International Journal of Medical Science and Current Research (IJMSCR)
Available online at: www.ijmscr.com
Volume2, Issue 3,Page No: 316-320 May-June 2019
316
Medicine ID-101739732
IJMSCR
Bacteriological Profile and Antimicrobial Drug Resistance Pattern of Urinary Tract
Pathogens
1
Arthi.K, 2GeethaBanu S* 1, 2
Assistant Professor, Department of Microbiology,
Meenakshi Ammal Dental College, Alapakkam Main Road,Maduravoyal, Chennai 600095, India
*Corresponding Author:
GeethaBanu S
Assistant Professor, Department of Microbiology
Meenakshi Ammal Dental College, Alapakkam Main Road,Maduravoyal, Chennai 600095, India
Type of Publication: Original Research Paper Conflicts of Interest: Nil
ABSTRACT
Urinary tract infections are among the most common infections worldwide for which empirical as well as over the counter medications are prescribed. Liberal use of antimicrobial agents have given rise to the emergence of multidrug resistant strains that are posing a threat to the community. This study was conducted on 135 urine samples received in the Microbiology laboratory of a General Hospital. Significant bacteriuria was observed in 19.3% of samples of which 85% were gram negative bacilli. Escherichia coli (64 %) and Klebsiella
pneumoniae (27%) were the common bacteria isolated. We also reported bacteria that were Extended spectrum
beta lactamase producing in 32% of the isolates and Amp C beta lactamase producing in 14%. All the bacteria isolated were sensitive to carbapenems. This study was conducted to emphasize the importance of culture and sensitivity testing and to curtail the use of a single antimicrobial agent for empirical use..
Keywords: antimicrobial, bacteriuria, multidrug, significant
INTRODUCTION
Urinary Tract Infections are one among the most common infections for clinic visits or inpatient admissions worldwide. They are also one among the reasons for which empirical antibiotic prescription is recommended. UTI is more common in women than men, however associated with complications in male patients. Bacteria implicated in the causation of UTI include Escherichia coli and Klebsiella, very commonly although other Gram negative bacilli, a few gram positive cocci and even fungus coud be the etiology. Common symptoms include fever, increase in frequency and burning micturition, urgency and lower abdominal pain. It has been noted that there is an increase in trend of antimicrobial resistance in urinary pathogens even in community acquired
immunocompromised individuals and hospital
acquired pathogens, multidrug resistant organisms have evolved in the general population due to reasons such as misuse of antibiotics, freely available over the counter drugs and indiscriminate use of antimicrobials in livestock. The primary mechanism of drug resistance could be attributed to random
mutations occurring spontaneously, enzymatic
degradation of antibiotics, alteration in the nature of bacterial proteins or due to changes in membrane permeability of antibiotics.[2]
This study was undertaken to analyse the percentage
of drug susceptibilities for the commonly
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
Pag
e
317
ETHICS APPROVAL: This study was approved by
the Institutional Review Board.
MATERIALS AND METHODS:
This study was conducted in a General hospital for a period of 3 months with a sample size of 135 subjects .Patients were given appropriate instructions for sample collection such as clean catch early morning midstream urine in a sterile container after cleaning the genital area with soap and water. The samples were transported to the Microbiology laboratory and were processed without any further delay. Samples were diluted 1:100 (100µl of urine with 900 µl of normal saline) and streaked onto MacConkey and 5% Sheep blood agar using a 100 µl volume calibrated loop. Plates were incubated aerobically with the agar surface down at 37°C in the presence of ambient air for 18-24 hours. Plates were read the next day
visually and a Gram stain was put up. Gram positive bacteria were processed further using catalase, slide and tube coagulase whereas for Gram negative bacteria, the basic biochemical reactions were carried out as per standard laboratory protocol. Antimicrobial susceptibility was carried out by Kirby Bauer’s disc diffusion method on Mueller Hinton agar and the antibiotics were chosen accordingly as per the Clinical Laboratory Standards and Institute (CLSI) guidelines. Interpretation of zone diameters and further testing of resistance pattern was also done according to CLSI guidelines.[3]
RESULTS.
This study was carried out on 135 urine samples received in the Microbiology laboratory during a time period of 3 months. Among the samples tested, 19.3% showed significant growth of bacteria.
