RESEARCH NOTE
Facilitating implementation
of the Decision‑Making Capacity Assessment
(DMCA) Model: senior leadership perspectives
on the use of the National Implementation
Research Network (NIRN) Model
and frameworks
Suzette Brémault‑Phillips
1, Ashley Pike
1*, Lesley Charles
2, Mary Roduta‑Roberts
1, Aruna Mitra
3, Steven Friesen
4,
Lynne Moulton
5and Jasneet Parmar
2Objective
Abstract:
Dementia and other chronic conditions can compromise a person’s ability to make independent personal
and financial decisions. In the wake of an ageing population and rising incidence of chronic conditions, the number
of persons who may require Decision‑Making Capacity Assessments (DMCAs) is likely to increase. Legislation (e.g.,
Trusteeship, Guardianship, Medical Assistance in Dying) also necessitates that DMCAs adhere to legislative require‑
ments and principles. An intentional, explicit and systematic means of implementing standardized DMCA best‑prac‑
tices is advisable. This single exploratory case‑study examined the perspectives of senior leaders and clinical experts
regarding the utility of using the National Implementation Research Network (NIRN) Model to facilitate implementa‑
tion, spread and sustainability of a DMCA Model. Participants learned about the NIRN Model and discussed its applica‑
tion during working and focus groups, all of which were audio‑recorded, transcribed, and analyzed using thematic
analysis.
Results:
Participants found that the NIRN Model aligned well with the DMCA Model, and offered utility to support
implementation, spread and sustainability of DMCA best‑practices. Participants also noted barriers related to its
language, inability to capture personal change, resource requirements, and complexity. It was recommended that a
NIRN‑informed DMCA‑specific implementation framework and toolkit be developed and NIRN‑champions be avail‑
able to guide implementation.
Keywords:
Capacity, Competency, Decision‑making, Capacity assessment, Capacity assessment model,
Implementation, Sustainability, NIRN
© The Author(s) 2018. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creat iveco mmons .org/licen ses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creat iveco mmons .org/ publi cdoma in/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Open Access
*Correspondence: [email protected]
1 Faculty of Rehabilitation Medicine, University of Alberta, Corbett Hall,
8205 14 St., Edmonton, AB T6G 2G4, Canada
Introduction
Adults are presumed to be independent
decision-mak-ers regarding their pdecision-mak-ersonal (e.g., health, housing,
asso-ciations, legal) and financial affairs. When a person’s
decision-making capacity (DMC) in specific domains,
however, comes into question due to diseases such
as dementia and other chronic conditions,
standard-ized Decision-Making Capacity Assessment (DMCA)
processes aligned with legislation are needed. In the
wake of an ageing population, increasing incidence of
chronic conditions and legislative requirements (e.g.,
Guardianship and Trusteeship, Medical Assistance in
Dying), DMCA best-practices and processes need to be
standardized and better-integrated into routine care.
Adherence to such processes best-positions healthcare
professionals to determine person-centred outcomes
that are least restrictive and intrusive, and that
maxi-mize autonomy.
The DMCA Model [
1
,
2
] is an innovative learning and
development model created in 2006 by an acute care
interprofessional (IP) team. The DMCA Model aims
to enable independent practitioners, IP teams,
organi-zations, and large-scale systems to effectively conduct
DMCAs. The Model outlines a standardized process
aligned with provincial legislation. Its aim is to support
screening and pre-assessment, facilitate
problem-solv-ing, support documentation, facilitate education and
mentoring, and enable widespread implementation,
spread and sustainability of DMCA best-practices.
Despite attempts to implement the DMCA Model
across the continuum of care and service sectors,
suc-cessful uptake, spread and sustainability of the Model
has had varying results. Use of intentional,
system-atic, “active and planned efforts to mainstream
inno-vation” [
3
, p. 582] may result in more effective DMCA
Model implementation. While various implementation
frameworks might be utilized [
4
–
9
], the DMCA Model
most closely aligns with the National Implementation
Research Network (NIRN) Model [
5
,
10
–
12
] and its five
overarching Active Implementation Frameworks (AIFs)
[
10
,
12
–
17
]. The purpose of this study was to explore
the perspectives of senior leaders and clinical experts
regarding the applicability of using the NIRN Model
and AIFs to implement the DMCA Model in healthcare
organizations.
Main text
Methodology
Design
A single exploratory case-study design was employed to
document participant perspectives regarding the
util-ity of applying the NIRN Model and AIFs to the DMCA
Model. As the study was exploratory, small-scale data
collection was found to be appropriate before
determin-ing specific research questions and hypotheses [
18
].
Participants
Senior leaders and clinical experts (i.e., managers, senior
leaders, physicians, social workers, occupational
thera-pists, nurse practitioners, professional practice leads)
from health-related organizations across Alberta with
expertise conducting DMCAs were invited to
partici-pate in a NIRN Working Group (a committee formed to
examine a specific question and provide
recommenda-tions) (WGs), a NIRN Bootcamp (an intensive 2-day
training workshop designed to introduce participants to
use of the NIRN Model and its tools), and a focus group
(FG). The in-person NIRN Bootcamp was held October
18–19, 2016. A 1-h teleconferenced FG was conducted
on October 24th, 2016. Participants represented
organi-zations at different stages of DMCA Model
implemen-tation and with varying amounts of DMCA experience.
