Rivaroxaban: A New Oral Factor Xa Inhibitor
Elisabeth Perzborn, Susanne Roehrig, Alexander Straub, Dagmar Kubitza,
Wolfgang Mueck, Volker Laux
Abstract—Rivaroxaban is a direct inhibitor of factor Xa, a coagulation factor at a critical juncture in the blood coagulation pathway leading to thrombin generation and clot formation. It is selective for human factor Xa, for which it has ⬎10 000-fold greater selectivity than for other biologically relevant serine proteases (half-maximal inhibitory concentration [IC50],⬎20mol/L). Rivaroxaban inhibits factor Xa in a concentration-dependent manner (inhibitory
constant [Ki], 0.4 nmol/L) and binds rapidly (kinetic association rate constant [kon], 1.7⫻10 7
mol/L⫺1 s⫺1) and reversibly (kinetic dissociation rate constant [koff], 5⫻10⫺
3
s⫺1). By inhibiting prothrombinase complex-bound (IC50,
2.1 nmol/L) and clot-associated factor Xa (IC50, 75 nmol/L), rivaroxaban reduces the thrombin burst during the propagation
phase. In animal models of venous and arterial thrombosis, rivaroxaban showed dose-dependent antithrombotic activity. In healthy individuals, rivaroxaban was found to have predictable pharmacokinetics and pharmacodynamics across a 5- to 80-mg total daily dose range, inhibiting factor Xa activity and prolonging plasma clotting time. In phase III clinical trials, rivaroxaban regimens reduced rates of venous thromboembolism in patients after total hip or knee arthroplasty compared with enoxaparin regimens, without significant differences in rates of major bleeding, showing that rivaroxaban has a favorable benefit-to-risk profile. (Arterioscler Thromb Vasc Biol. 2010;30:376-381.)
Key Words:anticoagulants 䡲 blood coagulation 䡲 factor Xa 䡲 rivaroxaban 䡲 venous thromboembolism
F
actor Xa is a coagulation factor that acts at the convergence point of the intrinsic and extrinsic pathways in the blood coagulation system.1It catalyzes the cleavage of prothrombinand, therefore, is critical for thrombin generation (Figure 1).1,2
Indirect factor Xa inhibitors, such as fondaparinux and biotinylated idraparinux, exert their thrombotic effect by binding to antithrombin; therefore, their efficacy depends on the circu-lating level of antithrombin. They are parenteral agents and cannot be administered orally.3Rivaroxaban is the first direct
factor Xa inhibitor to be licensed (in the European Union4and
several other countries) for the prevention of venous thrombo-embolism (VTE) in adult patients after elective hip or knee arthroplasty. Studies of rivaroxaban in the treatment of VTE, prevention of cardiovascular events in patients with acute coro-nary syndrome, prevention of stroke in those with atrial fibril-lation, and prevention of VTE in hospitalized medically ill patients are ongoing (Supplementary Table I, available at http:// atvb.ahajournals.org). Other direct factor Xa inhibitors are also in advanced development; apixaban and edoxaban (DU-176b) are undergoing phase III study, whereas betrixaban and YM150 have passed clinical phase II testing. This review discusses the properties of rivaroxaban and findings from clinical trials.
See accompanying article on page 369
Pharmacological Properties
Compound CharacteristicsRivaroxaban (chemical name 5-chloro-N-[[(5S )-2-oxo-3-[4-(3-
oxomorpholin-4-yl)phenyl]-1,3-oxazolidin-5-yl]methyl]thiophene-2-carboxamide) is a small-molecule factor Xa inhibitor (molec-ular weight, 436 g/mol). Rivaroxaban is only slightly soluble in organic solvents and is practically insoluble in water.5Plasma
protein binding varies between species (rats, 98.7%; rabbits, 76.6%5; and humans, 92%–95%),4 and serum albumin is the
main circulating binding component.4,5
Mode of Binding
As a prerequisite for potent activity, factor Xa inhibitors of the first generation, such as DX-9065a, needed a basic arginine-mimic P1 group for direct electrostatic interaction with Asp189 in the S1 pocket of factor Xa. However, those basic groups are also generally critical for oral bioavailability. The X-ray crystal structure of rivaroxaban in complex with human factor Xa6 revealed a
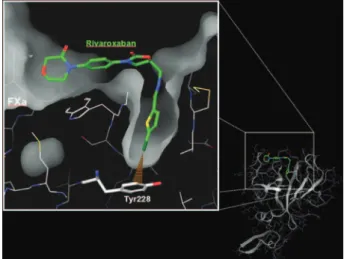
different binding mode for the S1 pocket, which no longer requires the P1 group to be basic. Instead, the key interaction in the S1 pocket involves the chlorine substituent of the chlorothio-phene moiety, which interacts with the aromatic ring of Tyr228 at the bottom of the S1 pocket (Figure 2). This novel chlorine–Tyr228 interaction enabled the combination of high potency and sufficient oral bioavailability for the nonbasic compound rivaroxaban.
