Abstract
Recurrence of colorectal cancer following surgical resection continues to be a major therapeutic
challenge. As local recurrence of the cancer may progress into metastatic disease, there is strong
interest in mitigating recurrence to improve patient survivability. Advancements in
radiotherapies, brachytherapy in particular, have shown promise in reducing the recurrence of
other types of cancer, such as those of the prostate. The large surface area, complex geometries
of colorectal tumors and their close proximity to solid organs, however, limit the use of such
radiotherapies. Therefore it may be beneficial to look toward other avenues of treatment to
reduce colorectal cancer recurrence. We hypothesized that a drug delivery device that can deliver
chemotherapeutics directly to the surgical resection margins will decrease recurrence. Here, we
demonstrate the fabrication of a drug delivery device with characteristics suitable for surgical
resection margins of the colon or rectum. Structural optimization led to the design of needles
engineered to withstand the shear forces present when driving the implant into the margins. The
dual-polymer composition confers the rigidity to pierce the tissue, but also the flexibility to
conform to the irregular surface geometries of the resection margins. As the device is fabricated
via the Continuous Liquid Interface Production additive manufacturing technique, the implant
may be customized to the patients’ unique resection margins for subsequent rapid manufacture
in-house. Furthermore, we show that the release rates of embedded compounds may be tuned
through varying polymer cross-link density. These results suggest that CLIP printed drug-eluting
Introduction
Colorectal cancer is the third most frequently diagnosed cancer and the third leading
cause of cancer-related death of both men and women in the United States.1 Despite modern
advancements in colorectal cancer treatment, local recurrence (LR) remains a significant
therapeutic challenge in up to 30% of resection patients.2 – 4 LR following resection of colorectal
cancer is associated with a poor prognosis; median survival of 11 – 15 months and a 5-year
survival rate less than 5%.5 As LR may evolve into distant metastases, strategies to control LR
may reduce metastatic progression and thus improve patient survival.6
In the past, reduced LR rates have been achieved through the refinement of resection
technique and development of chemoradiotherapy (CRT) treatments.7,8 Notably, the addition of
intraoperative radiation therapy (IORT) to either preoperative or postoperative CRT has shown
to decrease rates of LR in those with locally advanced rectal cancer.9 Intraoperative
brachytherapy, a form of IORT involving embedded radioactive seeds in or near the tumor, has
been integrated into the conventional multimodal treatment for a variety of tumors, including
those of the prostate, oropharynx, rectum and cervix. Unfortunately conventional brachytherapy
is not always feasible in colorectal cancer as large surface area, complex-geometry tumors can be
difficult to adequately irradiate.10 Additionally the use of radiotherapy in the abdominal viscera is
limited as the small bowels and solid organs are especially susceptible to radiation damage.11,12
Therefore it may be beneficial to look to other avenues of treatment to reduce local recurrence.
Localized delivery of chemotherapeutics may prove advantageous for reducing LR in
colorectal cancer. Controlled release systems (CRS) are of particular interest as they allow for
the localized drug delivery over a set amount of time.13,14 Typically drugs are loaded into a
these characteristics, clinicians could supply large dosages of chemotherapeutic directly to
resection margins for prolonged periods. The unique curvature of rectal or colon resection
margins, however, make the design of a universal implant infeasible. Recent advancements in
additive manufacturing techniques may be the solution to this problem.
Continuous liquid interface production (CLIP) has revolutionized conventional fusion
deposition three-dimensional printing. As CLIP utilizes ultraviolet light to photopolymerize the
monomer resin, resolution can be achieved on the micrometer scale and printed objects are
mechanically isotropic.16 Drugs may be mixed into the resin and incorporated into the
photopolymerized matrix, thus forming a CRS. Additionally, CLIP has been shown to work at
operating speeds of 500mm/hour in comparison to fusion deposition operating as slow as
5-50mm/hour depending on the width of the part. Using CLIP, personalized drug-loaded implants
could be rapidly manufactured in-house.