(See Additional file
1
: Table S1 for participant numbers
& activities).
Data collection
Working Groups, which included eight, 1-h biweekly
teleconferences held between June 20th and September
26th, 2016, aimed to introduce and review NIRN tools/
processes and AIFs and consider their utility in
facilitat-ing implementation, spread and sustainability of DMCA
processes. In advance of the WGs, participants reviewed
selected resources on NIRN’s Active Implementation
(AI) Hub [
17
].
Data analysis
Working Groups and the FG were audio-recorded,
transcribed, and entered into NVivo 11. Thematic
anal-ysis, which was conducted by research assistants
fol-lowing methodology outlined by Braun and Clarke [
19
],
employed both an inductive and deductive approach.
Results
Participants identified facilitators, barriers and
recom-mendations regarding the use of NIRN tools/processes
with the DMCA Model. These are described and
tabu-lated in the following section. (See Tables
1
,
2
,
3
for
themes and related quotes).
The NIRN Model, Active Implementation Frameworks (AIFs) and Tools [5, 10–17]
Table 1 Facilitators of use of the NIRN Model
Category/theme Supporting quotes
The NIRN Model is effective and gives credibility to imple‑
mentation of best‑practices “The NIRN Model has a strong practical element… it’s a very powerful framework.”“The utility is fantastic. What I found of value is just knowing that it is there.” (2016-10-24 (2016‑10‑24)) “It’s a structure to be followed to ensure practice implementation, things are done appropriately. [We] have been talking about that in the past three years; we felt we weren’t being taken seri-ously. Now all of the sudden we are.” (2016-09-12)
“[NIRN gave the language, credibility to speak about and frame implementation]. We all know in a practical sense that it is going to work. When you have a framework, people take things more seriously. Administrators in the group appreciated and understood that there was some research around the NIRN Model and that there was an actual tool we were following that could capture where the holes were. It really supports the work.” (2016-09-12)
“It facilitates adoption and practice change, and if you do it well, fidelity to the practice.” ( 2016-10-24)
The NIRN Model, AIFs and DMCA processes align well “[The NIRN Model] offers something familiar, and aligns with and makes explicit what people already do.” (2016-10-24)
“When I look at the DCMA Model and what the NIRN components suggest, both align very well from what I am seeing so far. Haven’t seen anything in the NIRN that hasn’t been introduced or utilized as people have been implementing decision-making capacity assessment pro-cesses.” (2016-10-24)
“I think the NIRN Model has a lot of use for the DMCA pre‑assessment because it is such a com-plex process that we are using. To have something as detailed and that allows you to explore all the different components of it made a lot of sense in my mind… I think it fits really well with this go around trying to implement this DMCA pre‑assessment process.” (2016-10-24) “It’s a good match, but only if you have someone guiding the process.” (2016-10-24) The NIRN Model provides a clear process for implementing
DMCAs “The NIRN Model facilitates a more global approach to implementing something so that you have a greater chance of it being permanently adopted and having that sustained change.” (2016-10-24)
“The NIRN Model has an enormous amount of detail to it, but it does provide excellent frame-work for figuring out where to go next.” (2016-09-26)
“Reflecting on items in the NIRN Model allowed me to distill where things are going well and where things aren’t and look at foundational things that may have been overlooked otherwise… It helped guide how to present things, influence corporate office around policy, support all these different sites, determine who needs to be involved, how to disseminate information and go from there." (2016-09-12)
"There is a lot of content, but as you are working your way through, it cues you to think about aspects that you might not have in place, to consider where are we… I like how it keeps re‑cueing you to think, “did you look at that”, “do you have a plan written out”, “how are you going to coach that”, “did the plan go out”, [I] see some great value there.” (2016-08-15) “It allowed me to see how the organization I worked for had implemented things. [If you] had
not gone through a process like this and then you wonder why certain initiatives don’t work and others do… it gives a very structured path and allows you to go back into it and double check: has anything been missed, are there areas that needs to be revisited and those are the things I really liked about it.” (2016-09-26)
“For the process itself, I think the way it is set out and the way it is displayed—how it follows the steps, it’s just set up really clearly and I think that is what I wanted to see. There is a structure to it and there is a way to follow through.” (2016-09-26)
“It makes things explicit and everyone is on the same page.” (2016-06-20) Usable innovation: the NIRN Model and AIFs challenge
professionals to define DMCA best‑practices “We are currently… trying to gain consistency with our terminology… I think all of us working through the process also helps confirm that at this level, we all have similar sort of ideas about what should be and what we think should be happening. I think our gold standard of what the practice is would be identified as quite similar. [The challenge is to] come up with something that is concise and using terminology that is consistent.” (2016-09-12)