Preclinical In Vitro and In Vivo
Pharmacological Profile
In Vitro StudiesFactor Xa Inhibition
Rivaroxaban inhibits factor Xa in a concentration-dependent manner (inhibitory constant [Ki], 0.4 nmol/L), and it is a
Received January 6, 2010; revision accepted January 15, 2010. From Bayer Schering Pharma AG, Wuppertal, Germany.
Correspondence to Elisabeth Perzborn, PhD, Cardiovascular Pharmacology, Pharma R&D Discovery Research, Bayer Schering Pharma AG, Aprather Weg 18a, D-42096 Wuppertal, Germany. E-mail [email protected]
© 2010 American Heart Association, Inc.
Arterioscler Thromb Vasc Biolis available at http://atvb.ahajournals.org DOI: 10.1161/ATVBAHA.110.202978
competitive inhibitor of the amidolytic activity of factor Xa.7It
has a rapid onset of action (kinetic association rate constant [kon], 1.7⫻10
7mol/L⫺1s⫺1) and is reversible (kinetic dissoci-ation rate constant [koff], 5⫻10⫺
3s⫺1).8Rivaroxaban inhibits prothrombinase-bound (half-maximal inhibitory concentration [IC50], 2.1 nmol/L)7 and clot-associated factor Xa (IC50, 75 nmol/L).9
Rivaroxaban was found to be selective for human factor Xa, for which it has⬎10 000-fold greater selectivity than for other biologically relevant serine proteases (IC50,⬎20mol/L).7The inhibition of factor Xa is species-dependent, as was shown for a number of factor Xa inhibitors.10 –12 Rivaroxaban showed a
similar affinity to purified human and rabbit factor Xa (IC50, 0.7 nmol/L and 0.8 nmol/L, respectively) but showed lower affinity to rat factor Xa (IC50, 3.4 nmol/L).
In commercially available chromogenic assays designed for measuring heparins in human plasma, rivaroxaban concentration-dependently inhibited factor Xa activity, with IC50 values between 21 and 80 ng/mL, depending on the anti-factor Xa assay.13
Inhibition of Thrombin Generation
In vitro studies in platelet-poor and platelet-rich plasma demonstrated that rivaroxaban prolonged the initiation phase of thrombin generation and reduced the thrombin burst produced in the propagation phase.14,15 In human plasma
obtained from healthy volunteers receiving rivaroxaban, ri-varoxaban inhibited thrombin generation at clinically relevant plasma concentrations and, thus, the propagation processes of coagulation through the inhibition of factor Xa generated via the intrinsic and extrinsic coagulation pathways.
Plasma Clotting Times
Rivaroxaban demonstrated effective anticoagulant effects in human plasma; it prolongs prothrombin time (PT) and acti-vated partial thromboplastin time in a concentration-dependent manner, with greater sensitivity for PT.7However,
the prolongation of clotting time varies depending on the PT
or activated partial thromboplastin time reagent used because the reactivity of rivaroxaban in the clotting assays is influenced by the composition of the reagents.16,17 This
variation cannot be reduced by conversion of PT values given in seconds to international normalized ratio values17;
therefore, PT and activated partial thromboplastin time are not useful for measuring the pharmacodynamic effects of rivaroxaban.
Thrombin–Thrombomodulin-Activated Protein C System
The coagulation pathway comprises negative and positive feed-back reactions to regulate hemostasis, and anticoagulants at therapeutic doses ideally should not interfere with the negative feedback mechanisms important in downregulating coagulation. One of the negative feedback reactions is the thrombin– thrombomodulin-activated protein C system, which limits fur-ther thrombin generation by inhibiting factor Va and factor VIIIa. In in vitro investigations of human plasma from healthy individuals or protein C-deficient plasma, factor Xa inhibitors, such as rivaroxaban, inhibited thrombin generation in a concentration-dependent manner after stimulation by tissue fac-tor and in the presence or absence of thrombomodulin.18This
suggests that rivaroxaban does not measurably interfere with the thrombin–thrombomodulin-activated protein C system.18
Inter-estingly, direct thrombin inhibitors, such as melagatran and dabigatran, also showed a concentration-dependent inhibition of thrombin generation over the whole range in the absence of thrombomodulin or in protein C-deficient plasma but in-creased thrombin generation at low concentrations in the pres-ence of thrombomodulin.18,19This suggests that low
concentra-tions of a direct thrombin inhibitor may partly suppress the negative feedback by activated protein C. However, whether this effect will influence clinical efficacy or safety remains to be investigated.
Platelet Aggregation
Rivaroxaban does not affect platelet aggregation induced by collagen, adenosine diphosphate, the selective agonist of pros-taglandin H2/thromboxane A2 receptor U46619, or throm-bin.20,21 However, rivaroxaban effectively and
concentration-dependently inhibited tissue factor-induced platelet
Figure 2.The entire X-ray crystal structure of factor Xa (FXa) with a focus on the active site showing the key interaction between rivaroxaban and Tyr228 in the S1 pocket.
