Tingstrom,
1991).
Solomon
andDraine
(1995)
supportBergmann
andWolfe's
observation,
citing
that the
more supportive assistanceindividuals
receive andthe
moreself-efficacy
andmastery
the
individual holds
the
less
subjectiveburden
they
experienceliving
with amentally ill
adult.As
individuals
age,
they
may be better
ableto
request andreceive assistanceandunderstandtheir
ownstrengths and weaknesseswhenliving
withamentally ill
family
member.Purpose
andHypotheses
Family
systemstheory
andresearchhas
setthe
groundworkto
examinefamily
relationships and specific subsystems within
the
family. The
literature
regarding sibling
relationships whenthere
is
anatypicalsibling
begins
to
supportthe
family
systemstheory
andresearchby focusing
onthe
subsystemofsibling
relationships.Specifically,
relationships
in
whichthere
wasasibling
with amooddisorder
experienced morerelationships of
HIV
infected
siblingshad
similarlevels
of warmth/closenessand conflict andheightened levels
ofrivalry
(Daniel,
1998).
The
literature
focusing
onsubstance abuse andsibling
relationships suggeststhat
substance abuse
by
onesibling
willnegatively impact
the
sibling
relationship.It
washypothesized
that the
sibling relationship
wouldbe less
close and moredistant
withlower
levels
oftrust
in
whichthe
participantdoes
notusedrugs
andthe
sibling does
usedrugs.
For
those
relationshipsin
whichboth
the
participant andthe
sibling do
not usedrugs it
washypothesized
that
higher levels
ofcloseness andtrust
would characterizethe
sibling
relationship.
The
third
hypothesis
wasthat
family
structural variableshad
nosignificantimpact
onthe
quality
ofthe
sibling
relationship.Method
Participants
Nineteen
participants,
ages19-47,
were recruitedfor
participationfrom Rochester
Institute
ofTechnology
psychology, sociology,
and social workclasses andby
word-of-mouth
among
the
researcher's associates and acquaintancesin Virginia. As
shownin
Appendix
A,
as anincentive
to
participatearafflefor
a$100
giftcertificate,
regardlessif
participants completedthe
interview,
was conducted after alldata
was collected.All
(19)
participants were
currently
enrolledin
college orhad
afour-year
collegedegree. Some
(4)
wereworking
towards
orhad
their
Master's degree.
Among
the
participants whohad
asibling
they
perceived ashaving
asubstanceabuseproblem,
four
werefemale
andfive
were
male,
aged19
to
47. Five
ofthe
sibling
pairshad
ayoungersibling
who wasthe
one was a
Female-Female dyad
andfour
wereboth
maledyads. The
mean agedifference
between
the
interviewed
sibling
andhis/her substance-abusing
sibling
was3.1
years(ranging
from
oneto
eightyears)
witheightCaucasian
andoneHispanic
participant.One interview
with a male substance abuser was conducted.He discussed his
relationship
withhis
younger sister andindicated he
abused marijuana.However,
this
interview
wasomittedfrom further
analysisbecause it
was not pertinentto the
hypothesizes.
Nine
(all
Caucasian)
participantswerealsointerviewed regarding
their
sibling
who
they
perceived as non-abusing.Four
females
andfive
maleswereinterviewed,
aged23
to
33. The sibling dyads
were composed oftwo
Female-Male
siblings, three
Female-Female
siblings andfive
Male-Male
siblings.The
meanagedifference between
the
interviewed sibling
andtheir
non-abusing sibling
was4.3
years(ranging
from
oneto
nineyears),
withfive
participantsdiscussing
their
oldersibling
andfour
discussing
their
youngersibling.
Since
asample of conveniencewasused,
generalizationsto
otherpopulations should
be
madewith caution.Seventeen
out ofthe
eighteen participantsreported minimal selfuseofdrugs
oralcohol and most reported
engaging in
socialdrinking
onthe
weekends ordrinking
alcohol with a meal.
Most (eight
out ofnine)
participants reportedthat their
sibling'susedmultiple
drugs
mostcommonly
alcohol and marijuana(88.8%)
followed
by
acid andotherpsychedelics
(44.4%>)
and cocaine(33.3%).
