Alternative Rehydration Methods: A Systematic Review
and Lessons for Resource-Limited Care
abstract
OBJECTIVE:Dehydration is a significant threat to the health of children
worldwide and a major cause of death in resource-scarce settings. Although multiple studies have revealed that oral and intravenous (IV) methods for rehydration in nonsevere dehydration are nearly equally effective, little is known about effectiveness beyond these 2 techniques. With this systematic review we analyzed the effectiveness of nonoral and nonintravenous methods of rehydration.
METHODS:The Medline, Cochrane, Global Health, Embase, and CINAHL
(Cumulative Index to Nursing and Allied Health Literature) databases were searched for articles on intraosseous (IO), nasogastric (NG), in-traperitoneal (IP), subcutaneous (hypodermoclysis), and rectal (proc-toclysis) rehydration through December 2009. Only human pediatric studies that included data on the effectiveness or complications of these methods were included.
RESULTS:The search identified 38 articles that met the inclusion
cri-teria: 12 articles on NG, 16 on IO, 7 on IP, 3 on subcutaneous, and none on rectal rehydration. NG rehydration was as effective as IV rehydra-tion for moderate-to-severe dehydrarehydra-tion. IO rehydrarehydra-tion was effective and easy to obtain, although only 1 randomized trial was identified. IP rehydration had some benefit for moderate dehydration, although none of the trials had control groups. Limited data were available on subcutaneous rehydration, and only 1 case series showed benefit.
CONCLUSIONS:NG rehydration should be considered second-line
ther-apy, after oral rehydration, particularly in resource-limited environ-ments. IO rehydration seems to be an effective alternative when IV access is not readily obtainable. Additional evidence is needed before
IP and subcutaneous rehydration can be endorsed.Pediatrics2011;
127:e748–e757
AUTHORS:Shada Rouhani, MD,aLaura Meloney, BS,bRoy
Ahn, SD,b,cBrett D. Nelson, MD, MPH, DTM&H,b,d,eand
Thomas F. Burke, MDb,c,d,e
aHarvard Affiliated Emergency Medicine Residency Program,
Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, MA;bDivision of Global Health and Human
Rights, Department of Emergency Medicine, Massachusetts General Hospital; Boston, MA; Departments ofcSurgery and ePediatrics, Harvard Medical School, Boston, MA;dDivision of
Global Health; MassGeneral Hospital for Children, Boston, MA
KEY WORDS
dehydration, critically ill children, diarrhea, international child health, intravenous rehydration
ABBREVIATIONS
IV—intravenous NG—nasogastric IO—intraosseous IP—intraperitoneal
ORS—oral rehydration solution NS—normal saline
www.pediatrics.org/cgi/doi/10.1542/peds.2010-0952
doi:10.1542/peds.2010-0952
Accepted for publication Nov 19, 2010
Address correspondence to Shada Rouhani, MD, Department of Emergency Medicine, Massachusetts General Hospital, 5 Emerson Place, Suite 100, Boston, MA 02114. E-mail: srouhani@ partners.org
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
Dehydration is one of the most com-mon problems confronting ill children worldwide. It is closely tied to many of
the leading causes of childhood mor-tality, including diarrheal illnesses, acute respiratory infections, malaria, and malnutrition. The United Nations
Children’s Fund has estimated that 1.7 million children per year die from
diar-rheal dehydration alone.1It is well
es-tablished that when available and tolerated, oral rehydration is the
pre-ferred method of rehydration. It is as effective as intravenous (IV) rehydra-tion in mild and moderate dehydrarehydra-tion and is more readily available and
af-fordable.2,3However, for some patients
oral rehydration is not possible be-cause of unwillingness or inability to drink, severity of illness, or comorbidi-ties. In resource-scarce settings,
ster-ile supplies needed to secure and maintain IV access are often absent. Even if supplies are available, children in the developing world frequently present with such severe dehydration
that intravascular access is techni-cally challenging or impossible.
Because oral and IV rehydration are not feasible for all children, it is impor-tant for clinicians to have alternative methods of rehydration available to them. Numerous alternative methods
have been used. Nasogastric (NG) re-hydration uses the intestinal system just as oral rehydration does. Procto-clysis relies on the absorption of fluids
through the rectal mucosa. Intraosse-ous (IO) fluid administration uses bone marrow as a direct access to the intra-vascular circulation. Hypodermocly-sis, or subcutaneous fluid
admin-istration, and intraperitoneal (IP)
rehydration both rely on indirect ab-sorption into the circulation. The rela-tive effecrela-tiveness of these methods for
acute rehydration is unclear. Some, such as NG and IO rehydration, are used today at the discretion of the
practitioner. Others are not widely used.
The aim of this review was to examine the literature on the effectiveness, benefits, and risks of alternative (ie, nonoral and non-IV) techniques for pe-diatric rehydration. Techniques exam-ined included NG, IO, IP, subcutaneous, and proctoclysis rehydration.
METHODS
A literature search was conducted in 5 databases: Medline, Cochrane, Global Health, Embase, and CINAHL (Cumula-tive Index to Nursing and Allied Health Literature). The following text search terms and Medical Subject Headings were used: rehydration; dehydration; hydration; fluid therapy; and injection, in combination with any of NG, IO, IP, subcutaneous, hypodermoclysis, or proctoclysis. The searches were limited to articles written in English and concerning human studies. The searches were not restricted by dates of publication and included all articles through the completion of the search in December 2009. In addition to the articles identified through this search, key references from included articles were also examined.