Intrinsic pathway Tenase complex Extrinsic pathway Prothrombinase complex Prothrombin Thrombin Fibrinogen Fibrin Phospholipids Factor Va–Factor Xa Ca2+ Free Factor Xa Factor XIa Factor IXa Factor VIIIa Phospholipids Ca2+ Rivaroxaban Factor VIIa Tissue factor Phospholipids Ca2+
Figure 1.Role of factor Xa in the coagulation cascade. Tissue factor/factor VIIa activates factor X and factor IX. Factor IXa also activates factor X. Factor Xa binds factor Va on membrane sur-faces. The prothrombinase and tenase trigger the amplified
for-mation of thrombin.2,53Rivaroxaban inhibits factor Xa, free or
aggregation by the inhibition of thrombin generation (IC50, 0.06 mol/L) in defibrinated plasma.22 In addition to the
anticoagulant effects of a factor Xa inhibitor, this indirect effect on platelet aggregation may be particularly beneficial for the prevention or treatment of arterial thrombosis.
In Vivo Studies
Venous Thrombosis Models
Rivaroxaban reduced thrombus formation7,23 in venous
thrombosis models (fibrin-rich and platelet-poor) in which a combination of stasis and an injection of tissue factor was used to induce thrombus formation. In rabbits, rivaroxaban was administered orally, leading to a half-maximal effective dose (ED50) of 1.3 mg/kg23; in rats, rivaroxaban was admin-istered intravenously, leading to ED50 of 0.1 mg/kg.7,24 These findings suggested rivaroxaban might reduce thrombus forma-tion in humans. In a rabbit thrombosis model, rivaroxaban also inhibited thrombus growth of preformed clots in the jugular vein (assessed by measuring the accretion of radiolabeled fibrino-gen),23which supported further research in VTE treatment.
Arterial Thrombosis Models
Rivaroxaban showed effective dose-dependent antithrombotic activity in arterial (fibrin-poor and platelet-rich) thrombosis models, such as the arteriovenous shunt model in rats and rabbits (ED50, 5.0 mg/kg after oral rivaroxaban in rats; ED50, 0.6 mg/kg after oral administration in rabbits7), and the ferric chloride
model in rats and mice (ED50, 2.4 mg/kg after intravenous rivaroxaban in rats; ED50, 1.0 mg/kg after intravenous rivaroxa-ban in mice24). These results are consistent with a role of the
coagulation system in arterial thrombus formation.
Bleeding Models
The antihemostatic effect of rivaroxaban was evaluated in well-characterized bleeding time models in rats (tail transec-tion bleeding time model) and rabbits (ear-bleeding time model). Bleeding times were not significantly affected at antithrombotic doses below the ED50required for antithrom-botic efficacy in the bleeding time models. At higher doses in the rat tail-bleeding time model, bleeding times were dose-dependently prolonged.7 Together with the antithrombotic
findings, these findings demonstrate that rivaroxaban might have a favorable efficacy-to-bleeding ratio.
Clinical Pharmacology
Rivaroxaban has a favorable safety and tolerability profile in healthy individuals.25,26
Pharmacodynamic and Pharmacokinetic Profiles
Rivaroxaban was found to have predictable pharmacokinetics and pharmacodynamics across a wide range of doses in healthy individuals (5– 80 mg total daily doses)25,26 and
patients undergoing total hip or total knee arthroplasty (5– 60 mg total daily doses).27
The inhibition of factor Xa activity and the prolongation of PT correlated strongly with the plasma concentrations of rivaroxaban in healthy individuals28and patients undergoing
total hip arthroplasty or total knee arthroplasty,27
corroborat-ing the predictability of the pharmacodynamics and pharma-cokinetics of rivaroxaban.
Studies in healthy individuals showed that rivaroxaban is rapidly absorbed, with maximum concentrations appearing 2 to 4 hours after tablet intake.4,25,26Oral bioavailability for the
10-mg dose (which has health regulatory authority approval for thromboprophylaxis after elective hip or knee arthroplasty in adult patients) is high (80%–100%).4 The mean terminal
half-life of rivaroxaban is 7 to 11 hours.4
The elimination of rivaroxaban from plasma was rapid, with no major or pharmacologically active circulating metab-olites detected in plasma.29Excretion occurred via renal and
fecal/biliary routes. Approximately two-thirds of the admin-istered dose is metabolized to inactive metabolites, with half then being eliminated renally and the other half eliminated by the fecal route. The remaining one-third of the administered dose undergoes direct renal excretion as unchanged active substance in the urine.29
Rivaroxaban is metabolized by a number of independent metabolic pathways involving different classes of enzymes; thus, rivaroxaban should be less prone to drug– drug interac-tions. The main oxidative metabolic pathway is hydroxylation at the morpholinone moiety and, to a lesser extent, at the oxazolidinone moiety, catalyzed by CYP3A4/3A5 and CYP2J2.30In addition, hydrolytic pathways were identified,
occurring at the morpholinone ring and the chlorothiophene amide moiety.