Other drugs
reportedincluded
crackDesign
andProcedure
The
researcher whois
trained
in
counseling
conductedthe
interviews
overthe
phone or
in
person.Most
(13)
interviews
were conductedviathe
phonedue
to
geographical
distance.
However,
sixinterviews
wereconductedin
person.The
interviews
took
approximately
15-30
minutesdepending
onthe treatment condition,
withcontrolparticipants
taking
less
time.
The
researcher, to
gaininsight into
the
sibling
relationship,
generatedthe
open-endedinterview
questionsandthe
results arequalitativein
nature(See Appendix B for
a completelisting
ofquestions).Questions included in
the
interview
askedthe
participantsto
describe
their
relationship
withtheir sibling,
describe
the
best
and worst partsoftheir relationship,
whetherornotthey
trusted the sibling,
andthe
degree
to
whichthe
substanceabuseimpacted
their
family,
friends
andschool.Questions
also asked aboutthe
amount andduration
ofdrug
use, the
communicationwithin
the
family,
andany factors
that
may have
predicatedthe
commencement ornon-useof
drugs.
Before
beginning
the
interview,
each participantsigned a consentform
that
indicated he/she
was over18
years ofage,
knew
he/she
wouldbe
asked abouthis/her
sibling
relationship,
andknew,
if he/she
choseto
participatein
the
researchstudy, that
he/she
couldrefuseto
answerany
question and/or could withdrawfrom
the
study
atany
time.
The
informed
consentform indicated
that
allmaterialswouldbe kept
confidentialand
anonymous,
withonly
the
consentform
having
his/her
nameonit. All
otherinformation
was codedto
preserveanonymity
and confidentiality.All
participants signedthe
informed
consentform
orgavetheir
consentviathe
phone(See Appendix
C)
and noparticipants were given
information
onhow
to
contactthe
researcherif
they
had any
further
questions or concerns and wereinformed
ofwhenthe
rafflewouldtake
place(See
Appendix D).
Results
Quality
ofRelationship
Eighty
percent(80%)
ofthe
participantswhohad
a youngersubstance-abusing
sibling
were stillcurrently abusing drugs
or alcohol atthe time
ofthe
interview.
Participants
whohad
asubstance-abusing sibling
who wasolderreportedthat
all(4
out of4
or100%>)
had
stoppedabusing drugs. One brother
wasin
rehabilitation, two
still useddrugs
recreationally,
and onewasdeceased. Participants
witholder siblings as substanceabusers appeared
to
have
a closerrelationship
withtheir
sibling (3
outof4)
whereasparticipants with youngersiblings assubstance abusers
(4
out of5)
characterizedtheir
relationship
asnot closeordistant
or as one participantphrasedit
as"pseudo
friends". In
all,
four
ofthe
nine participants(44.4%)
in
substanceabusing sibling
relationshipscharacterized
the
relationship
asclose comparedto the
control participantsin
whicheightout of
the
nine or88.8%)
characterizedtheir
relationship
as close regardless ofbirth
orderor gender.
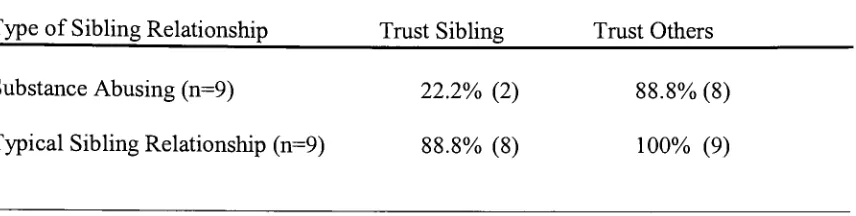
As
shownin Table
1,
gender,
whethersame-sexsibling
pairs ormixed sexsibling
pairs,
did
not seemto
influence
the
reporting
ofthe
relationship
asclose,
supporting
the
hypothesis
that
gender would notimpact
the
reporting
of closeness.Control
participants reportedthey
trusted
their
sibling
(88.8%)
more oftenthan
participants who
had
asubstance-abusing
sibling (22.2%). When it
cameto
trusting
others,
it
appearsthat
both
control participantsand participantswithsubstanceabusing
For
descriptive
purposesthe
next set ofdata
was examined.However,
it
there
aremany
confoundsin
this
data
such as adeceased
sibling
andextremely
small samplesizes,
limiting
the
results andgeneralizability
ofthe
data.
