MAMMAPLASTY
Introduction
Hypomastia is a common entity that is either develop-mental or due to postpartum involution. Women seek breast augmentation to improve their physical propor-tions, achieve a more feminine figure, and enhance their self-image and confidence. Candidates for augmenta-tion mammaplasty come from many walks of life and have myriad psychological profiles,1,2 but after surgery
they share similar feelings of enhanced self-image, increased self-esteem, improved sexual function, and bet-ter inbet-terpersonal skills.3
Breast augmentation is one of the most popular operations performed by plastic surgeons, and its popu-larity is a reflection of the high patient satisfaction with the procedure.4 The number of women seeking breast
augmentation in the United States continues to increase annually. According to a survey by the American Soci-ety for Aesthetic Plastic Surgery, 383,886 breast aug-mentations were performed in the United States in 2006. Breast augmentation is now the most commonly per-formed aesthetic surgical procedure in women (lipo-suction is the most common overall).5 It is estimated
that >1% of adult women in the U.S. have undergone breast augmentation.6
The literature is replete with articles on various aspects of breast augmentation. The procedure has not only generated copious academic debate about the tech-nical aspects of creating an aesthetically pleasing breast, but its safety has also sparked considerable angst in the political arena. The purpose of this review is to
•
Give the reader an overview of the history of breast augmentation surgery.•
Review and compare various methods of breast aug-mentation.•
Discuss preoperative examination, patient counsel-ing, and surgical planning.•
Evaluate the advantages and disadvantages of vari-ous implant types, incision locations, and pocket locations.•
Analyze the literature regarding outcomes of sur-gery, with an emphasis on complications such as cap-sular contracture, implant rupture, and revisional surgery.•
Review the controversy over silicone gel implants, the U.S. Food and Drug Administration (FDA) deci-sions, and the most current data on safety profiles, outcomes and health-related concerns.Plastic surgeons performing breast augmentation must thoroughly understand all the elements above in order to provide appropriate care to their patients.
HISTORY
The first reported augmentation mammaplasty dates back to 1895, when Czerny7 transplanted a lipoma to
the breast to replace tissue that was removed in resecting an adenoma. Berson8 attempted fat grafting to the breast
in the early 1940s but noticed 30–50% graft resorption
Rohit K Khosla MD
postoperatively, and subsequently proposed dermis-fat and dermis-fascia-dermis-fat grafts to minimize dermis-fat resorp-tion of grafts. In the 1950s Longacre9,10 described
pedicled dermis-fat flaps based at the inframammary fold to augment the breast. In those days petroleum gel, beeswax, shellac, and epoxy resin were all injected into the breast as soft-tissue fillers,11 and Uchida12
reported the use of injectable silicone in 1961.
These early methods had universally unsatisfac-tory results that led to the development of alloplastic materials. Sponges made from polyurethane, teflon, and polyvinyl alcohol were used as solid-material implants in the 1950s and 1960s,11 but resulted in firmly
contracted, immobile breasts without aesthetic appeal.13,14
The search for a softer implant material led to the manufacture of dimethylsiloxane (silicone) sponges. Silicone is inert and has unique properties that allow it to be produced as a spray, gel, or solid.15,16 Silicone
has been a component in hairspray, infant formula, beer, antacids, medical grade tubing, and lubricants because of its versatile properties. In 1962 Cronin and Gerow17 introduced the sealed silicone gel breast
implant that ushered in the modern era of prosthetic breast augmentation.
The inflatable saline-filled implant was first reported by Arion18 in 1965. It was billed as an
alter-native implant that could be introduced through smaller incisions than the silicone-gel prosthesis. Saline-filled implants were subsequently developed by American manufactures and marketed for clinical use in the 1970s.19,20
Rising concerns in the 1980s about the potential of silicone-gel implants as a cause of autoimmune disor-ders,21–23 fueled by media speculation and legal actions
against manufacturers, culminated in the FDA’s issu-ing a voluntary moratorium on their use in 1992, and silicone-gel implants were removed from the U.S. mar-ket soon after. Canada’s regulatory agency followed suit and silicone implants disappeared from the Canadian market as well.
During the time they were banned in North America, silicone-gel implants remained available in most other countries and were used extensively across the globe. Breast augmentation was still highly sought after in the U.S. despite health concerns. Saline
implants filled the void left by the absence of silicone implants but were plagued by high deflation rates and uncertain durability. The FDA eventually reapproved silicone-gel breast implants and allowed them back on the market in November 2006. Details of the FDA ban, epidemiologic studies, and the prospective indus-try studies designed to investigate the safety of sili-cone implants are reviewed below.
PREOPERATIVE EVALUATION Morphometric Analysis
Breast and chest wall asymmetries are inherent in humans and common in almost all women. While this is a recurring theme in the breast augmentation literature, ironically there is a distinct lack of data regarding anterior chest wall and breast asymmetries noted in women seeking breast augmentation. The spectrum of asymmetries in this patient population range from the subtle, almost unrecognizable differ-ence, to the severe deformity, Poland syndrome. There may be discrepancies in the size and position of the nipple-areola complex, volume of the breast mound, base width, or position of the inframammary fold (IMF). Chest wall deformities typically involve the manubrium (eg, pectus excavatum, pectus carinatum, or a prominent costosternal junction).24 There may be
rib torsion, rib rotation, sunken chest wall, flaring lower costal cartilages, or hypoplasia of the pectoralis major muscle.24
Recent studies attempted to apply more objective parameters to breast augmentation. In an extension of Penn’s analysis of breast morphology,25 Westreich26
measured 22 parameters in 50 women who had what he considered to be “aesthetically perfect breasts,” and concluded that the sternal notch-to-nipple and nipple-to-nipple distances determined the proper volume for breast augmentation. These studies suffer from the inherent bias of the authors’ selection criteria, which were purely subjective. The notion of a “perfect breast” is a misconception that does not exist in nature, nor can it be achieved surgically.
Brown and colleagues27 studied the breast
mor-phometry of 60 women in an attempt to establish a control group to define the “average breast” rather than the “perfect breast”. The women were all
con-tent with the shape of their breasts, had not had any previous breast surgery and did not desire alteration to their breasts. The authors noted sev-eral key landmarks on the breast; horizontal mea-surements were taken from the midline and vertical measurements were taken from the sternal notch on the midline axis. They found a high degree of bilat-eral asymmetry in all measurements (Table 1), though the only statistically significant difference between mean right and left breast measurements was in most inferior horizontal level of the IMF (55%). Breast projection and areolar diameter were asym-metric in 27% and 28%, respectively. These data confirm the natural asymmetry that occurs in an average population of women.
TABLE 1
Frequency of Breast Asymmetry in a General Population (N=60)
(From Brown TP, La H, Ringrose C, et al: A method of assessing female breast morphometry and its clinical application. Br J Plast Surg 52:355, 1999.)
Rohrich and coworkers28 looked at the incidence
of breast and chest wall asymmetries in a breast augmentation population. This was a retrospective review of 100 randomly selected women who underwent primary breast augmentation at their institution. Preoperative photographs were criti-cally evaluated by 4 independent surgeons to assess breast and chest wall characteristics. The anatomic parameters analyzed were nipple position, size of the nipple-areola complex, chest wall asymmetries, breast volume, base constriction, and IMF position. The results of the analysis are shown in Table 2.
