CrossMark
Published by DiscoverSys
ABSTRACT
Background: Urethral duplication is a rare congenital malformation mainly affecting men and boys. Although a number of theories have been proposed to describe this condition, the actual mechanism of this disorder is still not clear. The most frequent anomaly occurs in the sagittal plane, in which the duplicated urethra is in either dorsal or ventral position in relation to the orthotopic urethra. The therapeutic management of these conditions is complicated and depends on the presence of symptoms as well as the type of anomaly.
Case Description: We present a case of urethral duplication in a 2 years old male child. The malformation was characterised by the presence of the meatus in the dorsal penoscrotal and accompanied by the sign of infection in it. Urethrography showed contrast
stopped filling 2 cm from the meatus in the dorsal penoscrotal with a total dead-end impression as an accessory urethra and there was no abnormalities in the principal urethra looked from the contrast filled the penile urethra, bulbous urethra, prostatic urethra, and bladder. That was the form of Effmann Type IA urethral duplication. The dorsal accessory urethra was excised entirely without complication and he remains symptom-free eight months after surgery.
Conclusion: In summary, urethral duplication is a rare clinical condition. It has many variants that were classified by Effman. Management depends on the anatomy of the duplication involved and the patient’s clinical symptoms.
Keywords: Double urethra, urethral duplication, Effman’s classification, reconstructive surgery.
Cite This Article: Adityagama, M., Hutasoit, Y.I. 2019. Type IA urethral duplication: A case report. Bali Medical Journal 8(3): 587-591. DOI:10.15562/bmj.v8i3.1602
Type IA urethral duplication: A case report
Miftah Adityagama,1 Yonas Immanuel Hutasoit2*
INTRODUCTION
The urethral duplication, also known as double urethra, is a rare anomaly occurring in pediatric cases, this deformity is most often found in male children while for female children it is very rare, with a previous literature recording no more than 40 cases of double urethra found in female chil-dren.1,2 The clinical entity comprised of a wide
spectrum with various anatomical variations. Thus, there are several classifications used in defining each case of double urethra or urethral duplication, such as the Effmann classification system.3 It can
be complete or incomplete, the majority of cases occur in the sagittal plane, further divided into dorsal and ventral duplication according to the position of the ectopic urethra. Collateral duplica-tion without bladder duplicaduplica-tion may also be found without accompanying bladder duplication. The relative rarity of the case combined with the wide spectrum of manifestation creates some difficulties in pinpointing the exact pathophysiological mech-anism. Several literatures had suggested that there were multiple mechanisms that may cause urethral duplication, each possibly related with different types of manifestation.1
Individually tailored management is required due to the spectrum above of clinical manifesta-tions in cases of urethral duplication.1,4 The general
consensus is, presently, to treat only symptomatic
patients. The treatment aims to preserve renal function, achieve continence, and achieve the best possible cosmetic outcome. The ventral part of the urethra is always the functioning urethra, complete with sphincters and the urinary bladder. Several methods may be used in obliterating the accessory channels, such as injection of sclerosing agent or other ablative interventions. The tech-niques, however, are slowly being abandoned due to the risk of corporeal thrombosis and fibrosis. Reconstruction by combining the ventral and accessory urethra parts may be utilized, although it carries a potential risk for meatal stenosis and obliteration of dorsal meatus. The current golden standard is surgical excision of dorsal accessory urethra. The procedure itself needs to be done delicately in order to avoid damage to the external sphincter and neurovascular bundle.1
CASE REPORT
A 2-years-old male patient was referred to urology polyclinic at Fatmawati General Hospital with the chief complaint there was whitish discharge from a hole in the dorsal penoscrotal. That condition has been realised by the parents since the last one month, but they have noticed the small hole in the dorsal penoscrotal since the patient was 3-months-old. Previously they took the patients 1Department of Urology, Faculty
of Medicine Universitas Indonesia, Cipto
2Mangunkusumo National General Hospital, Jakarta, Indonesia
2Department of Urology, Fatmawati General Hospital, Jakarta, Indonesia
*Correspondence to:
dr. Yonas Immanuel Hutasoit; Department of Urology, Fatmawati General Hospital, Jakarta, Indonesia;
Received: 2019-09-11 Accepted: 2019-10-10 Published: 2019-12-01
Volume No.: 8
Issue: 3
First page No.: 587
P-ISSN.2089-1180
E-ISSN.2302-2914
to a paediatrician because the patients were fussy when urinating and looked reddish around the hole then stated there was inflammation. There was no difficulty in urinating. Good emission of urine, not branched, and there was no urine comes out of a hole in the dorsal penoscrotal. There were no abnormalities in growth and development or other congenital abnormalities. From the physical examination we found a normal external urethral meatus on the tip of the glans penis (Figure 1a) and the second meatus with a diameter of 2 mm in the dorsal penoscrotal (Figure 1b). The two testicles were found normal.