Effect of Rivaroxaban in Different Populations
Phase I and II clinical studies have investigated the effect of several factors on rivaroxaban pharmacokinetics and pharma-codynamics. The area under the plasma concentration curve was higher in healthy men and women older than age 75 years compared with younger men and women, but maximum plasma concentration was unaffected.31,32 Gender did not
affect the area under the plasma concentration curve or maximum plasma concentration of rivaroxaban.31,32 Area
under the plasma concentration curve was not affected by extreme body weight (ⱕ50 kg or ⬎120 kg), and although maximum plasma concentration was increased by 24% in those weighingⱕ50 kg, this increase was not considered to be clinically relevant.32 In patients with mild (creatinine
clearance, 50 –79 mL/min), moderate (creatinine clearance, 30 – 49 mL/min), or severe (creatinine clearance ⬍30 mL/ min) impairment of renal function, area under the plasma concentration curve was 44%, 52%, and 64% higher, respec-tively, compared with control subjects, whereas maximum plasma concentration was relatively unaffected.33In patients
with mild (Child–Pugh A) hepatic functional impairment, there were no clinically relevant differences in pharmacoki-netics and pharmacodynamics of rivaroxaban.34 Together,
these findings suggest that rivaroxaban can be administered to individuals with varying physical characteristics (age, gender, body weight, mild or moderate impairment of renal function, and mild hepatic functional impairment) at a fixed dose, with no requirement for dose adjustment or routine coagulation monitoring.4
Interaction With Food and Drugs
Phase I interaction studies have demonstrated no food interac-tions and no significant and few clinically relevant drug
inter-actions with rivaroxaban, with the exception of azole antimy-cotics or human immunodeficiency virus protease inhibitors. These strong inhibitors of CYP3A4 and P-glycoprotein lead to reduced clearance of rivaroxaban; therefore, rivaroxaban is not recommended in patients receiving these drugs. Strong CYP3A4 inducers may lead to reduced rivaroxaban plasma concentrations and should be coadministered with caution.4
No clinically significant interactions were observed when rivaroxaban was coadministered with the statin atorvastatin (a substrate of CYP3A4 and P-glycoprotein),35 the cardiac
glycoside digoxin (a substrate of P-glycoprotein),36 or the
benzodiazepine derivative midazolam (a substrate of CYP3A4).4 The histamine H
2-receptor antagonist ranitidine (a CYP3A4 inhibitor) and the antacid aluminum–magnesium hydroxide have no significant effect on the pharmacokinetics and pharmacodynamics of rivaroxaban.37
Coadministration of antiplatelet agents, such as the non-steroidal antiinflammatory drugs acetylsalicylic acid38 and
naproxen,39had no significant effect on the pharmacokinetics
and pharmacodynamics of rivaroxaban. The antiplatelet agent clopidogrel did not show a pharmacokinetic interaction with rivaroxaban.40
Clinical Trials in the Prevention of
Venous Thromboembolism
Phase II TrialsThe Oral Direct Factor Xa (ODIXa) program of four phase II dose-finding studies of rivaroxaban for the prevention of VTE in patients undergoing total hip or knee arthroplasty suggested that rivaroxaban 10 mg once daily (compared with approved enox-aparin doses) would provide the best balance between efficacy and safety.41– 44
Phase III Trials
In the orthopaedic setting, the phase III Regulation of Coagulation in Orthopaedic surgery to prevent deep vein thrombosis and pulmonary embolism (RECORD) program included⬎12 700 patients undergoing total hip arthroplasty or total knee arthroplasty.45– 48Patients were randomized to
oral rivaroxaban 10 mg once daily administered 6 to 8 hours after wound closure or after adequate hemostasis had been achieved, or subcutaneous enoxaparin 40 mg once daily starting 12 hours before surgery (enoxaparin dose approved in the European Union, North America, and other countries) in RECORD1, 2, and 3 or 30 mg twice daily administered 12 to 24 hours after wound closure (dose approved and more often used in North America) in RECORD4. In RECORD1 and 2, patients undergoing total hip arthroplasty were admin-istered rivaroxaban for 35⫾4 days. Enoxaparin was admin-istered for 35⫾4 days in RECORD1 or 12⫾2 days followed by placebo for up to 35⫾4 days in RECORD2. In RECORD3 and 4, patients undergoing total knee arthroplasty received prophylaxis for 12⫾2 days. All patients were followed-up for 30 to 35 days after the last dose of study medication.
