Jacobs Journal of Medical Diagnosis and Medical Imaging
Development and Testing of a Hybrid Synthetic-Biologic Phantom for the
Optimization of Mr Sequences for Articular Cartilage
Alessandro Marinetti1, Francesco Tessarolo2,3*, Alessandro Cristoforetti4,Fabrizio Cortese5, Sabino Walter Della Sala1 1Division of Diagnostic Radiology, Rovereto Hospital, Azienda Provinciale per i Servizi Sanitari, Trento, Italy
2Department of Industrial Engineering, University of Trento, Trento, Italy
3Healthcare Research and Innovation Program (IRCS-FBK-PAT), Bruno Kessler Foundation, Trento, Italy 4Department of Physics o University of Trento, Trento, Italy
5Division of Orthopaedics and Traumatology, Rovereto Hospital, Azienda Provinciale per i Servizi Sanitari, Trento, Italy
*Corresponding author: Dr. Francesco Tessarolo, PhD Healthcare Research and Innovation Program (IRCS-FBK-PAT), BRUNO KES-SLER FOUNDATION & Department of Industrial Engineering, University Of Trento via delle Regole, 101I-38123 Mattarello Tren-to-Italy. Phone: +39 0461 282775; Fax: +39 0461 283659 E-mail: [email protected]
Received: 10-18-2018
Accepted: 11-05-2018
Published: 11-08-2018
Copyright: © 2018Francesco Tessarolo
Abstract
Purpose
To develop and validate a hybrid phantom for optimizing MRI sequences of knee articular cartilage.
Methods
in-vivo
MR study of the knee was performed in two patients prior to total knee arthroplasty ( MR). Osteochondral surgical re-sections of femur and tibia were used to set-up a phantom consisting in a transparent polyethylene box filled with echographic gel. Phantom assemblage and in-vitro MRI was performed in one patient within 20 minutes after surgery (fresh MR) and, for the other patient, after having preserved the tissues in formalin for 12 months (post-fixation MR).
Morphological sequences (SE T1-weighted, DESS, TRUFI 3D) and compositional maps (SE T2, GR T2*) were obtained on sagittal plane. Phantom was validated by comparing MR data obtained in-vivo and in-vitro. Comparison of data obtained from fresh and fixed tissues allowed also to assess modifications in MR signal due to formalin preservation.
Results
MR imaging in-vitro allowed the evaluation of the whole articular surface of the femoral condyles and tibial plateau. Excellent concordance existed between in-vivo and in-vitro cartilage morphology in T1-weighted images. DESS and TRUFI 3D sequences showed limitations for in-vitro MR imaging because of their sensitivity to magnetic field inhomogeneities. Formalin fixation pre-served tissue morphology and T2 relaxation times of the chondral tissue.
Conclusions
The proposed hybrid synthetic-biologic phantom allowed obtaining in-vitro MR data super-imposable to in-vivo data for both fresh and formalin-fixed tissues, proving its usability for the optimization of knee cartilage MRI.
Keywords: Magnetic Resonance Imaging; T2 mapping; Cartilage; Phantom Research Article
old female, case B: 74 year old male). Both of them were sched-uled for total knee arthroplasty (TKA) because of advanced knee osteoarthritis without a history of rheumatoid arthritis or other joint-related infection. The study has been approved by the local Ethics Committee and patients gave informed con-sent.
In vivo MRI study of the knee cartilage was performed 12 hours prior to surgery (in-vivo MRI) on a 1.5 T scanner (Mag-netom Aera®, Siemens Medical Systems, Erlangen, Germany). Sagittal images for morphological tissue evaluation were col-lected with spin echo (SE) T1-weighted (TE 12 ms, TR 500 ms THK 3 mm) dual echo steady state (DESS) (TE 7 ms, TR 19 ms, FA 25, THK 2 mm) and three dimensional true fast imaging with steady-state free precession (TRUFI 3D) (TE 4 ms, TR 10 ms, FA 28, THK 0.7 mm) sequences. Compositional mapping were obtained from SE T2 (5 echoes at TE at 13.8, 27.6, 41.4, 55.2, 69.0 ms, TR 1030 ms, THK 3 mm) and GR T2* (5 echoes at TE 4.2, 11.3, 18.5, 25.6, 32.7 ms, TR 420, FA 60, THK 3 mm) sequences.