“The Practice Profile Activity really helped to describe the gold standard of DMC processes, what was acceptable and unacceptable.” (2016-10-24)
“Fidelity Assessments support determination of whether decision‑making capacity assessments are being done well.” (2016‑09‑26)
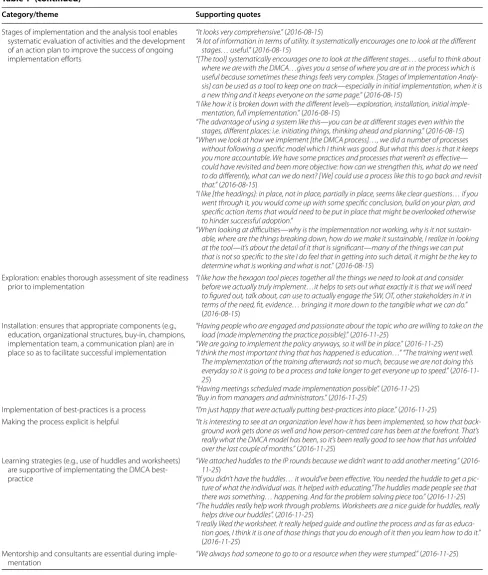
[image:3.595.57.537.99.648.2]Table 1 (continued)
Category/theme Supporting quotes
Stages of implementation and the analysis tool enables systematic evaluation of activities and the development of an action plan to improve the success of ongoing implementation efforts
“It looks very comprehensive.” (2016-08-15)
“A lot of information in terms of utility. It systematically encourages one to look at the different stages… useful.” (2016-08-15)
“[The tool] systematically encourages one to look at the different stages… useful to think about where we are with the DMCA…gives you a sense of where you are at in the process which is useful because sometimes these things feels very complex. [Stages of Implementation Analy-sis] can be used as a tool to keep one on track—especially in initial implementation, when it is a new thing and it keeps everyone on the same page.” (2016-08-15)
“I like how it is broken down with the different levels—exploration, installation, initial imple-mentation, full implementation.” (2016-08-15)
“The advantage of using a system like this—you can be at different stages even within the stages, different places: i.e. initiating things, thinking ahead and planning.” (2016-08-15) “When we look at how we implement [the DMCA process]…, we did a number of processes
without following a specific model which I think was good. But what this does is that it keeps you more accountable. We have some practices and processes that weren’t as effective— could have revisited and been more objective: how can we strengthen this, what do we need to do differently, what can we do next? [We] could use a process like this to go back and revisit that.” (2016-08-15)
“I like [the headings]: in place, not in place, partially in place, seems like clear questions… if you went through it, you would come up with some specific conclusion, build on your plan, and specific action items that would need to be put in place that might be overlooked otherwise to hinder successful adoption.”
“When looking at difficulties—why is the implementation not working, why is it not sustain-able, where are the things breaking down, how do we make it sustainsustain-able, I realize in looking at the tool—it’s about the detail of it that is significant—many of the things we can put that is not so specific to the site I do feel that in getting into such detail, it might be the key to determine what is working and what is not.” (2016-08-15)
Exploration: enables thorough assessment of site readiness
prior to implementation “I like how the hexagon tool pieces together all the things we need to look at and consider before we actually truly implement…it helps to sets out what exactly it is that we will need to figured out, talk about, can use to actually engage the SW, OT, other stakeholders in it in terms of the need, fit, evidence… bringing it more down to the tangible what we can do.” (2016-08-15)
Installation: ensures that appropriate components (e.g., education, organizational structures, buy‑in, champions, implementation team, a communication plan) are in place so as to facilitate successful implementation
“Having people who are engaged and passionate about the topic who are willing to take on the load [made implementing the practice possible].” (2016-11-25)
“We are going to implement the policy anyways, so it will be in place.” (2016-11-25) “I think the most important thing that has happened is education…” “The training went well.
The implementation of the training afterwards not so much, because we are not doing this everyday so it is going to be a process and take longer to get everyone up to speed.” ( 2016-11-25)
“Having meetings scheduled made implementation possible”. (2016-11-25) “Buy in from managers and administrators.” (2016-11-25)
Implementation of best‑practices is a process “I’m just happy that were actually putting best‑practices into place.” (2016-11-25)
Making the process explicit is helpful “It is interesting to see at an organization level how it has been implemented, so how that back-ground work gets done as well and how person‑centred care has been at the forefront. That’s really what the DMCA model has been, so it’s been really good to see how that has unfolded over the last couple of months.” (2016-11-25)
Learning strategies (e.g., use of huddles and worksheets) are supportive of implementating the DMCA best‑ practice
“We attached huddles to the IP rounds because we didn’t want to add another meeting.” ( 2016-11-25)
“If you didn’t have the huddles… it would’ve been effective. You needed the huddle to get a pic-ture of what the individual was. It helped with educating.”The huddles made people see that there was something… happening. And for the problem solving piece too.” (2016-11-25) “The huddles really help work through problems. Worksheets are a nice guide for huddles, really
helps drive our huddles”. (2016-11-25)
“I really liked the worksheet. It really helped guide and outline the process and as far as educa-tion goes, I think it is one of those things that you do enough of it then you learn how to do it.” (2016-11-25)
Mentorship and consultants are essential during imple‑ mentation
[image:4.595.55.544.94.670.2]positively impact adoption and practice change, clarify
and give credibility to implementation processes, and
improve fidelity to DMCA best-practices.
