Art & science |
The synthesis of art and science is lived by the nurse in the nursing act
JOSEPHINE G PATERSON
Correspondence [email protected] Kari Velzke is dementia knowledge exchange research assistant, University of Stirling Date of submission June 9 2014 Date of acceptance August 29 2014 Peer review
This article has been subject to double-blind review and has been checked using antiplagiarism software Author guidelines rcnpublishing.com/r/ nop-author-guidelines
Evaluation of a dementia
care learning programme
Kari Velzke describes how staff are achieving best practice
and changing the way patients with this disease are being treated
DEMENTIA IS recognised as an international health priority because around 35.6 million people worldwide have the condition, with projections doubling by 2030 and tripling by 2050 (World Health Organization (WHO) and Alzheimer’s Disease International 2012). National dementia strategies have been implemented in Scotland (Scottish Government 2013), Malta (Scerri 2014), China and Hong Kong (Chiu et al 2010) with indications of many others worldwide. These initiatives require the
integration and delivery of evidence-based research and best practice in dementia care.
The Best Practice programme
Many policies and programmes support best practice in dementia care, and vary between countries. To extend and improve services for people with dementia the Dementia Services Development Centre (DSDC) was founded in 1989 at the University of Stirling in Scotland. DSDC is recognised
internationally for its evidence-based service development in providing non-pharmacological support for people with dementia, their families and carers. The centre offers a Best Practice (BP) in Dementia Care Learning Programme involving hospital, care home, day centre and domiciliary care staff in the private, voluntary and statutory sectors.
The BP programme trains and supports
facilitators based in care settings to take a group of their own staff through a programme of training in dementia care over a six-month period. At the end of the programme, staff who complete the course produce a reflective exercise in which they consider a difficult issue that they have faced in their work and how they would have addressed the problem before and after completing the course. The programme is managed on national and international levels by the DSDC and staff from the centre score these reflective exercises. Participants who demonstrate mastery of course material and achieve learning outcomes receive a certificate of completion.
The BP programme has earned multiple accreditations and credentials that emphasise the support it provides as a leading evidence-based and best practice programme in dementia care. The programme integrates the Promoting Excellence Framework (Scottish Government 2011a) and Standards of Care for Dementia in Scotland (Scottish Government 2011b). This programme
Abstract
This article reports on an evaluation of the Dementia Services Development Centre’s Best Practice in Dementia Care Learning Programme for hospitals, care homes including day centres and domiciliary care settings. A multi-method qualitative and quantitative evaluation was undertaken using 100 course participant feedback questionnaires, 60 course participant reflective exercises and 89 online responses to a service manager survey.
Participants’ increased awareness and understanding of dementia in practice were evidence that the learning outcomes had been successfully met. Improved practice supported these results demonstrating a more expansive use of interventions and effective interactions between staff, families and people with dementia in multiple settings.
With this training, practitioners can provide evidence-based and best practice care and support to families and people with dementia in hospitals, care homes, day centres and domiciliary care settings.
Keywords
Best practice, care homes, day centres, dementia care, domiciliary care, hospitals
Art & science | acute care
Art & science | training
conforms to the Scottish Credit and Qualifications Framework (SCQF) (2014) at level 6. It is accredited by the Royal College of Nursing (RCN) (2014) in the UK, and City & Guilds with six SCQF credits at level six. It also references the dementia strategies and the common core principles (Department of Health (DH) 2011) of England (DH 2009), Wales (Welsh Government 2011) and Northern Ireland (Northern Ireland Department of Health, Social Services and Public Safety 2011).
The BP programme booklets that make up the course provide a knowledge base for the SCQF at levels 2 and 3.
Aim
An evaluation of the BP programme was carried out including course delivery in hospitals, care homes, day centres and domiciliary care settings.
The purpose was to support participants’ reflection and further development of the programme by establishing an updated evidence base and evaluating measures of outcomes and improved or changed practice. The learning outcomes, which guided the evaluation, are listed in Box 1. An earlier version of the programme was evaluated (Chapman and Law 2009).
