Evaluating factors associated with implementing of
evidence-based practice in nursing
Jamileh Farokhzadian PhD,1Reza Khajouei PhD2,3 and Leila Ahmadian PhD4
1Assistant Professor, Department of Community Health Nursing, School of Nursing and Midwifery, Kerman University of Medical Sciences, Kerman, Iran
2Assistant Professor of Medical Informatics, Medical Informatics Research Center, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran
3Assistant Professor of Medical Informatics, Department of Health Information Management and Technology, Faculty of Management and Medical Information Sciences, Kerman University of Medical Sciences, Kerman, Iran
4Assistant Professor of Medical Informatics, Health Services Management Research Center, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran
Keywords
attitude, barriers, evidence-based practice, self-efficacy, supporting factors, training needs
Correspondence Dr Leila Ahmadian
Health Services Management Research Center, Institute for Futures Studies in Health
Kerman University of Medical Sciences Haft-bagh Highway
PO Box 7616911320, Kerman Iran
E-mail: [email protected], [email protected]
Accepted for publication: 14 October 2015 doi:10.1111/jep.12480
Abstract
Rationale, aims and objectives Evidence-based practice (EBP) has emerged as an inno-vation for quality improvement in health care. Nurses have important role in implementing EBP but they face many challenges in this context. Evaluation of factors influencing implementation of EBP seems necessary. The aims of this study were to examine nurses’ attitude towards EBP, their self-efficacy and training needs, as well as supporting factors and barriers for implementing EBP.
Methods A cross-sectional study was conducted on 182 nurses from four teaching hospi-tals in Kerman, Iran. Data were collected using a questionnaire consisting of two main sections; a section to collect socio-demographic information of participants and a section collecting information on five topics (staff’s attitude, self-efficacy skills of EBP, supporting factors, barriers and training needs for implementing EBP).
Results The majority (87.4%) of the nurses had not attended any formal training on EBP and 60% of them were not familiar with the concept of EBP. Nurses’ attitude towards EBP was unfavourable (2.57±0.99) and their self-efficacy skills of EBP were poor (2.93±1.06). The most important supporting factor was mentoring by nurses who have adequate EBP experience (3.65±1.17) and the biggest barrier was difficulty judging the quality of research papers and reports (2.46±0.95). There was a moderate demand for training in all areas of EBP (3.62±1.12).
Conclusions Nursing care needs to move towards quality improvement using EBP. It is necessary to equip nurses with knowledge and skills required for EBP. Managers should design an appropriate strategic plan by considering supporting factors and barriers for integrating EBP into clinical setting.
Introduction
Factors such as dramatic changes in health care system, increasing emphasis on quality of care, cost limitations [1], the widespread usage of new information technologies, increasing patient and professional expectations [2], pressures for the patient-centred care and transparency in delivering clinical care increasingly push the health care industry towards utilization of more scientific research globally [3,4]. Therefore, nursing profession as a practi-cal discipline is expected to be accountable for integrating the best research evidence into the decision-making process with the aim
of improving care [5–7]. To achieve this goal, evidence-based practice (EBP) was introduced as an important initiative to health care system [8].
EBP is more than the use of research results because it includes all forms of nursing knowledge [9]. EBP in nursing is the process by which nurses make clinical decisions using the best available research evidence, which is blended with their clinical expertise, patient preferences and clinical guidelines [10]. This definition of EBP ensures a more patient-centred approach. EBP by filling the gap between theory, research and practice improves patient out-comes. It has been recognized by the health care community as the
gold standard for delivery of safe and compassionate care [11]. The International Council of Nurses (ICN) claims nurses have a pivotal role for determining and implementing standards of clini-cal nursing practice. Therefore, EBP should underpin their practice [12]. EBP supports nurses in their accountability and provision of accurate information to patients and their families [13].
Currently, nurses have been somewhat aware of the importance and benefits of EBP for health care systems, patients and them-selves [10,14]. Nevertheless, implementing EBP is rather slow in nursing practice [15]. There is a considerable gap between what is known in the research evidence and what happens in practice so that patients often do not receive the best (or even optimal) nursing care [16]. For example, it has been shown that about 30–40% of patients do not receive care based on current scientific evidence and about 20–30% of the provided care is not needed or is even potentially harmful [12].
