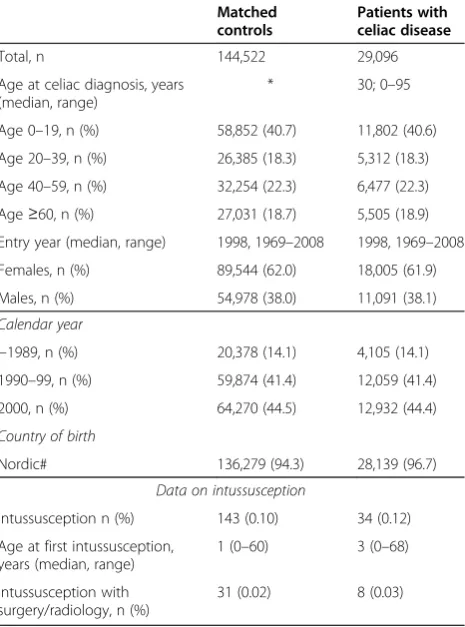
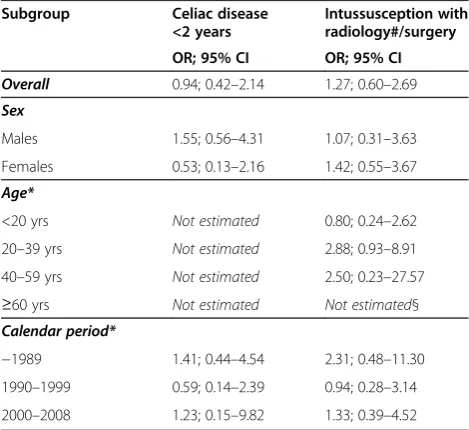
A large nationwide population-based case–control study of the association between intussusception and later celiac disease
Full text
Figure
Related documents
Τα διακριτά και τα πεπερασµένα Μαθηµατικά είναι τα µαθηµατικά που χρησιµοποιούν οι ηλεκτρονικοί υπολογιστές και η Γραµµική Άλγεβρα ασχολείται ακριβώς
The total coliform count from this study range between 25cfu/100ml in Joju and too numerous to count (TNTC) in Oju-Ore, Sango, Okede and Ijamido HH water samples as
Long-term follow-up of a randomized trial comparing concurrent single agent cisplatin, cisplatin- based combination chemotherapy, or hydroxyurea during pelvic
This study mainly aims at determining the tobacco and alcohol consumption patterns, there interdependence on each other and their interactions with drugs and enumerating diseases
These membranes have tunable chirality and show a rich array of emergent behaviors, including a transition from a circular shape to a striking starfish shape upon changing the
Initial presentation to staff Nov 11, 2008 Nov 13, 2008 Mar 23, 2009 Mar 27, 2009 Visibly post unit-specific data on unit b Nov 13, 2008 Continued Mar 23, 2009 Jun 1, 2010 Post
Using oxidation and toxicity analysis with several approaches, we demon- strate that the RuBpy-doped silica NPs could induce significant amount of ROS and toxicity in MH-S cells
investigated the morphologic alterations of podocyte - specific proteins in dia- betic nephropathy biopsies from patients with Type 2 diabetes mellitus and found