Method
The evaluation included analysis of 100 course participant feedback questionnaires, 60 course participant reflective exercises and 89 online responses to a service manager survey.
The feedback questionnaires and reflective exercises were sampled from each of the
three BP programme areas (hospitals, care homes and domiciliary settings). As the programme is regularly updated, the participants in the evaluation had all completed the programme within the past two and a half years (2011-2014). They came from Scotland, England, Northern Ireland and Wales. Service managers who were involved with the BP programme and able to observe its effect in the care setting they managed completed the online survey. The survey explored how and if the BP programme improved the quality of care, how it affected staff morale, recruitment and retention, and how it affected adverse incidents.
The evaluation received ethical approval from the School of Applied Social Science Research Ethics Committee at the University of Stirling. All participants gave their informed consent to take part in the evaluation. The reflective exercises were anonymised after their authors had given consent for their inclusion in the evaluation.
Results
Each dataset is considered separately.
Feedback questionnaires The pre- and post-test course participant feedback questionnaires analysed included 74 cases from care homes/day centres, 15 cases from hospitals, ten cases from domiciliary care and one case from a retired practitioner, totalling 100 evaluations.
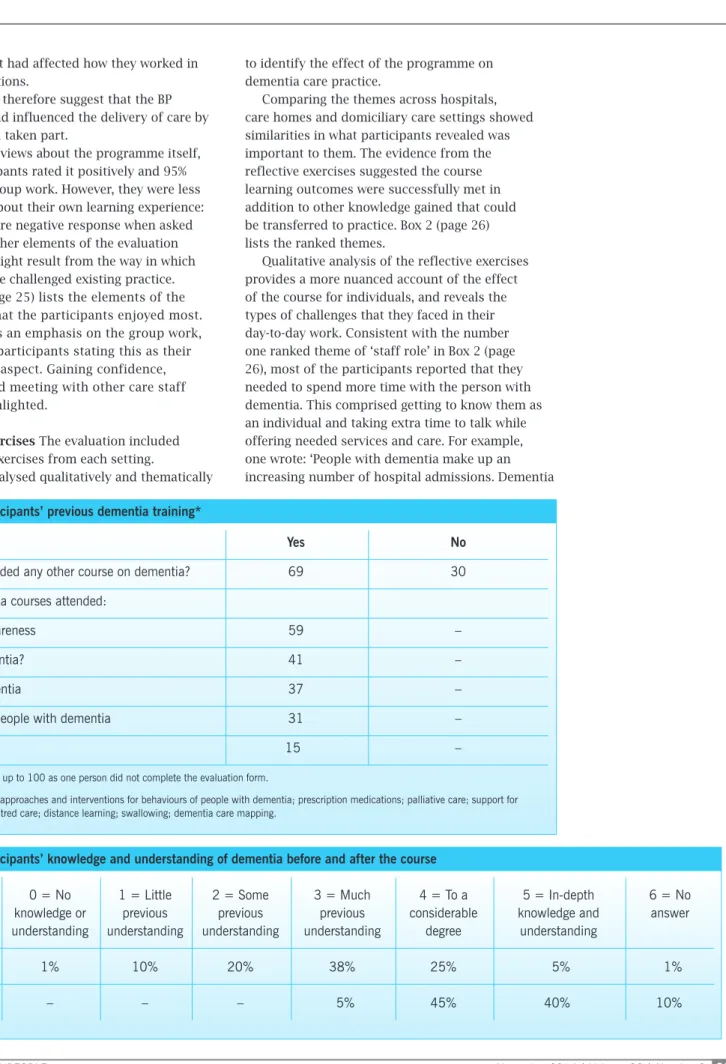
Table 1 outlines the dementia training that participants had received previously. Overall, 69 people had attended other courses before. These mainly covered basic knowledge of dementia and activities for people with the disease.