Studies conducted in various countries [1,17–20] revealed that implementing EBP in hospitals is a complex activity. Different issues have made integrating EBP into clinical practice difficult. Although from its original appearance in the early 1990s, the philosophies and methods of EBP has been changed over time to overcome some of the issues to optimize patients care the tie between scientific evidence, clinicians expertise and clinical envi-ronment need to be improved [21].
Researchers reported that ability to implement EBP depends on several important individual factors such as attitude, understand-ing, knowledge and self-efficacy (perceived ability) to perform EBP activities. In most of these studies, nurses’ self-efficacy, for example, their abilities in literature searching and assessment of research articles for implementing EBP, was low. Several studies [14,22–25] have revealed although nurses’ attitude towards EBP and its importance in clinical setting was positive, they were not familiar enough with principles of EBP. Nurses’ knowledge and skills were not desirable to implement EBP effectively [14,22,23]. It has been shown that most nurses are not fully aware of the meaning of EBP [24] and many nurses do not understand the concept of EBP [25].
Many studies reported a large number of barriers to EBP in recent years. A systematic review on 106 articles identified 1144 barriers for EBP, among which lack of resources was the most common barrier. The summary results showed that lack of time, inadequate skills, poor access to information resources, lack of knowledge and financial shortage are the next most common bar-riers to the implementation and use of EBP [26].
Like other countries, Iranian nurses need to use available research evidence in practice and be accountable for providing the best possible care. Nevertheless, EBP is a new phenomenon in Iran [4] and nursing practice is task-oriented [25,27]. Despite the growing body of research related to clinical practice and availabil-ity of different educational programmes and strategies, health care system in Iran faces many challenges to promote the use of EBP [4].
Limited Iranian literature examined nurses’ knowledge, attitude towards EBP [28,29], and barriers and supporting factors of EBP [4,25,30,31]. Although professional and individual characteristics such as attitude and self-efficacy were identified as predictor and modifiers of individual behaviours in the context of EBP [16,32], these have not been comprehensively examined in Iranian hospi-tals. Comprehensive assessment of these factors can help develop
appropriate strategies to promote EBP among nurses, to reduce or eliminate barriers and to develop comprehensive training pro-grammes in hospitals. The objective of this study was multifac-eted: to determine (1) nurses’ attitude towards EBP, (2) their self-efficacy in performing EBP, (3) barriers of EBP, (4) supporting factors of EBP, (5) nurses’ training needs in the context of EBP.
Materials and methods
This study is a part of a larger study. The results of the first part was published in [13]. The study was done on 730 nurses working in four referral teaching hospitals of a large medical university in Kerman. Kerman is the largest city in the southeast Iran with a population of around 722 000 [33]. Because of centralized decision-making policies in health care sector, the recruitment of nurses follows the same pattern in all hospitals [13]. Using Cochrane formula (d=0.06, α =0.05), a sample of 195 nurses were invited to participate in the study. Nurses with an academic degree in nursing and at least 1 year working experience as a nurse were included. Stratified sampling (according to the population of nurses in each hospital) was used to select participants randomly. A translated version of a previous questionnaire [18] was used to collect the data. For cross-cultural comparison of the translation [34], the original questionnaire was accurately translated into Persian (forward translations). The backward translation of Persian version was done by a proficient English translator. Then, its agreement with the original version was examined. Face valid-ity of the questionnaire and nurses’ perception about the items were checked. Three medical informatics specialists and eight faculty members of nursing confirmed the content validity of the questionnaire. Thirty nurses participated in the pilot test of the questionnaire and the reliability of each subsection of the ques-tionnaire was assessed using Cronbach’s alpha coefficients (α =0.71–0.94).
The questionnaire consisted of two main sections. The first section was concerning socio-demographic data such as partici-pants’ age, sex, degree of nursing, work position, duration of nursing experience, attending professional training and familiarity with EBP. The second section contained five subsections as follows to collect information concerning study objectives: (1) attitude towards EBP (five items on a five point Likert scale from strongly disagree to strongly agree), (2) level of self-efficacy related to EBP (nine items on a 5-point Likert scale from poor to excellent), (3) supporting factors for implementing EBP (six items on a 5-point Likert scale from least important to most important), (4) barriers of implementing EBP (nine items on a 5-point Likert scale from strongly disagree to strongly agree) and (5) training needs (seven items on a 5-point Likert scale from least important to most important). Five point responses were scored from 1 to 5 and the mean scores were calculated. The mean scores below 3, 3–4 and above 4 were considered as poor (unfavourable), moder-ate and desirable, respectively.