The identified articles were manually sorted to include patients younger than 18 years. If studies had both pedi-atric and adult populations, they were included only if they had listed the re-sults separately for the pediatric pa-tients. Adult studies were excluded, because much of the adult data on al-ternative rehydration methods, such as subcutaneous rehydration, come from geriatric and palliative care liter-ature. These patients have different physiology and goals of care from chil-dren with acute dehydration. Case re-ports and consensus-based guidelines were eligible for inclusion, whereas articles that were opinion-based were excluded. Articles in which a technique but not its effectiveness was described
were also excluded. However, articles in which a complication of a method was described, regardless of refer-ence to effectiveness, were included to allow an assessment of risks and ben-efits. The search strategy is outlined in Fig 1. The selection of articles was ini-tially conducted by 1 author; when an article was felt to be borderline for in-clusion or exin-clusion, it was examined by 2 or more authors, and a consensus on inclusion or exclusion was reached. Given the limited literature on this subject, articles that met the above-listed inclusion criteria were not ex-cluded on the basis of the quality of their methods, but assessment of the differences in methodology was in-corporated into the text of the review to allow the reader to weigh the qual-ity of the literature.
RESULTS
The initial search strategy identified 1436 articles. A significant number of these articles were excluded, be-cause they focused solely on adult pop-ulations. In addition, many studies did not relate to dehydration or hypovole-mia. After manual review of the titles and available abstracts of these cles, the list was narrowed to 82 arti-cles. Subsequent review of the full text of these articles identified 38 articles that met all inclusion criteria: 3 on sub-cutaneous rehydration, 12 on NG rehy-dration, 7 on IP rehyrehy-dration, 16 on IO rehydration, and none on proctoclysis.
NG Rehydration
Twelve articles about NG hydration met the inclusion criteria for our review. Of these studies, 5 were randomized con-trolled trials, 4 of which compared NG to IV rehydration and 1 of which com-pared different solutions for NG rehy-dration. The remaining articles in-cluded cohort studies, case series,
retrospective chart reviews, and
rehy-dration is effective in cases of moder-ate and severe dehydration.
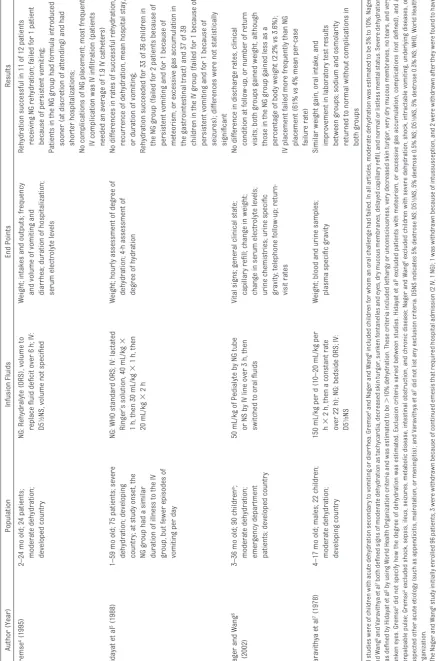
The 4 randomized trials that compared NG to IV rehydration are summarized in Table 1. In all 4 studies, NG rehydra-tion had efficacy similar to that of IV rehydration, although different end points and protocols were used in each study. NG rehydration failed in 2% of all patients (4 of 211 total) for rea-sons detailed in Table 1. These patients were switched to IV rehydration.
Several case series also supported the effectiveness of NG rehydration. In 2000, a prospective study of 4131 chil-dren with acute diarrhea and severe dehydration, defined as at least a 10% weight loss, supported NG rehydration. All children were rehydrated by NG tube using oral rehydration solution (ORS) at 20 to 30 drops per minute and a total volume of 50 to 100 mL/kg per day for the first 10 kg of weight and 25 to 50 mL/kg per day for the remaining
weight. Ninety percent of the patients had significant weight gain after 4 hours of NG infusion, 10% needed pro-longed NG infusion, and none required
IV fluids.8A subsequent study in 2003
included 4000 children with acute diar-rhea and a 10% weight loss, although patients in shock were excluded. Pa-tients were randomly assigned to re-ceive NG rehydration solutions of dif-ferent osmolarity. Of these children, 3537 (88%) had a rapid response to fluids, 316 (8%) needed prolonged re-hydration, and 147 (4%) needed
admis-sion to the hospital.9It is unclear if
chil-dren admitted to the hospital were given IV rehydration.
Smaller case series also supported the effectiveness of NG rehydration. In 2 studies focused on children with moderate dehydration, most patients experienced clinical improvement with NG rehydration, although 4 of 47 pa-tients (9%) in the 2 studies needed to
be switched to IV rehydration.10,11Two
other case series revealed benefits with NG rehydration consistent with those in other studies, although nei-ther the level of dehydration nor the rehydration protocol that was
fol-lowed were specified.12,13
Finally, one consensus guideline on the management of diarrhea with or with-out vomiting addressed NG rehydra-tion. It was developed by using a Delphi consensus process after a systematic literature review. The panel recom-mended NG rehydration over IV dration for patients in whom oral
rehy-dration had failed.14
Complications from NG rehydration were infrequent. One study found that emesis was more common in patients with gastroenteritis who were given NG rehydration compared with IV
rehy-dration.15One patient developed
mete-orism, or excessive gas accumulation in the gastrointestinal tract, and was successfully switched to IV
rehydra-tion.5In a study on adverse events in
patients with NG tubes for rehydration, reported adverse effects included mul-tiple insertions in 34%, sore throat in 13%, coughing in 16%, negligible epi-staxis in 3%, and need for mittens in
nearly 75% of the patients.16However,
in this study, data on adverse events were collected from only 26% of the eligible patients. There was only 1 as-piration event in any of the included studies, and after review of the chart in that case, the authors concluded that it was unclear if the recorded event was aspiration or misplacement.