Table 2 shows the reported effect of the BP programme, highlighting participant knowledge and understanding of dementia before and after the course. There was a distinct change in levels of understanding of dementia, with 95% of participants reporting a considerable degree or in-depth
understanding of dementia post-course, compared with 30% who reported contemporaneously that they had this degree of knowledge before the course started.
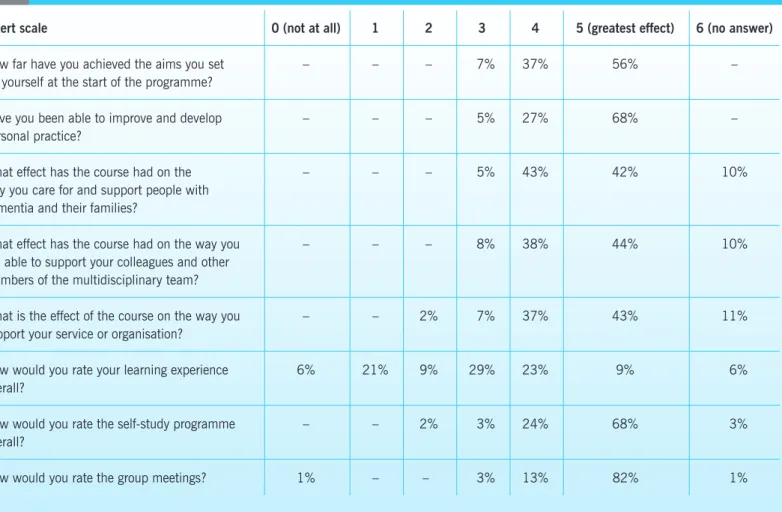
Table 3 (page 24) identifies particular aspects of the learning, thereby exploring participants’ assessments of their own achievement of objectives, the effect on their practice and their views about the course. Participants were asked to rank their learning from the course on a Likert scale ranked 0 to 5, with 0 representing ‘not at all’ (no learned outcomes) and 5 showing the course had the ‘greatest impact’ on their learning.
Most participants reported they had achieved the aims they set for themselves, with only 7% giving a mid-range response. Ninety five per cent reported they had improved and developed their personal practice and 85% that the programme had affected their care and support for people with dementia and their families. Eighty two per cent reported the programme had affected how they worked with, and supported, their colleagues in their teams,
■ Gain a greater understanding of dementia and its effect on individuals.
■ Take part in reflective evaluation of interventions and change practice accordingly.
■ Recognise a person-centred approach to care. ■ Demonstrate a more expansive use of
communication skills when interacting and understanding the needs of people with dementia. ■ Recognise the role of the carer/family, their needs
and the support networks.
Art & science | acute care
Art & science | training
and 80% said it had affected how they worked in their organisations.
The figures therefore suggest that the BP programme had influenced the delivery of care by those who had taken part.
In terms of views about the programme itself, 92% of participants rated it positively and 95% enjoyed the group work. However, they were less enthusiastic about their own learning experience: 30% gave a more negative response when asked to rate this. Other elements of the evaluation suggest this might result from the way in which the programme challenged existing practice.