Overall, 88% of women had at least one parameter of asymmetry and 63% had two or more, including asymmetrical position (53%) and size (24%) of the NAC; breast volume (44%); base constriction (29%); IMF position (30%); and chest wall deformity (9%). Their observations confirm the inherent differences among various anatomic components of a woman’s breast.28
These original studies are distinct in design and objective. Brown27 prospectively established a
con-trol group to serve as a reference range of “normal-ity” that may aid in the planning of reconstructive and aesthetic breast surgery. Their control group consisted of a wide age range of patients with a mean age of 38 years (range 15–88y). They made direct patient measurements and went on to compare breast morphometry in a small group of breast reduction and breast augmentation patients rela-tive to the control group. In contrast, Rohrich’s28
study design was that of a retrospective review. The authors’ goal was to evaluate the extent of pre-existing breast asymmetry in an average patient population seeking breast augmentation, age unspecified. The analysis was conducted from patient photographs rather than direct measure-ments, and there were no comparison groups. Yet despite the differences in study objectives and meth-odology (Table 3), both authors arrive at similar con-clusions regarding female breast morphometry: that is, asymmetry is highly common with regard to any given feature of the breast and chest wall.
TABLE 2
Asymmetry after Breast Augmentation
(Reprinted with permission from Rohrich RJ, Hartley W, Brown S: Incidence of breast and chest wall asymmetry in breast augmenta-tion: A retrospective analysis of 100 patients. Plast Reconstr Surg 111:1512, 2003.)
Clinical Examination
The preoperative clinical examination is of paramount importance to the success of the procedure. The chest wall must be critically evaluated for deformities and ir-regularities of the rib cage as well as hypoplasia of the pectoralis major. The physical characteristics of the breast tissue, base width, and nipple-areola size and position must be documented. The degree of breast ptosis should also be evaluated. Patients with grade II ptosis or greater may benefit from concomitant mastopexy.
Every plastic surgeon must develop an individual-ized and comprehensive approach to evaluate patients for breast and chest wall asymmetries. The physical exam findings must be candidly discussed with the pa-tient in preoperative counseling. Tebbetts29 advocates a
staged, repetitive patient education and informed con-sent process. All asymmetries must be discussed as part of the informed consent process. Breast augmentation patients must be aware that subtle differences in their breasts before surgery may become exaggerated after surgery. This must be emphasized in the informed con-sent. If our patients understand the prevalence of their anatomic variances, they will have realistic expectations for the outcome of surgery, which lessens postoperative complaints and leads to higher levels of patient satisfac-tion after breast augmentasatisfac-tion.
Women who seek surgical enhancement of their breasts place a considerable emphasis on physical
appearance. A surgeon must delve into a patient’s motives and try to identify patients who have unrealis-tic goals and expectations from surgery. The patient’s desires must be balanced against the reasonable likeli-hood of achieving those results. A high level of patient satisfaction can be ensured if the patient’s aesthetic goals are attainable given the surgeon’s skill and experience.
OPERATIVE PLANNING
As Hidalgo notes, the surgical plan involves three key variables: implant type; incision location; and pocket plane.30 Implant-related variables include size, shape,
shell texture, filler substance, and final implant volume. There is no incontrovertible evidence to support one choice over another.
Implant Selection
Bra and cup sizes are highly variable from one manufac-turer to the next.32 Patient perceptions of their own cup
size are also inaccurate.32,33 Regnault19 found that a 100mL
increase in volume translates roughly into one cup size increase.
Various methods have been proposed to predict the appropriate size of an implant for augmentation. The preoperative decision-making process is as important as any aspect of surgical technique. The resulting form of the augmented breast will be determined by the
TABLE 3
Differences in Two Studies of Breast Asymmetry
(Data from Brown TP, La H, Ringrose C, et al: A method of assessing female breast morphometry and its clinical application. Br J Plast Surg 52:355, 1999; and Rohrich RJ, Hartley W, Brown S: Incidence of breast and chest wall asymmetry in breast augmentation: A retrospective analysis of 100 patients. Plast Reconstr Surg 111:1512, 2003.)
dynamic interaction over time between the soft-tissue envelope, quality of the breast parenchyma, and dimen-sions of the breast prosthesis.33 Large implants (>350mL)
induce adverse changes on the native breast tissue;34 this
soft-tissue atrophy is progressive and must be consid-ered preoperatively.35 A breast implant will also cause
costal cartilage remodeling leading to a concave chest wall beneath the prosthesis.35
Tebbetts and Adams33 advocate a biodemensional
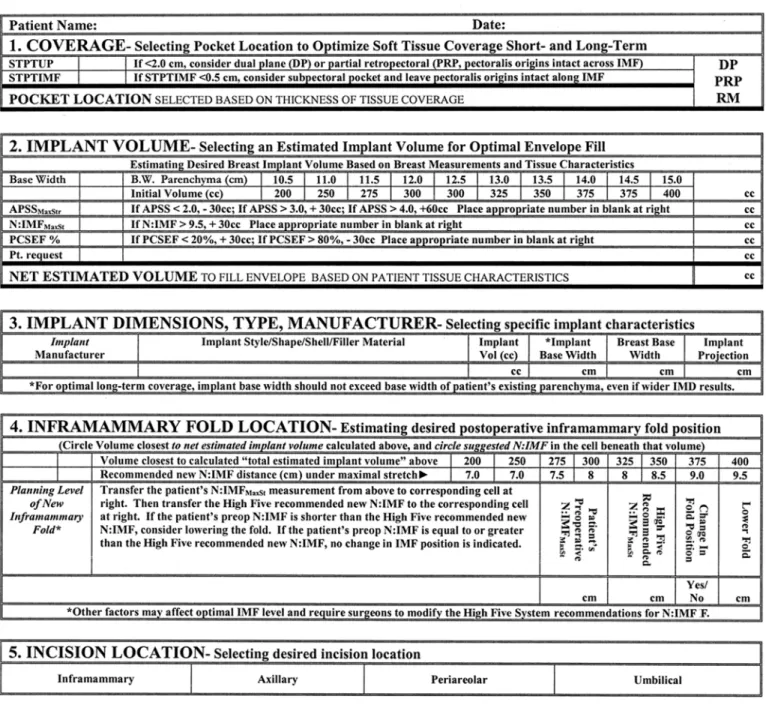
assessment they refer to as “the high five process.” This is a quantifiable approach to tissue assessment that uses defined measurements for making decisions. It consists of five key elements to consider when planning a breast augmentation, as follows:33
1. Optimal soft-tissue coverage/pocket location for the implant.
Determines risk of visible traction rippling, visible palpable implant edges, and possible excessive stretch or extrusion.
2. Implant volume (weight). Determines the effects of the implant on tissue over time, risks of excessive stretch, excessive thinning, palpability, visible traction rip-pling, ptosis, and parenchymal atrophy.
3. Implant type, size, and dimensions. Determines control over distribution of fill within the breast; adequacy of envelope fill; and risks of excessive stretch, thin-ning, palpability, rippling, ptosis, and parenchymal atrophy.
4. Optimal location of the inframmamary fold based on the width of the implant selected. Determines the posi-tion of the breast on the chest wall, the critical aes-thetic relationship between breast width and nipple-to-fold distance, and distribution of fill.
5. Incision location. Determines the degree of trauma to the adjacent soft tissues, exposure of implant to endogenous bacteria in the breast tissue, surgeon vis-ibility and control, potential injury to adjacent neuro-vasculature, and potential postoperative morbidity. The measurements are taken with the patient seated and back straight (Figs 1–6). On the basis of these measure-ments the surgeon makes the five key choices and these decisions are discussed with the patient at the time. Using the “high five” method of surgical planning and implant selection, Tebbetts and Adams33 report a
reoperation rate of 2.8–3% in nearly 2000 patients
fol-lowed for 6+ years. This compares very favorably with manufacturers’ premarket approval studies of saline implants submitted in 2000, in which the average reoperation rates were 17% for size exchange and 8.7% for adjustments.36,37
Incision Location
Various locations have been proposed to minimize or hide the incisional scar of surgical breast augmentation. The current choices include periareolar, inframammary, transaxillary, and periumbilical incisions. Surgeons should be skilled in various techniques to accommodate a patient’s anatomy or wishes for a specific approach.