IO Rehydration
Sixteen articles addressed IO infusions. One was a randomized controlled trial, 12 were case reports, and 3 were case series. Of the 12 case reports, 10 de-scribed the efficacy of IO infusion and 2 described complications.
The randomized controlled trial com-pared IV to IO hydration in severely
de-Database search:
Medline, Cochrane, Global Health, Embase, CINAHL
Manual sorng
Limits:
Human studies English language No date restricon
Exclude:
Adult-only results Opinion-based reports
Menons technique but not effecveness
Include:
All arcles with children <18 y old Menon of effecveness or complicaons
38 arcles
3 hypodermoclysis
12 NG
7 IP
0 proctoclysis
16 IO subcutaneous
FIGURE 1
TABLE 1 Randomized Controlled Trials in Which IV and NG Rehydration Were Compared Author (Year) Population Infusion Fluids End Points Results Gremse 4(1995) 2–24 mo old; 24 patients; moderate dehydration; developed country NG: Rehydralyte (ORS), volume to replace fluid deficit over 6 h; IV: D5
1⁄2
NS, volume not specified Weight; intakes and outputs; frequency and volume of vomiting and diarrhea; duration of hospitalization; serum electrolyte levels Rehydration successful in 11 of 12 patients receiving NG rehydration; failed for 1 patient because of persistent vomiting; Patients in the NG group had formula introduced sooner (at discretion of attending) and had shorter hospitalizations; No complications of NG placement; most frequent IV complication was IV infiltration (patients needed an average of 1.9 IV catheters) Hidayat et al 5(1988) 1–59 mo old; 75 patients; severe dehydration; developing country; at study onset, the NG group had a similar duration of illness to the IV group, but fewer episodes of vomiting per day NG: WHO standard ORS; IV: lactated Ringer’s solution, 40 mL/kg ⫻ 1 h, then 30 mL/kg ⫻ 1 h, then 20 mL/kg ⫻ 2h Weight; hourly assessment of degree of dehydration; 4-h assessment of degree of hydration No differences in rates of successful rehydration, recurrence of dehydration, mean hospital stay, or duration of vomiting; Rehydration succeeded for 33 of 36 children in the NG group (failed for 2 patients because of persistent vomiting and for 1 because of meteorism, or excessive gas accumulation in the gastrointestinal tract) and 37 of 39 children in the IV group (failed for 1 because of persistent vomiting and for 1 because of seizures); differences were not statistically significant Nager and Wang 6 (2002) 3–36 mo old; 90 children a; moderate dehydration; emergency department patients; developed country 50 mL/kg of Pedialyte by NG tube or NS by IV line over 3 h, then switched to oral fluids Vital signs; general clinical state; capillary refill; change in weight; change in serum electrolyte levels; urine chemistries; urine specific gravity; telephone follow-up; return-visit rates No difference in discharge rates, clinical condition at follow-up, or number of return visits; both groups gained weight, although those in the NG group gained less as a percentage of body weight (2.2% vs 3.6%); IV placement failed more frequently than NG placement (61% vs 4% mean per-case failure rate) Varavithya et al 7(1978) 4–17 mo old; males; 22 children; moderate dehydration; developing country 150 mL/kg per d (10–20 mL/kg per h ⫻ 2 h, then a constant rate over 22 h); NG: bedside ORS; IV: D5
1⁄3
NS Weight; blood and urine samples; plasma specific gravity Similar weight gain, oral intake, and improvement in laboratory test results between groups; sodium and osmolarity returned to normal without complications in both groups All studies were of children with acute dehydration secondary to vomiting or diarrhea. Gremse 4and Nager and Wang 6included children for whom an oral challenge had failed. In all articles, moderate dehydration was estimated to be 5% to 10%. Nager and Wang 6and Varavithya et al 7both defined signs of moderate dehydration as tachycardia, decreased skin turgor, sunken fontanelles and eyes, dry mucous membranes, delayed capill ary refill, and normal or listless mental status. Severe dehydration was defined by Hidayat et al 5by using World Health Organization criteria and was estimated to be ⬎ 10% dehydration. These criteria included lethargy or unconsciousness, very decreased skin turgor, very dry mucous membranes, no tears, and very sunken eyes. Gremse 4did not specify how the degree of dehydration was estimated. Exclusion criteria varied between studies. Hidayat et al 5excluded patients with meteorism, or excessive gas accumulation, complications (not defined), and a nonpalpable pulse; Gremse 4excluded shock, sepsis, ileus, seizures, metabolic disease, intestinal obstruction, and chronic disease; Nager and Wang 6excluded children with severe dehydration, shock, intractable vomiting, underlying diseases, or suspected other acute etiology (such as appendicitis, malrotation, or meningitis); and Varavithya et al 7did not list any exclusion criteria. D5NS indicates 5% dextrose NS; D5
1⁄2
NS, 5% dextrose 0.5% NS; D5
1⁄3
hydrated children with acute
gastro-enteritis.17Sixty children received a 20
to 30 mL/kg normal saline (NS) bolus by IO or IV routes, followed by identical protocols regarding the reintroduc-tion of oral fluids. End points included time to placement, stabilization of vital signs, correction of dehydration, and complications. There was no differ-ence in efficacy of rehydration or cor-rection of laboratory abnormalities between the groups. However, IO placement was significantly faster (67 vs 129 seconds) and more reliable (IV lines failed to be placed within 5 min-utes in 33% of the patients in the IV group, versus no failures in the IO group). IO needles were successfully placed in those patients in the IV group in whom IV placement had failed; it is unclear in which group these patients were subsequently analyzed. There were no short-term complications in
either group, although the study
lacked long-term follow-up.