The DMCA Model aligns well with the NIRN Model and AIFs
Participants recognized that the DMCA Model includes
an implementation strategy and capacity-building
pro-cesses. They concluded that the NIRN tools would
sup-port adoption of the DMCA Model at the provider,
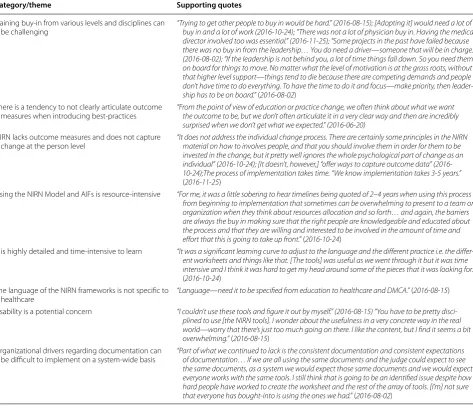
Table 1 (continued)Category/theme Supporting quotes
Implementation teams are critical to ensuring all aspects of
implementation “When I looked at our initial group as we embark on this project, we were all involvedus are front line staff who want to make a moral and ethical change. We looked at educating —a lot of our peers and being an example and model, resource to them. But we didn’t have authority to look at things like performance—providing feedback to upper level of the organization, to have other key changes take place….Things are able to be picked up within various part of the organization from front line staff and some things are reserved for senior leaders.” ( 2016-08-15)
Implementation drivers facilitate operationalization of the
best‑practice “The drivers piece is very important and a good reminder for us of all the various pieces that have to be in place in order to get this to work.” (2016-08-02) “The thing I like about the NIRN is identifying different drivers and the processes together, we came up with a number of concrete action plans that we can do to move forward. So there is an overall feeling of positivity that we are identifying goal along the way that we are achiev-ing but also realize that there are very significant issues that need to tackle as they are startachiev-ing to come up…” (2016-09-26)
Leadership drivers “Leadership at all levels but also in parallel lines.” (2016-08-02)
“Site leaders that are actually engaged and attached to the mentoring team.” (2016-11-25) “[Having] the right people… at the table almost starting into the initial stages of
implementa-tion…getting the people at the table that is actually part of what we have in our drivers. We acted on those right away and brought those people to the table. It changes the dynamic and makes the process richer.” (2016-09-26)
Competency drivers “Is it necessary to have a champion? I would say unequivocally yes. Would it be helpful to teach others what it means? Yes, if we were trying to learn from scratch, it would be the blind leading the blind… Experiential knowledge—it was key she had been through it with other groups before so she can give you that soft knowledge.” (2016-10-24)
“For some of these changes that take place, there is a time component where people have to set time aside to do training and to have the system support.” (2016‑08‑02)
“Coaching and training plan were really good. They make it very overt who is going to do what—very clear.” (2016-09-26)
Organizational drivers “Time… to sit down with people who are clinician and those who have the senior leader’s eye to facilitate practice change.” (2016-09-12)
“Dedicated human resources makes implementation possible. For example, one facility has a .8 FTE for one year to focus on capacity assessment implementation and sustainability.” (2016-10-24)
Documentation: “The structured note: it is key to success. It’s a collective space where people can go and input data, make it more real, as opposed to places where there is no system in place.” (2016-08-02)
Improvement cycles
support adaptation of processes to ensure success “You have to go back part way and then move forwardcycle… carry forward what you have already, but add pieces that you need.”—so we have been engaging in that (2016-09-26) Evaluation: the NIRN framework provides measurable
components and helps service providers identify organizational gaps and barriers to the uptake of the best‑practice
“What I like is that it’s broken down into measurable components.” (2016-06-20)
“I like how it’s broken down with the different levels—exploration, installation… It cues you as you work through to think about aspects that you might not have/have put in place… consider where are we.” (2016-08-15)
“It’s helpful that there’s a framework to use to ask: who, what, where, when, how, why. When applied to CHOICE day program, seniors clinic, long‑term care, that is where we found that as we were working through [the NIRN framework], we found the gaps quite clearly…as a result, they helped guide how we present and influence our umbrella, organization, our corporate office around policy, how to support all these different sites, who needs to be involved, how to disseminate information and go from there.” (2016-09-12)
“Probably having tick marks as a starting point is a good start… Percentage is difficult evaluate—what does 60 versus 80% mean?” (2016-08-15)
“One of the nice things of a tracking tool is that it keeps the momentum going.” (2016-08-15) Communication: NIRN helps to facilitate communication
[image:5.595.56.546.111.626.2]organizational, and system levels, and ensure fidelity to
DMCA best-practices.
The DMCA Model [1–3] is a usable innovation [20]
Participants appreciated the DMCA Model’s
person-centred approach, alignment with provincial legislation,
problem-solving strategies, and emphasis on
determi-nation of least restrictive and least intrusive solutions
to declining DMC. Participants acknowledged the need
for further discussion among service providers to
bet-ter define critical components of DMCAs and gold or
acceptable standards so as to ensure consistency of
DMCA administration.
Implementation stages [5]
Participants indicated that the NIRN’s stages of
imple-mentation and accompanying analysis tool is valuable for
assessing and communicating an organization’s current
state of delivery of DMCA services. Participants
evalu-ated implementation and sustainability processes pro-
and retrospectively using the Analysis Tool, considering
reasons that implementation, spread and sustainability of
the DMCA may have been less effective and ways to
miti-gate barriers.
Implementation drivers [21, 22]
Participants discussed the applicability of
implementa-tion drivers (leadership, competency and organizaimplementa-tional)
to the DMCA Model:
Leadership drivers
—participants
emphasized that senior leader buy-in/support and the
availability of champions is critical to successful
imple-mentation;
Competency drivers
—clinician competencies
were noted to be essential to effective DMCA practice.