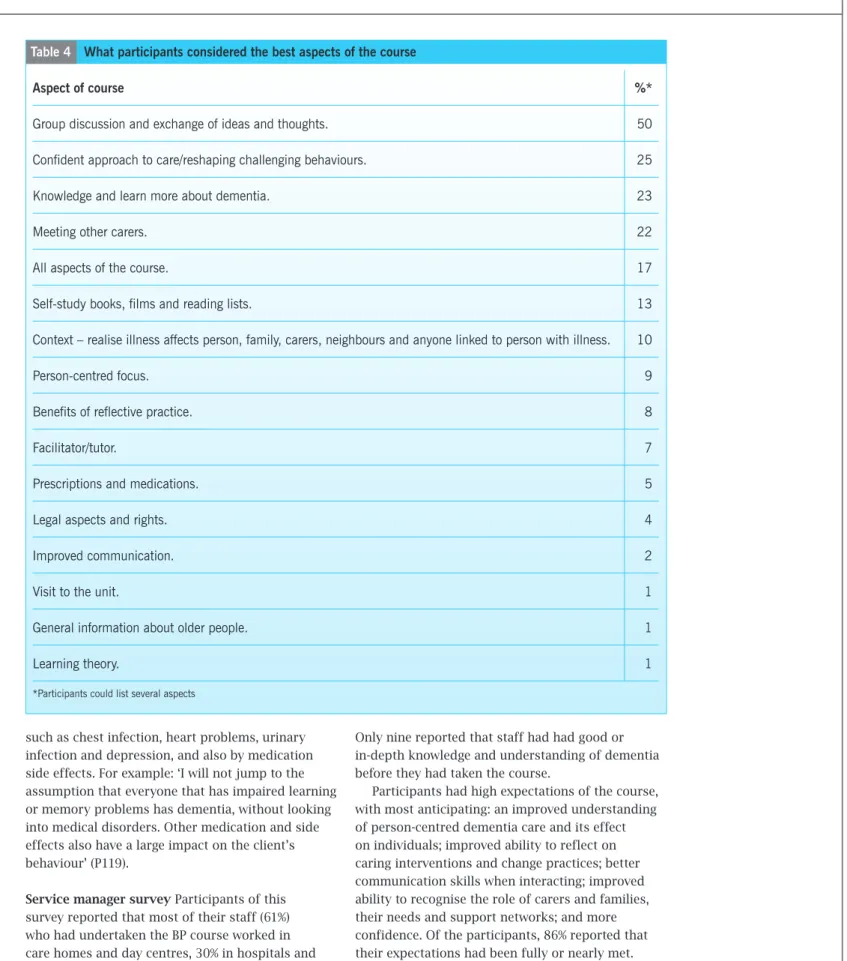
Table 4 (page 25) lists the elements of the programme that the participants enjoyed most. Again, there is an emphasis on the group work, with half the participants stating this as their most enjoyed aspect. Gaining confidence, knowledge and meeting with other care staff were also highlighted.
Reflective exercises The evaluation included 20 reflective exercises from each setting.
These were analysed qualitatively and thematically
to identify the effect of the programme on dementia care practice.
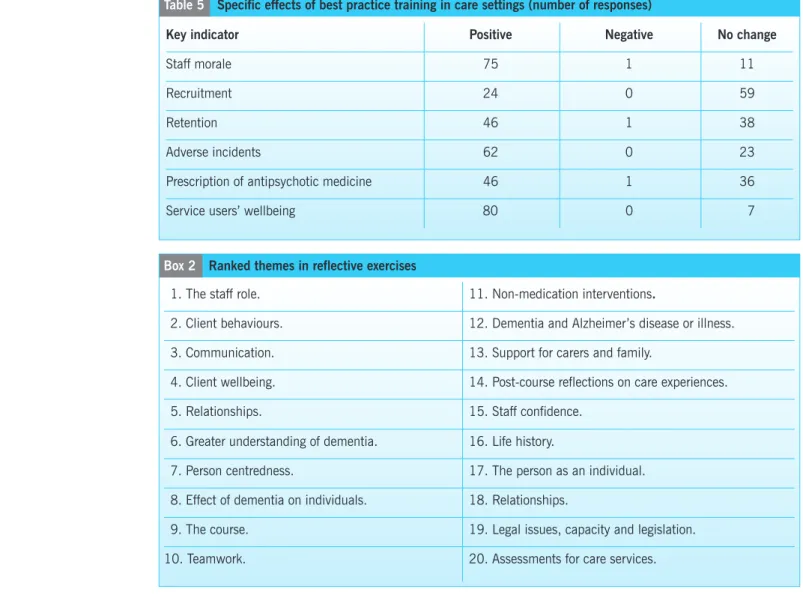
Comparing the themes across hospitals, care homes and domiciliary care settings showed similarities in what participants revealed was important to them. The evidence from the reflective exercises suggested the course learning outcomes were successfully met in addition to other knowledge gained that could be transferred to practice. Box 2 (page 26) lists the ranked themes.