Results of another study of 22 children aged 1.5 to 10 months with shock fur-ther supported the efficacy of IO fluids
for rehydration.18 Children had an IO
line placed either immediately if they had gasping respirations or after 2 to 3 failed IV-line-placement attempts. Twenty-one of 22 patients (95.5%) had improvement in their circulatory state with fluids, blood, and medications given through the IO route. Sixteen (73%) of the patients ultimately sur-vived. The only patient with no re-sponse to fluids was apneic and brady-cardic on arrival. It is important to note that in all patients, IO access was obtained by using a standard 18-gauge butterfly needle rather than an IO-specific needle.
Four case reports focused on IO-fluid resuscitation in patients with burns. A total of 6 patients (age range: 17 days to 3 years) were included in these
reports.19–21All 6 children were
suc-cessfully initially resuscitated with IO
fluid, and 2 continued to receive IO
flu-ids for 48 hours.20One child died from
smoke inhalation 2 days after the
ini-tial resuscitation.21
Two case reports involved fluids given through the IO route during cardiac arrest. One child was suc-cessfully resuscitated after receiv-ing lactated Rreceiv-inger’s solution and
multiple vasoactive medications.22
The other child did not survive, but a femoral vein puncture above the site of the IO infusion produced diluted blood that appeared to be mixed with saline, which provided evidence that the IO-infused saline had reached the
intravascular space.23
Two additional case reports on hypo-volemic patients who were resusci-tated with IO access reported success-ful outcomes. One was a 5-year-old patient with diabetic ketoacidosis and an estimated 10% fluid deficit. The ini-tial 14 hours of the resuscitation were accomplished via the IO route and
produced clinical improvement.24The
other was a 7-month-old infant who had dehydration caused by vomiting and was successfully resuscitated with NS through a spinal needle
in-serted into the tibia.25 In both cases,
initial attempts at IV access had been unsuccessful.
Several articles addressed IO use in neonates. In 1 study, 27 neonates in the ICU who had unsuccessful attempts at routine means of access had IO nee-dles inserted for resuscitation. All pa-tients had an IO catheter inserted in less than 2 minutes and were success-fully initially resuscitated through the IO route with volume expanders and medications. However, 44% of the pa-tients later died of underlying
dis-ease.26 Two case reports described
successful use of IO infusions in neo-nates: 1 in a 38-day-old preterm infant who weighed 800 g and another in a 10-day-old infant with dehydration and poor feeding secondary to coarctation
of the aorta.27,28 In both cases, the
in-fants were successfully resuscitated from circulatory collapse through the IO route.
Few complications were noted from these studies. The authors of a study of 27 neonates reported 3 cases in which the IO catheter dislodged, 1 case of subcutaneous necrosis, and 1 case of
hematoma formation.26 Two case
re-ports of compartment syndrome after IO infusion were found: 1 in a 3-year-old who had bilateral IO infusions and 1 in an 11-month-old who had an IO
infu-sion for 53 hours.29,30Both patients
un-derwent fasciotomies and recovered;
1 had minimal residual deficit.30Local
swelling in 1 patient from another case report, which resolved without
long-term complications.31 No recent
re-ports of infection were identified in our literature search. In a 1946 series of 495 patients, 5 (1%) developed
osteo-myelitis.32 The protocols followed at
that time included using iodine and hand-washing but not gloves.
IP Rehydration
Seven articles on IP hydration met the inclusion criteria. All were case series that ranged in size from 4 to 96 pa-tients. All of them were conducted in developing countries, and only 1 was conducted after 1975. Reports from 6 studies noted benefits with IP fluids, although none of the studies had com-parison groups. Patients included ranged from mildly to severely dehy-drated. IP rehydration produced better results in patients who were moder-ately rather than severely dehydrated. The studies on IP rehydration are sum-marized in Table 2.
Adverse effects from IP infusion were uncommon in these studies. Dyspnea was noted in 4 patients (2 of 56 chil-dren [4%] in 1 case series and 2 of 91
children [2%] in another).36,37 In 1
recovered without incident (ref38and M. J. VanRooyen, MD, MPH, personal
e-mail communication, March 18,
2010). Meteorism was seen in 9 of 56
patients (16%) in 1 case series.36The
authors of this study also noted a slight increases in average leukocyte count (from 8.4 to 11.7) and
tempera-ture (from 37.7 to 38.2°C) after infu-sion. Of 20 postmortem examinations performed after IP transfusion, there was 1 child with peritonitis that was
TABLE 2 Articles on Intraperitoneal Rehydration
Author (Year) Population Study Protocol End Points Results
Agusto-Odutola33
(1971)
15 patients; 3–23 mo old; moderate dehydration
55 mL/kg IP bolus of NS with potassium
Clinical rehydration; serum electrolytes; hemoglobin; PCV; urea; plasma osmolarity
14 patients (93%) improved and were discharged within 24 h; 1 patient died; postmortem examination showed no complications from IP infusion;
Improvements in electrolyte levels were seen by 2 h after infusion Carter34(1953) 96 children; ages not given;
patients in whom “death appeared inevitable”
IP bolus of D2.5NS; volume was not standardized
Rate of absorption (which was assumed to be proportional to clinical hydration state and physical examination)
Rate of absorption was very good in 15 cases, good in 34, fair in 15, and poor in 6; remainder of patients were not accounted for; the total number of deaths was not listed; 20 postmortem examinations were performed
Mahalanabis et al35
(1970)
26 patients; 7 mo to 6 y old; moderate-to-severe dehydration
4 patients given only IP fluids: 70–100 mL/kg IP lactated Ringer’s solution bolus; 22 patients given IV fluids for 1–3 h, then 50–70 mL/kg IP lactated Ringer’s solution bolus
Clinical state; weight; plasma specific gravity; pH; CO2
IP-only group: all 4 children were initially normotensive and all were successfully treated.