Figure 1. Cartilage specimen collection from patients A undergoing
TKA. a) Surgical field showing severe cartilage degeneration especial -ly in the medial compartment of the knee. b) The seven osteochon-dral fragments obtained from surgery. From top to bottom: anterior central and posterior condyle fragments and tibial plate immediately after resection.
Both patients underwent total knee arthroplasty, where the seven osteochondral fragments (anterior medial and lateral condyle, central medial and lateral condyle, posterior medial and lateral condyle, tibial plateau) were collected (Figure 1),
and identified for anatomical orientation adapting the method
proposed by Li et al [9]. Case A fragments were washed from blood excess with sterile saline and preserved by immersion Abbreviations
MR: Magnetic Resonance;
MRI: Magnetic Resonance Imaging; 3D: Three-Dimensional;
TKA: Total Knee Arthroplasty; SE: Spin Echo;
TSE: Turbo Spin Echo; GR: Gradient Echo;
DESS: Dual Echo Steady State;
TRUFI: True Fast Imaging With Steady-State Free Precession; TR: Time Of Repetition;
TE: Time Of Echo; FA: Flip Angle; THK: Slice Thickness
Introduction
Magnetic resonance imaging (MRI) has proved to be an effec-tive non-invasive diagnostic tool in the assessment of articular cartilage [1,2]. Accuracy of cartilage MRI has been improved in
the last decade by developing cartilage specific sequences. The
use of high-field magnetic resonance (MR) scanners with in
-creased signal-to-noise ratio, allowed increasing spatial reso-lution and acquisition times [3-5]. Moreover, the development of new imaging techniques such as three-dimensional (3D) acquisition and spectral fat suppression [6] further increased diagnostic values of MRI.
More recently, specific MRI imaging relaxation protocols for
articular cartilage mapping allowed to delineate and quantify early stage alterations related to the macromolecular structure
of the cartilage (T2, T2*and T1ρ mapping) [6,7]. Indeed, com
-positional MRI reveals biochemical and microstructural chang-es in cartilage before morphologic alterations are detectable [8]. However, the optimization of sequence parameters and the validation process required to assess the diagnostic reliability of these MRI protocols are needed before their introduction in the diagnostic routine. Since optimization and validation processes are excessively time consuming to be executed on patients in vivo, there is the need for reliable phantoms able to represent properly the complex morphology and chemical composition of the articular cartilage.
This study aimed at developing and validating a hybrid phan-tom, composed by synthetic components and biological tissue, to be used in the optimization of MRI protocols for the mor-phological and structural evaluation of the knee articular car-tilage.
Materials And Methods
Patients and MRI protocol
Two patients have been enrolled for this study (case A: 67 year
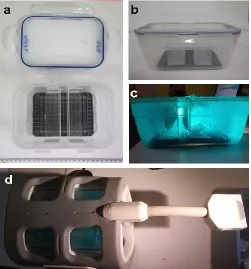
teochondral fragments. b) Side view of the phantom in the closed configuration before gel filling. c) Side view of the complete phantom with gel and osteochondral fragments obtained from TKA. d) Top view of the complete phantom inside the MR coil just before insertion into the scanner.
MR data processing for map reconstruction
T2 maps were reconstructed with a software specifically de
-veloped on Matlab programming platform, by using the
se-quence of five spin-echo magnitude images Miacquired at echo
times TEi ranging from 13.8 to 69.0 ms. A noise bias correction scheme for low signal-to-noise ratio MR images, adapted from the method proposed by McGibney and Smith [10] and Miller and Joseph [11], was employed. Assuming a Rician distribu-tion of noise, the unbiased estimate of the power signal
was computed, where the noise variance σ was estimated as
the second order moment on a sample in a background region (air) of the image:
The model for the power signal decay was then
fitted on the Pi sequence, finding the optimal A0 and T2 values
that minimize the sum of square errors, under the constraints of positive A0 and T2. The minimization was performed by a fast
dyadic progressive refinement search, overcoming the caveats
that small, or even negative, Pi values could pose to the conven-tional log-linear interpolation. A similar approach was applied to obtain T2* maps.