During urethrography and urethroscopy exam-ination, it was obtained a meatus from the dorsal penoscrotal as long as 2 cm, a pinpoint hole and debris appeared, and the wire could not be inserted. Contrast stopped filling 2 cm from the meatus in the skin, with a total dead-end impression (Figure 2a). 7 Fr ureteroscopy sheath was inserted through the external urethral meatus on the tip of the glans penis; urethra, verumontanum, bladder neck and bladder were found normal. There were no holes along the urethra; the right and left uret-eral opening were identified. Contrast filled the penile urethra, bulbous urethra, prostatic urethra, and bladder. There was no stenosis and there were no tracts to another place (Figure 2b).
Patients had no other complaint besides a whit-ish discharge from a meatus in the dorsal peno-scrotal which is then followed by the presence of pain and redness around it. The patient was then planned for exploration and excision of the tract from the meatus in the dorsal penoscrotal.
Surgical Technique
Patient was positioned under general anaesthe-sia. The aseptic and antiseptic procedure was conducted at surgical site and the surrounding area. Evaluation of genitalia external was carried out; the external urethral meatus was located at the tip of glans penis, two testicles were found normal, and there was a second meatus at the dorsal penoscrotal.
Mattress stitch on glans penis using suturing thread prolene 4-0. Foley catheter 8 Fr was inserted at the opening of external urethral meatus at the tip of the glans penis. Circumglandular incision was made following marker and penile deglov-ing was conducted, identification of the dorsal tract (Figure 3a). The dorsal tract appears to the symphysis (Figure 3b). Excision of the dorsal tract and released up to the symphysis, obliteration of the tissue appeared (Figure 4). The tissue was sent to be
Figure 1 The normal external urethral meatus
(a) and the second meatus in the dorsal penoscrotal (b)
Figure 2 Urethrography showed contrast stopped
filling 2 cm from the meatus in the dor-sal penoscrotal, with a total dead-end impression (a), and contrast filled the penile urethra, bulbous urethra, pros-tatic urethra, and bladder (b)
Figure 3 Penile degloving and identification the
dorsal tract (a), the dorsal tract appears to the symphysis (b)
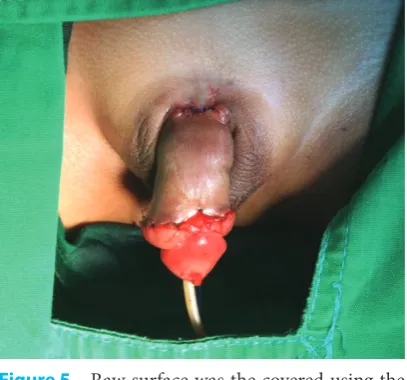
examined into the anatomical pathology laborato-rium. Raw surface was the covered using the byars flap technique with PDS 5-0 interrupted (Figure 5).
RESULT
The results of examination from anatomical pathol-ogy of the tissue shown a picture of the urethra with a chronic inflammatory reaction and no signs of malignancy appeared. Ten days after surgery (Figure 6), patient came back to our urology poly-clinic. Physical examination showed good surgical wound healing, there was no discharge from the surgical wound in the dorsal penoscrotal was found as before and there were no problems with voiding.
