POINT-OF-CARE HIV TESTING FOR EARLY INFANT DIAGNOSIS DURING THE POSTPARTUM PERIOD: TIMING AND TYPE OF TEST MATTERS
Emily Rose Smith
A dissertation submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Epidemiology
in the Gillings School of Global Public Health.
Chapel Hill 2015
ABSTRACT
Emily Rose Smith: Point-of-Care HIV Testing for Early Infant Diagnosis During the Postpartum Period: Timing and Type of Test Matters
(Under the direction of Annelies Van Rie)
In the past decade, large gains have been made in reducing pediatric HIV infections during the prenatal or peripartum period. However, recent changes in the World Health Organization (WHO)
breastfeeding guidelines will likely shift the majority of new infant HIV infections to the postnatal period1,2. Although breastfeeding guidelines have changed, early infant diagnosis (EID) recommendations have not been updated.
In this dissertation, I evaluated the performance of two HIV rapid tests, Determine and Unigold, on a cohort of 121 Malawian HIV-exposed, breast-fed infants who were HIV negative at 6 weeks postpartum from 3 to 18 months of age. I also evaluated the cost-effectiveness for several EID strategies that varied in type, timing, and number of rapid tests, including an Alere test, a point-of-care virological assay, through Markov modeling.
ACKNOWLEDGEMENTS
I’ve often thought over the past few years that the journey of going through a PhD program is
made up of more than just the person pursuing the degree. Often, they are surrounded by mentors and support. I have been fortunate to have had both.
First and foremost, I want to thank my committee chair and academic advisor, Annelies Van Rie. Annelies’ reputation of being brilliant and expecting excellence preceded her and I am thankful to have
benefited from these qualities. She has pushed me farther than I thought I could go which, in turn, has resulted in academic maturing and becoming more of a researcher. I will always be grateful to her guidance, advice, and pursuit of excellence, as well as friendship as a woman in academia.
I would also like to thank my other committee members who in their each unique way provided mentorship and guidance. To Bill Miller, thank you for serving as a “life coach” not only concerning my
dissertation but life in general. To Stephanie Wheeler, thank you for being patient in teaching me a semester’s worth of modeling concepts in a few weeks. Thank you for also serving as a woman/mother
academic in research. To Michael Hudgens, thank you for your guidance, patience, and availability as well as being very approachable to ask questions and learn. To Jeff Stringer, thank you for your insight regarding “in the field” applications to the questions I asked. Thank you to the entire committee for
striving for a project that was not simply a way to get a degree but one that mattered in the world. Prior to UNC, there have been several key players in my academic career, beginning with my Dad. Dad, you said the word “can’t” was a bad word and I was young and naive enough to believe you
who both afforded the ability to stretch my academic wings, encouraged excellence, and have become lifelong friends.
I would like to thank Nancy Colvin and Valerie Hudock for their open doors and arms to all of us epidemiology students, including myself. I would also like to thank my friends I have made in the SPH, especially Katie Lesko, Jaymin Patel, Liz Cromwell, Melissa Arvay, and Kathy Lancaster. I am grateful to have made such strong professional connections and life friends.
I am also thankful for the many friends that have loved and encouraged myself and my family. Specifically, I want to extend a special thank you to the Ladies at Immanuel Baptist Church and Mark and Gayla Partin who have become extended family members.
Thank you to my parents and Mike’s parents for more than I can express. I am grateful to be
loved so deeply by them all without ever having to earn any of it through accomplishments. To my Dad, you have been my biggest teacher of life and learning and I’m convinced this entire journey started with you. To my Mom, you are the unsung hero with the many meals you’ve made, the tons of laundry you’ve folded, the coffee gift cards you’ve sent, and many other countless ways you expressed your love. To my
in-loves (i.e., in-laws), I am so grateful for the support of both Mike and I through this journey. To all the grandparents and my sister, I cannot express enough how grateful I am for you all loving on Bella and Jonathan. I don’t think they even knew how hard of a journey this has been because you all have loved
them when I needed some help. Thank you, thank you for that.
To my kids, Bella and Jonathan. You two are my greatest joy and blessing (second to your Dad). You have reminded me what is truly important in life every day when I come home. When we started this program, you were 2 years and 3 months old. I studied while rocking at 3am by the light of an iPhone, you marked and colored on all my school books, you greeted me with cake and balloons when I finished a big test, you did your “homework” with me, we took first and last day of school pictures together
To Mike, we had no idea what we were about to do 4 years ago and how challenging (and wonderful) it would be. You have provided consistent strength, love, and security to us as a family. You have held us together, celebrated at each juncture, and pointed us to grace. You have provided the gracious encouragement to pursue good works and fix my eyes on faith, while also reminding me what Sabbath rest looks like. This journey is much more joyous with you. Thank you for being a safe place to call home.