To collect the data, one of the authors distributed the paper questionnaires among participants and instructed them about the objectives of the study and how to fill out the questionnaires. Their consent was implied from their agreement to complete the ques-tionnaires. There was no ethical issue during the study and data collection.
We analysed the data by SPSS version 20 using descriptive statistics (frequency, percentage, mean and standard deviation) and inferential statistics [independent samplest-test, analysis of vari-ance (ANOVA) and Pearson correlation]. Level of significvari-ance was considered asP≤0.05.
Results
Demographic information
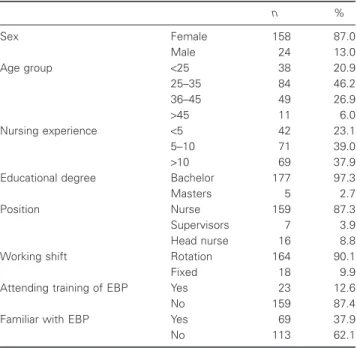
In this study, 182 out of the 195 respondents replied to the ques-tionnaires (93% response rate). The majority of participants were female (87%), aged between 25 and 35 years (46.2%), had between 5 and 10 years of nursing experience (39.0%) and had a bachelor degree (97.3%). Most of the respondents were in the position of a regular nurse (87.3%), had shift rotation (90.1%), had not attended any specific training on the implementation of EBP in patient care (87.4%) and were not familiar with the term evidence-based practice (62.1%; Table 1).
Attitude towards EBP
Table 2 presents nurses’ attitude towards EBP. Generally, the respondents’ attitude towards EBP was unfavourable (2.57±0.99). We found significant differences between mean scores of attitude of respondents based on different age groups (F=2.80,P<0.05) and years of nursing experience (F=4.24,
P<0.001). There were no statistically significant differences between attitude based on degree of nursing, participation in EBP training and other demographic variables (P>0.05).
Self-efficacy of EBP skills
Table 3 indicates that the nurses perceived their level of self-efficacy to undertake different EBP activities, as poor (2.93±1.06). There were significant differences between mean scores of self-efficacy based on years of nursing experience (F=4.95, P<0.01), working shifts (t=3.17, P<0.01) and
Table 1Demographic information (n= 182)
n % Sex Female 158 87.0 Male 24 13.0 Age group <25 38 20.9 25–35 84 46.2 36–45 49 26.9 >45 11 6.0 Nursing experience <5 42 23.1 5–10 71 39.0 >10 69 37.9
Educational degree Bachelor 177 97.3
Masters 5 2.7
Position Nurse 159 87.3
Supervisors 7 3.9
Head nurse 16 8.8
Working shift Rotation 164 90.1
Fixed 18 9.9
Attending training of EBP Yes 23 12.6
No 159 87.4
Familiar with EBP Yes 69 37.9
No 113 62.1
Table 2Nurses’ attitude towards EBP
Statement Mean SD
1. I prefer using more traditional methods instead of new approaches 3.34 1.20
2. Most research articles are not relevant to my daily practice 3.02 1.02
3. I believe evidence-based practice has only limited utility 2.82 0.96
4. I don’t like people questioning my clinical practice which is based on established methods. 1.99 0 .95
5. My workload is too high to keep up-to-date with all new evidence 1.69 0.86
Total 2.57 0.99
Table 3Self-efficacy of EBP skills
Statement Mean SD
I am able to
1. Identify clinical issues/problems. 3.26 0.95
2. Translate a clinical issue/problem into a well-formulated clinical question. 3.10 1.03
3. Distinguish between different types of questions (e.g. intervention, prognosis, harm and cost-effectiveness). 2.93 0.97
4. Conduct online searches (using databases and web search engines). 2.92 1.15
5. Relate research finding to my clinical practice and point out similarities and differences. 2.99 1.04
6. Use a checklist to assess research articles. 2.73 1.13
7. Read a research report and have a general notion about its strengths and weaknesses. 2.69 1.13
8. Apply an intervention based on the most applicable evidence. 2.82 1.09
9. Evaluate the application of intervention and identify areas of improvement. 2.92 1.11
attending training of EBP (t=3.87, P<0.001). No significant differences were found between self-efficacy based on other demographic variables (P>0.05). The Pearson’s correlation coef-ficient revealed significant correlation between the subscales of
self-efficacy and nurses attitude (r=0.20, P<0.01), indicating that nurses who had a positive attitude felt more confidence and competency in their abilities to implement EBP activities.