IV-followed-by-IP group: children had lower blood pressures at admission to the study and 19 (86%) of the children were successfully treated. Noerasid et al36
(1975)
56 children; 2–18 mo old; moderate dehydration
40 mL/kg IP bolus of 2 parts NS, one part D5 at 0 and 4 h;
Weight; vital signs; degree of dehydration; frequency of vomiting and diarrhea; urine output; leukocyte count; serum electrolyte levels
89.3% were fully rehydrated after 8 h; 3.6% had no response to IP fluids and required IV rehydration; Significant increase in weight and
decrease in diarrhea was seen 8 h after initial infusion
Ransome-Kuti et al37(1969)
105 children; 91 included in the analysis; 3 mo to 4 y old; mild-to-severe dehydration
11.4 mL/kg bolus of IP fluids in 1 of 5 compositions
6-h clinical observation; hemoglobin; osmolarity; serum electrolyte levels
14 patients with severe dehydration were excluded from the analysis after they deteriorated and needed IV fluids; 74.7% of the remaining children were able to be discharged within 24 h; 11 patients died, 7 were moderately or severely dehydrated, 4 had pneumonia and malnutrition VanRooyen et al38
(1995)
14 children; 4 mo to 15 y old; significant dehydration; patients for whom oral therapy and IV placement failed
80 mL/kg IP bolus of1⁄
2NS Clinical improvement, defined
as: ability to tolerate oral fluids, improved level of consciousness, absence of tachycardia and
hypotension, improved skin turgor, moist mucous membranes
13 children improved (93%); 1 died within 24 h
Wenzel and Phillips39(1971)
4 children; 5–10 y old; moderate dehydration
Bolus amount not specified State of hydration; stool output; urinary output
No child had improvement in clinical dehydration or stool or urine output after 4 h; all were given IV or oral rehydration and recovered; did not specify if other children were successfully treated
Definitions on the degree of dehydration varied between studies: Agusto-Odutola33and Ransome-Kuti et al37both used 1952 criteria from the Medical Research Council that defined moderate
dehydration as a 5% to 10% decrease in body weight associated with restlessness, decreased skin turgor, cool skin, sunken eyes and anterior fontanelle, dry mucous membranes, and a pulse of 160 to 180 beats/minute. Severe dehydration was defined as⬎10% weight loss, with semi-coma, worsened signs of the above, and a pulse of⬎180 beats per minute.33,37VanRooyen
et al38defined “significant dehydration” as decreased level of consciousness, dry mucous membranes, poor skin turgor or tenting, and tachycardia or hypotension. Noerasid et al36, Wenzel
and Phillips,39and Mahalanabis et al35did not provide criteria for their dehydration classifications, although Wenzel and Phillips noted that all of their patients had tachycardia and poor skin
turgor. Carter34did not discuss the degree of dehydration but included patients in whom “death appeared inevitable.” PCV indicates packed cell volume; D5, 5% dextrose; D2.5NS, 2.5%
found on autopsy. However, it was at-tributed to dysentery causing multiple full-thickness ulcerations of the distal ileum with one site of perforation 2 inches from the peritoneal infusion
site.34
Subcutaneous Rehydration (Hypodermoclysis)
Three studies met the inclusion crite-ria for subcutaneous rehydration. One was a series of 51 patients with mild or moderate dehydration treated with subcutaneous fluid infusion assisted by a hyaluronidase enzyme. Patients were given an initial bolus of 20 mL/kg isotonic fluid over 1 hour, followed by further fluid if needed. Forty-three
patients (84.3%) were rehydrated
through subcutaneous fluid in the emergency department. An additional 5 patients (10%) were reported as suc-cessfully rehydrated (judged to have been “clinically rehydrated primarily
through the subcutaneous route”40). It
is unclear if they were given any other forms of rehydration.
The other 2 publications about subcu-taneous rehydration date back to the 1960s. One was a case series of 4 pa-tients with significant metabolic ab-normalities who were transferred to a pediatric center after failing to im-prove with subcutaneous fluids. All 4 patients later improved with IV fluids, and the author concluded that the sub-cutaneous fluids were ineffective and
worsened the symptoms.41 However,
the volume of subcutaneous fluid given to each patient was not indicated, and the author provided no reasons for postulating that subcutaneous fluid worsened the patients’ conditions
rather than the natural disease
course. The other publication was a case report of a 5-month-old child with pneumonia who was given an unspec-ified amount of subcutaneous NS with 5% dextrose. Three days later the pa-tient developed oliguria and edema,
which were attributed to the
subcuta-neous infusion.42
In the case series of 51 patients, 1 se-rious adverse event (cellulitis) was re-ported. Most patients had pain on the infusion of hyaluronidase, but two-thirds of them had no pain with fluid
infusion.40
Proctoclysis
There were no studies on proctoclysis that met the inclusion criteria. Only 3 studies on proctoclysis were identified in our literature search: 2 studies were of adults, and 1 failed to meet our study inclusion criteria because it was opinion-based rather than empirically driven.