TABLE OF CONTENTS
LIST OF TABLES ... xi
LIST OF FIGURES ... xii
LIST OF ABBREVIATIONS ... xiii
CHAPTER 1: SPECIFIC AIMS ... 1
CHAPTER 2: BACKGROUND ... 4
2.1 Dramatic improvements in PMTCT to reduce prenatal and perinatal transmission ... 4
2.2 Early infant HIV diagnosis ... 7
2.3 Increasing importance of MTCT during breastfeeding ... 8
2.4 Monitoring of HIV infection during the breastfeeding period ... 12
2.5 The acquisition and decay of maternal antibodies ... 16
2.6 Current recommended HIV testing algorithms for HIV-exposed infants with a negative 4-6 week virological test ... 22
2.7 Significance of the proposed project: The intersection of the current PMTCT structure, current EID testing algorithms, and 2010 WHO breastfeeding recommendations ... 25
CHAPTER 3: DESCRIPTION OF THE STUDY POPULATION AND DATA COLLECTION ... 26
3.1 Study setting ... 26
3.2 Study population ... 27
3.3 Data Collection for the parent study ... 27
3.4 Data collection for proposed study ... 32
CHAPTER 4: METHODS ... 35
4.1 Specific Aim 1 ... 35
4.1.2 Statistical Analysis ... 36
4.2 Specific Aim 2 ... 37
4.2.1 Study Sample and Data Collection ... 37
4.2.2 Statistical Analysis ... 37
4.3 Specific Aim 3 ... 38
4.3.1 Analytic overview ... 38
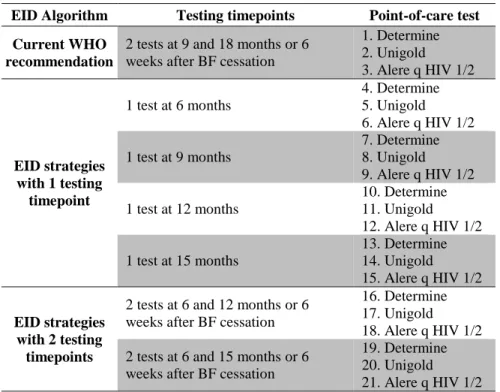
4.3.2 Early infant diagnosis algorithms ... 38
4.3.3 Model structure ... 42
4.3.4 Model input parameters for the base case model: Clinical input parameters (Table 11) ... 46
4.3.5 Model input parameters for the base case model: Economic input parameters (Table 11) ... 56
4.3.6 Model input parameters for the base case model: Test performance parameters (Table 11) ... 58
4.3.7 Outcomes ... 62
CHAPTER 5: RESULTS. PERFORMANCE OF HIV RAPID TESTS AMONG BREASTFEEDING, MALAWIAN INFANTS ... 64
5.1 Results ... 65
5.2 Discussion ... 67
CHAPTER 6: RESULTS. TIMING OF HIV SEROREVERSION AMONG HIV-EXPOSED, BREASTFED INFANTS IN MALAWI: TYPE OF RAPID TEST MATTERS ... 76
6.1 Results ... 77
6.2 Discussion ... 77
CHAPTER 7: EVALUATION OF POINT-OF-CARE EARLY INFANT HIV DIAGNOSIS ALGORITHMS AMONG HIV-EXPOSED INFANTS DURING THE BREASTFEEDING PERIOD: A COST-EFFECTIVENESS ANALYSIS ... 80
7.1 Base case results (see Appendix B, Table 20 for full results) ... 81
7.2 Discussion ... 82
APPENDIX A. COMPARISON BETWEEN DEMOGRAPHIC CHARACTERISTICS
IN COMPLETE CASE VERSUS MISSING POPULATION ... 93
APPENDIX B. RESULTS: AIM 3 ... 97
Base case results ... 97
LIST OF TABLES
Table 1. 2006 and 2010 WHO recommendations on HIV and infant feeding. ... 11
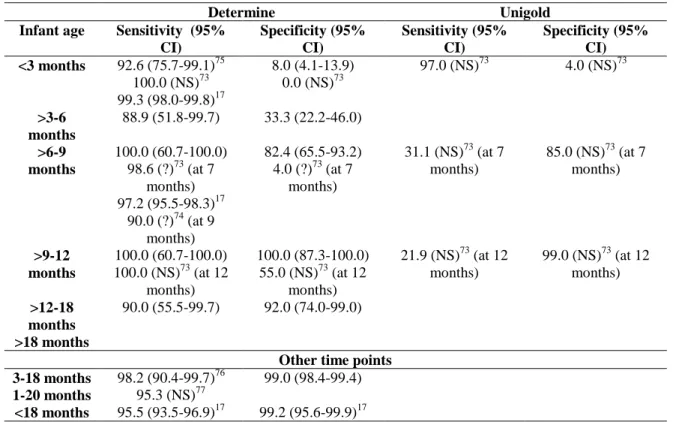
Table 2. Sensitivity and specificity of Determine and Unigold rapid test ... 14
Table 3. Procedures for HIV-exposed infants ... 28
Table 4. Procedures for HIV positive mothers or primary caregivers ... 29
Table 5. Rapid test results for parent study during follow-up period ... 31
Table 6. Summary of UNC rapid testing ... 33
Table 7. Description of collected or missing rapid test data throughout follow-up, stratified by type of rapid test. ... 34
Table 8. Description of early infant HIV diagnosis testing strategies ... 39
Table 9. Cumulative incidence of postpartum HIV infant infection. ... 41
Table 10. Markov model transition matrix ... 44