The ideal location for the incision offers ample control of the surgical field and least trauma to normal tissue.34
These criteria must be combined with the desires of an informed patient who is aware of the risks and benefits of each incision.
Spear and associates38 present an algorithm for
locat-ing the incision in breast augmentation surgery (Fig 7) that takes into account nipple size, fold position, and need for concurrent procedures.
Hidalgo30 reviews his experience with breast
augmen-tation and discusses how to choose the optimal incision (Table 4).
Periareaolar
Some surgeons believe that the periareolar approach is the most versatile.30,38 The scar is generally camouflaged
well along the areolar border. A periareolar incision gives central access to all quadrants of the breast for subglandular and submuscular dissection; it proves use-ful when the inframammary fold needs to be lowered a considerable distance; and is the logical approach when a concurrent mastopexy needs to be performed. A periareolar incision is also indicated for patients with tuberous breasts in whom parenchymal alterations— eg, scoring of the lower poles or parenchymal excision— are necessary.30,38 The incision is also useful in secondary
procedures that require a capsulectomy, implant exchange, or capsulorrhaphy to correct implant mal-position.
The periareolar incision is contraindicated in patients whose areolar diameter is <3cm or who have lightly
pig-Fig 1. High five tissue analysis and operative planning form. (Reprinted with permission from Tebbetts JB, Adams WP: Five critical decisions in breast augmentation using five measurements in 5 minutes: the high five decision support process. Plast Reconstr Surg 116:2005, 2005.)
Figs 2-6. Breast measurements. (Reprinted with permission from Tebbetts JB, Adams WP: Five critical decisions in breast augmentation using five measurements in 5 minutes: the high five decision support process. Plast Reconstr Surg 116:2005, 2005.)
mented areolae with indistinct margins. It also transects the lactiferous ducts, which can increase the risk of bac-terial contamination of the pocket. It may potentially interfere with nipple sensation, as superficial nerves are undoubtedly severed. Despite a usually well-concealed scar, this incision does place a potentially visible scar on top of the breast mound.
Inframammary
The inframammary incision is currently the most com-mon approach to breast augmentation, as well as the simplest and most straightforward.38 It is suited to
patients who have significant breast volume preopera-tively, slight glandular ptosis, or postpartum atrophy.30
These patients’ nipple-to-IMF distance is usually long enough to prevent IMF displacement after surgery. The incision also allows direct access to the subglandular and submuscular dissection planes; the subpectoral plane is entered without disruption of the breast paren-chyma. The length of the incision varies to accommo-date implants of all sizes. The scar is hidden in the well-developed IMF and usually visible only with the patient lying down.
Depending on the implant and tissue characteristics, the IMF may need to be lowered.33,38 Tebbetts33 and
Spear38 describe techniques to estimate the new incision
location below the original IMF. It is important to keep the incision off the lower pole of the breast and hidden in the new crease.
The inframammary approach is not indicated when the IMF is high or nonexistent, in the constricted breast, or in the tubular breast deformity.28 Some surgeons
believe that the IMF incision is less versatile in second-ary cases requiring capsulectomy or capsulorraphy of the superior pole. This approach may be associated with a high risk of wound dehiscence or scar widening as the weight of the implant is forced onto the incision by gravity.
Transaxillary
The transaxillary incision is appealing because it avoids a scar on the breast, is well-concealed under the arm, and offers direct access to the subpectoral plane. The short, transverse incision in the axilla does not violate the breast parenchyma. The transaxillary incision is said to be
indi-Fig 7. Breast augmentation algorithm. (Modified from Spear SL, Bulan EJ, Venturi ML: Breast Augmentation. Plast Reconstr Surg
cated in very thin patients, those with small parenchy-mal volume, high breast position on the chest, sparenchy-mall areolae, ill-defined IMF, or minimal breast ptosis.30,38
The technique was originally described as a blunt dissection in the subglandular plane,39 but this was not
practical30 and most surgeons today use the incision to
access the subpectoral space. The blunt dissection is not ideal because it is blind and gives rise to concerns over insecure hemostasis, inadequate pocket dissection, and malposition of the implant.40 Since the advent of
endoscopic techniques, sharp dissection under direct visualization with accurate hemostasis and precise muscle release are all possible.38,41 Howard42 notes the
incidence of implant malposition decreased from 8.6% to 2% with the use of endoscopy.
Tebbetts43 reviewed his 28-year personal experience
with transaxillary augmentations using both blunt (331) and endoscopic (359) techniques. He details the relevant anatomy and key surgical steps in a successful endo-scopic transaxillary breast augmentation. The Baker III/ IV capsular contracture rate was 4.2% vs 1.3% for blunt and endoscopic dissection, respectively. Problems with
the inframmamary fold or contour irregularities were seen in 3.6% of the blunt dissection group compared with 1.1% of the endoscopic group. Transient lymphaden-opathy or lymphatic banding was observed in 10.3% of the blunt group vs 2.2% of the endoscopic group. Implant malposition was seen in 1.8% of the blunt dissection group and 0.2% of the endoscopic group.
The transaxillary approach is not indicated in cases where parenchymal manipulation is expected, such as tuberous breasts or ptotic breasts,30,38,43 or when using
“anatomic” implants or large silicone gel implants because of potential damage to the prosthesis during insertion.38 Secondary procedures are essentially
impossible via the transaxillary approach.30,38
Transumbilical
The transumbilical breast augmentation (TUBA) is another endoscopic approach that keeps the incision off the breast and places it in the umbilicus. A subcutane-ous tunnel is carved above the rectus fascia, the dissec-tion is carried superiorly to the subglandular space, and
TABLE 4 Incision Options
(Reprinted with permission from Hidalgo DA. Breast augmentation: choosing the optimal incision, implant, and pocket plane. PlastReconstr Surg 105:2202, 2000.)
an implant pocket is fashioned hydraulically with the use of expanders.
The potential for implant malposition and trauma increases with remote-access augmentation, especially with textured and anatomic implants.38 The
trans-umbilical approach is not approved by the FDA for sili-cone gel implants.
Pound and Pound44 review the outcomes of 1400
TUBA procedures involving both subglandular and submuscular implant placement. The incidence of deflation was reported as 1.1%. The contracture rate was 4.2% Baker II and <1% Baker III/IV. The incidence of hematoma was <1%.
Brennan and Haiavy45 review a single surgeon’s
experience with TUBA in 245 patients followed for 1 year. The authors note more postoperative firmness with subglandular implants relative to subpectoral implants, and this was a negative predictor of patient satisfaction in the study group. The rate of hematoma was 0.4%; umbilical wound infection, 3.2%; implant deflation, 1.2%; tunnel seroma rate, 2%; asymmetry, 4.1%; and capsular contracture, 3.7%.
TUBA is contraindicated in very thin women and in patients who have truncal obesity, <2cm pinch test on the breast, previous abdominal surgery or hernia, and for secondary breast augmentation.38,46 Many surgeons
also dislike this approach because of poor access to the implant pocket, inability to create a subpectoral pocket, and need for a second incision if revision or replacement is required.30
Pocket location
The terminology to describe the location of the implant pocket in breast augmentation surgery can be confus-ing. Most surgeons refer to implants placed either in the subglandular space or in the submuscular space. Submuscular implantation can be partial retropectoral or total submuscular (complete muscle coverage with pectoralis major and serratus anterior).47 Tebbetts47
introduced the concept of dual-plane breast augmenta-tion, which combines subglandular and partial retro-pectoral pocket location. He believes this implant posi-tion maximizes the benefits of each pocket locaposi-tion and limits the risks of a single pocket location.47 The author
clarifies the nomenclature and details potential benefits and tradeoffs of each pocket location (Table 5).