DISCUSSION
Dehydration threatens the lives of at
least 2 million children annually.1The
effectiveness of oral and IV rehydra-tion has been well established, al-though at times neither is available, ef-fective, or possible. In this review we examined the data on alternative methods of rehydration.
NG rehydration for moderate and se-vere dehydration is supported by the results of several randomized con-trolled trials. The data have suggested that NG hydration is safe and effective. Despite this fact, it is not as widely
used as it could be.43Larger studies
may be needed to determine if the ben-efits of oral rehydration can be
repli-cated with NG rehydration.44
Further-more, although not one of our primary areas of interest, limited data suggest that compared with IV rehydration, NG rehydration results in shorter hospital stays and cost savings of as much as $115 per case in a developed
coun-try.2,15It is important to note that,
un-like IV infusion, NG infusion does not require sterile fluids but can rely on standard ORS, which makes it a more accessible technique in low-resource environments.
With the exception of NG rehydration, the quality of evidence behind other methods of hydration is poor. The qual-ity of data on IO infusions was not as robust as expected, given its wide-spread use as a rescue technique for intravascular access. Our literature search identified only 1 randomized trial of IO versus IV access. The results of this study and other published re-ports support IO infusions as effective and easy to obtain. In addition, multiple resuscitation guidelines recommend IO access in cases of shock when IV access cannot be obtained quickly. Our review has demonstrated that IO ac-cess in infants can be achieved with needles that are not specifically de-signed for IO cannulation, such as
18-gauge butterfly needles19 or spinal
needles.25
The quality of evidence on IP rehydra-tion is not as robust as would be de-sired. Multiple case series have shown that IP hydration is effective in moder-ately dehydrated patients, although the results in severely dehydrated pop-ulations have been mixed. In addition, there have been no comparative stud-ies on IP rehydration. Therefore, until further evidence is obtained, IP rehy-dration can only be recommended when oral, NG, IV, and IO rehydration either fail or are not available.
The quality of evidence on subcutane-ous rehydration is also poor. The au-thors of 2 older case reports warned against subcutaneous rehydration but without clear justification. Only 1 case series supported its use. However, this case series was small and designed to test a specific medication as an ad-junct. As such, its results may not be generalizable. Literature on rehydra-tion of adults has suggested that subcutaneous rehydration may be ad-ministered without hyaluronidase, al-though the effect on absorption is
unclear.45Although data on
care literature suggest some benefit, more research in the pediatric popula-tion is required before its use can be
endorsed.46,47
Serious complications were uncom-mon in all of the methods we analyzed. Infection, which is a theoretical com-plication of all methods of rehydration, was infrequent. One case of cellulitis was reported after subcutaneous
infu-sion.40Low rates of osteomyelitis (1%)
were reported from a 1946 series of IO
infusions,32and pooled data from adult
and pediatric patients from 1942 to 1977 revealed osteomyelitis rates of
0.6%.48More recent data from children
were not available, but infection rates would likely be lower given improve-ments in sterile technique. The 1 case of peritonitis in a patient with IP infu-sion was not felt to be attributable to the infusion but to the underlying disease. Two other serious events were identified: a possible aspiration in a patient who was receiving NG re-hydration and 2 cases of compart-ment syndrome in patients who were receiving IO infusions. Although pre-vious studies have shown that oral rehydration has fewer complications
than IV rehydration,44we did not
an-alyze the frequency of these adverse events in our review. As such, it is not possible to compare the frequency of complications with NG, IO, IP, or sub-cutaneous rehydration to those of IV or oral treatment.
Overall, the data support a role for NG rehydration as an alternative to IV re-hydration when patients are unable to be rehydrated orally. IV access can be used when NG rehydration fails, and IO access can be used if an IV line is not quickly obtainable. It is important to note that specialized techniques for in-travascular access, including central vein catheterization and neonatal um-bilical vein catheterization, were not reviewed here but remain available to
the clinician. If none of the above-mentioned techniques are successful or safely available, IP rehydration and
subcutaneous rehydration can be
used as life-saving measures, although the data supporting their use are limited.
The articles summarized here include data from poor and resource-rich environments. As such, the results are applicable to either setting. How-ever, they are likely to be particularly relevant to clinicians who work in resource-limited settings, where lim-ited supplies necessitate flexible treat-ment plans. In these situations, sup-plies such as sterile fluids or tubing may be limited, which makes tech-niques such as NG rehydration with ORS more accessible. In addition, NG rehydration can be accomplished by parents using a syringe, which frees up limited nursing resources. In other situations, training or experience with IV cannulation may be limited. Meth-ods such as IO, subcutaneous, or IP re-hydration may represent life-saving alternatives if IV access cannot be obtained.
The results of our review are limited by several factors. Our search terms, al-though broad, focused on hydration and may have missed patients in shock, severe trauma, or cardiac ar-rest. We also limited our data to hu-man pediatric studies and required an outcome measure or complication be documented. In particular, the limited number of studies on IO infusions may have been a result of these limitations, because the IO literature may focus more on emergent resuscitation. Our data are also limited by the different inclusion criteria, protocols, and pri-mary end points in each study. Even the definitions of degree of dehydra-tion varied from article to article. These factors made it difficult to group studies or perform any quantitative
analysis. In addition, the sample size for most of the studies we identified was small. Even for the randomized controlled trials that compared IV to NG rehydration, sample sizes were less than 100 patients. This number may have been too small to detect a small difference in effectiveness or adverse events between techniques. The largest studies identified had no comparison groups. Finally, our re-view focused on the effectiveness of these techniques, but we did not con-sider the paucity of data on the rela-tive discomfort experienced by pa-tients undergoing each procedure.