Table 11. Model input and sensitivity parameters ... 60
Table 12. Characteristics of cohort of HIV-exposed infants with negative PCR test at 6 weeks in Malawi ... 70
Table 13. Sensitivity and specificity of Determine and Unigold assays during the postpartum period ... 71
Table 14. Positive and negative predictive values of Determine and Unigold assays during the postpartum period with varying pediatric HIV incident infections ... 72
Table 15. Estimated probability of seroreversion at a certain age, by rapid test ... 79
Table 16. Base case results: POC test results, total costs, and pediatric outcomes for early infant diagnosis algorithms ... 85
Table 17. Incremental cost-effectiveness ratio (ICER) comparison of EID strategies ranked by total EID costs ... 87
Table 18. Comparison of demographic characteristics in complete case population versus missing population: Determine ... 93
Table 19. Comparison of demographic characteristics in complete case population versus missing population: Unigold ... 95
LIST OF FIGURES
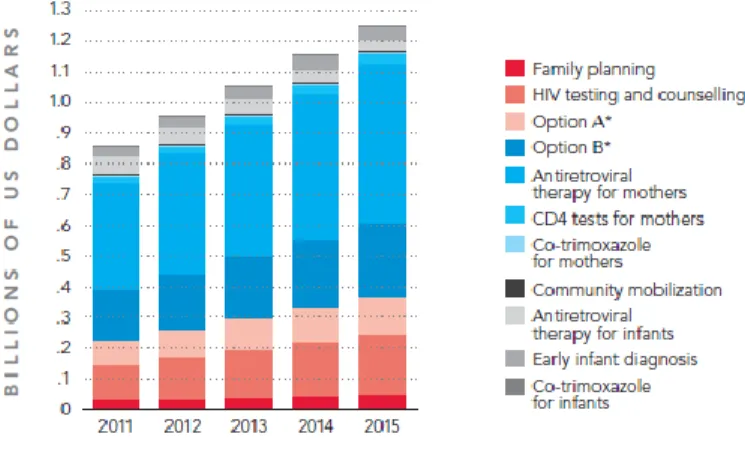
Figure 1. Investment needs in 22 priority countries from Global Plan ... 6
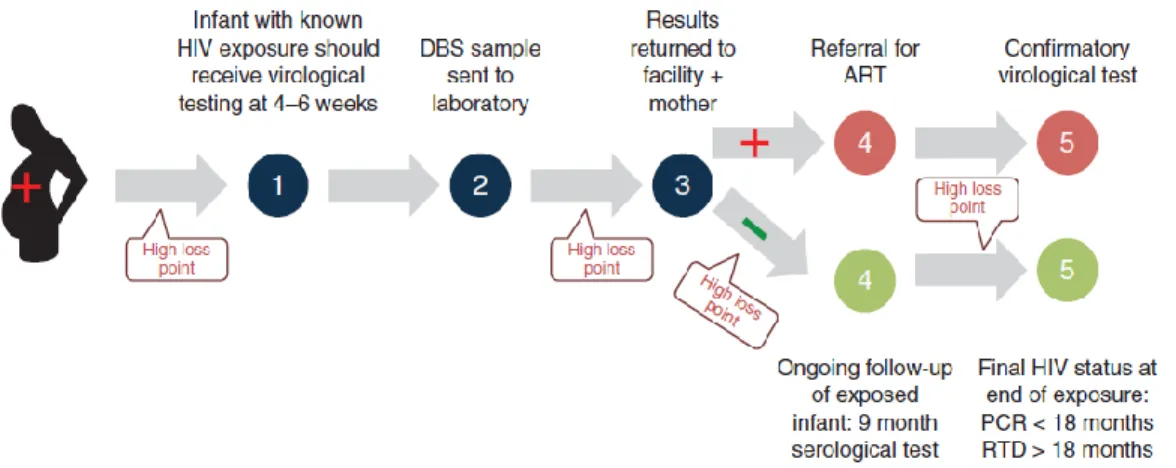
Figure 2. Early Infant Diagnosis Testing Cascade ... 7
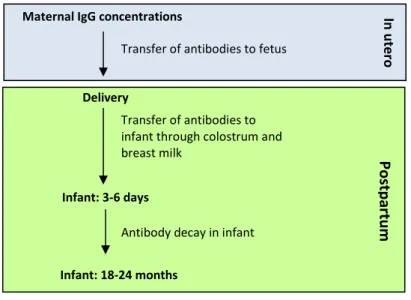
Figure 3. The acquisition and decay of maternal antibodies ... 17
Figure 4. WHO early infant HIV testing algorithm ... 23
Figure 5. Model structure ... 43
Figure 6. Markov model and transition matrices for each 3 month time cycle ... 45
Figure 7. Specificity of Determine and Unigold assays during the postpartum period ... 74
Figure 8. Results of rapid tests in 21 children with negative HIV DNA PCR at age 6 weeks and subsequent confirmed HIV infection ... 75
LIST OF ABBREVIATIONS
AIDS Acquired Immune Deficiency Syndrome ART Antiretroviral therapy
ARV Antiretroviral
BAN Breastfeeding, Antiretrovirals, and Nutrition Study CDC Centers for Disease Control
CI Confidence interval
DT Determine
EBF Exclusive breastfeeding EID Early infant diagnosis
ELISA Enzyme-linked immunosorbent assay HAART Highly active antiretroviral therapy HEU HIV-exposed, uninfected
HIV Human immunodeficiency virus
Ig Immunoglobulin
IQR Interquartile range
MDG Millennium Development Goal
MF Mixed feeding
MTCT Mother-to-child transmission NPV Negative predictive value PCR Polymerase chain reaction
PMTCT Prevention of mother-to-child transmission PPV Positive predictive value
UN Unigold
CHAPTER 1: SPECIFIC AIMS
About 1.5 million HIV positive women become pregnant each year3, resulting in a 1.5 million infants at risk of HIV infection. In 2010, the Joint United Nations Programme on HIV/AIDS Global Plan set forth ambitious goals including reducing the mother-to-child transmission (MTCT) of HIV to less than 5% by 2015. Efforts to scale up prevention of mother-to-child transmission (PMTCT) services for HIV positive mothers in low resource settings has yielded promising results, such as more widespread distribution of antiretroviral (ART) therapy and an increased uptake in PMTCT services. Despite these improvements, an estimated 260,000 children under 5 were infected with the virus in 20113, almost all (90%) of these infections occurred in sub-Saharan Africa.