It
is
intended
to
suggestfuture
directions
ofresearch andis only
qualitativein
nature.Therefore,
as shownin
Table
3,
it
is
appearsthe time that the
substance abuse endedhad
agreaterimpact
onthe
reportedquality
ofthe
relationship
ratherthan the type
of substances abused.For
example,
for
those
participants who reportedthat their
sibling had
stoppedabusing drugs
atthe
time
ofthe
interview
(n=5),
60%
reported acloserelationship
comparedto
25% reporting
acloserelationship
whenhis/her sibling
continuedto
abusesubstances atthe time
ofthe
interview (n=4). Those
participantswho reportedthat
his/her sibling had
continuedabusing drugs
atthe time
ofthe
interview
(n=4)
reported adistant relationship
(75%)
compared
to
20%
whohad
stoppedabusing
substances(n=5).
Among
the
sibling
relationships
in
whichthe
sibling had
abused"hard"
drugs (defined
asdrugs
otherthan
marijuanaand
alcohol, n=3),
allhad
stoppedabusing hard drugs
atthe time
ofthe
interview,
withonesibling
deceased,
andonerelationship
characterizedas close andthe
otheras
distant. The
abuseof "soft"drugs
(n=6)
did
notimpact
the
reportedquality
ofthe relationship,
withthree
participantsreporting
a closerelationship
andthree
participants
reporting
adistant
relationship.Of
the
substance abusers characterized aspreferring
softerdrugs
(n=6),
four
continuedto
abusedrugs
andofthose
four
substanceabusing sibling
relationships,
three
reportedadistant
relationship.However,
two
out oftwo
ofthe
substance abuserspreferring
softdrugs
and whohad
stoppedabusing
substances at
the
time
ofthe
interview
reported a closerelationship.Thus,
it
appearsthat
quality
ofthe
relationship
ratherthan the type
ofdrug
abusedbut
future
researchshouldcontinue
to
examinethese
issues
withlarger
sample sizes.Quality
ofCommunication
Communication
withinthe
family
wasalso assessed.It
wasfound
that
participants with a
typical
sibling relationship
reportedthat
communicationin
their
family
was more open(66.6%
offamilies),
enabling
them to
discuss both
important
andunimportant
information
withtheir
family
withnoconsequences,
comparedto
33.3%
offamilies
where substance abuse occurredby
the
sibling.Among
the
controlparticipants,
of
those that
reported communicationwas closed orimpaired in
someway,
otherfamily
stressorswereprominent
including
sexual orientationissues
and alcoholism withinthe
family.
Catalysts for Substance Abuse
Among
all(18)
participants,
parentalbehavior
andmodeling may have influenced
whether or not a
sibling
abusedor avoidedusing drugs
andalcohol.Within
the
substanceabusing sibling
pairs,
five
out of nine participants reportedparentswho werealcoholicsorused
drugs.
Other
possiblecatalyststhat
werereportedfor why
the
substance-abusing
sibling
abuseddrugs
andalcoholincluded
losing
aleg,
peerinfluences,
orincest/rape.
Eight
out ofthe
nineparticipantsfrom substance-abusing
relationshipsindicated
that
they
all avoided
drugs but
used alcoholin
moderation,
whileone participantindicated
that
he
was
initially
introduced
to
drugs
by
his
olderbrother
but
later
stoppedusing
oncehe
sawwhat
it
did
to
his brother.
Participants from
typical
sibling
relationshipsalso reportedthat
parentalmodeling
participants reported
that their
parents engagedin
the
following
behaviors
whichthe
participants credit
to them
notgetting involved
in
drug
abuse: notusing drugs
themselves,
disapproving
of alcohol and notkeeping
it in
the
home,
feeling
trusted andsupported
in
other endeavors.One
participantindicated he
andhis sibling
avoideddrug
use
because
his
father
was an alcoholic andthey
did
notwantto
be like him. Other
positive
influences included
peer avoidanceofdrugs
and/orviewing
the
negativeconsequences of
drug
useby
friends.