This study sought to design and optimize drug-loaded CLIP-printed implants for reducing
colorectal recurrence. We hypothesize that implants loaded with taxanes and platinum based
chemotherapeutics will help to control recurrence in the surgical margins. Taxol and platinum
combination treatments are the most commonly utilized cancer regimen.17 This research could
lead to significant changes in conventional colorectal tumor treatment by improving local
Materials and Methods Implant Design
The three-dimensional structure of the implant was modeled in Solidworks according to
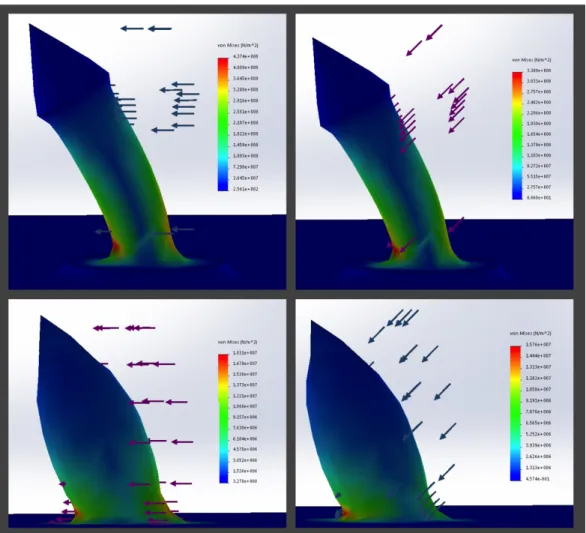
physician dimensional guidelines. Force analysis simulations were utilized to extrapolate the
maximum von Mises stresses due to shear forces acting on the drug-loaded needles. Said shear
forces (1 Newton in magnitude) were first placed perpendicular to, and next placed 135° from
the needle-pointing direction. The implants structure was optimized through successive
modifications that minimized the maximum von Mises stress. Using the application Slic3r, the
model was subsequently converted from stereolithography format to 10 µm thick G-code layers.
Synthesis of poly-ε-caprolactone dimethacrylate (PCL-diMAc) macromer
Poly-ε-caprolactone (PCL) diol (102 g, 192.5 mmol) was added to a 2-neck round bottom flask
and dried in a vacuum oven. The reaction flask was equipped with an addition funnel, sealed
with rubber septa, and placed under magnetic stirring and N2 flow. Anhydrous dichloromethane
(DCM, 310mL) and triethyamine (TEA, 445 mmol) was added and the flask was placed in an ice
bath. A 10% molar excess of methacryloyl chloride (MAcCl, 420 mmol) in 200mL DCM was
added dropwise from the addition funnel over the course of 1.5 hours and the reaction was
allowed to proceed for an additional 3 hours. The formed TEA•HCl salt was filtered off and
filtrate diluted 3-fold with DCM, washed three times with NaCl solution and three times with DI
water. The organic layer was collected, dried over magnesium sulfate and filtered. DCM was
removed under reduced pressure on a rotary evaporator and the remaining DCM was removed in
a vacuum oven at 35°C. Degree of functionalization and reaction progress was monitored by 1H
Continuous Light Interface Production Printing of Implant
The implant was synthesized by the CLIP photopolymerization method.16 A digital
light-processing unit projected 370 nm ultraviolet (UV) images of the implant in G-code form. These
images were incident onto an amorphous fluoropolymer window (Teflon AF 2400) that is
permeable to oxygen, transparent to UV light, and chemically inert. The photopolymerizable
resins were placed atop of this window; 770 MW polyethylene glycol (PEG) dimethacrylate was
bought from Sigma-Aldrich and the PCL dimethacrylate was synthesized in lab (see above).
Diphenyl(2,4,6–trimethylbenzoyl)phosphine oxide (0.9 mole percent) was utilized as a
photoinitiator for the radical polymerization reaction. A controlled oxygen inhibition layer
quenched the excited photoinitiators up to 50 µm above the window, thus stopping all radical
photopolymerization up to this point. Just above this dead zone, the curing part is drawn from the
resin bath while new layers of polymer are added continuously. Implants were printed at a speed
of 60 mm/Hr. PEG dimethacrylate resin composed the flexible base layer of the implant, while
PCL dimethacrylate composed the drug-eluting needles. The implant was photographed via light
microscopy with a Zeiss AxioCam mRr microscope.
Rhodamine Release from Needles
Rhodamine dye was added (0.5% w/v) to the PCL dimethacrylate resin prior to printing. Varying
UV light intensity, three rhodamine-containing implants were synthesized, each having a
different PCL dimethacrylate cross-link density. Said light intensities were 7.617, 9.375 and
11.719 mW/cm2. The implants were embedded into 2mm thick layers of agarose gel (23% w/v).