PMTCT guidelines recommend at least 4 antenatal care visits during pregnancy, provision of ARV prophylaxis to the infant during pregnancy and delivery, and virological testing at 4-6 weeks4. Under these guidelines and the widespread scale-up of ART services in resource-poor settings, MTCT of HIV is likely to be successful in further reducing vertical transmission of HIV during the antenatal, delivery, and early infancy (i.e., first 6 weeks) periods. However, the current PMTCT cascade
inadequately captures the postpartum period as it typically stops after delivery or, at best, after the 4-6 week infant virological test. In addition, postpartum transmission of HIV comprises 15% to 35% of new pediatric infections, suggesting current PMTCT strategies insufficiently capture the postpartum period and are not sufficient to eliminate HIV among infants5-7. Postpartum-acquired HIV is expected to increase given the recent changes in breastfeeding guidelines. HIV positive mothers are now encouraged to
months of life8. The extended duration of breastfeeding will increase the duration an infant’s exposure, which will increase the incidence of infant HIV acquisition through breastfeeding.
Early infant diagnosis (EID) of HIV infection is critical in the survival of HIV infected children9. The WHO currently recommends HIV-DNA/RNA polymerase chain reaction (PCR) and ultra-sensitive p24 antigen assays for EID10. In countries where the risk of infant HIV infection is the highest, the utility of virologic tests are hindered by significant financial and logistical challenges. EID is also crucial in identifying seroreversion and seroconversion. Current PMTCT recommendations suggests testing infants with a rapid test 6 weeks after weaning but have not adequately addressed how to test infants in the interim period between 6 weeks of age and the cessation of breastfeeding. Rapid tests could be used in infants age 3 to 24 months, but their performance is hindered by the presence of maternal HIV antibodies. After the age of 3 months, it is unclear when rapid tests are able to distinguish between an infant HIV infection and maternal antibodies in breastfeeding populations, severely inhibiting the utility of rapid tests during the postpartum period8,11,1213-17. Furthermore, different rapid tests have been shown to perform differently in infants and have not been evaluated during the entire breastfeeding period.
The Global Plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive will only be achievable if we redefine the PMTCT cascade to encompass the mother/infant dyad throughout the entire breastfeeding period. Changes in breastfeeding guidelines will increase the number of HIV-exposed infants after the 6 week virological test. Given the importance of early ART initiation, timely, cost effective, and accurate HIV testing strategies are critical for
breastfeeding infants who escaped HIV infection during the first 6 weeks of life.
Specific Aim 1:
Evaluate the performance of Determine and Unigold tests by:
Aim 1a. Determining the sensitivity, specificity, positive predictive values, and negative predictive values of Determine and Unigold rapid tests for identifying incident HIV infections, compared with the PCR reference standard, among breastfeeding, HEU infants (i.e., PCR negative at 6 weeks).
Aim 1b. Describing the Determine and Unigold rapid test results for all children with documented incident HIV infection during the breastfeeding period among infants who were PCR negative at 6 weeks.
Specific Aim 2:
Determine the median time to seroreversion in a cohort of breastfeeding, HEU infants (i.e., PCR negative at 6 weeks) during the first 3 to 18 months of life.
Specific Aim 3:
CHAPTER 2: BACKGROUND
2.1 Dramatic improvements in PMTCT to reduce prenatal and perinatal transmission
Large gains have been made in reducing infant HIV acquisition by the effective development and implementation of prevention of mother-to-child transmission (PMTCT) programs over the past two decades and most notably after 2010. In 2010, the Global Plan set forth ambitious goals including reducing the mother-to-child transmission (MTCT) of HIV to less than 5% by 201518. Efforts to scale up PMTCT services for HIV positive mothers in 22 priority countries, 1 in India and 21 in Africa, has yielded promising results, such as an increase in HIV testing and counseling among pregnant women, more widespread distribution of antiretroviral (ARV) therapy and an overall uptake in PMTCT services19. Rapid scale up of PMTCT services has been dramatic over the last few years with over 60% of pregnant women receiving some PMTCT service15,20. Coverage of ART programs has increased from 10% in 200421 to 62% in 201219. From 2009-2011, ART prophylaxis prevented an estimated 409,000 new infant infections in resource poor settings22. Since 2003, new infections in children worldwide dropped by 43% and in the last 4 years alone new infections declined by 24%22. New HIV infections among infants have been reduced by 50% in seven of the Global Plan’s priority countries1
. Although the number of new infections among children is decreasing, the number of women newly infected with HIV has remained stable since 20091.