The rivaroxaban regimens were significantly more effec-tive than both enoxaparin regimens at reducing the composite of symptomatic and asymptomatic (detected by systematic bilateral venography) deep vein thrombosis, nonfatal
pulmo-nary embolism, and all-cause mortality.45– 48Rates of major
bleeding did not differ significantly between rivaroxaban and enoxaparin regimens.45– 48 Also, the proportion of patients
with elevated liver enzymes (alanine aminotransferase level
⬎3-times the upper limit of the normal range) was low in the rivaroxaban and enoxaparin groups.45– 48
In a pooled analysis of the RECORD1– 4 data, the composite of symptomatic VTE and death was reduced for the rivaroxaban regimens compared with the enoxaparin regimens at day 12⫾2 (0.47% vs 0.97%;P⫽0.001) and in the planned treatment period (rivaroxaban or enoxaparin for 12⫾2 days [RECORD3 and 4] or 35⫾4 days [RECORD1 and 2], including the enoxaparin pla-cebo phase in RECORD2; 0.57% vs 1.32%;P⬍0.001). There were no statistical differences in the rates of major bleeding at any of the time points analyzed. The composite of major and clinically relevant nonmajor bleeding for the rivaroxaban and enoxaparin regimens were 2.85% vs 2.45% (P⫽0.186) at day 12⫾2 and 3.19% vs 2.55% (P⫽0.039) in the planned treatment period.49
Clinical Trials in the Treatment of
Venous Thromboembolism
The phase III EINSTEIN EXT study (NCT00439725) showed that in patients who had completed 6 or 12 months of previous therapy for acute VTE, there was a risk reduction of 82% for rivaroxaban vs placebo for recurrent symptomatic VTE.50
Re-search is ongoing in the EINSTEIN DVT (NCT00440193) and EINSTEIN PE (NCT00439777) studies (Supplementary Table I).
Other Studies
Rivaroxaban is also being studied for the prevention of cardio-vascular events in patients with acute coronary syndrome (ATLAS ACS TIMI 51; NCT00809965), stroke prevention in patients with atrial fibrillation (ROCKET AF51; NCT00403767),
and thromboprophylaxis in hospitalized medically ill patients (MAGELLAN; NCT00571649; Supplementary Table I).
Conclusion
Rivaroxaban was selected as a drug candidate based on its hypothetical therapeutic potential as a direct inhibitor of factor Xa, in vitro potency, demonstrated selectivity against factor Xa,7
anticoagulant activity in clotting assays in human plasma,7and
consistent in vivo antithrombotic activity in venous and arterial thrombosis models.7,23,24 Because of its favorable safety and
tolerability profile in healthy individuals and a positive benefit-to-risk ratio for the prevention of VTE in patients after total hip arthroplasty or total knee arthroplasty,41– 44the 10-mg once-daily
dose has been granted health regulatory authority approval for the prevention of VTE after elective hip or knee arthroplasty in adult patients.4 The oral bioavailability of rivaroxaban is an
advantage over parenteral anticoagulant agents and could pro-vide better convenience in outpatient settings.
The pharmacodynamic and pharmacokinetic profiles, which were found to be predictable,25–27together with the low
interac-tion potential with food or other drugs,4,35– 40the wide
therapeu-tic window,7 and the absence of a requirement for routine
coagulation monitoring,4enhance the likelihood that oral factor
Xa inhibitors such as rivaroxaban may become an alternative to vitamin K antagonists in patients at risk for thromboembolism.
Use of factor Xa inhibitors might also obviate the drawbacks of vitamin K antagonists, which include unpredictable pharmaco-dynamics and pharmacokinetics, multiple food– drug and drug– drug interactions, considerable interindividual variability in dose response, and requirement for regular coagulation monitoring.52
At present, there is a substantial clinical need for an oral anticoagulant to replace vitamin K antagonists for long-term prevention or treatment of patients with venous and arterial thromboembolic events. There is currently a variety of new, promising, oral anticoagulants at various stages of clinical evaluation, with the most advanced being the direct factor Xa inhibitor rivaroxaban and the direct thrombin inhibitor dabigat-ran (reviewed in this series).
One major focus in the development of drugs targeting 1 coagulation factor was factor Xa. Emerging data for rivar-oxaban and other potent factor Xa inhibitors, such as apixa-ban, betrixaapixa-ban, edoxaapixa-ban, and YM150, suggest that factor Xa is a highly promising target for new antithrombotic agents for short-term and long-term usage.
Orthopaedic surgery has proved to be a reliable clinical model for assessing the efficacy and safety profile of a new oral anticoagulant. Rivaroxaban has shown superiority over standard therapy with enoxaparin without significantly increasing the major bleeding rate;45– 48thus, it might be effective and safe in
other indications such as the prevention and treatment of VTE, the prevention of stroke in patients with atrial fibrillation, and the recurrence of cardiovascular events in patients with acute coro-nary syndrome. Thus, new oral factor Xa inhibitors such as rivaroxaban herald a new era of anticoagulation.
Acknowledgments
The authors acknowledge Li Wan, who provided medical writing services with funding from Bayer Schering Pharma AG and Johnson & Johnson Pharmaceutical Research & Development, LLC.
Disclosures
The authors are employees of Bayer Schering Pharma AG.
References
1. Ansell J. Factor Xa or thrombin: is factor Xa a better target?J Thromb Haemost.2007;5(Suppl 1):60 – 64.
2. Furie B, Furie BC. Mechanisms of thrombus formation.N Engl J Med. 2008;359:938 –949.
3. Weitz JI, Hirsh J, Samama MM. New antithrombotic drugs: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, 8th Edition.Chest.2008;133:234S–256S.
4. Xarelto. Summary of Product Characteristics. Available at: http:// www.xarelto.com/html/downloads/Xarelto_Summary_of_Product_ Characteristics_ May2009.pdf. 2009. Accessed January 14, 2010. 5. European Medicines Agency (EMEA). CHMP Assessment Report for
Xarelto. Available at: http://www.emea.europa.eu/humandocs/PDFs/EPAR/ xarelto/H-944-en6.pdf. 2008. Accessed January 14, 2010.