Table1: Distribution of Samples With Reference To Colony Count
CFU/ml No.of samples (n=135)
102 Nil (0%)
103 18 (13%)
104 10 (7.4%)
105 26 (19.3%)
Cfu/ml- colony forming units/ml
Table 2: List of Bacteria Isolated
Total number of bacteria isolated (n=26)
GRAM POSITIVE COCCI (n=4) (15%) GRAM NEGATIVE BACILLI (n=22) (85%)
Staphylococcus aureus 4 (100%) Escherichia coli 14 (64%)
Klebsiella pneumoniae 6 (27%)
Pseudomonas aeruginosa 2 (9%)
Table 3: Susceptibility Pattern of The Bacterial Isolates
Gram Positive Cocci
BACTERIA PEN AK GM TET NITRO CIP NOR COT
S.aureus
(n=4)
50% 100% 100% 100% 100% 100% 100% 75%
All isolates were screened for Methicillin resistance using a cefoxitin 30µg disc on Mueller Hinton agar and all were found to be susceptible giving a zone diameter of more than 22mm.
e
318
e
318
e318
e
318
e318
e
318
e318
e
318
e318
e
318
e
318
e
318
e
318
e318
e
318
e318
e
318
e318
e
318
e318
e
318
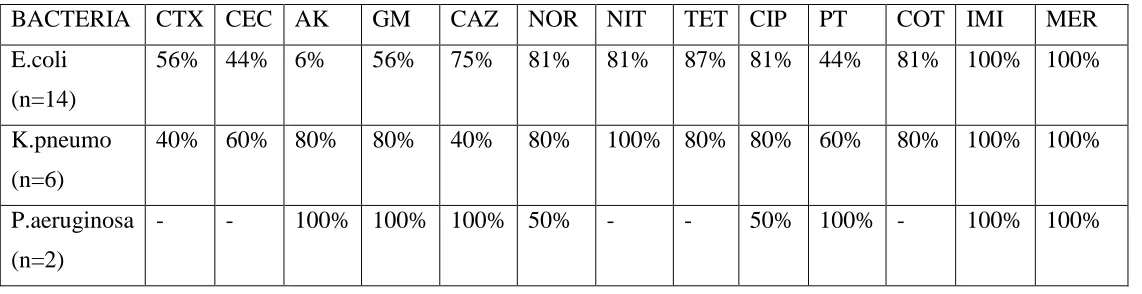
BACTERIA CTX CEC AK GM CAZ NOR NIT TET CIP PT COT IMI MER
E.coli
(n=14)
56% 44% 6% 56% 75% 81% 81% 87% 81% 44% 81% 100% 100%
K.pneumo
(n=6)
40% 60% 80% 80% 40% 80% 100% 80% 80% 60% 80% 100% 100%
P.aeruginosa
(n=2)
- - 100% 100% 100% 50% - - 50% 100% - 100% 100%
PEN- Penicillin, GM- Gentamicin,AK-Amikacin,TET-Tetracycline, NIT-Nitrofurantoin,
CIP-Ciprofloxacin, NOR-Norfloxacin, COT-Cotrimoxazole, CTX-Cefotaxime, CEC-Cefotaxime-clavulanate, CAZ-Ceftazidime, PT-Piperacillin Tazobactam,IMI- Imipenem, MER- Meropenem.
Table 4: Drug Resistance Pattern Of The Bacteria Isolated
GRAM POSITIVE COCCI
(n=4)
GRAM NEGATIVE BACILLI
(n=22)
MRSA 0 ESBL producers 7 (32%)
Carbapenemase producers 0 (0%)
Amp C producers 3(14%)
DISCUSSION
Among 135 urine samples tested 19.3% (26 samples) showed significant growth of bacteria with a colony count of 1,00,000 and above.It has been studied that urine colony counts of more than 1,00,000 cfu/ml have been associated with clinically significant illness and those less than 105 cfu/ml are infrequently associated with clinically significant disease.Over reporting of such cases may contribute to unnecessary antibiotic usage and spread of resistance. Hence colony counts of ≥ 105
cfu/ml were chosen as the cut off in our study [4] Majority of the patients in our study were females (69.6%) which could be attributed to factors such as the short urethra and its proximity to the perianal region [5].The prevalence rate of UTI in our study was similar to the one reported by Gupta et al which was 17.16%. Gram negative bacilli were isolated with a maximum of 85% and 15% of the bacteria isolated were gram positive cocci. Among the GNB isolated Escherichia coli were the majority (64%), while Klebsiella
pneumoniae and Pseudomonas aeruginosa amounted
to 27% and 9% of the gram negative isolates
respectively[6]. Escherichia coli was found to be the most common organism isolated in several other Indian studies conducted by Nivedita Thass (53.9%)
and Thattil (37.4%) followed by Klebsiella
pneumoniae[7]. Gram positive cocci caused only
15% of the UTIs in our set up, caused by
Staphlococcus aureus and were found to be
Methicillin sensitive.