The agarose plates were placed into an incubator at 37° C. Rhodamine diffusion was monitored
Results
Structural optimization
Finite element stress simulations returned color maps depicting the surface von Mises stress
resulting from a uniformly distributed 1 N shear force on both the original and optimized implant
designs (Fig. 1). The maximum von Mises stresses of the original implant were at least an order
of magnitude higher than those of the optimized implant. Maximum von Mises stresses for the
original implant design were 4.374×108 and 3.309×108 N/m2 for shear forces positioned 90° and
135° from the needlepointing direction. The optimized implant, however, held maximum von
Mises stresses of 1.831×107 and 1.576×107 for 90° and 135° shear forces. In total, design
optimization achieved 95.8 and 95.2% reductions in maximum von Mises stress. Furthermore,
the original design experiences von Mises stresses comparable to the optimized design’s
maximal stress throughout the faces anterior and posterior to the applied shear force.
Chemical characterization of poly-ε-caprolactone dimethacrylate resin
The 1H– NMR spectral analysis of the PCL-dimethacrylate resin is shown in Fig. 2. The peaks at
6.08, 5.29 and 1.93 ppm correspond to the Hydrogen atoms located within the methacrylate
group, thus confirming methacrylate functionalization of poly-ε-caprolactone’s hydroxyl groups.
By comparing the integrated area of said peaks to known peak (4.08 ppm) of the PCL backbone,
Implant Synthesis
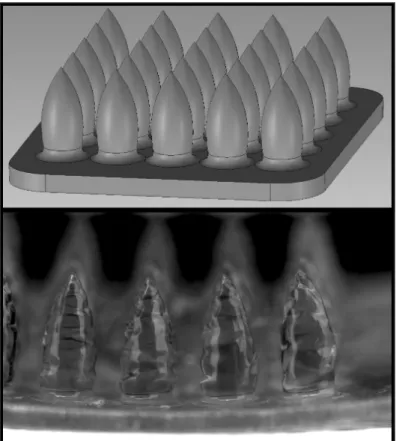
The final implant design and light microscopy (Zeiss Axio Cam mRr) of a fabricated implant
may be viewed in Fig. 3. While the overall shape of the implant resembles that of the design,
there are notable structural deviations. First of all, the resolution is lower than expected, leaving
a fairly blunted tip to the needle. Next, the surface of the needle is not smooth but rather has
rounded invaginations at regularly spaced intervals. A reduction in the thickness of the PEG
baseplate from 1 mm to 400 µm enhanced baseplate flexibility. Supplementary figure 1 depicts
baseplate elasticity unachievable with the thicker 1mm baseplate due to fracturing.
Rhodamine Release
Visualization of the rhodamine dye release from the needles is shown one and six hours after
implantation into 23 (w/v) agarose (Fig. 4). For the first hour, it appears as if rhodamine release
holds a positive relation to UV polymerization intensity. This is a counterintuitive result as
greater cross-linking density is typically associated with slower release rates.15 After six hours,
however, the implant printed with 9.375 mW/cm2 intensity light surpassed the release rates of
F100 shown by an augmented diffusional spread. In relation to the others, the 7.617 mW/cm2
Discussion
Despite advancements in the treatment of colorectal cancer, local recurrence (LR)
remains a significant therapeutic challenge. As LR may progress into distant metastases, there is
a strong interest in mitigating LR as a way to improve patient survivability. We hypothesized
that a drug delivery device that can deliver chemotherapeutics to the surgical resection margins
will decrease cancer recurrence. We have demonstrated the fabrication of a novel intraoperative
device, capable of eluting embedded compounds at a tunable rate. Furthermore, its
biodegradable, dual-polymer composition gives rise to properties suitable for permanent
placement into the surgical margins. The PEG baseplate allows the implant to conform to the
complex surface geometries of the resection margins, while the PCL confers the needle rigidity
necessary to pierce into tissue. These needles were structurally optimized to maximize resistance
to shear force, thus ensuring that the needles will drive straight into the tissue without deviating
to or away from each other. With the addition of methacrylate functional groups to these
polymers, the implant may be fabricated via the CLIP additive manufacturing technique.
Therefore implant designs could be personalized to the patient’s unique tumor geometry using
CT scans, and subsequently manufactured rapidly in-house. These results suggest that CLIP
printed drug delivery devices hold potential for clinical translation in colorectal cancer treatment.
Before translation to the clinic, however, there are a few obstacles.