A partial retropectoral or total submuscular pocket provides the necessary soft-tissue coverage superiorly in a glandular, ptotic breast with a thin superior pole,47
but risks a “double bubble” deformity as the parenchyma slides inferiorly off the pectoralis and implant. A con-stricted lower pole in a thin patient needs additional coverage superiorly while muscle cover inferiorly restricts expansion of the lower pole.47
Subglandular
Early augmentation procedures involved limited blunt dissection in the subglandular plane that created pock-ets slightly larger than the implant.48–50 It was then
real-ized that the forces of wound contraction further reduce the size of the implant pocket and emphasis shifted to developing a generous pocket.
Some believe that subglandular implants restore breast shape more effectively and correct ptosis better than submuscular implants.30 However, there must be
adequate soft-tissue coverage when considering a subglandular implant. Tebbetts recommends a subpec-toral pocket for patients with a skin pinch test <2cm.33,47
Subpectoral
Dempsey and Latham51 described the first breast
aug-mentation with implantation in the subpectoral plane. The subpectoral plane has many advantages, as follows:
•
a lower incidence of capsular contracture47•
implant edges are blunted by the muscle, producing a better breast contour•
less exposure of the prosthesis to bacterial contami-nation from contact with glandular tissue52•
dissection in a less vascular plane and lower rates of hematoma•
maximal preservation of nipple sensationRegnault53 observed that subpectoral implants tend
to shift superiorly and laterally when the muscle ori-gins are not released to the level of the sternum. Scully54
believes that an intact pectoralis origin is the reason for lower capsular contracture rates due to the repeated
TABLE 5
Alternative Pocket Locations: Tradeoffs and Benefits
(Modified from Tebbetts JB: Dual plane breast augmentation: optimizing implant-soft-tissue relationships in a wide range of breast types. Plast Reconstr Surg 107:1255, 2001.
compressive forces generated by pectoralis contraction. Biggs and Yarish55 reported a capsular contracture rate
of 32% with subglandular implants vs 12% in the sub-pectoral group.
Dual-plane
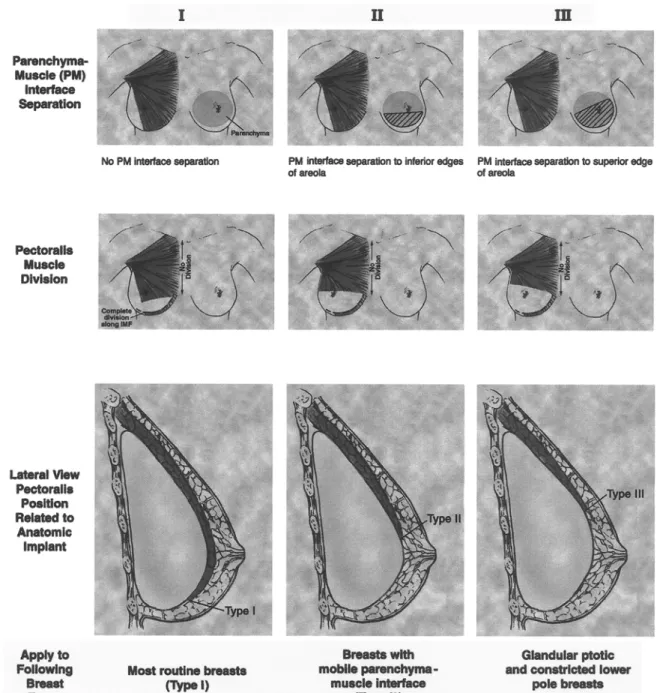
Tebbetts47 introduced the principle of dual-plane breast
augmentation to alter the parenchyma–muscle interface
in an attempt to counteract the double bubble phenom-enon. It is important to preserve intact the muscle ori-gins of the pectoralis major along the sternum to avoid medial visibility of the implant, synmastia, and rippling of the overlying skin.47,56 Illustrations of the various
dual-plane methods are shown in Figure 8. The potential ben-efits of the dual-plane technique over traditional subglandular and partial subpectoral augmentations are listed in Table 5 above.
Fig 8. Extent of dissection at the parenchyma-muscle interface (above), the position of the inferior edge of divided pectoralis origins
(center), and pectoralis position relative to the implant (below) for types I, II, and III dual plane augmentation techniques. (Reprinted with permission from Tebbetts JB: Dual plane breast augmentation: optimizing implant-soft-tissue relationships in a wide range of breast types. Plast Reconstr Surg 107:1255, 2001.)
Capsular Contracture
The etiology of capsular contracture remains unclear. Both hypertrophic scar and infectious hypotheses have been proposed to explain the formation of a hard cap-sule around the implant in breast augmentation.
Hypertrophic Scar Hypothesis
Although hematomas left in place without drainage have been incriminated in the development of hard capsules in an animal model,57 microscopic analyses of hard
periprosthetic capsules fail to substantiate a hyper-trophic scar etiology.58–60 Hypertrophic scarring may
have hematoma, granuloma, or genetic causes. The occurrence of unilateral capsular contracture after bilateral augmentation negates a humoral mechanism. The histology of the fibrous capsule around smooth-walled silicone implants is well documented.58,59,61–63 The
membrane consists of a thin inner layer of fibrocytes and histiocytes surrounded by a thick layer of relatively acellular collagen fiber bundles. The outermost layer is composed of loose connective tissue. The middle layer is made up of densely packed collagen bundles lying par-allel to each other. Synovial metaplasia may be present in as many as 50% of implant capsules.64–66 Secretory
cells contribute proteoglycans and other friction-reducing moieties to the implant lumen.65
Myofibroblasts are known to be present on the cap-sules around breast implants.63,67 These contractile cells
are believed to contribute to capsular contracture as part of a foreign body reaction61,68 initiated by silicone that is
either shed by the implant shell69–72 or filtered through
the walls of an implant.73–77
Prantl and colleagues77 attempted to correlate the
histologic features of capsules with the clinical classi-fication of contracture.78 Samples of capsular tissue
obtained from 24 patients with various degrees of con-tracture were analyzed for thickness and cellular com-ponents. There was a positive correlation between capsular thickness and Baker score. Greater capsular thickness was also associated with a higher number of silicone particles and silicone-loaded macrophages in the capsule. Despite this and many other studies of the capsular contracture phenomenon, a definitive correlation between the presence of silicone in the
sule, number of fibroblasts, and hardness of the cap-sule has not been established.62,67,76–77,79–82
Confounding this hypothesis is delayed capsular con-tracture developing years after implantation. High lev-els of peptide growth factors have been identified in advanced contractures83 that may signify a chronic,
low-grade, foreign body reaction around gel implants pro-longing the healing process.
Calcification has also been observed in as many as 16% of capsules during explantation84 and relates to
lon-gevity of implantation: Implants in place for 23–26 years had a 100% incidence of capsular calcification; implants in place for 11–20 years had a 26% incidence of capsular calcification; and implants in place for <10 years had a 0% incidence of calcification. The significance of this find-ing is not known.
Capsular contracture rates are lower with saline implants, low-bleed silicone implants, textured implants, submuscular placement, and primary aug-mentation versus revision or reconstruction.72 Factors
associated with elevated risk of capsular contracture are years of implantation, small surgical pocket, and thickness of the implant shell.47
Infectious Hypothesis
Subclinical infections have been incriminated in the development of capsular contracture.86–91 Studies in
ani-mal models show increased implant hardness and accelerated capsule formation when implants were con-taminated with Staphylococcus epidermidis or Staphylococ-cus aureus,89,90 supporting an immunologic reaction in
con-tracted capsules.