DISCUSSION
Double urethra or urethral duplication is a congen-ital disorder which rarely happens. Approximately 150 – 300 cases have been reported to date and is more frequently found in male children, with a previous literature recording no more than 40 cases of double urethra found in female children. This disorder is often associated with other abnormal-ities in the genitourinary tract, heart, bowel, and
bones.5 Arena et al.,6 found that in 60% of cases
is accompanied by genitourinary malformation such as ureteropelvic junction obstruction, extra rotation of the penis, vesicoureteral reflux, renal ectopia, renal agenesis, or posterior urethral valves. There was no additional abnormality in our patient.
Various theories have been proposed to explain the embryological development of urethral dupli-cation, including disorders of mesoderm develop-ment, abnormal Mullerian ducts, ischemia during embryogenesis, and defects in the development of the urogenital sinus.7–10 Casselman and Williams10
suggested that a partial failure or an irregularity of the ingrowth of the lateral mesoderm between the ectodermal and endodermal layers of the cloacal membrane in the midline accounts for the forms with a dorsal epispadias channel. Das and Brosman8 stated that abnormal termination of the
Mullerian duct was responsible for the development of urethral duplication. Rica et al.,11 reported that
asymmetry in the closure of the urorectal septum results in an urethra-perineal fistula.
There were a few anatomical variations of urethral duplication. Duplication may occur at bladder neck area or only affecting the distal part of the urethra.12,13 This disorder commonly occurs
on the sagittal section, with urethra on the dorsal part and ventral of penis. Ventral urethra is usually more functional as it has sphincter and verumon-tanum mechanisms. Urethral duplication rarely occurs on the coronal section.12–14 There are many
classifications used to categorise urethral duplica-tion. Gross and Moore classified urethral dupli-cation as a complete second passage originating from the bladder to the dorsum of the penis and or as an accessory pathway which is unfunctional that ends blindly on the dorsal or ventral surface. Williams and Kenawi15 categorised urethral
dupli-cation based on the ectopic lodupli-cation of the urethra compared to normal urethra. However, the most commonly used and accepted in this area recently is the Effmann classification. Effman categorised urethral duplication into three types. Type I is composed of incomplete with blind-ending and/ or accessory urethra, if the accessory urethra opens onto the dorsal or ventral surface of the penis with-out communicating with principal urethra or blad-der it is classified as type IA and classified as type IB when the accessory urethra emerges from principal urethra and terminates blindly within the periure-thral tissue. Type II duplication is complete patent urethral duplication with four subtypes, namely type IIA 1 when the second channel of the urethra arising independently from the bladder, type IIA 2 if the second channel arising from the first urethra and courses into a second meatus, when the second
Figure 5 Raw surface was the covered using the
byars flap technique
Figure 6 The surgical wound ten days after
type IIA “Y”, and type IIB with the second channel arising independently from the bladder but joining the first and coursing into one meatus. Type III is when urethral duplication as a component of partial or complete caudal duplication, usually associated with bladder duplication.16
This classification is more functional, repre-senting all clinical types of urethral duplication.17
Eiffmann type IIA 2”Y” is the most common type reported of urethral duplication18–20 and usually
associated with severe congenital anomalies like imperforate anus, cloacal atrophy, conjoined twins, early amnion rupture syndrome, prune belly syndrome and hand-foot genital syndrome.21
According to this classification, our patient belonged to type IA. Although this classification is considered to be the most exhaustive, it does not distinguish sagittal from coronal duplication and does not recognise female form. Lima at al.22
suggested a new classification, the proposed clas-sification scheme is based on the required surgi-cal approach, this classification is more complete and includes coronal and sagittal pieces and also divided between men and women.
Diagnosis of urethral duplication is based on simple physical examination of the penis and is confirmed by a voiding cystourethrography or retrograde urethrogram to identification the pres-ence of urethral duplication and its anatomical type.23 Ultrasound may be helpful in the diagnosis of
other associated anomalies.23,24 Upper urinary tract
abnormalities are found in up to 80% of patients and are diagnosed with intravenous urography or ultrasonography.5 Clinical signs and symptoms
of urethral duplication are diverse. Patients may complain of intermittent discharge from the acces-sory urethra having two emission sites of urine, incontinence, recurrent urinary tract infections, obstructive symptoms, or no symptoms at all.25,26 In
our patient there were no complaints experienced before and the until there was sign of infection in the accessory urethra with sign and symptoms in the form of whitish discharge from meatus of acces-sory urethra.