Knowledge experts with a dedicated role, protected
time, and critical attributes (i.e., confident,
knowledge-able, credible, trusted, collaborative), were seen as being
best-able to advance DMCA practice. Resources and
ongoing education are also critical to the sustainability
of the DMCA Model;
Organizational drivers
—success-ful DMCA Model implementation requires that
organi-zational drivers be put in place including intake and
documentation processes, mentoring teams, education/
training, and medico-legal-ethical supports.
Implementation teams [5]
Participants identified parallels between NIRN
imple-mentation teams and DMCA Advisory Committees and
Mentoring Teams. Engagement of key players early in the
implementation process was noted to maximize success.
Improvement and communication cycles [5, 23]
Plan-Do-Study-Act (PDSA) and policy-practice
commu-nication cycles were routinely employed by participants
implementing the DMCA Model. More deliberate
com-munication efforts would be helpful. NIRN tools may
support such efforts.
Evaluation [5, 24]
Participants appreciated that a systematic
implementa-tion framework can make successes and potential gaps
more explicit. The NIRN tools and AIFs helped
partici-pants identify what was/was not going well regarding the
implementation of DMCA best-practices.
Barriers to use of the NIRN Model and AIFs
Participants identified barriers related to language,
resources and complexity. Some participants
strug-gled to interpret the NIRN and AIF resources (often
education-specific) into the healthcare context. They
suggested adapting the language to be DMCA-specific
and developing a NIRN-informed Implementation
Framework and Toolkit for the DMCA Model
inclu-sive of a Practice Profile. They also commented on the
time needed to learn and apply the NIRN Model and
AIFs. Participants felt that partnering with a NIRN
implementation specialist or establishing a NIRN
interest-group would be valuable. As implementation
can be lengthy and demanding, (requiring an average
of 2–4 years), strong buy-in, commitment, and a clear
process is needed. To increase the likelihood of
suc-cess, use of the NIRN implementation process in its
entirety is advisable.
Recommendations regarding use of the NIRN Model with the DMCA Model
Participants insisted that use of and training in the
NIRN Model and AIFs is needed, coupled with
sen-ior leader buy-in and access to a NIRN champion or
implementation team.
Discussion
This paper reports on a single-exploratory case study that
considered the perspectives of senior leaders and clinical
experts regarding the applicability of the NIRN Model
and AIFs in supporting implementation, spread and
sus-tainability of the DMCA Model. The emerging themes
suggest that a NIRN-informed DMCA-specific
imple-mentation framework and toolkit would be helpful in
guiding independent healthcare professionals, IP teams,
and organizations when attempting to embed DMCA
processes into routine practice. Participants also
identi-fied challenges associated with use of such a framework
to support DMCA Model implementation.
with the DMCA Model and best-practices. They
indi-cated that implementing the DMCA Model would be
better managed using such an explicit, intentional,
and systematic framework. The NIRN tools helped
par-ticipants identify readiness for DMCA Model adoption,
implementation stages and strategies, and successes,
barriers and gaps related to previous implementation
attempts. Examination of the NIRN tools stimulated
reflection on the importance of champions, fidelity to
DMCA practices, and evaluation and sustainability of the
best-practice. Participants anticipated that utilization of
the NIRN AIFs would increase credibility of the
imple-mentation and the evaluation processes. Overall, the
NIRN Model was found to provide a clear framework for
implementing DMCAs.
Barriers were also identified. The NIRN
implementa-tion process was found to be resource-intensive and its
lengthy timeline was concerning for those who felt that
staff turnover may compromise the process. Some
partic-ipants also indicated that it would be difficult to apply the
NIRN tools and AIFs without the support of dedicated
implementation specialists. Participants further noted
that, while the NIRN Model facilitates evaluation at the
system and process levels, it is less effective in so doing at
the service provider level. Outcome measures to evaluate
the effectiveness of implementation were also found to be
lacking. Finally, the language is more specific to
educa-tional rather than healthcare environments.