Phantom validation
Phantom was validated by comparing MR data of the same knee osteochondral tissue obtained in patient before TKA sur-gery (in-vivo) and in the phantom (in-vitro). Moreover, com-parison of data obtained from in-vitro MRI of case A and case
B, representative for formalin-fixed and fresh tissues respec
-tively, allowed to assess any alteration to MR signal due to
al-dehydic fixation and prolonged storage time before phantom
set-up.
The following aspects were considered for the evaluation of the in vivo and in vitro images:
1) Correct identification of the most significant anatomical
sites (lateral and medial tibial articular surface and tibial spine morphology).
2) Morphological damage grading according to semi-quanti-tative scale (0: normal cartilage, 1: cartilage signal inhomo-geneities with preserved tissue thickness, 2: cartilage tissue loss <50%, 3: cartilage tissue loss >50%, 4: exposition of sub-chondhral bone).
3) Consistency of color-coded maps of T2 and T2* relaxation in 10% formalin buffered solution. Case B fragments were
washed and kept hydrated by using sterile saline moistened gauze in a plastic airtight container. Collected fragments were then used in setting-up the hybrid synthetic-biologic phantom as reported below.
Phantom set-up
The phantom consisted of a 1.8 L transparent polyethylene box
filled with echographic gel (Cogel Ultrasound, Comedical, Ita
-ly). A calibration squared grid was placed on the bottom of the container. Moreover, two “L” shaped polypropylene supports were installed for positioning the biological phantom compo-nents according to knee anatomy (Figure 2a and 2b). All osteo-chondral tissue fragments obtained from a single patient were
fitted in the gel taking care of reproducing in-vivo orientation
(Figure 2c). The phantom was completed by sealing the con-tainer with an airtight lid.
Phantom assemblage and MRI was perform 12 months after
surgery for formalin-preserved case A fragments (fixed tis
-sues), and 20 minutes after surgery for case B fragments (fresh tissues).
In-vitro MR data were acquired by scanning the above-de-scribed phantom with same imaging protocols used for the in vivo imaging. Positioning of the phantom within the MR scan-ner was realized to emulate patient’s knee orientation (Figure 2d).
Figure 2. Phantom components and set-up. a) Top view of the
os-the subchondral bone was found on os-the medial compartment and on the posterior part of the lateral condyle. This feature was obvious at the gross pathology analysis of the lateral con-dyle fragments (Figure 4c). From the in-vitro MR images, a
chondral elevated flap was recognized in between the central
and posterior lateral condyle that was put on evidence during the surgical resection of the osteochondral samples (Figure 4b). This detail was not evident at the in-vivo MR analysis (Fig-ure 4a).
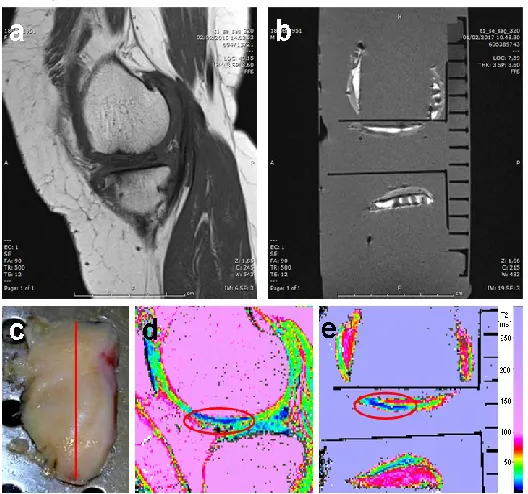
Figure 3. Case A: comparative evaluation between in-vivo (a
and d) and in-vitro formalin-fixed tissue (b and e). The macro
-scopic inspection of the surgical fragment (c) showed that the cartilage thickness is preserved but a discoloration is present in the central and anterior portion. T1 weighted images (a and b) and reconstructed T2 maps (d and e) refers to the imaging plane indicated by the red straight line on the tissue fragment in the macrophotography (c).
Bone cavities due to sampling with Jamshidi needle to evaluate tissue thickness are visible in (c) Red circles (d and e) indicate areas in the cartilage showing a variation in the relaxation time T2 both for in-vivo and in-vitro.