Current PMTCT guidelines
interventions during labor and delivery4. All pregnant women are encouraged to have at least 4 antenatal care visits with services for vaccinations, screening and treatment for infections, and early identification of warning signs. During the antenatal care visits, women are also offered HIV testing and counseling. If the woman is HIV positive, she is given offered an ARV regimen and encouraged to deliver in a facility equipped with PMTCT interventions. Postpartum PMTCT guidelines include following up of the infant and mother with HIV testing and linkage to HIV services if needed.
Limitations of the current PMTCT guidelines
Although PMTCT guidelines have greatly increased the number of women on ART during antenatal care, there is a paucity of guidance on how to manage HIV-exposed infants during the postpartum period for two reasons.
Figure 1. Investment needs in 22 priority countries from Global Plan
ARV prophylaxis is recommended for the infant during labor and delivery and extended NVP is recommended while the mother is breastfeeding. However, there remains a paucity of recommendations on how to ensure the health and well-being of the HIV-exposed infant during the postpartum period.
#2: The PMTCT cascade typically stops after delivery or, at best, after the infant’s 4-6 week
Figure 2. Early Infant Diagnosis Testing Cascade
2.2 Early infant HIV diagnosis
Accurate and timely diagnosis of HIV is crucial for the survival of HIV infected children as early initiation of treatment is required given the risk of rapid progression of disease in young infants. Without ART, up to 60% of HIV-infected infants die by the second year25,26. Given that EID and early ART initiation, regardless if the disease has progressed clinically or immunologically, can dramatically increase an infected infant’s health outcomes, including mortality, timely detection should be a priority9
. HIV testing methods for EID
The WHO recommends HIV-DNA or HIV-RNA PCR tests as well as ultra-sensitive p24 antigen assays for EID in resource limited settings10. A virological test is recommended at the first postnatal visit at 4-6 weeks and a serological test is recommended after the initial 4-6 week test if the infant develops signs or symptoms suggestive of HIV or when the infant reaches 9 months of age (Figure 3)27. Virological testing in HEU infants occurs again 6 weeks after discontinuation of breastfeeding to rule out HIV
Implementation of EID
Significant increases in EID have been seen worldwide through integrating EID with
immunization services and scaling up virological testing using dried blood spots for PCR. However, these tests require samples to be transported from remote sites to centralized laboratory facilities. In developing countries where the risk of infant HIV infection is the highest, significant financial and logistical
challenges hinder the utility of these tests.
EID is not only hindered by logistical factors but also greatly affected by attrition after delivery. Recent data shows that an alarming number of infants born to women with HIV do not receive testing within the first 2 months of life, with attrition numbers as high as 92%21,24. Recent studies in sub-Saharan Africa among lactating populations have documented attrition rates of up to 80% by 6 months, greatly impacting the utility and evaluation of virological diagnostic assays, particularly since the women have to return to the clinics a few weeks later to receive test results31-42.
2.3 Increasing importance of MTCT during breastfeeding
real-world scenarios. Thus, it is likely the 36% breastfeeding-associated mortality risk is underestimated and highlights the need for timely and accurate detection of infection during the postpartum period.
Until recently, most of the reductions in infant HIV infections have occurred during pregnancy, delivery, and early infancy (i.e., birth to 6 week virological test)1. The current PMTCT guidelines of ARV interventions for pregnant and lactating women have been highly successful in reducing vertical
transmission of HIV during antenatal, delivery, and early infancy (i.e., first 6 weeks) periods. As a consequence, it is estimated that over half of all new infections in high burden countries will occur during the breastfeeding period1. In areas with long breastfeeding, as many as 8 out of 10 newly acquired HIV infections will occur during the breastfeeding period 1. Recent changes in the WHO breastfeeding guidelines will likely increase the duration and intensity of breastfeeding in many countries and thus increase an infant’s recurrent exposure to HIV over a longer period of time, thereby increasing breastfeeding-associated MTCT.
WHO Guidelines on HIV and infant feeding (Table 1)
In 2006,HIV infected women were to choose the most appropriate infant feeding option based on their individual circumstance. Exclusive breastfeeding was recommended for the first six months of life unless replacement feeding in the local setting was acceptable, feasible, affordable, and sustainable. When such a replacement feeding was found, HIV infected mothers were encouraged to avoid all breastfeeding. When replacement feeding was not acceptable, feasible, affordable, and sustainable, HIV infected mothers should continue breastfeeding with complementary foods. Breastfeeding should then be stopped once a nutritionally adequate diet without breast milk could be provided. No recommendations regarding the use of ARV during breastfeeding were given.
growth deficits and other severe infections, such as bouts of diarrhea and pneumonia44,49-53. Similarly, exclusive breastfeeding was found to improve HIV free survival in HEU infants54,55. Decreased HIV transmission within the first six months of life was also found to be associated with exclusive breastfeeding compared to mixed feeding46,55,56.