Burkhardt et al85 cultured pathogens in 30 of 42 (71%)
breast capsules during open capsulotomy for contrac-ture. The dominant organism was S. epidermidis, which is also routinely cultured from nipple secretions.86–88
Dobke et al92 report 81 positive cultures in 150
explanted silicone implants—a 54% rate overall. When the capsules were contracted the incidence of positive cultures was 76%, vs 28% when they were not clinically contracted. S. epidermidis was the predominant organism (in 84%).
Virden and coworkers93 believe that subclinical
infec-tion around silicone breast implants is more common than the results of standard laboratory cultures may
suggest. They noticed a slime layer referred to as a “glycocalyx biofilm” on the surface of explanted pros-theses. This biofilm is made of extracellular polysaccha-rides and glycoproteins produced by bacteria. The authors theorize that the bacteria hide within this biofilm and go undetected by routine culture methods. Using special culture media, they found 56% of con-tracted implants and 18% of nonconcon-tracted implants were positive for S. epidermidis. In contrast, routine cul-tures of the entire series were positive in only 5%.
Classification
Baker78 introduced a clinical classification scheme for
grading the severity of capsular contracture that is based on symptoms and physical examination (Table 6).
TABLE 6
Baker Classification of Capsular Firmness in Augmented Breasts
(Reprinted with permission from Little G, Baker JLJr: Results of closed compression capsulotomy for treatment of contracted breast implant capsules. Plast Reconstr Surg 65:30, 1980.)
Preventing Contracture
Several modalities have been proposed to prevent cap-sular contracture. These range from antibiotics in the implant or in the pocket, to systemic medications, to various implant massage techniques.
Antibiotics
Dubin instilled bacitracin foam in the pocket of more than 2000 breast augmentations and reported firm breasts in fewer than 3% postoperatively.94 Burkhardt
et al85 initially recommended adding 1 to 2mg of Keflin
(or gentamicin in cases of penicillin allergy) to saline implants to promote slow diffusion of antibiotic through the shell and into the pocket. The authors subsequently reviewed the postoperative course of 124 women with subglandular saline implants to determine the effects of pocket irrigation with antibiotics.91 Various antibiotics
were injected in and around the prostheses and patients were followed for 24 months. Early (<3mo) contracture was reduced from 29% in the control group to 4.25% in the treatment group. Although the protective effect of antibiotics dissipated after 3 months, the final contrac-ture rate was still lower in the experimental group: 19% vs 41% in controls at 24 months.
In a later study, Burkhardt and Eades95 report 12% Baker
III/IV contractures when the implant pockets were irri-gated with Betadine and 28% when irriirri-gated with saline. They conclude that pocket irrigation with 5% povidone-iodine (50% Betadine) was as effective as other antimicro-bial agents in controlling bacterial invasion around the prosthesis. They found no correlation between capsular contracture and hematoma formation, intercurrent infection, breast injury, or displacement exercises.91
Adams and colleagues96 compared the in-vitro
effi-cacy of various agents in retarding bacterial growth on implants. Dilutions of povidone-iodine and combina-tions of double antibiotic solucombina-tions were tested. The authors conclude that a combination of 10% povidone-iodine, gentamicin 80mg and cefazolin 1gm was most effective in controlling common pathogens associated with infection around breast implants.
In 2000 the FDA issued a caution alert regarding Betadine in contact with any breast implant due to potential weakening of the shell.97,98 On the basis of
unpublished data submitted by the Mentor Corpora-tion (Santa Barbara, CA) showing delaminaCorpora-tion of the adhesive on the valve patch of saline implants,99 which
the manufacturer believed was caused by Betadine, the FDA recommended discontinuing pocket irrigation with Betadine. A review of the data shows that 75% of the observed deflations were reported by a single surgeon who used intraluminal injection of Betadine, not pocket irrigation.99 No other series to date confirm a
relation-ship between Betadine and implant deflation.99
Adams and associates100 looked for an alternative
antibiotic regimen for breast augmentation after the Betadine ban and found the following combination was most effective in reducing bacterial concentrations:
50,000 units of Bacitracin 1gm Ancef
80mg gentamicin 500mL saline
Shah and coworkers101 studied the effect of
cepha-losporins added to the outer lumen of inflatable pros-theses implanted in pockets contaminated with S. epidermidis. They conclude that intraluminal antibiotics are of value in decreasing capsular contracture, particu-larly at low levels (<103) of bacterial contamination of
the implant pocket.
In 2007 Wiener99 analyzed implant deflation and
cap-sular contracture rates in 1244 women operated on between 1998 and 2005 who received pocket irrigation with Betadine at various dosages and saline implants. The observed deflation rate was 0.24% and the rate of capsular contracture grade Baker II or greater ranged from 0.5–2.2% in the four groups reviewed. These data suggest that proper use of Betadine irrigation has no effect on the rate of deflation of saline implants and may contribute to a low risk of capsular contracture.
Corticosteroids
Two studies in the 1970s looked at the effect of pocket irrigation with Kenalog102,103 and demonstrated
favor-able results in terms of maintaining capsular softness. Subsequently there were reports of thinning of skin flaps, subcutaneous tissue erosion, and implant exposure associated with steroid administration.104 The steroid
apparently pools in the lower pole of the pocket and can predispose to skin erosion and implant extrusion.105
Intraluminal methylprednisolone was reported to dif-fuse through the shell of implants over 60 days,105 though
clinically only 5/100 patients developed capsular con-tracture. Intraluminal doses of methylprednisolone
≤20mg may be beneficial and have few complica-tions;106,107 higher doses are associated with
complica-tion rates of 60-80%.106,107
The diffusion rate of methylprednisolone through the elastomer envelope of a breast implant is concentration-dependent rather than dose-related.108 As expected,
dif-fusion across the implant shell is slower for double-lumen implants and levels off after 10 months for all types of inflatable implants.108 In a study by Morykwas and
col-leagues,109 the diffusion half-life of methylprednisolone
was 20 months and the authors believe that steroids are released from breast prosthesis for a longer time than previously thought. This might explain some of the long-term detrimental effects of steroid use.
A multicenter review of 504 women by Gutowski and others110 found that although intraluminal antibiotics
and steroids confer a protective effect against capsular contracture, they double the risk of implant deflation.
Cyclosporine A
Stark and coworkers111 tested the immunologic,
T-lym-phocyte-induced reaction hypothesis of capsule forma-tion in the rat model. They found a significant decrease in capsular thickness when intraluminal cyclosporine A was utilized. The collagen layer of the capsule in the treat-ment group was thinner and less organized than that of the control group. The mechanism of action of cyclo-sporine A is believed to be inhibition of the release of interleukin-1, which is a fibroblast proliferation factor that can be responsible for excessive collagen deposition. Cyclosporine A has not been tested in clinical trials.
Vitamin E
Peters et al112 studied the effects of vitamin E on implant
capsules in the rat model and noted delayed develop-ment of a periprosthetic capsule. It was suggested that patients ingest vitamin E after augmentation mamma-plasty to capitalize on its known anti-inflammatory properties and reduce the rate of capsular hardness. Baker113 recommends a regimen of 1000 units of vitamin
E orally twice a day, beginning 1 week prior to surgery and for 2 years postoperatively. It is unclear whether the positive results in his series were due to vitamin E or to other factors. Despite much study, there is no defini-tive evidence that vitamin E prevents or ameliorates cap-sular contracture.114
Cyclooxygenase-2 (COX-2) Inhibitors
COX-2 is expressed primarily in response to inflam-matory stimuli and mediates the production of pros-taglandins that support the inflammatory process.115
The COX-2 enzyme has been detected in the capsules of silicone implants in animal models,115 and researchers
hypothesize that COX-2 inhibitors may be of benefit in preventing capsular contracture. Many surgeons have prescribed COX-2 inhibitors in an attempt to minimize contracture and anecdotally mention a benefit; how-ever, there are no published data to date on the effects of COX-2 inhibitors after breast augmentation in humans.116
Implant Massage
Implant massage was independently described in the 1970s by Vinnik117 and Hoehler39 to preserve the dissected
volume of the implant pocket. They describe forcibly moving the implant within the pocket in a series of “ex-pansion exercises” that are performed every few hours. This frequent movement theoretically keeps that devel-oping capsule from tightening around the implant.