Images obtained in-vitro with DESS and TRUFI 3D sequences showed relevant limitations for the proper morphological eval-uation of the cartilage surface because of their sensitivity to
magnetic field inhomogeneity. This could be related to metallic
debris released by the surgical procedure or to the presence of small air bubbles within the phantom gel. It is therefore of the
uttermost importance to avoid bubble formation when fitting
osteochondral fragments in the phantom gel. Cartilage surface should be deeply scrutinized before imaging the phantom and air bubbles should be removed.
times.
The evaluation was performed blindly by two radiologists with expertise in musculoskeletal RM imaging and inter-observer agreement was assessed.
Results And Discussion
The viscosity of the gel and the optical clarity of the polymeric components used in the phantom facilitated the spatial posi-tioning of the full set of osteochondral fragments emulating their anatomical location.
The correct anatomical orientation was evaluated by recogniz-ing the anatomy of the tibial articular surface on in-vitro MR
images and, more specifically, by discriminating the convexi
-ty of the lateral tibial plateau and the planari-ty of the medial tibial plateau. Moreover, morphology of tibial spine was also checked for consistency between in-vivo and in-vitro collected MR images. According to both radiologists, excellent concor-dance existed between the in-vivo anatomical morphology of the knee articular knee surfaces and the in-vitro correspond-ing reconstructed anatomy (Figure 3a and 3b, Figure 4a and 4b). A minor discrepancy was observed in the latero-lateral alignment of the condyles with respect to the tibial fragments within the phantom due to lack of anatomical links (cruciate ligaments) between fragments that were removed during TKA surgery.
The in-vitro MR imaging within the phantom allowed the eval-uation of the whole articular surface of femoral condyles and tibial plateau, with the only exception of the trochlear groove region, which is not usually integrally available in the resection material during TKA.
Inter-observer agreement between radiologists was very strong for both location and grading of chondral lesion in the tissue imaged in-vivo and in-vitro. MR findings were also con
-firmed by evaluating the gross pathology aspects of the osteo
-chondral fragment by an independent researcher (Figure 3c and Figure 4c).
In case A, the thickness of the cartilage was preserved in the lateral compartment and markedly reduced in the medial com-partment. Focusing on the lateral compartment, the anterior portion of the condyle cartilage showed a diffuse hypointense tissue signal in T1 weighted images (Figures 3a and 3b) with a corresponding alteration of the values of the T2 relaxation time in the T2 maps (blue area in Figure 3d and 3e). The corre-sponding area evaluated by gross pathology showed the pres-ervation of the cartilage surface integrity and thickness (eval-uated by obtaining several osteochondral sample by a 2.5 mm Jamshidi needle), but a loss of the hyaline aspect typical of the healthy cartilage (Figure 3c) was also present.
In case B, a complete erosion or the cartilage with exposition of
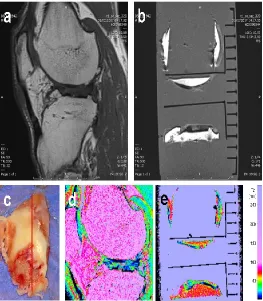
Figure 4. Case B: comparative evaluation between in-vivo (a and d) in-vitro
and fresh tissues (b and e). The macroscopic inspection of the surgical fragment (c) showed the preservation of the cartilage thick-ness in the anterior portion of the lateral condyle but a variation in the intensity of the MR signal is in accordance with the discoloration of the tissue. In the central portion, the cartilage delamination visi-ble at the macroscopic inspection of the fragment (c) is more evident
in-vitro (b) than in-vivo (a). Clearly T1 weighted images (a and b) and
reconstructed T2 maps (d and e) refers to the imaging plane indicated by the red straight line on the tissue fragment in the macrophotogra-phy (c).
The qualitative and quantitative comparison of relaxation time in T2 maps obtained from in-vitro MR imaging (Figures 3e and 4e) were found spatially and quantitatively equivalent to those realized in-vivo (Figures 3d and 4d). As an example, the varia-tion of the relaxavaria-tion time T2 found in the cartilage of the ante-rior portion of the lateral condyle in case A in-vivo (Figure 3d) presented the same features in-vitro (Figure 3e).
Similarly to DESS and T2 TRUFI 3D sequences, T2* mapping of the tissues in-vitro resulted severely limited by sensitivity of
T2* images to local field inhomogeneity.