Supporting factors for implementing EBP
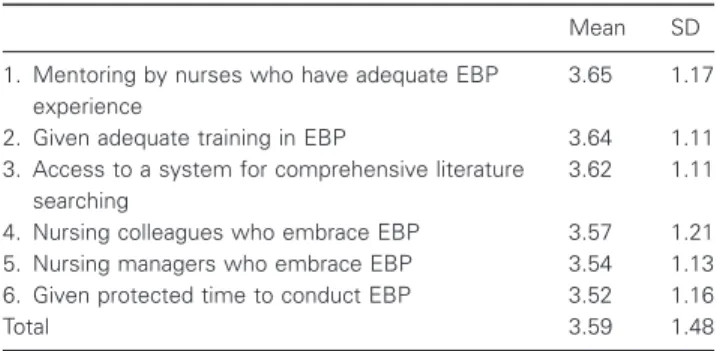
Nurses were asked about the importance of factors that can help them for implementing EBP (Table 4). Mean scores showed that nurses believed that all factors in Table 4 can moderately facilitate implementation of EBP.
Pearson’s correlation coefficient revealed significant relation-ships between the subscale of supporting factors and attitude and also self-efficacy (r=0.18, r=0.20, P<0.05, respectively). Nurses who had positive attitude towards EBP and felt more com-petent to implement EBP perceived more supporting factors for implementing EBP.
Barriers of implementing EBP
Table 5 presents the barriers of implementing EBP mentioned by nurses. The most important barrier was difficulty in judging the quality of research papers and reports (2.46±0.92) and the least important one was difficulty in finding time at work place to search for these resources (2.01±0.99).
Pearson’s correlation coefficient revealed significant relation-ship between the subscale of perceived barriers and self-efficacy of EBP skills (r=0.22,P<0.05). Nurses who felt more competent to implement EBP perceived more barriers for implementing EBP. There were no significant relationships between subscale of per-ceived barriers with attitude, supporting factors and training needs of EBP (P>0.05).
Training needs for implementing EBP
The nurses were asked to select the areas in which they need to receive training for implementing EBP. There was a moderate demand for training in all areas with very narrow range of mean scores from 3.4 to 3.78 (Table 6).
Pearson’s correlation coefficient revealed that the subscale of training needs have positive relationships with nurses attitude and self-efficacy of EBP skills (r=0.24 and 0.27, P<0.05, respectively).There were no significant relationships between training needs and other variables in the study (P>0.05).
Discussion
This study examined nurses’ attitude towards EBP, their self-efficacy of EBP skills, as well as, supporting factors, barriers and their training needs for implementing EBP. The findings showed that nurses’ attitude and self-efficacy were not desirable and there are many barriers for implementing EBP. They felt that for imple-menting EBP they need different supporting factors and training in an average level.
Findings indicated that majority of the nurses were not familiar with the term EBP and even had not heard of it. Findings are consistent with some previous studies conducted in Iran [35,36] and other countries [15,17]. This can be concluded from the result that most of the participants had not attended any specific training on EBP or even may not have had the opportunity to receive any EBP training.
Result showed that the majority of nurses are not sufficiently prepared for EBP because they had somewhat negative attitude towards EBP. The undesirable views of the participants could, to some extent, be explained by the controversy surrounding negative and unintended consequences of EBP besides its benefits, as dis-cussed in a newly published article by Mileset al. [21].
Moreover, self-efficacy of nurses to engage in EBP was low. These can result in the failure to proceed to EBP. Previous studies
Table 4Supporting factors for implementing EBP
Mean SD
1. Mentoring by nurses who have adequate EBP experience
3.65 1.17
2. Given adequate training in EBP 3.64 1.11
3. Access to a system for comprehensive literature searching
3.62 1.11
4. Nursing colleagues who embrace EBP 3.57 1.21
5. Nursing managers who embrace EBP 3.54 1.13
6. Given protected time to conduct EBP 3.52 1.16
Total 3.59 1.48
Table 5Barriers of implementing EBP
Mean SD
1. Difficulty in judging the quality of research papers and reports. 2.46 0.92
2. Difficulty in determining the applicability of research findings. 2.37 0.95
3. Inability to implement recommendations of research studies into clinical practice. 2.32 0.96
4. Inability to properly interpret the results of research studies. 2.31 0.94
5. Inability to understand statistical terms used in research articles. 2.29 0.99
6. Inadequate understanding of terms used in research articles. 2.21 0.90
7. Insufficient resources (e.g. equipment, materials) to implement EBP. 2.19 0.98
8. Insufficient time at work place to implement changes in their current practice. 2.09 0.95
9. Difficulty in finding time at work place to search for and read research articles and reports. 2.01 0.99
identified attitude and self-efficacy as important factors in imple-menting EBP [8,22,37]. The attainment of professional qualifica-tions and the ability to apply knowledge in practice are necessary for providing the nursing care of highest standard. However, these results support the fact that the dominant paradigm of nursing in Iran is a routine-based and traditional nursing care. This is worri-some because despite the academic degree of nurses (the majority were bachelors), they do not receive relevant and adequate infor-mation about EBP as a part of their curricula [29]. On the other hand, most of the nursing graduates with PhD and MSc degrees tend to work in educational institutions instead of clinical settings. These problems have increased challenges of EBP in Iran [38].