Implications
ofthe
Substance Abuse for
the
Substance
Abusing Sibling
andRelationship
Among
the
substance-abusing
siblings,
legal
problems(including
arrestsandjail
time)
resultedfor four
out ofninesiblings, two
enteredrehabilitation,
and one wasinstitutionalized
at one pointin
time.
Not
a single participant claimedany
influence
onpersuading
the
sibling'sto
stop abusing
substances.Among
the
biggest fears
ofparticipantswithsubstance
abusing
siblings wasfinding
the
sibling getting into bad
situations
including
jail, dropping
out ofschool,
living
onthe street,
screwing up
their
lives,
finding
them
dead,
orseeing
them
kill
themselves
in
a car accidentor overdose.They
alsofeared
finding drug
paraphernaliaaroundthe
house
leading
to
disease
transmission
andtheft
ofmoney
and/or otheritems from
them
andothers.Participants
from
abusiverelationshipshad
severalthemes
emergeasthe
mostpainful aspect of
their
relationship.These included watching
a sisterdie (1
participant),
knowing
how
the
abuse affectedtheir
parents(4),
seeing
othershurt emotionally
(2),
feeling
helpless
(2),
andfeeling
angry
atthe
sibling
and parentsfor
notpreventing
the
abuse
(1). Four
participants stillhad feelings
ofanger andhelplessness
years afterthe
indicate
any
area ofdifficulty
or painin
their
relationship.Other
typical
relationship
participants
indicated
that
otherissues
withintheir
family,
such aslarge
agedifferences
between
the siblings,
hiding
asibling'shomosexuality
from
aparentandsibling
rivalry,
had
causeddisruption
in
forging
a closerelationship.However,
these
participants stillindicated
they
currently
felt
close withtheir
sibling.Substance
abusing sibling relationship
participantsindicated
that their
behaviors
and
their
siblings'behaviors
changed whenthe
sibling
wasabusing
drugs. Substance
abusing
siblings werefound
to steal,
lie,
cheat,
andbecome verbally
abusiveto siblings,
parents and
others,
flunk
outofschool,
lose
jobs,
runaway
or moveoutofthe
parentalhome. One
participantindicated
her
sister soldher
children'sChristmas
gifts andthe
furniture in her home
to
raisemoney for drugs. While
the
substanceabusing sibling
engaged
in
these
behaviors,
the
non-abusing
counterparttried
to
cope withit
by
covering
for
the
sibling
orgoing
to
the
otherextreme andtelling
their
parents everything.Others
tried to
distance
themselves.
On
ascaleofoneto seven,
whereone equals not atall and seven equalsvery
much, the
participants reportedthe
degree
to
whichdrug
abusecaused problems atschool,
home,
and withfriends,
the
participant,
andfor
the
abusing
sibling.On
average,
the
drug
abuseimpacted
the
substanceabusing
sibling'sschooling
alot
witharating
of5.9.
At
home,
the
averagelevel
ofdisruption
was6,
followed
by
5.6
for
the
abusing
sibling,
5.3 for
the
participantand2.5 for
the
abusing
siblings'
friends. The
participantreported
that
most oftheir
substanceabusing
sibling'sfriends had little
to
noproblemChange
in
the
Sibling Relationship
overthe
Years
Typically (N=9))
the
substance abusebegan
during
adolescence.Before
this
time,
participantsindicated
varying
degrees
of closenessincluding being
playmates,
sibling
rivalry,
orhaving
an older protectivebrother. Once
the
substance abusebegan,
the
relationship
changed.Five
relationshipsbecame
moredistant,
including losing
respect
for
their
sibling
(2),
being
unableto
forgive
their
sibling
(1),
talking
less
frequently
(1),
andfeeling
regretful(1). What
wasmoreinteresting
is how
the
non-abusing
siblings changed afterthe
drug
abusebegan.
They
became
moreaware ofdrugs,
were afraid of
trying
any drugs
andbecame
moreclose-minded aboutdrug
use andthose
who engaged
in
that
activity.One
participantbecame
more vigilantin watching
overher
children whileanother
became
more awareofthe
warning
signs ofdrug
abusefor
the
adolescents
he
teaches.