Specific to the DMCA Model, participants highlighted
commonality and variability regarding DMCA
best-practices. Terminology regarding, conceptualization and
Table 2 Barriers to the use of the NIRN ModelCategory/theme Supporting quotes
Gaining buy‑in from various levels and disciplines can
be challenging “Trying to get other people to buy in would be hard.” (2016buy in and a lot of work (2016‑10‑24); “There was not a lot of physician buy in. Having the medical ‑08‑15); [Adopting it] would need a lot of director involved too was essential.” (2016‑11‑25); “Some projects in the past have failed because there was no buy in from the leadership… You do need a driver—someone that will be in charge.” (2016‑08‑02); “If the leadership is not behind you, a lot of time things fall down. So you need them on board for things to move. No matter what the level of motivation is at the grass roots, without that higher level support—things tend to die because there are competing demands and people don’t have time to do everything. To have the time to do it and focus—make priority, then leader-ship has to be on board.” (2016-08-02)
There is a tendency to not clearly articulate outcome
measures when introducing best‑practices “From the point of view of education or practice change, we often think about what we want the outcome to be, but we don’t often articulate it in a very clear way and then are incredibly surprised when we don’t get what we expected.” (2016‑06‑20)
NIRN lacks outcome measures and does not capture
change at the person level “It does not address the individual change process. There are certainly some principles in the NIRN material on how to involves people, and that you should involve them in order for them to be invested in the change, but it pretty well ignores the whole psychological part of change as an individual” (2016‑10‑24); [It doesn’t, however,] “offer ways to capture outcome data” (2016‑ 10‑24);The process of implementation takes time. “We know implementation takes 3‑5years.” (2016‑11‑25)
Using the NIRN Model and AIFs is resource‑intensive “For me, it was a little sobering to hear timelines being quoted of 2–4years when using this process from beginning to implementation that sometimes can be overwhelming to present to a team or organization when they think about resources allocation and so forth… and again, the barriers are always the buy in making sure that the right people are knowledgeable and educated about the process and that they are willing and interested to be involved in the amount of time and effort that this is going to take up front.” (2016‑10‑24)
It is highly detailed and time‑intensive to learn “It was a significant learning curve to adjust to the language and the different practice i.e. the differ-ent worksheets and things like that. [The tools] was useful as we wdiffer-ent through it but it was time intensive and I think it was hard to get my head around some of the pieces that it was looking for.” (2016‑10‑24)
The language of the NIRN frameworks is not specific to
healthcare “Language—need it to be specified from education to healthcare and DMCA.” (2016‑08‑15) Usability is a potential concern “I couldn’t use these tools and figure it out by myself.” (2016‑08‑15) “You have to be pretty
disci-plined to use [the NIRN tools]. I wonder about the usefulness in a very concrete way in the real world—worry that there’s just too much going on there. I like the content, but I find it seems a bit overwhelming.” (2016‑08‑15)
Organizational drivers regarding documentation can be difficult to implement on a system‑wide basis
[image:7.595.62.536.104.512.2]the intent of the DMCA Model was a point of
discus-sion and at times sensitivity. “Process” appeared to be a
more agreeable term than “Model” when referring to
DMCAs. Further, although similar concepts were used
by participants regarding DMCA processes,
inconsisten-cies appeared. For example, it was challenging to define
DMCA processes, and isolate assessment components,
essential information to be gathered and by whom, and
gold standard indicators. Reflections on DMCA
pro-cesses stimulated through consideration of the NIRN
Model and tools facilitated greater dialogue,
collabora-tion, DMCA Model development, and consistency of
DMCA practice at organizational, zonal and provincial
levels.
Participants recognized the utility of the NIRN Model,
AIFs and tools. As the NIRN Model provides a clear
process and framework for implementing DMCA
best-practices, organizations might utilize it to support
imple-mentation of the DMCA Model and processes. Such use
may support local as well as widespread adoption of the
DMCA best-practice processes and ensure fidelity.
Com-mitment to its use, however, would necessitate buy-in
at the leadership levels and access to NIRN-specific
resources.
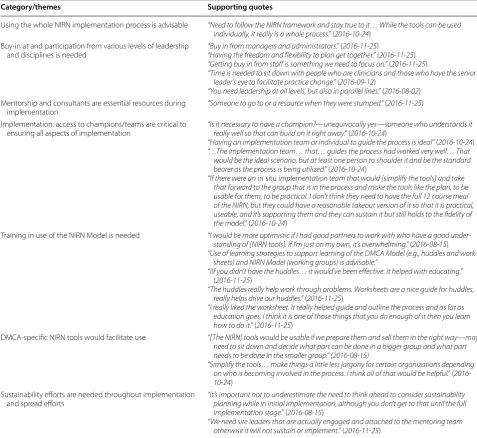
Table 3 Recommendations regarding use of NIRN Model with the DMCA Model
Category/themes Supporting quotes
Using the whole NIRN implementation process is advisable “Need to follow the NIRN framework and stay true to it… While the tools can be used individually, it really is a whole process.” (2016‑10‑24)
Buy‑in at and participation from various levels of leadership
and disciplines is needed “Buy in from managers and administrators.”“Having the freedom and flexibility to plan get together.” (2016‑11‑25 ()2016‑11‑25) “Getting buy in from staff is something we need to focus on.” (2016‑11‑25)
“Time is needed to sit down with people who are clinicians and those who have the senior leader’s eye to facilitate practice change.” (2016‑09‑12)
“You need leadership at all levels, but also in parallel lines.” (2016‑08‑02) Mentorship and consultants are essential resources during
implementation “Someone to go to or a resource when they were stumped.” (2016‑11‑25) Implementation: access to champions/teams are critical to
ensuring all aspects of implementation “Is it necessary to have a champion?really well so that can build on it right away.”—unequivocally yes (2016‑10‑—24someone who understands it ) “Having an implementation team or individual to guide the process is ideal” (2016‑10‑24) “…The implementation team… that… guides the process had worked very well… That
would be the ideal scenario, but at least one person to shoulder it and be the standard bearer as the process is being utilized.” (2016‑10‑24)
“If there were an in situ implementation team that would [simplify the tools] and take that forward to the group that is in the process and make the tools like the plan, to be usable for them, to be practical. I don’t think they need to have the full 12 course meal of the NIRN, but they could have a reasonable takeout version of it so that it is practical, useable, and it’s supporting them and they can sustain it but still holds to the fidelity of the model.” (2016‑10‑24)
Training in use of the NIRN Model is needed “I would be more optimistic if I had good partners to work with who have a good under-standing of [NIRN tools]. If I’m just on my own, it’s overwhelming.” (2016‑08‑15) “Use of learning strategies to support learning of the DMCA Model (e.g., huddles and
work-sheets) and NIRN Model (working groups) is advisable.”