In our study, the relationship between attitude and self-efficacy skills of EBP supports the importance of nurses’ attitude in pro-moting EBP. Hence, it can be suggested that enhancing attitude towards EBP may be helpful to engage nurses in EBP activities. If nurses do not believe in the value of EBP, its implementation can be difficult. Meanwhile, the relatively negative attitude to EBP shown in this study might be due to their poor self-efficacy. Atti-tude and self-efficacy should be considered together as a gauge for implementing EBP and objectively be measured for evaluating overall success of EBP initiatives [9,37]. Nursing students in a study reported that self-efficacy have positive effects on their learning, academic motivation, skill development, job progress and professional behaviour [39].
In this study, nurses reported that the most important supporting factors for implementing EBP are mentoring by nurses having EBP experience and receiving sufficient training in EBP. In line with the present study, Brown et al. [11] reported that nurses acknowledged learning opportunities, discussion group and mentorship as facilitators for changing towards EBP. They believed that education alone is not enough to change practice. Mentorship is a necessary adjunct to educational courses due to the complexity of the nurses working environment. Mentors such as clinical nurse educators can provide support by setting up com-puter links to local library databases, providing relevant systematic reviews that summarize findings, circulating valid and reliable research literature within clinical settings, and introducing nurses to the Cochrane Library and EBP journals. As well, professional development courses on EBP and research inquiry courses can assist nurses in critically examining evidence [40].
The main barriers to adopting EBP were difficulty in judging the quality of research and determining the applicability of findings. Most of the reported barriers were consistent with the results of
previous studies [11,15,18,40]. The vast amount of literature high-lighted that lack of time is the greatest barrier [4,11,12,22,41–43], while in our study, lack of time was less important than other barriers. This difference may be because nurses in our study were not practising EBP activities and had low self-efficacy for involv-ing EBP. While lack of time is plausible, it may reflect other factors such as lack of knowledge, lack of interest and denying the need for EBP [4].
Significant differences were found between nurses’ attitude as well as their self-efficacy of EBP skills based on some demo-graphic variables (age groups, years of nursing experience, working shifts and attending EBP training). For example, nurses who had longer experience in nursing and attended EBP training were more confident in implementing EBP. This supports the finding of a previous study [44], which reported that new nurses who had limited practical knowledge and experience and difficulty in identifying client values felt less confident and willing to engage in decision making and EBP. Self-efficacy has been considered a vital factor in implementing EBP, while lack of self-efficacy and being accustomed to routine tasks were considered as barriers of EBP [45]. Researchers in two studies [16,46] reported that indi-vidual determinants such as beliefs and attitude, education, attend-ing educational programmes, participation in research activities and professional characteristics such as educational degree, and current position influence nurses use of research findings.
Nurses in this study stated a moderate demand for training in all areas of EBP particularly understanding what EBP is and conduct-ing literature searches. Therefore, the findconduct-ings may indicate a tendency for nurses with higher education to use the best available evidence in practice, which was consistent with the results of some previous studies [11,18]. Findings showed that although nursing research is advancing, nurses still struggle with how to implement EBP into clinical practice. To help them reach this goal, perceived barriers by nurses should be eliminated and the supporting factors should be provided. Previously, factors such as lack of training, knowledge, experience and negative attitudes were identified as the most important barriers for implementation of health informa-tion systems [47]. Likewise, these factors could prohibit the suc-cessful implementation of EBP and should be considered when conducting a readiness assessment for EBP.