The benefit of implant massage is debated. Many authors advocate its use and demonstrate a reduction in capsular contracture rate,117–119 while others120 find
no benefit with implant massage initiated at 2 weeks postoperatively. Because a capsule is histologically evident on postop day 3,62 it could be argued that
mas-sage is effective only if it begins very soon after sur-gery. The clinical evidence for pocket massage is inconclusive, as are animal studies of implant compres-sion/expansion.121,122
Multimodal
Effective management of the implant capsule probably involves a number of measures. Becker and Springer123
describe a multimodal approach to the breast implant capsule which over 15 years led to a decrease in contrac-ture rate in their series from 20% to 2%. The specific management components that brought about the improved outcome could not be identified.
Management of Capsular Contracture Closed Capsulotomy
The goal of closed capsulotomy is to hydraulically tear the scar of the capsule without rupturing the implant.118,124
This is accomplished by manually compressing the breast until there is an audible “crack” signifying capsular frac-ture. One report shows successful return to Baker I level
after closed capsulotomy in most patients,125 whereas
oth-ers describe recurrence of firmness in 31-80% after closed capsulotomy.78,120,126 Planas and colleagues127 advocate
the use of external ultrasound to prevent recurrence of contracture after closed capsulotomy and report a suc-cess rate of 82% in cases treated 12 months after capsulotomy.
Closed capsulotomy is associated with complications such as hematoma, implant rupture, gel migration, dumbbell deformity, and incomplete rupture of the cap-sule.128,129 A combined report of 750 plastic surgeons
dem-onstrate an overall complication rate of 10% after closed manipulation of implants in the treatment of contrac-ture.129,130 Extracapsular rupture seems to be associated
with a history of closed capsulotomy;130 more than 50%
of women found to have ruptured implants during explantation have had closed capsulotomy.129 This
observation is not surprising given that the manual force (lbs/sq inch) applied during closed capsulotomy almost always exceeds the breaking strength of most implants.131
In 1999 the Institute of Medicine of The National Acad-emies of Science released its final report after 2 years of investigation of silicone implants.132 The committee does
not recommend closed capsulotomy for the treatment of capsular contracture.
Open Capsulotomy/Capsulectomy
A capsule can be surgically scored in several places, par-tially stripped or totally excised.102,133,134 The overall
results of open capsulotomy and implant replacement using primarily gel-filled smooth-surfaced implants are disappointing, with recurrence of contracture in 37-89% of patients.85,120,125
The indications for capsulectomy are ill-defined and not universally accepted. Young’s135 recommendations
for post-augmentation prosthesis explantation and capsulectomy (Tables 7 and 8) are one surgeon’s per-spective and not a consensus.
Collis and Sharpe136 found a significantly lower rate
of recurrent contracture when implant exchange was combined with total capsulectomy.
Revision with Dual-plane Technique
Spear et al137 prefer to correct capsular contracture by
dual plane. The authors reviewed their 7-year experi-ence in 85 patients who had a long-standing history of capsular contracture and who were treated by this tech-nique. The original implants had been placed either subglandularly or submuscularly and were either sili-cone gel- or saline-filled. The original implants were removed, the pocket was converted to a dual-plane con-figuration, and new implants were inserted. The most frequent complication seen was implant malposition (3.5%) requiring reoperation. One year after surgery only 2% of patients were Baker class II and the rest were Baker I. These data suggest that established cap-sular contracture can be effectively treated with implant exchange and conversion to a dual-plane pocket.
Surgical Complications Hematoma
Williams102 reported a hematoma rate of 3% in more than
600 breast augmentations. Significant hematomas are associated with wound infection and capsular firmness
and should be surgically evacuated.57,86 One study
showed that 86% of patients with postoperative hemato-mas developed capsular contracture.120
Seroma
Periprosthetic seromas usually resorb within 4 or 5 days.138 A persistent seroma should be drained under
ultrasound control.139 Excessive use of electrocautery and
concentrated antibiotic irrigations intraoperatively have been linked to seroma formation.140,141
Wound Infection
Courtiss and coworkers86 reported a wound infection
rate of 2.2% in 899 breast augmentation cases. The infec-tion typically became evident at a mean 12 days postop-eratively. Treatment consisted of drainage of the implant pocket and administration of appropriate systemic antibiotics after culture; 16/29 implants were salvaged with this protocol. The most common pathogen was S. aureus.
Toxic shock syndrome following infection around a breast implant has been reported in a handful of patients.142,143 The infecting organism in these cases was
S. aureus. Other rare pathogens isolated from implant infections include Candida albicans,144 Curvularia spp,145
Aspergillus niger,146,147 mycobacteria,148–151 and Clostridium
perfringens.152
The nipple–areola complex has to be considered as a legitimate source of bacterial contamination during breast augmentation surgery because the lactiferous ducts connect directly with the skin through the nipple. Positive cultures from the NAC have been obtained in more that 90% of samples.153
Decreased Nipple Sensation
The nipple–areola complex is innervated by a lateral branch of the fourth intercostal nerve with overlapping contributions from the anterior and lateral cutaneous branches of the third through fifth intercostal nerves.154
The nerves parallel corresponding arteries of the same name. The anterior branches of these neurovascular bundles must be preserved to ensure nipple sensation; this is accomplished by displacing them laterally with blunt dissection.155 The nerve branches are more easily
TABLE 7
Guidelines for Explantation and Replacement– Capsulotomy Optional
(Annotated from Young VL: Guidelines and indications for breast implant capsulectomy. Plast Reconstr Surg 102:884, 1998.)
TABLE 8
Guidelines for Capsulectomy during Explantation
(Annotated from Young VL: Guidelines and indications for breast implant capsulectomy. Plast Reconstr Surg 102:884, 1998.)
mobilized in the subpectoral plane than in the subglan-dular plane because they become more fixed as they pass through the deep fascia into the glandular breast tissue and are therefore more likely to be injured during exten-sive electrocautery or sharp dissection of the lateral breast pocket. Early reviews show an incidence of diminished nipple sensation after breast augmentation averaging around 15%,78,154 but this has probably
decreased in more recent series.
Galactorrhea
Spontaneous lactation is a rare complication of aesthetic breast surgery156–159 thought to be due to transection or
irritation of the thoracic nerves during dissection, trig-gering impulses that travel via the dorsal nerve roots to the hypothalamus and pituitary to stimulate a rise in prolactin secretion. Prolactin elevation in the presence of falling estrogen and progesterone levels (in a men-strual cycle regulated by birth control pills) can bring about spontaneous lactation 1–2 weeks after surgery.
The galactorrhea is effectively treated with bromo-criptine to suppress prolactin secretion.160 Intercostal
nerve blocks have also been suggested to interrupt the afferent pituitary stimulation.161,162
Pain
Pain after breast augmentation is most often associated with severe capsular contracture, though another cause may be neurapraxia of the fourth intercostal nerve sec-ondary to the dissection. The discomfort usually resolves spontaneously within 6 months.
Huang163 reports 8 patients who after breast
augmen-tation complained of pain specific to the lateral breast mound and subscapular area and who exhibited an unsightly inferolateral bulge. Surgical exploration revealed the serratus anterior muscle was detached from the rib beyond the posterior axillary line in every case. All patients were relieved of their symptoms after removal of the implants or repair of the defect in the lateral wall of the submuscular pocket.