CONCLUSIONS
Dehydration is a common presenting condition of children worldwide and plays a significant role in many of the leading causes of mortality in children younger than 5 years. Various meth-ods of pediatric rehydration are avail-able to the clinician, each with its unique utility and limitations. In set-tings with limited material and human resources, it is helpful to have a clear understanding of alternative rehydra-tion methods.
REFERENCES
1. United Nations Children’s Fund. State of the word’s children. Available at: www.unicef. org/sowc08. Accessed March 28, 2010
2. Spandorfer P, Akessandrini EA, Joffe MD, Lo-calio R, Shaw KN. Oral versus Intravenous rehydration of moderately dehydrated children: a randomized, controlled trial.
Pe-diatrics. 2005;115(2):295–301
3. American Academy of Pediatrics, Provi-sional Committee on Quality Improvement, Subcommittee on Acute Gastroenteritis.
Practice parameter: the management of acute gastroenteritis in young children. Pe-diatrics. 1996;97(3):424 – 436
4. Gremse DA. Effectiveness of nasogastric
re-hydration in hospitalized children with acute diarrhea.J Pediatr Gastroenterol Nutr. 1995;21(2):145–148
5. Hidayat S, Srie Enggar KD, Pardede N, Ismail R. Nasogastric drip rehydration therapy in
acute diarrhea with severe dehydration.
Paediatr Indones. 1988;28(3– 4):79 – 84
6. Nager AL, Wang VJ. Comparison of nasogas-tric and intravenous methods of
rehydra-tion in pediatric patients with acute dehy-dration.Pediatrics. 2002;109(4):566 –572
7. Varavithya W, Posayanond P, Tontisirin K, Chernjitra L, Kashemsant C. Oral hydration in infantile diarrhoea.Southeast Asian J
Trop Med Public Health. 1978;9(3):414 – 419
8. Pignatelli S, Simporè J, Ruggieri M, Musu-meci S. Effectiveness of forced rehydration and early re-feeding in the treatment of
acute diarrhoea in a tropical area [in Ital-ian]. Minerva Pediatr. 2000;52(7– 8): 357–366
9. Pignatelli S, Musumeci S. Comparison of
three oral rehydration strategies in the treatment of acute diarrhea in a tropical country.Curr Ther Res. 2003;64(3):189 –202
10. Green SD. Treatment of moderate and se-vere dehydration by nasogastric drip.Trop
Doct. 1987;17(2):86 – 88
11. Seriki O, Olambiwonnu NO. Management of moderately severe dehydration by continu-ous intra-gastric infusion of electrolyte
so-lution.Trop Doctor. 1978;8(3):134 –136
12. Sammartino L, James D, Goutzamanis J, Lines D. Nasogastric rehydration does have a role in acute paediatric bronchiolitis.J Paediatr Child Health. 2002;38(3):321–322
13. Yiu WL, Smith AL, Catto-Smith AG. Nasogas-tric rehydration in acute gastroenteritis.J Paediatr Child Health. 2003;39(2):159 –161
14. Armon K, Stephenson T, MacFaul R,
Ec-cleston P, Werneke U. An evidence and con-sensus based guideline for acute diarrhoea
management. Arch Dis Child. 2001;85(2): 132–142
15. Duke T, Mokela D, Frank D, et al. Manage-ment of meningitis in children with oral
fluid restriction or intravenous fluid at maintenance volumes: a randomised trial.
Ann Trop Paediatr. 2002;22(2):145–157
16. Perng CL, Lin HJ, Chen CJ, Lee FY, Lee SD, Lee CH. Characteristics of patients with
bleed-ing peptic ulcer requirbleed-ing emergency en-doscopy and aggressive treatment. Am J Gastroenterol. 1994;89(10):1811–1814
17. Banerjee S, Singhi SC, Singh S, Singh M. The intraosseous route is a suitable alternative to intravenous route for fluid resuscitation
in severely dehydrated children.Indian Pe-diatr. 1994;31(12):1511–1520
18. Daga SR, Gosavi DV, Verma B. Intraosseous access using butterfly needle.Trop Doct. 1999;29(3):142–144
19. Goldstein B, Doody D, Briggs S. Emergency
intraosseous infusion in severely burned children. Pediatr Emerg Care. 1990;6(3): 195–197
20. Hurren JS, Dunn KW. Intraosseous infusion for burns resuscitation.Burns. 1995;21(4):
285–287
21. Rutter JM. Resuscitation in a shocked in-fant.Br J Hosp Med. 1993;50(8):487
22. Harte FA, Chalmers PC, Walsh RF, Danker P R , S h e i k h F M . I n t r a o s s e o u s fl u i d administration: a parenteral alternative in
pediatric resuscitation.Anesth Analg. 1987; 66(7):687– 689
23. Sacchetti A, Linkenhelmer R. On the effec-tiveness of intraosseous infusion.J Emerg Med. 1988;6(5):433
24. Alawi KA, Morrison GC, Fraser DD, Al-Farsi S,
Collier C, Kornecki A. Insulin infusion via an intraosseous needle in diabetic ketoacido-sis. Anaesth Intensive Care. 2008;36(1): 110 –112
25. McNamara RM, Spivey WH, Unger HD,
Ma-lone DR. Emergency applications of in-traosseous infusion.J Emerg Med. 1987; 5(2):97–101