MRI of in-vitro fresh and formalin-preserved fragments re-sulted in similar morphology and composition (T2 relaxation times) of the chondral tissue. Minor variations in the relax-ation times were present for the bone tissue in-vitro,
especial-ly when formalin fixation was performed (case A). However,
these variations did not interfere with the evaluation of T2 map for chondral tissue. Taking these results into consider-ation, it seems feasible and reliable to realize the phantom
with osteochondral tissue fragments fixed in formalin after a
medium-long period of storage (several months), preserving the quality of the MR signal for both morphological and com-positional analysis. However, considering that this explorative feasibility study has been conducted on a limited number of subjects, further research should be provided to support these preliminary data.
One of the major advantages of the phantom here described is the large availability of the osteochondral resections due to the increasing number of TKA in the last years that facilitate the possibility of realizing a number of phantoms with different chondral characteristics both in term of morphology and com-position (relaxation times). Previous studies using osteochon-dral resection obtained from TKA were limited by the need of analyzing only fresh tissue [9,12]. Our data indicate that
for-malin fixed tissues has equivalent morphological character
-istics to fresh tissue and T2 relaxation times for the chondral
tissue are sufficiently preserved.
Conclusions
In a summary, the study showed a good correspondence be-tween MR data obtained by using the proposed hybrid synthet-ic-biologic phantom and the in-vivo results, giving equivalent information about both the knee articular cartilage morpholo-gy and composition. The phantom can be therefore considered
as a valid tool for the optimization of specific MR sequences for
the articular knee cartilage.
Acknowledgments
Authors are grateful to the technical staff of the Division of Di-agnostic Radiology at Rovereto Hospital for assistance in col-lecting MR data.
Financial support
The study has been supported in part by the Healthcare Re-search and Innovation Program (IRCS) of the Autonomous Province of Trento.
Competing interest
The authors declare that they have no competing interests.
References
1. Recht M, Bobic V, Burstein D, Disler D, Gold G, Gray M et al. Magnetic resonance imaging of articular cartilage. Clin Orthop Relat Res. 2001, 391:S379–396.
2. Recht MP, Goodwin DW, Winalski CS, White LM. MRI of artic-ular cartilage: revisiting current status and future directions. AJR Am J Roentgenol. 2005,185:899–914.
3. Link T, Stahl R, Woertler K. Cartilage imaging:
motiva-tion, techniques, current and future significance. Eur Radiol.
2007,17:1135–1146.
4. Gold G, Chen C, Koo S, Hargreaves B, Bangerter N. Recent advances in MRI of articular cartilage. AJR Am J Roentgenol. 2009,193:628–638.
5. Burstein D, Gray M, Mosher T, Dardzinski B. Measures of mo-lecular composition and structure in osteoarthritis. Radiol Clin North Am. 2009,47: 675–686.
6. Crema MD, Roemer FW, Marra MD, Burstein D, Gold GE, Eck-stein F et al. Articular cartilage in the knee: current MR im-aging techniques and applications in clinical practice and re-search. Radiographics. 2011,31(1): 37-61.
7. Kijowski R, Blankenbaker DG, Munoz Del Rio A, Baer GS, Graf BK. Evaluation of the articular cartilage of the knee joint: value of adding a T2 mapping sequence to a routine MR imaging pro-tocol. Radiology. 2013, 267(2): 503-513.
8. Roemer FW, Kijowski R, Guermazi A. Editorial: from theory to practice - the challenges of compositional MRI in osteoar-thritis research. Osteoarosteoar-thritis Cartilage. 2017, 25(12) 1923-1925.
9. Li X, Cheng J, Lin K, Saadat E, Bolbos RI, Jobke B et al.
Quanti-tative MRI using T1ρ and T2 in human osteoarthritic cartilage
specimens: correlation with biochemical measurements and histology. Magn Reson Imaging. 2011,29(3): 324-334.
10. McGibney G, Smith MR. An unbiased signal-to-noise ra-tio measure for magnetic resonance images. Med Phys. 1993, 20(4): 1077-1078.
11. Miller AJ, Joseph PM. The use of power images to perform quantitative analysis on low SNR MR images. Magn Reson Im-aging. 1993,11(7):1051-1056.