Synmastia
Synmastia after breast augmentation is the result of migration across the midline of one or both implants164
from overdissection of the pocket medially—a technical error. Synmastia is entirely avoidable with appropri-ate preoperative planning, implant selection, and surgi-cal execution.
Spear and associates164 analyzed a series of 20 patients
treated for synmastia and note 60% had excessively large (>400mL) and wide (base width ≥14cm) implants. The authors list the following risk factors for synmastia after breast augmentation: 1) excessively large implants; 2) disproportionately wide implants for the patient’s chest wall dimensions; 3) chest wall skeletal deformities (eg, thoracic hypoplasia, pectus excavatum); and 4) simulta-neous mastopexy and augmentation.
The correction of synmastia is very challenging. Some surgeons recommend maintaining the pectoral muscle fascia attachments medially during the augmentation procedure to avoid visible rippling and synmastia later.164 However, synmastia can develop even when the
fascia is intact as long as the medial sternal attachments of the muscle are aggressively released.164
Implant-related Complications Displacement
Implant displacement and asymmetry are second to cap-sular contracture as a source of patient dissatisfaction after breast augmentation.165 Inferior displacement
below the desired inframammary fold has been associ-ated with irrigation of the pocket with steroids.166–168
Taping the breast in the desired position is often help-ful provided the malposition is recognized early in the postoperative period. Some surgeons recommend tap-ing for 6 weeks to prevent superior migration of submuscular implants.30 Many authors describe
revi-sion and capsulorrhaphy techniques to correct persis-tently low implants.166–169 Implant displacement is
reported in 4% of closed capsulotomies but is rare after open procedures for capsule release.129
Rippling
Rippling can occur from underfilling or traction. Underfill rippling is seen in the upper pole of the breast due to folds in the implant shell.170 Traction rippling
occurs when bands of scar tissue form between the implant, capsule, and overlying dermis. It can be avoided
by ensuring adequate soft-tissue coverage, precise pocket dissection, and appropriate size of implants that are not too large for the patient’s body habitus.170 Traction
rip-pling is often associated with textured implants.
Effects on Lactation and Breast Feeding
Most women who have breast augmentation are in their reproductive years, yet the effect of the surgery on future breast-feeding ability is seldom considered. Breast milk has nutritional and immunologic proper-ties that make it superior to infant formulas.171,172
Breast-fed babies have enhanced protection against eczema, otitis media, asthma, diabetes mellitus, and iron-defi-ciency anemia.173,174 Breast-feeding also assists with the
infant’s digestion, neural development, and overall growth.174 Women who undergo breast augmentation
are unlikely to produce adequate milk to nourish an infant without supplementation175,176—lactation
insuf-ficiency.
Lactation is a complex process mediated by the hor-mones prolactin and oxytocin. In breast-feeding, the act of an infant suckling the nipple stimulates the produc-tion of prolactin, which fills the breast with milk via a process called lactogenesis, in preparation for the next feed. Oxytocin is also released, which triggers milk let-down. Nipple sensation as well as the afferent limb of the suckling reflex can be significantly altered by breast augmentation surgery, particularly when the peri-areolar approach is used.177 The periareolar approach
also leads to direct damage of glandular tissue: the severed lactiferous ducts cannot empty properly and eventually atrophy,177 further decreasing total milk
pro-duction.175 Women who have had a periareolar breast
augmentation are 5X more likely to have lactation insufficiency.175
Up to 20% of women who have had breast augmenta-tion may experience discomfort for 5 years or longer, making breast-feeding uncomfortable. Other identified risk factors for postoperative lactation difficulties are capsular contracture, hematoma, tissue atrophy, infec-tion, and multiple revisional surgeries.175
Rupture
Ruptures of both saline- and silicone gel-filled implants have been reported.
Saline Implants
In a multicenter study of 995 saline-filled implants, Gutowski et al110 found a 5.5% deflation rate overall: 2–
5% at 5 years and 5–10% at 10 years. Risk factors included underfilling by 25mL or more and intraluminal antibi-otics or steroids.
Silicone Implants
The rupture of silicone gel-filled implants is of much greater concern because of the possibility of gel migra-tion outside the breast capsule. Dowden178 describes
degrees of escape of silicone gel from a prosthesis as follows: A leak occurs when a small amount of gel passes through a small detectable hole in the shell. This results in a thin coating of gel around the external surface of the shell. A rupture occurs when there is a major tear and a significant amount of gel migrates out of the shell, but is still confined to the capsule. An extrusion is dis-placement of gel outside the capsule into adjacent tis-sue. Most surgeons refer to silicone implant ruptures as intracapsular or extracapsular based on the integrity of the capsule.179
[Editor’s Note: Silicone oil diffusing out of the semiper-meable implant envelope is called silicone bleed and is con-sidered a normal process of all silicone implants. The amount of oil bleed varies with implant age, brand, and gel characteristics.179 Some silicone implants from the
1980s contained a fluorinated silicone shell that signifi-cantly decreased the amount of gel bleed.]
The true prevalence of implant rupture is unknown but seems to be mainly related to time since implanta-tion. With increasing implant age, the strength and elas-ticity of the implant shell decrease,180,181 though the
spe-cific in-vivo conditions that cause the weakening remain a mystery. Some surgeons believe that lipid infiltration of the implant shell is responsible,182 while others
hypothesize that swelling of the elastomer shell by sili-cone fluid is the cause.183 Surgical trauma during the
insertion process may also weaken the implant shell184
Robinson and colleagues185 reviewed the records of
300 consecutive patients at the time of implant removal and noted 63.5% of implants were disrupted. They believe that most implants lose their integrity between 8 and 14 years. Cohen and coworkers186 examined 350
exchange and also noted a rupture rate of 63% among implants that had been in place for >12 years.
Other risk factors for rupture include implant type, degree of contracture, and patient’s habits. The data on implant rupture is very difficult to interpret because there are many variables involved, most notably implant characteristics and generations. The thin-walled, sec-ond-generation implants exhibit the highest rate of rup-ture.187,188 Collis and Sharpe189 reviewed data from 478
explanted prostheses190 and report a 33.7% overall
rup-ture rate: 33% for first-generation implants, 65% for sec-ond-generation implants, and 9% for third-generation implants. These data suggest that the newer generation, thicker-shelled implants resist rupture better.
Intracapsular ruptures account for 80–90% of detected implant ruptures.191,192 Although intracapsular ruptures
do not pose a danger to the patient, the FDA recommends removal of the implant.190 Extracapsular rupture and
gel migration can lead to silicone granulomas.193 In
Marotta’s meta-analysis183 the incidence of
implant-related complications that required surgical correction was 33% in the first 6 years.
Diagnosis of Rupture
Many ruptured silicone implants are silent and only dis-covered at the time of routine mammography or im-plant exchange. Magnetic resonance imaging (MRI), mammography (MMG), ultrasonography (US), and com-puted tomography (CT) have been used to detect rup-tured silicone implants; each has advantages and disad-vantages as discussed below. When choosing a diag-nostic technique for a given patient, other considerations include the cost of the test, its availability, expertise of the radiologist, and potential contraindications or patient limitations.
MRI. MRI has the highest (>90%) sensitivity and speci-ficity for detection of silicone implant rupture.191,194–196
The entire implant, and especially the tissue in close prox-imity to the chest wall that may be difficult to appreci-ate with other imaging techniques, can be visualized in multiple planes on MRI. Silicone’s unique frequency on T1 and T2 imaging makes for excellent images in diag-nosing implant rupture,197 and MRI does not use
ioniz-ing radiation.