The first step in the management of urethral duplication is to recognise the normal-functioning urethra; in fact, the true urethra is that with the largest calibre, a normal verumontanum, and an intact sphincter. Urethroscopy can be conducted to evaluate the diameter and the presence of veru-montanum.23 Treatment of urethral duplication
should be individualised based on the anatomic types and also clinical findings and severity of the accompanying anomaly. Many patients are asymp-tomatic and do not require any surgery. There is no clear consensus yet regarding the management of
urethral duplication, some experts recommended that surgical management is unnecessary in asymp-tomatic patients. Surgical treatment is needed for reconstructing deformities, such as dorsal meatus, to fix the emission sites of urine, incontinence, recurrent urinary tract infections, obstructive symptoms as well as to mend urinary leakage on the perineal area.23,27 Surgical management can be
conducted with various techniques, consisting of one step to two steps of surgery, with simple coagu-lation or reconstructive surgery, depending the type of urethral duplication. If the two urethral orifices are too close to each other on the glans, then the septum between the two meatus can be excised to give a single urinary meatus. Other than this, most procedures involve excision of the accessory urethra with reconstruction of the normal urethra.18,28 The
simplified treatment scheme proposed by Salle at al. based on the type of urethral duplication from Effmann classification. In the cases of type IA urethral duplicationspectrum above they proposed meatoplasty or exeresis of the accessory urethra. Urethro-urethrostomy can be done with or without urethroplasty for the type IIA 1 while for the type IIA 2 the treatment is urethroplasty. They proposed to exeresis the non-functional bladder for type III urethral duplication in sagittal plane and exeresis bladder septum or hemibladder plus reimplan-tation of the urethra in the contralateral bladder zone for the type III urethral duplication in coro-nal plane without diphallia and if accompanied by diphallia penoplasty and glans plasty is needed. No surgical intervention is needed for cases of urethral duplication type IB and IIB.29
In our case the accessory urethra was excised completely, we did that procedure in accordance with the treatment scheme proposed by Salle at al. because in this Type 1A urethral duplication the accessory urethra was blind-ending in distal loca-tion and was not connected to the principal urethra or bladder. The outcome of this patient was very good.
CONCLUSION
CONFLICT OF INTEREST
The authors affirm no conflict of interest in this study.
FUNDING
There is no external funding done for this study. All expenses were covered by the institution and authors.
AUTHOR CONTRIBUTIONS
Y.I.H made assessment of the case, performed the operation, followed up the patient, gifted knowledge and supervised the case; M.A collected the data, followed up the patient and wrote the manuscript.
REFERENCES
1. Coleman RA, Winkle DC, Borzi PA. Urethral duplica-tion: Cases of ventral and dorsal complete duplication and review of the literature. J Pediatr Urol. 2010;6:188–91. 2. Ismail A, Al Rayes T, Alsalihi M, Abbas T. Female double
urethra: A case report. J Pediatr Surg. 2012;47:e29–31. 3. Abouzeid AA, Safoury HS, Mohammad SA, el-Naggar O,
Zaki AM, Hassan TA, et al. The double urethra: Revisiting the surgical classification. Ther Adv Urol. 2015;7:76–84. 4. Lopes RI, Giron AM, Mello MF, Neto CMB, dos Santos J,
Moscardi PRM, et al. Urethral duplication type influences on the complications rate and number of surgical proce-dures. Int Braz J Urol. 2017;43:1144–51.
5. Haleblian G, Kraklau D, Wilcox D, Duffy P, Ransley P, Mushtaq I. Y-type urethral duplication in the male. BJU Int. 2006;97:597–602.