Qualitative analysis of the reflective exercises provides a more nuanced account of the effect of the course for individuals, and reveals the types of challenges that they faced in their day-to-day work. Consistent with the number one ranked theme of ‘staff role’ in Box 2 (page 26), most of the participants reported that they needed to spend more time with the person with dementia. This comprised getting to know them as an individual and taking extra time to talk while offering needed services and care. For example, one wrote: ‘People with dementia make up an increasing number of hospital admissions. Dementia
Yes No
Had you attended any other course on dementia? 69 30
Other dementia courses attended:
Dementia awareness 59 –
What is dementia? 41 –
Types of dementia 37 –
Activities for people with dementia 31 –
Other** 15 –
*Rows do not add up to 100 as one person did not complete the evaluation form.
**Other includes: approaches and interventions for behaviours of people with dementia; prescription medications; palliative care; support for carers; person-centred care; distance learning; swallowing; dementia care mapping.
Table 1 Participants’ previous dementia training*
Likert scale 0 = No knowledge or understanding
1 = Little previous understanding
2 = Some previous understanding
3 = Much previous understanding
4 = To a considerable
degree
5 = In-depth knowledge and
understanding
6 = No answer
Before 1% 10% 20% 38% 25% 5% 1%
After – – – 5% 45% 40% 10%
Art & science | acute care
Art & science | training
changes the client’s relationship with those around them, healthcare assistants can help the person with dementia preserve their memories and abilities, while also helping family members and friends come to terms with who the person is now, rather than once was’ (participant (P) 118).
Environment They recognised that such work, although desirable, could prove challenging to fulfil in a hospital environment.
Other participants reported on the physical environment of the workplace and recognised that this needed change to assist people with dementia. For example, one commented: ‘In our emergency department our flooring is not ideal either; we have flecked flooring with a lot of bold dark stripes in between doors which may appear as a barrier to a client with dementia. Our toilet door is marked W.C. [water closet], which is also not ideal. We need a bright coloured sign with a picture of a toilet on it to help easily identify a toilet to a person with dementia’ (P127).
Another participant had perceived changes in the people she was seeing in hospital: ‘I have worked as a healthcare assistant for 17 years in my current
post in a busy elderly ward. I noticed in my years of working with elderly people that a lot more elderly patients with dementia are being admitted to general wards, as there are not as many specialised dementia units, as seems to be needed to care for those clients’ (P119).
Some participants concluded that a hospital should be the last resort for people with dementia, and when they did have to attend hospital, they should be accompanied by care staff or a family member.
These examples show course participants observing more acute challenges experienced by a person with dementia during a visit to hospital. They are also suggesting changes that could be made.
Changing practice In terms of how they had changed their own practice, staff working in hospitals reported they were better informed about the various types of dementia, signs and symptoms of dementia, and identifying other medical disorders with similar symptoms. Therefore, participants were better at distinguishing people whose dementia-like symptoms could be caused by physical illness
Likert scale 0 (not at all) 1 2 3 4 5 (greatest effect) 6 (no answer)
How far have you achieved the aims you set for yourself at the start of the programme?
– – – 7% 37% 56% –
Have you been able to improve and develop personal practice?
– – – 5% 27% 68% –
What effect has the course had on the way you care for and support people with dementia and their families?
– – – 5% 43% 42% 10%
What effect has the course had on the way you are able to support your colleagues and other members of the multidisciplinary team?
– – – 8% 38% 44% 10%
What is the effect of the course on the way you support your service or organisation?
– – 2% 7% 37% 43% 11%
How would you rate your learning experience overall?
6% 21% 9% 29% 23% 9% 6%
How would you rate the self-study programme overall?
– – 2% 3% 24% 68% 3%
How would you rate the group meetings? 1% – – 3% 13% 82% 1%
Art & science | acute care
Art & science | training
such as chest infection, heart problems, urinary infection and depression, and also by medication side effects. For example: ‘I will not jump to the assumption that everyone that has impaired learning or memory problems has dementia, without looking into medical disorders. Other medication and side effects also have a large impact on the client’s behaviour’ (P119).