New research also highlighted that providing HIV infected mothers and/or their infants with ARV interventions could significantly reduce their risk of postnatal HIV transmission through breastfeeding. The provision of ARV along with breastfeeding through 12 months was found to prevent transmission and detrimental health benefits seen with mixed feeding57-62. In particular, HIV infected women who were given 3-drug antepartum ARV prophylaxis, regardless of CD4 count, through six months of study had lower rates of MTCT during breastfeeding61. Likewise, the Breastfeeding, Antiretrovirals and Nutrition (BAN) trial found 53% protective efficacy associated with providing 3-drug ARV prophylaxis during breastfeeding in women with CD4 > 250 cells/ul60. A 2011 systematic review also reported that the risk of HIV transmission during breastfeeding can be substantially reduced to 1-2% with ARV intervention62. These findings had profound implications for the HIV-infected mothers and their decision to breastfeed and how long to breastfeed for HIV positive mothers.
In 2010, the WHO changed the recommendations for HIV and infant feeding. HIV positive mothers are now encouraged to exclusively breastfeed for the first 6 months of life, introduce
Table 1. 2006 and 2010 WHO recommendations on HIV and infant feeding.
Maternal and infant interventions for prevention of HIV transmission during breastfeeding Treatment recommendations for HIV positive pregnant and postpartum women have been streamlined since 2010 with the adoption of a single, universal regimen of ART for life 4. Since 2010, countries could choose between Option A, Option B, and Option B+ for pregnant, HIV positive women. Under Option A, women with CD4 counts ≤350 cells/mm receive triple ARVs starting as soon as diagnosed and infants receive a prophylactic regimen of daily nevirapine from birth through 1 week beyond the cessation of breastfeeding. Under Option B, women received triple ARVs as early as 14 weeks gestation and continued after cessation of breastfeeding and infants receive daily nevirapine or AZT from birth through age 4-6 weeks regardless of infant feeding method. Under Option B+, women receive tripe ARVs starting as soon as diagnosed and continued through life and infants receive the same prophylactic therapy as Option B. The simplified approaches of Option B and Option B+ have greatly increased the number of HIV positive women who initiated ARV while pregnant.
Even though the simplified treatment approaches of Option B and Option B+ have significantly increased the number of HIV positive, pregnant women initiating ART, significant challenges remain. Only 4 of the 22 priority countries of the Global Plan achieved the goal of providing ARV to 90% of pregnant women living with HIV. Among women residing in sub-Saharan Africa, only 59% received ARV therapy or prophylaxis during pregnancy and delivery in 201119,63. Only 58% of mothers64 and 29-41% of HIV-exposed infants received antiretroviral (ARV) therapy in 200965,66.
2006 recommendations 2010 recommendations
Based on clinical stage and CD4 cell count. Mothers known to be HIV-infected should be provided with lifelong ARV therapy or ARV prophylaxis interventions to reduce HIV transmission through
breastfeeding. The most appropriate infant feeding option for an
HIV-infected mother depends on her individual circumstances. Exclusive breastfeeding is recommended for HIV-infected mothers for the first six months of life unless replacement feeding is acceptable, feasible, affordable, sustainable and
safe for them and their infants before that time. All breastfeeding should stop once a nutritionally adequate and
safe diet without breast milk can be provided.
Mothers known to be HIV-infected (and whose infants are HIV uninfected or of unknown HIV status) should exclusively breastfeed their infants, regardless if ARVs
are available, for the first 6 months of life, introducing appropriate complementary foods thereafter, and continue breastfeeding for the first 12 months of life. Breastfeeding should then only stop once a nutritionally adequate and
Problems with adherence to ART in the postpartum period
Among HIV positive women who initiated ART, high rates of non-adherence are observed in the prenatal and postpartum period (33% and 47%, respectively)67. Moreover, the highest rates of treatment default occur after 6 weeks postpartum and occurs progressively throughout the first 12 months1131,36,68,69. Long-term ART adherence in PMTCT programs during the postpartum period has received less attention, even though the risk of nonadherence is higher36,37,42. The large drop off in treatment throughout the postpartum period results in missed opportunities to improve the health of the HIV positive mother and exposed infant through appropriate testing and treatment, if needed.
2.4 Monitoring of HIV infection during the breastfeeding period
Monitoring infant HIV infection status in the breastfeeding period is critical to timely identify HIV and to accurately rule out HIV infection. Early initiation of ART can dramatically increase the infant’s likelihood of survival, particularly among perinatally-infected children. Ruling out HIV infection
(i.e., identifying the time of seroreversion) is also critical to breastfeeding, HIV positive mothers of HEU infants as this gives the mother peace of mind and increases the likelihood she will continue to breastfeed.
Ideally, virological tests should be used in the breastfeeding period to accurately determine the infant’s HIV infection status. As previously discussed, these tests are hindered by significant challenges
in resource poor settings and repeat virologic tests throughout the breastfeeding period are not affordable in most settings. Rapid tests during the breastfeeding period could serve as a cost-effective and efficient tool for testing HIV. Repeat rapid tests are cheaper and allow for quick results that eliminate the loss-to-follow-up often seen when using virological tests that require lab transportation time, batch testing, and longer waiting time for results11,12.
Performance of rapid tests after the 4-6 week virological test
(ELISA) in detecting HIV infection in low resource settings, although each test performs differently in clinical practice with varied sensitivities and specificities70,71.