26. Ellemunter H, Simma B, Trawoger R, Maurer H. Intraosseous lines in preterm and full term neonates.Arch Dis Child Fetal
Neona-tal Ed. 1999;80(1):F74 –F75
27. Ramet J, Clybouw C, Benatar A, Hachimi-Idrissi S, Corne L. Successful use of an in-traosseous infusion in an 800 grams pre-term infant.Eur J Emerg Med. 1998;5(3): 327–328
28. Martino Alba R, Ruiz Lopez MJ, Casado Flores J. Use of the intraosseous route in
resuscitation in a neonate.Intensive Care Med. 1994;20(7):529
29. Galpin RD, Kronick JB, Willis RB, Frewen TC. Bilateral lower extremity compartment syn-dromes secondary to intraosseous fluid re-suscitation.J Pediatr Orthop. 1991;11(6): 773–776
30. Wright R, Reynolds S, Nachtsheim B. Com-partment syndrome secondary to pro-longed intraosseous infusion. Pediatr Emerg Care. 1994;10(3):157–159
31. Evans RJ, Jewkes F, Owen G, McCabe M, Palmer D. Intraosseous infusion: a tech-nique available for intravascular adminis-tration of drugs and fluids in the child with burns.Burns. 1995;21(7):552–553
32. Heinild S, Sondergaard T, Tudvad F. Bone marrow infusions in childhood: experi-ences from a thousand infusions.J Pediatr. 1947;30(4):400 – 412
33. Agusto-Odutola T. The intraperitoneal ad-ministration of physiological saline solution in the rehydration of children at the casu-alty department of the Lagos University teaching hospital.West Afr Med J Niger Pract. 1971;20(5):324 –326
34. Carter FS. Intraperitoneal transfusions as a method of re-hydration in the African child.
East Afr Med J. 1953;30(12):499 –505
35. Mahalanabis D, Sack RB, Kaplan J, Jacobs B, Mondal A. Intraperitoneal fluid therapy in cholera and non-cholera diarrhoea: with special emphasis on the treatment of in-fants and children.Bull World Health Organ. 1970;42(6):837– 846
36. Noerasid H, Soeparto P, Rudyanto B, Sugi-janto S, Hamid A, Saraswati A. Intraperito-neal fluid therapy in children.Paediatr In-dones. 1975;15(7– 8):211–218
37. Ransome-Kuti O, Elebute O, Agusto-Odutola T, Ransome-Kuti S. Intraperitoneal fluid in-fusion in children with gastroenteritis.Br Med J. 1969;3(5669):500 –503
38. VanRooyen MJ, VanRooyen JB, Sloan EP. The use of intraperitoneal infusion for the out-patient treatment of hypovolemia in Soma-lia.Prehosp Disaster Med. 1995;10(1):57–59
39. Wenzel RP, Phillips RA. Intraperitoneal infu-sions for initial therapy of cholera.Lancet. 1971;2(7722):494 – 495
41. Steffey JM. Hypodermoclysis in infants and chil-dren.J Iowa State Med Soc. 1963;53:393–396
42. Hall BD. Complications of hypodermoclysis (re-emphasis with a case presentation).J Ky Med Assoc. 1968;66(7):626 – 627
43. Ozuah PO, Avner JR, Stein RE. Oral rehydra-tion, emergency physicians, and practice parameters: a national survey.Pediatrics. 2002;109(2):259 –261
44. Fonseca BK, Holdgate A, Craig JC. Enteral vs
intravenous rehydration therapy for chil-dren with gastroenteritis: a meta-analysis
of randomized controlled trials.Arch Pedi-atr Adolesc Med. 2004;158(5):483– 490
45. Constans T, Dutertre JP, Froge E. Hypoder-moclysis in dehydrated elderly patients: lo-cal effects with and without hyaluronidase.
J Palliat Care. 1991;7(2):10 –12
46. Remington R, Hultman T. Hypodermoclysis to treat dehydration: a review of the
evi-dence. J Am Geriatr Soc. 2007;55(12): 2051–2055
47. Slesak G, Schnurle JW, Kinzel E, Jakob J, Dietz PK. Comparison of subcutaneous and intravenous rehydration in geriatric patients: a randomized trial.J Am Geriatr Soc. 2003;51(2):155–160
48. Rosetti VA, Thompson BM, Miller J, Mateer JR, Aprahamian C. Intraosseous infusion: an alter-native route of pediatric intravascular access.
DOI: 10.1542/peds.2010-0952 originally published online February 14, 2011;
2011;127;e748
Pediatrics
Shada Rouhani, Laura Meloney, Roy Ahn, Brett D. Nelson and Thomas F. Burke
Resource-Limited Care
Alternative Rehydration Methods: A Systematic Review and Lessons for
Services
Updated Information &
http://pediatrics.aappublications.org/content/127/3/e748
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/127/3/e748#BIBL
This article cites 46 articles, 7 of which you can access for free at:
Subspecialty Collections
grative_medicine_sub
http://www.aappublications.org/cgi/collection/complementary_-_inte
Complementary & Integrative Medicine following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2010-0952 originally published online February 14, 2011;
2011;127;e748
Pediatrics
Shada Rouhani, Laura Meloney, Roy Ahn, Brett D. Nelson and Thomas F. Burke
http://pediatrics.aappublications.org/content/127/3/e748
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.