“IIf you didn’t have the huddles… it would’ve been effective. It helped with educating.” (2016‑11‑25)
“The huddles really help work through problems. Worksheets are a nice guide for huddles, really helps drive our huddles.” (2016‑11‑25)
“I really liked the worksheet. It really helped guide and outline the process and as far as education goes, I think it is one of those things that you do enough of it then you learn how to do it.” (2016‑11‑25)
DMCA‑specific NIRN tools would facilitate use “[The NIRN] tools would be usable if we prepare them and sell them in the right way—may need to sit down and decide what part can be done in a bigger group and what part needs to be done in the smaller group.” (2016‑08‑15)
“Simplify the tools… make things a little less jargony for certain organizations depending on who is becoming involved in the process. I think all of that would be helpful.” (2016‑ 10‑24)
Sustainability efforts are needed throughout implementation and spread efforts
“It’s important not to underestimate the need to think ahead to consider sustainability planning while in initial implementation, although you don’t get to that until the full implementation stage.” (2016‑08‑15)
[image:8.595.56.534.102.540.2]Conclusions
The goal of the DMCA Model is to effectively integrate
DMCA best-practices into routine service provision.
Study findings support the future development and
evaluation of a DMCA-specific NIRN-informed
imple-mentation framework and toolkit to facilitate
implemen-tation. Decreased resource requirements would result
from development of such an implementation framework
and toolkit and support best-practice uptake. Access to
a dedicated NIRN-champion or implementation team
would further enable the uptake of DMCA and other
evi-dence-based practices, drive change and offer leadership.
With respect to the implementation of the DMCA
Model, it is recommended that organizations consider
using the NIRN Model, AIFs and tools to support the
uptake of DMCA processes, and ensure sustainability
of and fidelity to DMCA best-practices. Employing the
NIRN Model as a framework for implementation,
sus-tainability and spread of the DMCA Model would offer
an explicit, intentional, and systematic process for
imple-menting and sustaining DMCA processes. While time
and resources are required to do so, not employing an
implementation model can result in failure to implement
or sustain the best-practice, demoralization of staff, and
loss of time and resources. Rather than being focused
on costs associated with the use of an implementation
framework, however, perhaps the better question is
whether or not organizations can afford not to use a
pro-cess and tools that can best-position teams for integrated,
sustained and successful implementation of DMCA
best-practices.
Limitations
This study has a number of limitations. While a
num-ber of organizations from across the continuum of care
participated in this project, the results focus on the
per-spectives of 13 senior leaders and clinical experts who
voluntarily attended some, though not all of, the working
and focus groups, and a NIRN Bootcamp; perspectives
of frontline staff were not captured. As a result, reported
findings are not necessarily representative of all
organiza-tions that have implemented the DMCA Model, nor are
they generalizable to other organizations.
Additional file
Additional file 1: Table S1. Project Activities and Participants. This table includes the number of participants that attended each of the working groups, NIRN Bootcamp and focus group. Also included is the aim and focus of each of the project activities.
Abbreviations
AI: Active Implementation; AIF: Active Implementation Frameworks; DMC: decision making capacity; DMCA: decision making capacity assessment; FG: focus group; IP: interprofessional team; NIRN: National Implementation Research Network; PDSA: Plan‑Do‑Study‑Act; WG: Working Group.
Authors’ contributions
SBP and AP conceived the study concept including examination of the utility of NIRN Framework through stakeholder engagement and its design. LC, MR, AM, SF, LM, and JP contributed to the conception and design of the study. SBP facilitated the FGs. Data analysis and interpretation was supervised by AP and validated by SBP, MR, SF and LM. AP and SBP drafted the manuscript; LC, MR, AM, SF, LM, and JP assisted with manuscript revisions. All authors have given final approval for the current version to published and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Author details
1 Faculty of Rehabilitation Medicine, University of Alberta, Corbett Hall, 8205
14 St., Edmonton, AB T6G 2G4, Canada. 2 Division of Elderly Care, Department
of Family Medicine, Glenrose Rehabilitation Hospital, 10230 111 Ave, Edmon‑ ton, AB T5G 0B7, Canada. 3 Central West Local Health Integration Network,
199 County Court Blvd., Brampton, ON L6W 4P3, Canada. 4 Bethany Care
Society, 101 17 ST, Calgary, AB T2N 2E5, Canada. 5 Edmonton Zone Continuing
Care‑Facility Living, Alberta Health Services, 406‑10216 124 St, Edmonton, AB T5N 4A3, Canada.
Acknowledgements
The authors would like to thank Bryan Sluggett and Karen Lee for their contri‑ bution to the data collection and analysis.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due ethics and operational requirements, but are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical approval for the study was obtained through the University of Alberta’s Health Research Ethics Board (Panel B). Operational approval was obtained from participating organizations and sites, and written consent was obtained from participants.
Funding
This project was funded by the Covenant Health Network of Excellence in Seniors’ Health and Wellness.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in pub‑ lished maps and institutional affiliations.