6. Roehrig S, Straub A, Pohlmann J, Lampe T, Pernerstorfer J, Schlemmer KH, Reinemer P, Perzborn E. Discovery of the novel antithrombotic agent 5-chloro-N-([(5S)-2-oxo-3-[4-(3-oxomorpholin-4-yl)phenyl]-1,3-oxazolidin-5-yl]methyl)thiophene-2-carboxamide (BAY 59-7939): an oral, direct Factor Xa inhibitor.J Med Chem. 2005;48:5900 –5908. 7. Perzborn E, Strassburger J, Wilmen A, Pohlmann J, Roehrig S,
Schlemmer KH, Straub A. In vitro and in vivo studies of the novel antithrombotic agent BAY 59-7939 —an oral, direct Factor Xa inhibitor.
J Thromb Haemost. 2005;3:514 –521.
8. Tersteegen A, Schmidt S, Burkhardt N. Rivaroxaban—an oral, direct Factor Xa inhibitor— binds rapidly to Factor Xa.J Thromb Haemost.
2007;5(Suppl 2):Abstract P-W-651.
9. Depasse F, Busson J, Mnich J, Le Flem L, Gerotziafas GT, Samama MM. Effect of BAY 59-7939 —a novel, oral, direct Factor Xa inhibitor— on clot-bound Factor Xa activity in vitro. J Thromb Haemost. 2005;3: Abstract P1104.
10. Abendschein DR, Baum PK, Martin DJ, Vergona R, Post J, Rumennik G, Sullivan ME, Eisenberg PR, Light DR. Effects of ZK-807834, a novel inhibitor of factor Xa, on arterial and venous thrombosis in rabbits.
J Cardiovasc Pharmacol. 2000;35:796 – 805.
11. Hara T, Yokoyama A, Morishima Y, Kunitada S. Species differences in anticoagulant and anti-Xa activity of DX-9065a, a highly selective factor Xa inhibitor.Thromb Res. 1995;80:99 –104.
12. Wong PC, Pinto DJ, Knabb RM. Nonpeptide factor Xa inhibitors: DPC423, a highly potent and orally bioavailable pyrazole antithrombotic agent.Cardiovasc Drug Rev. 2002;20:137–152.
13. Perzborn E, Harwardt M, Samama M. Assessment of Factor Xa chromo-genic assays for measuring the pharmacodynamics of rivaroxaban—an oral, direct Factor Xa inhibitor.Haemostaseologie.2010;in press:Abstract A-218 – 0051-00067.
14. Gerotziafas GT, Elalamy I, Depasse F, Perzborn E, Samama MM. In vitro inhibition of thrombin generation, after tissue factor pathway activation, by the oral, direct Factor Xa inhibitor rivaroxaban.J Thromb Haemost. 2007;5:886 – 888.
15. Perzborn E, Harwardt M, Huetter J. Inhibition of thrombin generation by rivaroxaban (BAY 59-7939)—an oral, direct Factor Xa inhibitor-in human plasma.Hamostaseologie. 2007;27:A47.
16. Samama MM, Martinoli J, Leflem L, Guinet C, Plu-Bureau G, Depasse F, Perzborn E. Assessment of laboratory assays to measure rivaroxa-ban—an oral, direct Factor Xa inhibitor. Thromb Haemost.Published online before print February 2, 2010. DOI: 10.1160/th09-03-0176. 17. Smith SA, Morrissey JH. Thromboplastin composition affects the
sensi-tivity of prothrombin time (PT) clotting tests to direct Factor Xa inhibi-tors.Blood.2007;110:Abstract 928.
18. Perzborn E, Harwardt M. Direct Thrombin Inhibitors, but Not Factor Xa Inhibitors, Enhance Thrombin Formation in Human Plasma by Interfering with the Thrombin–Thrombomodulin–Protein C System.Blood. (ASH Annual Meeting Abstracts). 2008;112:Abstract 528.
19. Furugohri T, Shiozaki Y, Muramatsu S, Honda Y, Matsumoto C, Isobe K, Sugiyama N. Different antithrombotic properties of factor Xa inhibitor and thrombin inhibitor in rat thrombosis models. Eur J Pharmacol. 2005;514:35– 42.
20. Perzborn E, Strassburger J, Wilmen A, Lampe T, Pernerstorfer P, Pohlmann J, Roehrig S, Schlemmer KH, Straub A. Biochemical and pharmacologic properties of BAY 59-7939, an oral, direct Factor Xa inhibitor. Pathophysiol Haemost Thromb. 2004;33(Suppl 2):Abstract PO079.
21. Hoppensteadt D, Neville B, Schultz C, Cunanan J, Duff R, Perzborn E, Misselwitz F, Fareed J. Interaction of BAY 59-7939 —a novel, oral, direct Factor Xa inhibitor—with antiplatelet agents: monitoring and ther-apeutic applications.J Thromb Haemost.2005;3 Suppl 1:Abstract P1717. 22. Perzborn E, Lange U. Rivaroxaban—an oral, direct Factor Xa inhibitor— inhibits tissue factor-mediated platelet aggregation.J Thromb Haemost.