Adults.Several rapid tests have been approved by the FDA for point of care HIV testing. In a study directly comparing all FDA approved rapid tests, the sensitivity and specificity of all tests exceeded 95%72 although Unigold had the lowest sensitivity compared to Reveal G3, Multispot HIV-1/2, OraQuick Advance HIV-1/2, Stat-Pak, and Complete (96.8%, 98.9%, 99.6%, 99.5%, 98.3%, 100%, respectively)72. Infants.Rapid tests have been evaluated in children, but there is a paucity of data regarding rapid tests performance among infants younger than 9 months. Table 2 summarizes the studies which examined sensitivities and specificities of two rapid tests, Determine and Unigold, in infants younger than 18 months. All studies were conducted in resource-poor settings. Sensitivities and specificities are stratified by infant age. There were also instances where results were not stratified by infant age, making age-specific interpretation of test performances difficult. Those sensitivities and age-specificities are noted at the bottom of the table under “Other time points”.
Table 2. Sensitivity and specificity of Determine and Unigold rapid test
Determine Unigold
Infant age Sensitivity (95% CI) Specificity (95% CI) Sensitivity (95% CI) Specificity (95% CI) <3 months 92.6 (75.7-99.1)75
100.0 (NS)73 99.3 (98.0-99.8)17
8.0 (4.1-13.9) 0.0 (NS)73
97.0 (NS)73 4.0 (NS)73
>3-6 months
88.9 (51.8-99.7) 33.3 (22.2-46.0)
>6-9 months
100.0 (60.7-100.0) 98.6 (?)73 (at 7
months) 97.2 (95.5-98.3)17
90.0 (?)74 (at 9 months)
82.4 (65.5-93.2) 4.0 (?)73 (at 7
months)
31.1 (NS)73 (at 7 months)
85.0 (NS)73 (at 7 months)
>9-12 months
100.0 (60.7-100.0) 100.0 (NS)73 (at 12
months)
100.0 (87.3-100.0) 55.0 (NS)73 (at 12
months)
21.9 (NS)73 (at 12 months)
99.0 (NS)73 (at 12 months)
>12-18 months
90.0 (55.5-99.7) 92.0 (74.0-99.0)
>18 months
Other time points 3-18 months 98.2 (90.4-99.7)76 99.0 (98.4-99.4)
1-20 months 95.3 (NS)77
Performance of alternative rapid tests
Fourth generation assays.Fourth generation assays have recently been developed and detect both HIV antibody and p24 antigen, antigen expressed in the seroconversion phase of HIV infection, providing an earlier detection of HIV infection than previous generation assays.
Adults.Field assessment of the fourth generation Determine HIV-1/2 Ag/Ab Combo rapid test was conducted among 1,009 participants in testing and counseling center in Malawi78. Although the test detected established HIV infection, it did not detect acute HIV infections better than the current testing algorithms of using Determine and Unigold tests. In a large study of 21,334 HIV positive persons in San Francisco, the potential for case finding of acute HIV cases was the highest for the 4th generation
ARCHITECT HIV Ag/Ab Combo (99.1%; [95% CI: 91.1, 100.0]) and lower for Determine (96.6%; [95% CI: 84.7, 100.0]), Unigold (94.3%; [95% CI: 82.4, 100.0]), OraQuick Advance on blood plasma (92.8%; [95% CI: 88.2, 97.3), and Clearview Stat-Pak (92.8%; [95% CI: 83.8, 100.0])79.
Infants. In theory, fourth generation rapid tests should be able to detect HIV infection sooner than third generation rapid tests because of early p24 antigen in infants. A recent study among infants in South Africa found that the fourth generation Determine Combo HIV-1/2 Ag/Ab Combo Test failed to detect p24Ag in 98% of HIV infected infants80. Even at 3 months of age, the sensitivity of the p24 antigen component was less than 10%. Among 13 infants with clinical symptoms and advanced stage disease, the test detection p24 antigen in one resulting in a sensitivity of 1.7%. The use of fourth generation rapid tests does not perform better than that of third generation HIV rapid tests, particularly among younger infants.
Oral rapid tests.Oral rapid tests serve as a less invasive option for sampling since the test requires oral fluid instead of blood. These tests are generally easier to perform and consume less time to perform.
performance of 4 rapid HIV tests among 21,234 HIV positive patients in San Francisco found OraQuick ADVANCE Rapid HIV-1/2 Antibody test using oral fluid was much lower (86.6%; [95% CI: 79.4-92.0]) than the other three rapid tests (OraQuick Advance using fingerstick blood, Vironostika HIV-1
Microelisa, Genetic Systems HIV ½ Plus 0)79.
Infants.The performance of oral rapid tests among infants has not been as widely studied. A South African cross-sectional study among 597 HIV-exposed infants (birth-6 months of age) compared three oral rapid tests (OraQuick, Calypte, and Orasure)84. OraQuick performed best in detecting and excluding HIV exposure but the test did not detect exposure in 12% of infants. Although this study is generally relevant to the literature, it is not the goal of the proposed study since all of our infants will be HIV-exposed already. No studies have been evaluated the performance of oral rapid tests among infants who have been exposed to the disease.