Received: 5 July 2018 Accepted: 16 August 2018
References
1. Parmar J, Bremault‑Phillips S, Charles L. The development and implemen‑ tation of a decision‑making capacity assessment model. Can Geriatr J. 2015;18(1):15–28.
•fast, convenient online submission
•
thorough peer review by experienced researchers in your field
• rapid publication on acceptance
• support for research data, including large and complex data types
•
gold Open Access which fosters wider collaboration and increased citations maximum visibility for your research: over 100M website views per year
•
At BMC, research is always in progress.
Learn more biomedcentral.com/submissions
Ready to submit your research? Choose BMC and benefit from:
3. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and commenda‑ tions. Milbank Q. 2004;85:581.
4. Proctor E, Brownson RC. Measurement issues in dissemination and imple‑ mentation research. In: Brownson RC, Colditz GA, Proctor EK, editors. Dis‑ semination and implementation research in health: translating science to practice. New York: Oxford University Press; 2012. p. 3–22.
5. National Implementation Research Network (NIRN). National implemen‑ tation research network’s active implementation hub. University of North Carolina at Chapel Hill’s FPG Child Development Institute; 2017. http://
imple menta tion.fpg.unc.edu/. Accessed 15 June 2016.
6. Getting to outcomes improving community‑ based prevention. A toolkit to help communities to implement and evaluate their programs. RAND Corporation and the University of South Carolina; 2016. http://www.rand.
org/healt h/proje cts/getti ng‑to‑outco mes.html. Accessed 17 Oct 2016.
7. RE‑AIM. Reach, effectiveness, adoption, implementation, maintenance; 2016. http://www.re‑aim.org/RE‑AIM. Accessed 17 Oct 2016.
8. Consolidated Framework for Implementation Research. Center for Clinical Management Research North Campus Research Complex; 2014. http://
www.cfirg uide.org/ . Accessed 17 2016.
9. Aarons GA, Hurlburt M, McCue Horwitz S. Advancing a conceptual model of evidence‑based practice implementation in public service sectors. Adm Policy Ment Health. 2011;38(1):4–23.
10. Fixsen DL, Naoom SF, Blase KA, Friedman RM, Wallace F. Implementation research: a synthesis of the literature. Tampa: University of South Florida, Louis de la Parte Florida Mental Health Research, The National Implemen‑ tation Research Network; 2005.
11. Bertram RM, Blase KA, Fixen DL. Improving programs and outcomes implementation framework and organization change. Res Soc Work Pract. 2014;25(4):477–87.
12. National Implementation Research Network (NIRN). National implemen‑ tation research network’s active implementation hub‑about NIRN. Uni‑ versity of North Carolina at Chapel Hill’s FPG Child Development Institute; 2016. http://nirn.fpg.unc.edu/about ‑nirn. Accessed 15 June 2016. 13. Fixsen DL, Blase KA, Timbers GD, Wolf MM. In search of program imple‑
mentation: 792 replications of the teaching‑family model. In: Bernfeld DP, Farrington Leschied AW, editors. Offender rehabilitation in practice: implementing and evaluating effective programs. London: Wiley; 2001. p. 149–66.
14. Metz A, Bartley L, Ball H, Wilson D, Naoom S, Redmond P. Active imple‑ mentation frameworks for successful service delivery: catawba county child wellbeing project. Res Soc Work Pract. 2015;25(4):415–22. 15. Dean Fixsen, Karen Blase, Allison Metz. Van Dyke Melissa. State‑
wide implementation of evidence‑based programs. Except Child. 2013;79(2):213–30.
16. Metz A, Bartley L. Active implementation frameworks for program success: how to use implementation science to improve outcomes for children. Zero Three. 2012;32(4):11–8.
17. Blanchard C, Livet M, Ward C, Sorge L, Sorensen TD, McClurg MR. The active implementation frameworks: a roadmap for advancing implemen‑ tation of comprehensive medication management in primary care. Res Social Adm Pharm. 2017;13(5):922–9.
18. Zainal Z. Case study as a research method. J Kemanusi. 2007;9:1–6. 19. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol.
2006;3(2):77–101.
20. National Implementation Research Network (NIRN). National implemen‑ tation research network’s active implementation hub—usable innova‑ tions. University of North Carolina at Chapel Hill’s FPG Child Development Institute; 2016. http://imple menta tion.fpg.unc.edu/modul e‑1/usabl
e‑innov ation s. Accessed 15 June 2016.
21. National Implementation Research Network (NIRN). National implemen‑ tation research network’s active implementation hub‑implementation drivers. University of North Carolina at Chapel Hill’s FPG Child Develop‑ ment Institute; 2016. http://imple menta tion.fpg.unc.edu/modul e‑1/
imple menta tion‑drive rs. Accessed 15 June 2016.
22. Blase K, Fixsen D, Van Dyke M, Duda M. Implementation drivers: best‑ practices for coaching. Chapel Hill: National Implementation Research Network; 2010.
23. National Implementation Research Network (NIRN). National implemen‑ tation research network’s active implementation hub‑improvement cycles. University of North Carolina at Chapel Hill’s FPG Child Develop‑ ment Institute; 2016. http://imple menta tion.fpg.unc.edu/modul e‑1/
impro vemen t‑cycle s. Accessed 15 June 2016.