First of all, the irregular surface invaginations seen in Fig. 3 may be resulting from
overexposure. If the resin above the oxygen inhibition layer is overexposed, it can polymerize all
the way to the translucent window. This layer will remain attached to the window until the force
of the stepper motor removing the object overcomes this attachment force. At this point, the
the object that is severely underexposed to UV. A reduced UV intensity may limit overexposure,
but would do so at the cost of reducing print speed. Next, drug release rates are to be precisely
quantified. This will be accomplished by placing docetaxol-loaded implants into agarose gel, and
later removing concentric disks of gel from around the implant for HPLC analysis. After the
characterization of release rates, the implant’s in vivo efficacy at mitigating recurrence will be
examined with mouse xenograft models of the human colorectal cancer cell line HT29.
Subcutaneous tumor xenografts will be removed via blunt resection aseptic surgical techniques.
The HT29 cell line will be transfected with luciferase, thus giving a quantitative metric to track
Figures
Fig. 1. Finite element stress simulation of the original and optimized implants
Fig. 3. Computer model and light microscopy of fabricated implant
References
1. Siegel R, DeSantis C, Ahmedin D. (2014). Colorectal cancer statistics, 2014. Ca : A Cancer Journal for Clinicians, 64(2), 104.
2. Scholefield JH, Steele RJ. Guidelines for follow up after resection of colorectal cancer. Gut. 2002;51(5):v3–v5.
3. Amitai MM, Fidder H, Avidan B, et al. Contrast-enhanced CT colonography with 64-slice MDCT compared to endoscopic colonoscopy in the follow-up of patients after colorectal cancer resection.
Clinical Imaging. 2009;33(6):433–438.
4. Kobayashi H, Mochizuki H, Sugihara K, et al. Characteristics of recurrence and surveillance tools after curative resection for colorectal cancer: a multicenter study. Surgery. 2007;141(1):67–75.
5. Lybeert ML, Martijn H, Neve W, Crommelin MA, Ribot JG. (1992) Radiotherapy for locoregional relapses of rectal carcinoma after initial radical surgery: definite but limited influence on relapse-free survival and survival. Int J Radiat Oncol Biol Phys. 24(2):241–246
6. McDermott FT, Hughes ES, Pihl E, Johnson WR, Price AB. Local recurrence after potentially curative resection for rectal cancer in a series of 1008 patients. Br J Surg. 1985; 72:34–37.
7. Stewart SL, Wike JM, Kato I, Lewis DR, Michaud F. A population-based study of colorectal cancer histology in the United States, 1998-20 01. Cancer. 2006;107: 1128-1141.
8. Moriya Y (2006) Treatment strategy for locally recurrent rectal cancer. Jpn J Clin Oncol 36:127–131
9. Kang MK, Kim MS, Kim JH. Intraoperative Radiotherapy for Locally Advanced Rectal Cancer.
Journal of the Korean Society of Coloproctology. 2010;26(4):274-278. doi:10.3393/jksc.2010.26.4.274.
10. Harrison L, Enker W. High-Dose-Rate Intraoperative Radiation Therapy For Colorectal Cancer.
Oncology 1995. 9(8):737-41.
11. Kuehne J, Kleisli T, Biernacki P, et al. Use of high dose rate brachytherapy in the management of locally recurrent rectal cancer. Dis Colon Rectum 2003;46:895–899
12. Rodel C, Grabenbauer G, Matzel K, et al. Extensive surgery after high dose preoperative chemoradiotherapy for locally advanced recurrent rectal cancer. Dis Colon Rectum 2000;43:312– 319.
13. Brown L, Wei C, Langer R. In vivo and in vitro release of macromolecules from polymeric drug delivery systems. J. Pharm. Sci. 1983. 72, 1181-1185
14. Mansour H, Sohn M, Al-Ghananeem, DeLuca P. Materials for Pharmaceutical Dosage Forms: Molecular Pharmaceutics and Controlled Release Drug Delivery Aspects. Int J Mol Sci 2010. 11: 3298-3322.
16. Tumbleston J, Shirvanyants D, Ermoshkin N, Janusziewicz R, Johnson A, Kelly D, Chen K, Pinschmidt R, Rolland J, Ermoshkin A, Samilski E, Desimone J. Continuous liquid interface production of 3D objects. Science 2015. 347(6228): 1349-1352.
17. Du X, Parikh R, Lairson D, Giordano S, Cen P. Comparative effectiveness of platinum-based
chemotherapy versus taxane and other regimens for ovarian cancer. Medical Oncology 2013. 30:440.
Supplementary Materials