High-resolution images are optimized with special-ized breast coils that suspend the breast and minimize breathing artifacts.197–203 The breast coil raises
sensitiv-ity in detecting implant rupture to the 95–100% range.198,201,204–206
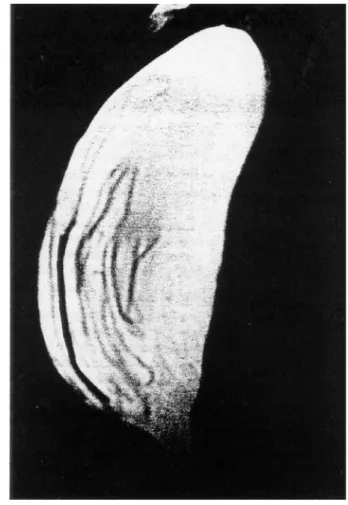
The most reliable sign of intracapsular rupture is the “linguine sign,” defined as the presence of multiple, cur-vilinear, low-signal-intensity lines within the silicone gel (Figure 9).
Fig 9. MRI of implant rupture showing linguine sign. (Reprinted
with permission from Brown SL, Silverman BG, Berg WA: Rupture of silicone-gel breast implants: causes, sequelae, and diagnosis. Lancet 350:1531, 1997.)
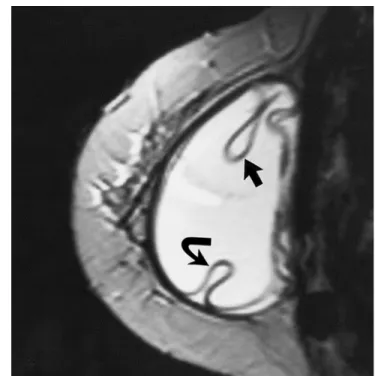
Extracapsular implant rupture is diagnosed when focal areas of high-signal-intensity representing free sili-cone are seen beyond the capsule and in the surround-ing tissue (Figure 10). The lsurround-inguine sign is also frequently seen in extracapsular rupture and is relatively more common in second-generation implants filled with a less-viscous gel.197
An uncollapsed silicone implant rupture is an intracapsular rupture and is defined as a tear of the sili-cone implant shell without collapse or with only partial collapse of the implant.197 The teardrop sign will be
present when free silicone enters a radial fold in the implant shell (Figure 11). Uncollapsed ruptures often result from focal tears that can be easily missed on gross inspection of the implant.197
Third generation and newer implants have thicker, more viscous gel and are more likely to produce the tear-drop sign when ruptured.197
MRI evaluation may not be an option because of its cost. Patients who have pacemakers, aneurysm clips, or other metallic foreign bodies and patients who are claus-trophobic are not candidates for MRI.
Mammography. Mammography is relatively inexpensive and recommended for breast cancer screening in women over 40. The implants can be examined for potential changes during the annual mammogram.
With traditional mammographic views, only a lim-ited amount of breast tissue can be visualized: 56% and
75% with subglandular and submuscular implants, respectively.207 The Eklund displacement views208—
manually pushing the implant toward the chest while selectively compressing the breast— increase the amount of breast tissue that can be evaluated, to 64% and 85% respectively.208
Mammography effectively visualizes the breast parenchyma and therefore any extracapsular silicone can be easily detected.197 Intracapsular ruptures,
how-ever, are not so easily seen. Mammographic features that are not specific to implant rupture include a mea-surable dense periprosthetic band or rim of tissue that might correlate with the implant capsule, periprosthetic calcification, asymmetry of implant size or shape, or focal herniation of the implant.197 Reports of implant rupture
from the compressive forces of the mammography tech-nique have been published for both saline-filled and sili-cone-gel implants.209
A study by Nemecek and Young210 found 62%
sensi-tivity and 82% specificity for mammograms in implant rupture after augmentation. The overall accuracy was
Fig 10. Ruptured implant after closed capsulotomy showing
collapse of the silicone shell—the linguine sign (curved arrow). (Reprinted with permission from Gorczyca DP, Gorczyca SM, Gorczyca KL. The diagnosis of silicone breast implant rupture. Plast Reconstr Surg 120:49S, 2007.)
Fig 11. Rupture of implant shell without complete collapse of
the implant shell. Teardrop signs (arrows) indicate silicone within a radial fold and outside the implant lumen itself. (Reprinted with permission from Gorczyca DP, Gorczyca SM, Gorczyca KL. The diagnosis of silicone breast implant rupture. Plast Reconstr Surg 120:49S, 2007.
73%. Ruptures were more easily detected in subglan-dular implants than in those placed beneath the muscle.
Ultrasound. Reports on the effectiveness of ultrasound in detecting implant failure range from 32–74% sensitiv-ity.198–200,211–214 Operator experience, type of equipment
used, or other technical factors may account for the spread.197 Ultrasonography also requires real-time
evaluation for best results and has a steep learning curve. Ultrasound is relatively inexpensive relative to MRI and CT, can be used in women who are claustrophic or in whom MRI is contraindicated, and does not involve ionizing radiation. Small amounts of free silicone in breast parenchyma or axillary lymph nodes may be iden-tified.196
Reliable signs of rupture seen with ultrasound include hyperechoic or hypoechoic masses, dispersion of the sonographic beam (“snowstorm sign”), or multiple par-allel echogenic lines within the implant interior (“step-ladder sign”).191,194,206,211,214–218 The stepladder sign is the
most consistent sign of implant rupture.197 The parallel
echogenic lines represent the collapsed implant mem-brane floating within the silicone gel and is analogous to the linguine sign on MRI.
Extracapsular rupture is diagnosed when there are focal nodules of free silicone in the breast parenchyma.197
In this case the snowstorm sign stems from increased echogenicity of the breast tissue and loss of normal parenchymal interfaces resulting in dispersion of the US beam. The nodules represent silicone granulomas.
Ultrasound is limited in evaluating the posterior wall of the implant and adjacent soft tissue deep to it due to attenuation of the beam by silicone.211 Reverberation
artifacts may be mistaken for echoes and give false posi-tive findings. US sensitivity decreases significantly in the presence of a contracted capsule;219 in cases of Baker
III/IV contracture, CT or MRI is preferable.
Computed Tomography. CT is an alternative diagnostic modality for claustrophobic patients or those in whom MRI is contraindicated. The radiologic findings and diagnostic accuracy of CT in intracapsular rupture are similar to those of MRI197—ie, collapse of the implant shell
creating the classic linguine sign.191,201,220–222
Extracapsu-lar ruptures can de difficult to appreciate on CT scan because of the poor soft-tissue differentiation of CT
imaging; Hounsfield units are similar between silicone and soft tissues.197 Nevertheless, most extracapsular
ruptures may be identified by the collapsed implant shell. CT uses ionizing radiation, a possible contraindi-cation in young patients.197
Evolution of Silicone Implants
Maxwell and Baker223 identify five generations of
sili-cone gel implants on the basis of gel viscosity and prop-erties of the elastomer shell (Table 9).
TABLE 9
Evolution of Silicone Gel-Filled Breast Implants
(Reprinted with permission from Maxwell GP, Baker MR: Augmen-tation mammaplasty: general considerations. In: Spear, SL (ed),
Surgery of the Breast, 2nd ed. Baltimore, Lippincott Williams and
Wilkins, 2006. Vol 2, p 1237.)
The third generation of implants was developed in the mid 1980s in an attempt to strengthen the shell and minimize the silicone bleed phenomenon. When a tex-tured surface was added, the resulting implants were fourth generation devices. Cohesive silicone gel implants are considered fifth generation devices.
The extent of cross-linking of the silicone polymers during implant manufacture determines the firmness of the silicone gel. A cohesive gel implant is “form-stable,” meaning that cross-linking is to such a degree that the