Service manager survey Participants of this survey reported that most of their staff (61%) who had undertaken the BP course worked in care homes and day centres, 30% in hospitals and 16% in domiciliary settings (several staff worked across settings). A total of 68% of service managers reported having previously attended dementia training, although 30% of service managers had not.
Only nine reported that staff had had good or in-depth knowledge and understanding of dementia before they had taken the course.
Participants had high expectations of the course, with most anticipating: an improved understanding of person-centred dementia care and its effect on individuals; improved ability to reflect on caring interventions and change practices; better communication skills when interacting; improved ability to recognise the role of carers and families, their needs and support networks; and more confidence. Of the participants, 86% reported that their expectations had been fully or nearly met. All reported having made improvements in practice after the course, with most reporting these as significant. The strongest effects were reported to be on ways that staff cared for and supported
Aspect of course %*
Group discussion and exchange of ideas and thoughts. 50
Confident approach to care/reshaping challenging behaviours. 25
Knowledge and learn more about dementia. 23
Meeting other carers. 22
All aspects of the course. 17
Self-study books, films and reading lists. 13
Context – realise illness affects person, family, carers, neighbours and anyone linked to person with illness. 10
Person-centred focus. 9
Benefits of reflective practice. 8
Facilitator/tutor. 7
Prescriptions and medications. 5
Legal aspects and rights. 4
Improved communication. 2
Visit to the unit. 1
General information about older people. 1
Learning theory. 1
*Participants could list several aspects
Art & science | acute care
Art & science | training
people with dementia, with significant effects on mutual support among colleagues and the service or organisation concerned as a whole. Of participants, 80 rated the programme overall as useful (14) or very useful (66).
Table 5 lists the responses to specific indicators that reflect challenges often experienced in care organisations.
These responses suggest significant effects in several particularly difficult areas, notably morale and recruitment and retention of staff. Adverse incidents and the use of antipsychotic medications – two areas that have been a cause of serious public and political concern – seem to have been improved in many cases. The results about service users’ wellbeing confirm the indications from the previous responses.
Discussion
Overall, the BP programme appears to have been successful in meeting its aims. Although some staff found it challenging, staff and managers reported
the positive effects on practice across various care settings. In particular, the course addressed some of managers’ main concerns in terms of workforce management and adverse incidents. The evaluation therefore adds weight to arguments for improved training of front line staff in dementia care. However, among the challenges staff encountered in making changes in practice was the difficulty in being given time to be released for training.
The reported strengths of the course, which were deemed to be important parts of the learning process, included the booklets, watching videos and conversing with colleagues.
Limitations included the course length – it takes six months to complete – and it has been suggested by a small number of managers that it should be shortened. Another manager stated there are a few areas of the course that need adapting for day care. Another stated questions and role plays were sometimes ambiguous, however, the facilitator handbook clarified these.
Key indicator Positive Negative No change
Staff morale 75 1 11
Recruitment 24 0 59
Retention 46 1 38
Adverse incidents 62 0 23
Prescription of antipsychotic medicine 46 1 36
Service users’ wellbeing 80 0 7
Table 5 Specific effects of best practice training in care settings (number of responses)
1. The staff role. 11. Non-medication interventions.
2. Client behaviours. 12. Dementia and Alzheimer’s disease or illness.
3. Communication. 13. Support for carers and family.
4. Client wellbeing. 14. Post-course reflections on care experiences.
5. Relationships. 15. Staff confidence.
6. Greater understanding of dementia. 16. Life history.
7. Person centredness. 17. The person as an individual. 8. Effect of dementia on individuals. 18. Relationships.
9. The course. 19. Legal issues, capacity and legislation.
10. Teamwork. 20. Assessments for care services.
Art & science | acute care
Art & science | training
References
Alzheimer’s Society (2013) This is Me Tool. tinyurl.com/d9qbftx (Last accessed: September 30 2014.)