2007;5(Suppl 2):Abstract P-W-642.
23. Biemond BJ, Perzborn E, Friederich PW, Levi M, Buetehorn U, Buller HR. Prevention and treatment of experimental thrombosis in rabbits with rivaroxaban (BAY 59-7939)—an oral, direct Factor Xa inhibitor.Thromb Haemost. 2007;97:471– 477.
24. Perzborn E, Arndt B, Fischer E, Harwardt M, Lange U, Trabandt A. Anti-thrombotic effects of rivaroxaban—an oral, direct Factor Xa inhibitor—in animal models of arterial and venous thrombosis: comparison with enox-aparin, an antithrombin-dependent anticoagulant. Eur Heart J. 2006; 27(Suppl):762 Abstract P4571.
25. Kubitza D, Becka M, Voith B, Zuehlsdorf M, Wensing G. Safety, pharma-codynamics, and pharmacokinetics of single doses of BAY 59-7939, an oral, direct factor Xa inhibitor.Clin Pharmacol Ther. 2005;78:412– 421. 26. Kubitza D, Becka M, Wensing G, Voith B, Zuehlsdorf M. Safety,
phar-macodynamics, and pharmacokinetics of BAY 59-7939 —an oral, direct Factor Xa inhibitor—after multiple dosing in healthy male subjects.Eur J Clin Pharmacol. 2005;61:873– 880.
27. Mueck W, Eriksson BI, Bauer KA, Borris L, Dahl OE, Fisher WD, Gent M, Haas S, Huisman MV, Kakkar AK, Kalebo P, Kwong LM, Misselwitz F, Turpie AG. Population pharmacokinetics and pharmacodynamics of rivaroxaban—an oral, direct factor xa inhibitor—in patients undergoing major orthopaedic surgery.Clin Pharmacokinet. 2008;47:203–216. 28. Mueck W, Becka M, Kubitza D, Voith B, Zuehlsdorf M. Population
rivaroxa-ban—an oral, direct Factor Xa inhibitor—in healthy subjects.Int J Clin Pharmacol Ther. 2007;45:335–344.
29. Weinz C, Schwarz T, Kubitza D, Mueck W, Lang D. Metabolism and excretion of rivaroxaban, an oral, direct Factor Xa inhibitor, in rats, dogs and humans.Drug Metab Dispos. 2009;37:1056 –1064.
30. Lang D, Freudenberger C, Weinz C. In vitro metabolism of rivaroxa-ban—an oral, direct Factor Xa inhibitor—in liver microsomes and hepa-tocytes of rat, dog and man.Drug Metab Dispos. 2009;37:1046 –1055. 31. Kubitza D, Becka M, Mueck W, Zuehlsdorf M. The effect of extreme age,
and gender, on the pharmacology and tolerability of rivaroxaban—an oral, direct Factor Xa inhibitor.Blood.2006;108:Abstract 905. 32. Kubitza D, Becka M, Zuehlsdorf M, Mueck W. Body weight has limited
influence on the safety, tolerability, pharmacokinetics, or pharmacody-namics of rivaroxaban (BAY 59-7939) in healthy subjects. J Clin Pharmacol. 2007;47:218 –226.
33. Halabi A, Maatouk H, Klause N, Lufft V, Kubitza D, Zuehlsdorf M, Becka M, Mueck W, Schaefers R, Wand D, Philipp T, Bruck H. Effect of renal impairment on the pharmacology of rivaroxaban (BAY 59-7939)—an oral, direct Factor Xa inhibitor.Blood.2006;108:Abstract 913.
34. Halabi A, Kubitza D, Zuehlsdorf M, Becka M, Mueck W, Maatouk H. Effect of hepatic impairment on the pharmacokinetics, pharmacody-namics and tolerability of rivaroxaban—an oral, direct Factor Xa inhib-itor.J Thromb Haemost.2007;5(Suppl 2):Abstract P-M-635.
35. Kubitza D, Mueck W, Becka M. No interaction between rivaroxaban—a novel, oral, direct factor Xa inhibitor—and atorvastatin.Pathophysiol Haemost Thromb. 2008;36:A40.
36. Kubitza D, Becka M, Zuehlsdorf M. No interaction between the novel, oral direct Factor Xa inhibitor BAY 59-7939 and digoxin. J Clin Pharmacol.2006;46:702 Abstract 11.
37. Kubitza D, Becka M, Zuehlsdorf M, Mueck W. Effect of food, an antacid, and the H2 antagonist ranitidine on the absorption of BAY 59-7939 (rivaroxaban), an oral, direct Factor Xa inhibitor, in healthy subjects.
J Clin Pharmacol. 2006;46:549 –558.
38. Kubitza D, Becka M, Mueck W, Zuehlsdorf M. Safety, tolerability, pharmacodynamics, and pharmacokinetics of rivaroxaban—an oral, direct Factor Xa inhibitor—are not affected by aspirin.J Clin Pharmacol. 2006;46:981–990.