6. Arena S, Arena C, Scuderi MG, Sanges G, Arena F, Di Benedetto V. Urethral duplication in males: Our experi-ence in ten cases. Pediatr Surg Int. 2007;23:789–94. 7. Woodhouse C, Williams D. Duplications of the lower
uri-nary tract in children. Br J Urol. 1979;51:481–7.
8. Das S, Brosman S. Duplication of the male urethra. J Urol. 1977;117:452–4.
9. Sánchez M, Vellibre R, Castelo J, Arias M, Sarmiento R, Costa A. A new case of male Y-type urethral duplication and review of literature. J Pediatr Surg. 2006;41:e69-71. 10. Casselman J, Williams D. Duplication of the urethra. Acta
Urol Belg. 1966;34:535–41.
11. Rica P, Holder T, Ashcraft K. Congenital posterior urethral perineal fistula: a case report. J Urol. 1978;199:416–7. 12. Alanee S, Gupta P, Gleich P, Shukla AR. Complete
ure-thral duplication: Description of surgical approach mim-icking distal epispadias repair. J Pediatr Urol [Internet]. 2012;8:343–7.
13. Palmer LS, Palmer JS. Management of Abnormalities of the External Genitalia in Boys. In: Campbell-Walsh Urology Eleventh Edition. 2016. p. 3379–80.
14. Onofre LS, Gomes AL, Leão JQDS, Leão FG, Cruz TMA, Carnevale J. Urethral duplication - A wide spectrum of anomalies. J Pediatr Urol. 2013;9:1064–71.
15. Williams D, Kenawi M. Urethral duplication in the male. Eur Urol. 1975;1:209–15.
16. Effmann E, Lebowitz R, Colodny A. Duplication of the urethra. Radiology. 1976;119:179–85.
17. Maitama HY, Tella UM, Mbibu HN. Urethral duplica-tion: Case report and literature review. Ann Afr Med. 2012;11:186.
18. Podesta M, Medel R, Castera R, Ruarte A. Urethra dupli-cation in children: Surgical treatment and results. J Urol. 1998;160:1830–3.
19. Wagner J, Carr M, Bauer S, AH C, Retik A, Hendren W. Congenital posterior urethral perineal fistulae: A unique form of urethral duplication. Urology. 1996;48:277–80. 20. Slavov C, Donkov I, Popov E. Case of duplication of the
urethra in an adult male, presenting with symptoms of bladder outlet obstruction. Eur Urol. 2007;52:1249–51. 21. Stephens F. Abnormal Embryology-cloacal dysgenesis.
Congenital Malformations of the Urinary Tract. Part 1, Chapter 2. Vol. 5, New York: Praeger Scientific. p. 1983. 15–52.
22. Lima M, Destro F, Maffi M, Persichetti Proietti D, Ruggeri G. Practical and functional classification of the double urethra: A variable, complex and fascinat-ing malformation observed in 20 patients. J Pediatr Urol [Internet]. 2017;13:42.e1-42.e7.
23. Okur MH, Aydogdu B, Arslan S, Basuguy E, Zeytun H, Arslan MŞ. Type II A2 duplication of urethra in an 8-month-old male child: A case report. Pediatr Urol Case Reports. 2015;2:17–22.
24. Baid M, Dutta A. Urethral duplication in a 15-year-old: case report with review of the literature. Rev Urol. 2014;16:149–51.
25. Erdil H, Mavi A, Erdil S, Gumusburun E. Urethral Duplication. Acta Med Okayama. 2003;57:91–3.
26. Gozar H, Prișcă R, Derzsi Z. Two Cases of Dorsal Urethral Duplication. Acta Medica Marisiensis. 2013;59:52–4. 27. Cicek T, Kizilkan Y, Coban G, Kosan M. Urethral
duplica-tion: A rare cause of recurrent urinary infection. J Pak Med Assoc. 2015;65:90–2.
28. Middleton AJ, Melzer R. Duplicated urethra: an anomaly best repaired. Urology. 1992;39:538–42.
29. Salle J, Sibai H, Rosenstain D, Brzezinski A, Corcos J. Urethral duplication in the male: review of 16 cases. J Urol. 2000;163:1936–40.