This study has a limitation. The use of self-reported question-naire to evaluate self-efficacy of EBP skills may result in inflated scores. Future studies using tools and methods such as triangula-tion (observatriangula-tion, competency test and interview) can help deter-mining real skills and obtaining more reliable findings. However, this study shed lights on nurses’ attitude towards EBP, the main barriers and educational needs to attain it, and supporting factors that can help to overcome the barriers.
Implications for nursing
The findings suggest a need for greater efforts in promoting EBP in Iran particularity to gain competences in nurses. Nursing man-agers must be aware of nurses’ perceptions, required recourses to meet educational needs and motivating strategies to promote self-confidence in relation to EBP. This study creates an evidence-based foundation for organizational strategic planning and can help to determine opportunities and threats of implementing EBP. The findings of this study will also be useful for hospital and
Table 6Training needs of EBP
Mean SD
1. Understanding EBP 3.78 1.13
2. Conducting literature searches 3.67 1.17
3. Identifying clinical issues for implementing EBP 3.65 1.17
4. Conducting critical appraisal of articles 3.63 1.14
5. Synthesizing evidence 3.52 1.12
6. Understanding research and statistical terms and methods
3.47 1.08
7. Implementing recommendations in practice 3.40 1.06
nursing managers, policy- and decision-makers, and nursing edu-cators to develop appropriate strategies to promote EBP in the nursing community and to plan for reducing or eliminating barri-ers. These strategies may include assessment of training needs and corresponding modification of educational curricula, bringing creativity into different aspects of the educational curricula and developing comprehensive training programmes. Education will likely play an important role in changing less desirable attitude and behaviours of nurses. Future studies can help facilitate the process of applying knowledge into practice. In this regard, we suggest conducting qualitative and quantitative studies addressing benefits of EBP as a guide for the safe and high-quality nursing care.
Conclusions
Although EBP is crucial for providing quality nursing care, many requirements are needed to implement EBP in nursing. Attitude and self-efficacy of nurses to engage in EBP are not adequate and there are many barriers making it difficult to integrate EBP into practice. Nurses need to be equipped by knowledge, skills and positive attitude for using new methods to provide effective and high-quality care. This study highlighted the main barriers of implementing EBP and the supporting factors that can help to overcome the barriers. Moreover, the main areas in which nurses need to be trained are determined. Based on the results, training and continual support by experienced mentors or managers can improve the nurses’ ability and help to encourage the nurses’ confidence in using EBP.
Conflict of interests
The authors declare no conflict of interest.
Acknowledgements
The researchers would like to thank participating nurses who devoted so graciously a part of their time to participate in the study.
References
1. Boström, A.-M., Rudman, A., Ehrenberg, A., Gustavsson, J. P. & Wallin, L. (2013) Factors associated with evidence-based practice among registered nurses in Sweden: a national cross-sectional study.
BMC Health Services Research, 13 (1), 165.
2. Wan, T. T. (2006) Healthcare informatics research: from data to evidence-based management.Journal of Medical Systems, 30 (1), 3–7. 3. Ciliska, D., Dicenso, A. & Cullum, N. (1999) Centres of evidence-based nursing: directions and challenges.Evidence-Based Nursing, 2 (4), 102–104.
4. Mehrdad, N., Salsali, M. & Kazemnejad, A. (2008) The spectrum of barriers to and facilitators of research utilization in Iranian nursing.
Journal of Clinical Nursing, 17 (16), 2194–2202.
5. Gifford, W., Davies, B., Edwards, N., Griffin, P. & Lybanon, V. (2007) Managerial leadership for nurses’ use of research evidence: an inte-grative review of the literature. Worldviews on Evidence-Based Nursing, 4 (3), 126–145.
6. Spallek, H., Song, M., Polk, D. E., Bekhuis, T., Frantsve-Hawley, J. & Aravamudhan, K. (2010) Barriers to implementing evidence-based clinical guidelines: a survey of early adopters.Journal of Evidence Based Dental Practice, 10 (4), 195–206.
7. Estabrooks, C. A. (1998) Will evidence-based nursing practice make practice perfect?Canadian Journal of Nursing Research, 30, 15–36. 8. Thiel, L. & Ghosh, Y. (2008) Determining registered nurses’ readiness for evidence-based practice.Worldviews on Evidence-Based Nursing, 5 (4), 182–192.
9. Penz, K. L. & Bassendowski, S. L. (2006) Evidence-based nursing in clinical practice: implications for nurse educators. The Journal of Continuing Education in Nursing, 37 (11), 250–254.