Chapman A, Law S (2009) Bridging the gap: An innovative dementia learning program for healthcare assistants in hospital wards using facilitator-led discussions. International Psychogeriatrics. 21, Suppl 1, 58–63.
Chiu H, Yu X, Lam L (2010) Dementia strategy in China and Hong Kong. International Journal of Geriatric Psychiatry. 25, 9, 905–907.
Department of Health (2009) Living Well with Dementia: A National Dementia Strategy. tinyurl.com/bwzgnor (Last accessed: September 23 2014.)
Department of Health (2011) Common Core Principles for Supporting People with Dementia. tinyurl.com/ozjsh5b (Last accessed: September 23 2014.)
Northern Ireland Department of Health, Social Services and Public Safety (2011)
Improving Dementia Services in Northern Ireland: A Regional Strategy. tinyurl.com/cbdwn5n (Last accessed: September 23 2014.)
Royal College of Nursing (2014) RCN Endorsement of Professional Standards and Resources. tinyurl.com/q9lmkae (Last accessed: September 23 2014.)
Scerri C (2014) National Dementia Strategy: Malta 2015-2023. tinyurl.com/qh7Kp4n (Last accessed: September 25 2014.)
Scottish Credit and Qualifications Framework (2014) SCQF Levels. www.scqf.org.uk/The%20Framework/ Level%20Descriptors (Last accessed: September 23 2014.)
Scottish Government (2011a) Promoting Excellence: A Framework for All Health and Social Services Staff Working with People with Dementia, their Families and Carers. www.scotland.gov.uk/Resource/ Doc/350174/0117211.pdf (Last accessed: September 23 2014.)
Scottish Government (2011b) Standards of Care for Dementia in Scotland. www.scotland. gov.uk/Resource/Doc/350188/0117212.pdf (Last accessed: September 23 2014.)
Scottish Government (2013) Scotland’s National Dementia Strategy 2013-2016. www. scotland.gov.uk/Resource/0042/00423472.pdf (Last accessed: September 23 2014.)
Welsh Government (2011) National Dementia Vision for Wales. tinyurl.com/mex2js5 (Last accessed: September 23 2014.)
World Health Organization and Alzheimer’s Disease International (2012) Dementia: A Public Health Priority. tinyurl.com/6n9hr6e (Last accessed: September 23 2014.)
Implications for practice
There have been reports that reflective practice has led to new ways to approach situations on the ward. Participants reported that care planning is an essential part of good practice and when clients were admitted some wards created a profile, changing the colour of folders for people admitted with dementia to achieve the best quality of care. Most wards reported using ‘This is Me’ documents (Alzheimer’s Society 2013), which list information about the patient such as where they were born, family members, likes and dislikes and favourite pastimes. Information was reported as helpful when trying to communicate with a person who has dementia because it assisted in building trust with the client. Participants also reported that distraction techniques, added communication and conversation and additional activities were used to divert unwanted behaviour and agitation.
Areas of changed practice overlapped into multiple areas such as collecting additional information about medical and life histories,
person-centred care and viewing the person as an individual, rather than focusing on illnesses. Other areas included changed practice evidenced by observations of increased empathy, understanding and sympathy, increased confidence and communication, medications and alternative interventions and service options and support for families.
Conclusion
Practitioners reported the course resulted in changing their practice, implementing evidence-based and best practice care,
and supporting families and people with dementia in hospitals, care homes, day centres and domiciliary care settings. Successful course learning outcomes were evidenced by increased awareness and understanding of dementia in practice in these settings. Improved practice supported these results, demonstrating a more expansive use of interventions and effective interactions between staff, families and people with dementia in multiple settings.
Acknowledgements
The author offers special thanks to Professor Alison Bowes for multiple contributions and sharing her expertise, and to Dementia Services Development Centre (DSDC) staff for support during the research process Conflict of interest
This project was funded in full by the DSDC at the University of Stirling. The Best Practice programme is the property of the DSDC. DSDC staff did not take part in the evaluation process
Online archive
For related information, visit our online archive and search using the keywords