39. Kubitza D, Becka M, Mueck W, Zuehlsdorf M. Rivaroxaban (BAY 59-7939)—an oral, direct Factor Xa inhibitor— has no clinically relevant interaction with naproxen.Br J Clin Pharmacol. 2007;63:469 – 476. 40. Kubitza D, Becka M, Mueck W, Zuehlsdorf M. Co-administration of
rivaroxaban—a novel, oral, direct Factor Xa inhibitor—and clopidogrel in healthy subjects.Eur.Heart J.2007;28(Suppl 1):189 Abstract P1272. 41. Turpie AG, Fisher WD, Bauer KA, Kwong LM, Irwin MW, Kalebo P, Misselwitz F, Gent M. BAY 59-7939: an oral, direct factor Xa inhibitor for the prevention of venous thromboembolism in patients after total knee replacement. A phase II dose-ranging study.J Thromb Haemost. 2005; 3:2479 –2486.
42. Eriksson BI, Borris LC, Dahl OE, Haas S, Huisman MV, Kakkar AK, Muehlhofer E, Dierig C, Misselwitz F, Kalebo P; ODIXa-HIP Study Investigators. A once-daily, oral, direct Factor Xa inhibitor, rivaroxaban
(BAY 59-7939), for thromboprophylaxis after total hip replacement.
Circulation.2006;114:2374 –2381.
43. Eriksson BI, Borris L, Dahl OE, Haas S, Huisman MV, Kakkar AK, Mis-selwitz F, Ka¨lebo P; ODIXa-HIP Study Investigators. Oral, direct Factor Xa inhibition with BAY 59-7939 for the prevention of venous thromboembolism after total hip replacement.J Thromb Haemost.2006;4:121–128. 44. Eriksson BI, Borris LC, Dahl OE, Haas S, Huisman MV, Kakkar AK,
Misselwitz F, Muehlhofer E, Kalebo P. Dose-escalation study of rivar-oxaban (BAY 59-7939)—an oral, direct Factor Xa inhibitor—for the prevention of venous thromboembolism in patients undergoing total hip replacement.Thromb Res. 2007;120:685– 693.
45. Eriksson BI, Borris LC, Friedman RJ, Haas S, Huisman MV, Kakkar AK, Bandel TJ, Beckmann H, Muehlhofer E, Misselwitz F, Geerts W; RECORD1 Study Group. Rivaroxaban versus enoxaparin for thrombo-prophylaxis after hip arthroplasty.N Engl J Med.2008;358:2765–2775. 46. Kakkar AK, Brenner B, Dahl OE, Eriksson BI, Mouret P, Muntz J, Soglian AG, Pap AF, Misselwitz F, Haas S. Extended duration rivar-oxaban versus short-term enoxaparin for the prevention of venous throm-boembolism after total hip arthroplasty: a double-blind, randomised con-trolled trial.Lancet. 2008;372:31–39.
47. Lassen MR, Ageno W, Borris LC, Lieberman JR, Rosencher N, Bandel TJ, Misselwitz F, Turpie AG. Rivaroxaban versus enoxaparin for throm-boprophylaxis after total knee arthroplasty. N Engl J Med. 2008;358: 2776 –2786.
48. Turpie AG, Lassen MR, Davidson BL, Bauer KA, Gent M, Kwong LM, Cushner FD, Lotke PA, Berkowitz SD, Bandel TJ, Benson A, Misselwitz F, Fisher WD. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): a randomised trial.Lancet. 2009;373:1673–1680.
49. Turpie AGG, Lassen MR, Kakkar AK, Eriksson BI, Misselwitz F, Bandel TJ, Homering M, Westermeier T, Gent M. A pooled analysis of four pivotal studies of rivaroxaban for the prevention of venous thromboembolism after orthopaedic surgery: effect on symptomatic venous thromboembolism and death, and bleeding.Haematologica.2009;94(Suppl 2):Abstract 0439. 50. Buller HR. Once-daily oral rivaroxaban versus placebo in the long-term
prevention of recurrent symptomatic venous thromboembolism. The Einstein-Extension Study. Late breaking abstract presented at 51st American Society of Haematology annual meeting and exposition, New Orleans, LA, December 5– 8, 2009. Abstract. http://ash.confex.com/ash/ 2009/webprogram/Paper25669.html. Accessed January 14, 2010. 51. Patel M, Becker R, Breithardt G, Hacke W, Halperin J, Hankey G,
Mahaffey K, Singer D, Califf R, Fox K. Rationale and design of the ROCKET AF study: comparison of rivaroxaban with warfarin for the prevention of stroke and systemic embolism in patients with atrial fibril-lation.Eur Heart J. 2009;30(Suppl):705.
52. Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G; American College of Chest Physicians. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians evidence-based clinical practice guidelines (8th Edition).Chest.2008;133:160S–198S.
53. Leadley RJ Jr. Coagulation factor Xa inhibition: biological background and rationale.Curr Top Med Chem. 2001;1:151–159.