10. Koivunen, M., Välimäki, M. & Hätönen, H. (2010) Nurses’ informa-tion retrieval skills in psychiatric hospitals–Are the requirements for evidence-based practice fulfilled?Nurse Education in Practice, 10 (1), 27–31.
11. Brown, C. E., Wickline, M. A., Ecoff, L. & Glaser, D. (2009) Nursing practice, knowledge, attitudes and perceived barriers to evidence-based practice at an academic medical center.Journal of Advanced Nursing, 65 (2), 371–381.
12. Breimaier, H. E., Halfens, R. J. & Lohrmann, C. (2011) Nurses’ wishes, knowledge, attitudes and perceived barriers on implementing research findings into practice among graduate nurses in Austria.
Journal of Clinical Nursing, 20 (11–12), 1744–1756.
13. Farokhzadian, J., Khajouei, R. & Ahmadian, L. (2015) Information seeking and retrieval skills of nurses: nurses readiness for evidence based practice in hospitals of a medical university in Iran. Interna-tional Journal of Medical Informatics, 84 (8), 570–577.
14. Mashiach Eizenberg, M. (2011) Implementation of evidence-based nursing practice: nurses’ personal and professional factors?Journal of Advanced Nursing, 67 (1), 33–42.
15. Pravikoff, D. S., Tanner, A. B. & Pierce, S. T. (2005) Readiness of US nurses for evidence-based practice: many don’t understand or value research and have had little or no training to help them find evidence on which to base their practice.AJN The American Journal of Nursing, 105 (9), 40–51.
16. Squires, J. E., Estabrooks, C. A., Gustavsson, P. & Wallin, L. (2011) Individual determinants of research utilization by nurses: a systematic review update.Implementation Science, 6 (1), 1–20.
17. Mokhtar, I. A., Majid, S., Foo, S.,et al. (2012) Evidence-based prac-tice and related information literacy skills of nurses in Singapore: an exploratory case study.Health Informatics Journal, 18 (1), 12–25. 18. Majid, S., Foo, S., Luyt, B.,et al. (2011) Adopting evidence-based
practice in clinical decision making: nurses’ perceptions, knowledge, and barriers. Journal of the Medical Library Association, 99 (3), 229–236.
19. Wallin, L., Boström, A. M. & Gustavsson, J. P. (2012) Capability beliefs regarding evidence-based practice are associated with applica-tion of EBP and research use: validaapplica-tion of a new measure.Worldviews on Evidence-based Nursing, 9 (3), 139–148.
20. McSherry, R., Artley, A. & Holloran, J. (2006) Research awareness: an important factor for evidence-based practice? Worldviews on Evidence-based Nursing, 3 (3), 103–115.
21. Miles, A., Asbridge, J. E. & Caballero, F. (2015) Towards a person-centered medical education: challenges and imperatives (I).Educación Médica, 16 (1), 25–33.
22. Koehn, M. L. & Lehman, K. (2008) Nurses’ perceptions of evidence-based nursing practice.Journal of Advanced Nursing, 62 (2), 209–215. 23. Stokke, K., Olsen, N. R., Espehaug, B. & Nortvedt, M. W. (2014) Evidence based practice beliefs and implementation among nurses: a cross-sectional study.BMC Nursing, 13 (1), 8.
24. Foo, S., Majid, S., Mokhtar, I.,et al. (2011) Nurses’ perception of evidence-based practice at the National University Hospital of Singa-pore. Journal of Continuing Education in Nursing, 42 (11), 522– 528.
25. Adib-Hajbaghery, M. (2007) Factors facilitating and inhibiting evidence-based nursing in Iran.Journal of Advanced Nursing, 58 (6), 566–575.
26. Sadeghi-Bazargani, H., Tabrizi, J. S. & Azami-Aghdash, S. (2014) Barriers to evidence-based medicine: a systematic review.Journal of Evaluation in Clinical Practice, 20 (6), 793–802.
27. Hajbaghery, M. A. & Salsali, M. (2005) A model for empowerment of nursing in Iran.BMC Health Services Research, 5 (1), 24.