One
participantindicated
that
he became
closer withhis
parents.Some
ofthe
participants(4)
indicated
they
felt bad for
their
parents and whatthey
wentthrough
because
ofthe
substanceabuse,
while one wasvery angry
athis
parentsfor
notdoing
anything
to
stop
the
abuse.Compared
to the
substanceabusing sibling
relationship
the typical
sibling
relationship dyads became
closeroverthe
years.Siblings
wentfrom
being
playmates, to
distancing during
the
middle school yearsdue
to
dissimilar interests
to
becoming
closeras adults
because
ofsimilarlifestyles
andinterests
including having
ajob
andstarting
afamily.
One
relationship
began
asdistant
andcontinuedto
be
distant
as adults.Several
(6)
participants mentionedspecifically that
asthey
movedfarther away
geographically
Discussion
Overall,
it
wasfound
that
participantsfrom
substanceabusing sibling
relationships
had
moredistant
relationships
withtheir sibling, trusted their
sibling
less,
and
had
morecommunication
problems withintheir
family
whencomparedto the
non-abusing sibling relationships,
whichis
similarto the theoretical
findings
ofKaufman
(1981),
Levine
(1985)
andBank
andKahn (1997). Compared
to the
atypicalsibling
researchaddressed
above,
it
appearsthat
substance-abusing sibling
relationships aresimilar
to
HIV,
chronically
ill,
and other research on substanceabusing
relationshipsby
causing
more psychologicaldistress
andanxiety for
the
non-abusing
participant(Bergmann &
Wolfe, 1971; Daniel, 1998;
Hall
etal.,
1992).
However,
because
mostofthe
researchwasdone
withchildren,
comparablelevels
ofwarmth andrivalry
cannotbe
estimated
because
they
arein different life
cycles oftheir
relationship.The
currentfindings
are similarto
siblings withantisocialbrother
or sisters(Slomkowski
etal.,
1997)
in
whichthe
sibling relationship is
characterized asless
close.Since
substance abuseis
often characterizedas an antisocial
behavior
this
appearsfitting.
The
relationshipsmay have been
moredistant because
the
non-substanceabusing
participant
may have developed
acoping
mechanismto
deal
withhis/her
feelings
ofanger,
fear,
sadness,
andhurt
by distancing
him/herself
in
orderto
preservehis/her
emotionalandmental
well-being
by
notdealing
withhis/her
thoughts
on adaily
basis.
Behavior
onthe
partofthe
non-substanceabusing
sibling
andthe
substanceabusing
sibling
changeddramatically
asthe
substance use progressedto
abuse andit negatively
impacted
their relationship creating
a moredistrustful
anddistant
relationship.Thereby
closeness and
trust.
Due
to
a small samplesize,
it
is
not clearwhether genderimpacted
the
degree
of closeness reportedby
the
participants.Within
this research, gender,
age orage-spacing did
notimpact
the
degree
of closenessreportedby
the
participantsin
eitherthe
controlgroup
orthe
substanceabusing
relationship.Families
with poorcommunication
patterns alsohad higher levels
of substanceabuse or
family
issues
in
their
homes.
The
substanceabusing sibling may have
turned
to
drugs
andalcohol asaresultofhaving
poorcoping
strategiesincluding
nothaving
aperson
he/she
couldtalk to
regarding difficult
times
withinhis/her life. Often
the
substance-abusing sibling had
a parentalrolemodelthat
engagedin
alcohol abuseorhad
anegative
life
event such aslosing
aleg
orexperiencing incest/rape
that
precipitatedhis/her
abuse ofdrugs. While
these
siblings engagedin
substance abuseto
cope withtheir
life,
the
participantsinterviewed did
not engagein any
seriousdrug
or alcohol useand
in fact
the
sibling's abuse ofdrugs
inversely
effectedtheir
ownuse and consumptionof
drugs. The non-abusing sibling
avoidedorused alcoholin
moderationregardlessofbirth
order.This
is
contrary
to
researchon adolescentdrug
abusewhichfound
alink
between
an older sibling's use ofdrugs
andyoungersibling's commencement ofdrug
abuse
(Brook,
Whiteman,
Gordon
&
Brook,
1990;
Conger &
Rueter, 1996; Needle,
McCubbin, Wilson,
Reineck,