Phenotypic testing was carried out to determine the drug resistance of the isolated bacteria. S.aureus was screened for methicillin resistance by disc diffusion method using a 30µg cefoxitin disk and all the isolates were found to be susceptible ruling out the presence of methicillin resistance.
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
Pag
e
319
pattern and all gram negative bacilli were susceptible to imipenem and meropenem by Kirby Bauer’s disk diffusion testing. mCIM (Modified Carbapenem Inactivation Method) test was performed for all the isolates to determine carbapenemase production and all the GNB were susceptible to Imipenem in mCIM testing. We noted that norfloxacin,nitrofurantoin, cotrimoxazole and carbapenems could be considered for first line treatment of UTI while awaiting the
culture reports as the response was found to be good based on the susceptibility rates. More or less a similar combination of drugs were suggested for first line treatment of UTI in a study by Angus.N.Oli et al [8]. It can be observed that different organisms show
varying patterns of susceptibility and
recommendation of a single drug for empirical treatment of UTI will remain a challenge for the
treating physician.
Figure 1: Testing of Amp C betalactamase resistance pattern
e
320
e
320
e320
e
320
e320
e
320
e320
e
320
e320
e
320
e
320
e
320
e
320
e320
e
320
e320
e
320
e320
e
320
e320
e
320
CONCLUSION
We are very much aware of the fact that E.coli is the commonest bacteria responsible for urinary tract infections, however the current change in trend is that drug resistant strains have become more common amongst this common bacteria, which is a warning for the healthcare fraternity to device control measures to stop spread of multidrug resistant strains. As a prelude to that we recommend culture and sensitivity testing for cases with clinical evidence of UTI and strict adherence to the reported susceptibility pattern.
REFERENCES
1. Rudrajit Paul. State of the globe: Rising antimicrobial resistance of pathogens in urinary tract infection. Journal of Global ID 2018; 10(3):117-118
2. Thattil S.J, Santhosh S. Prevalence of UTI in Different Age Groups in a Tertiary Care Hospital and their Antibiogram. IJCMR 2018; 5(1):
3. Performance Standards for Antimicrobial
Susceptibility Testing, CLSI, M100, 29th ed. Wayne,PA: ; 2019.
4. Patricia.M.Tille. Bailey & Scott's Diagnostic Microbiology, 14th ed. Missouri: Elsevier; 2017.
5. Kwon J.H, Maureen K, Hongyan Du F, Ari Robicsek MS, Lance R, Peterson, MD. Impact of Laboratory-Reported Urine Culture Colony Counts on the Diagnosis and Treatment of Urinary Tract Infection for Hospitalized Patients. American Journal of Clinical Pathology 2012; 137(5):
6. Kumari SS, Ramya T, Reddy K, Swarnalatha
G, Swapna V, Reddy BS. Aetiology And
Antibiotic Resistance Pattern Of
Uropathogens In A Tertiary Care Hospital. J. Evolution Med. Dent. Sci 2016; 5(75): 778-784
7. Smita Sood, Ravi Gupta. Antibiotic
Resistance Pattern of Community Acquired Uropathogens at a Tertiary Care Hospital in Jaipur, Rajasthan. Indian J Community Med. 2012; 37(1).
8. Oli A.N, Akabueze V.B, Ezeudu C.E, Eleje G.U, Ejiofor O.S, Ezebialu I.U, Oguejiofor C.B . Bacteriology and Antibiogram of Urinary Tract Infection among Female Patients in a Tertiary Health Facility in South Eastern Nigeria. The Open Microbiology