28. Aghahoseini, S. (2011) Nurses ‘knowledge and attitude in evidence-based nursing in Kashan University of Medical Sciences’ teaching hospitals.Tabriz Nursing & Midwifery Journal, 6 (2), 45–54. 29. Heydari, A., Mazlom, S. R., Ranjbar, H. & Scurlock-Evans, L. (2014)
A study of Iranian nurses’ and midwives’ knowledge, attitudes, and implementation of evidence-based practice: the time for change has arrived.Worldviews on Evidence-Based Nursing, 11 (5), 325–331. 30. Khammarnia, M., Haj Mohammadi, M., Amani, Z., Rezaeian, S. &
Setoodehzadeh, F.(2015) Barriers to Implementation of evidence based practice in Zahedan Teaching Hospitals, Iran, 2014. Nursing research and practice.
31. Kermanshahi, S. & Parvinian, A. M. (2012) Barriers to implementa-tion of evidence-based care: viewpoints of nursing staff. Iranian Journal of Medical Education, 12 (2), 84–92.
32. Salbach, N. M. & Jaglal, S. B. (2011) Creation and validation of the evidence-based practice confidence scale for health care professionals.
Journal of Evaluation in Clinical Practice, 17 (4), 794–800. 33. Dehghan, M., Nayeri, N. D. & Iranmanesh, S. (2015) Validating the
PERSIAN version of the Hill-Bone’s Scale of ‘Compliance to High Blood Pressure Therapy’.British Journal of Medicine and Medical Research, 5 (2), 235–246.
34. Acquadro, C., Conway, K., Hareendran, A. & Aaronson, N. (2008) Literature review of methods to translate health-related quality of life questionnaires for use in multinational clinical trials.Value in Health, 11 (3), 509–521.
35. Moeintaghavi, A., Mokhtari, M. R., Alizadeh, F. L., Farazi, F. & Sohrabi, M. (2014) Evaluation of evidence based dentistry knowledge and usage among postgraduate dental students of Mashhad Dental School in 2012–2013.Journal of Mashhad Dental School, 38 (1), 61–70.
36. Sadeghi, M., Khanjani, N. & Motamedi, F. (2011) Knowledge, attitude and application of evidence based medicine (EBM) among residents of Kerman Medical Sciences University.Iranian Journal of Epidemiol-ogy, 7 (3), 20–26.
37. Lai, N., Teng, C. & Lee, M. (2010) The place and barriers of evidence based practice: knowledge and perceptions of medical, nursing and allied health practitioners in Malaysia.BMC Research Notes, 3 (279), 1–8.
38. Farsi, Z., Dehghan-Nayeri, N., Negarandeh, R. & Broomand, S. (2010) Nursing profession in Iran: an overview of opportunities and challenges.Japan journal of nursing science, 7 (1), 9–18.
39. Lauder, W., Holland, K., Roxburgh, M.,et al. (2008) Measuring com-petence, self-reported competence and self-efficacy in preregistration students.Nursing Standard, 22 (20), 35–43.
40. Ciliska, D. K., Pinelli, J., DiCenso, A. & Cullum, N. (2001) Resources to enhance evidence-based nursing practice.AACN Advanced Critical Care, 12 (4), 520–528.
41. McInerney, P. & Suleman, F. (2010) Exploring knowledge, attitudes, and barriers toward the use of evidence-based practice amongst aca-demic health care practitioners in their teaching in a South African University: a pilot study.Worldviews on Evidence-Based Nursing, 7 (2), 90–97.
42. O’Connor, S. & Pettigrew, C. M. (2009) The barriers perceived to prevent the successful implementation of evidence-based practice by speech and language therapists.International Journal of Language & Communication Disorders, 44 (6), 1018–1035.
43. Griffiths, J., Bryar, R., Closs, S.,et al. (2001) Barriers to research implementation by community nurses.British Journal of Community Nursing, 6 (10), 501–510.
44. Ferguson, L. & Day, R. (2007) Challenges for new nurses in evidence-based practice. Journal of Nursing Management, 15 (1), 107– 113.
45. Adib Hajbaghery, M. (2007) Factors facilitating and inhibiting evidence-based nursing in Iran.Journal of Advanced Nursing, 58 (6), 566–575.
46. Estabrooks, C. A., Floyd, J. A., Scott-Findlay, S., O’Leary, K. A. & Gushta, M. (2003) Individual determinants of research utilization: a systematic review. Journal of Advanced Nursing, 43 (5), 506– 520.
47. Ahmadian, L., Khajouei, R., Nejad, S. S., Ebrahimzadeh, M. & Nikkar, S. E. (2014) Prioritizing barriers to successful implementation of hospital information systems.Journal of Medical Systems, 38 (12), 1–6.