2.5 The acquisition and decay of maternal antibodies
Rapid serological tests cannot distinguish between maternal antibodies and infant antibodies, making a definitive HIV diagnosis in the infant difficult13,14. Transfer of maternally acquired antibodies, particularly IgG antibodies, is crucial to an infant’s early defense of infectious agents. Of the five
antibody classes, only significant amounts of IgG are transferred across the placenta, and, after birth, IgA becomes the predominant class transferred through colostrum and breast milk. During the breastfeeding period, maternal antibodies are replaced by the child’s own antibodies. This progression of the transfer
and decay of maternally-acquired IgG are affected by several factors, including maternal characteristics, pregnancy outcomes, and infant age and is depicted in Figure 4.
In utero factors contributing to transplacental antibody transfer
of gestation, placental integrity, maternal IgG concentrations.
Figure 3. The acquisition and decay of maternal antibodies
Length of gestation: The most significant factor directly associated with total IgG transfer in newborns length of gestation. Maternal transfer of IgG occurs in a linear fashion beginning as early as 13 weeks, with the largest amount transferred in the last trimester85-88. During the second trimester, fetal IgG concentrations are only 5%-10% of maternal levels, and concentrations reach 50% of maternal levels during weeks 28-32. The largest total IgG amount acquired by the fetus occurs during the last 4 weeks of pregnancy. The association between length of gestation of IgG levels in newborns has been observed for specific antibodies against measles, mumps, diphtheria, tetanus, pertussis, influenza, rubella, and E. Coli86,89-92.
Low birth weight:Reduced IgG transfer efficiency has been observed among low birth weight babies87,91. In a cohort of infants in Sri Lanka, infants with low birth weights demonstrated low levels of antibody transfer, even after adjusting for gestational age93. It should be noted that all mothers with low birth weight infants in the Sri Lankan study were anemic. Although birth weight may have a direct effect on IgG transfer, length of gestation serves as a more significant contributor since IgG transfer is greatly dependent on weeks in utero than the infant’s weight at birth. Thus, birth weight may serve as a proxy for
length of gestation.
Maternal IgG concentrations
Transfer of antibodies to fetus
Delivery
Transfer of antibodies to infant through colostrum and breast milk
Infant: 3-6 days
Antibody decay in infant
Infant: 18-24 months
In
u
te
ro
Po
stp
ar
tu
Total maternal IgG concentrations: Newborn IgG levels typically correlate with maternal ones94. However, IgG levels can be saturated and depend on the amount of cell surface receptors present in the infant. After a saturation point, there is an inverse relationship between maternal IgG concentrations and IgG transfer to the infant, resulting in lower neonatal IgG values than maternal ones87. This phenomenon of lower IgG transfer is observed in certain regions in Africa where high maternal IgG values are
common87,95,96. Specifically for HIV, mean levels of maternal IgG concentrations for all antibodies except HSV are significantly higher in HIV-infected mothers than non-infected mothers, thereby lowering the transfer of IgG to the infant97,98.
Maternal IgG concentrations and transfer of IgG to the infant are impacted by ART exposure, both in utero and prophylactically. In a European study, infants with ART exposure in utero through maternal ART or neonatally through prophylactic therapy had lower IgG levels than infants with no ART exposure. Similarly, ART reduced the number of circulating IgG in chronically infected individuals in New York99. The majority of women in the European and New York studies had lower IgG levels than women in Africa, rendering it difficult to deduce if this relationship is observed in women with higher baseline maternal IgG concentrations typically seen in Africa. High baseline maternal IgG concentrations among HIV-infected women in Africa (i.e., above the saturation point) are correlated with lower IgG transfer. Thus, ART administration to HIV-infected women with high baseline IgG concentrations, as in Africa, would reduce the activation of the chronically-activated immune system, thereby increasing the amount of IgG transferred to the infant.
a higher severity of disease, displaying the inverse relationship between maternal IgG levels and IgG transfer to the infants87,97,98,105.
Clinical indicators of HIV severity, including viral load and CD4 count, are associated with placental IgG transfer. In a cohort of HIV positive, pregnant women in Nairobi, a strong inverse association between placental IgG transfer and HIV-1 viral load in the third trimester or at delivery has been observed 105,106. In addition, women with CD4 counts less than 200 had reduced placental transfer of IgG compared with women with CD4 counts above 500. Controlling HIV viremia and boosting
production of CD4 counts through effective ART at the end of a woman’s pregnancy, the time where the
majority of transfer of IgG occurs, could increase the efficiency of placental transfer.
Other: Although gestational age, maternal IgG concentrations, and placental integrity are noted most consistently in the literature as significant contributors to IgG transfer to the infant, other
characteristics may also impact IgG transfer. Among women in Kenya, transfer of tetanus-specific antibodies was lower in women with low BMI, transfer of measles- and tetatnus-specific antibodies was lower in women with preterm delivery, transfer of measles-specific antibodies was lower in younger ages101,106. However, the majority of other studies do not find an association between BMI, maternal age, preterm delivery, and parity once gestational age, maternal IgG concentration, and co-morbidities are adjusted for90,101.
Persistence of maternal antibodies during the postpartum period
Maternal HIV Immunoglobulin G (IgG) antibody can be detectable up to 18 months but usually become undetectable by 9 months of age. Studies from industrialized countries have reported median ages at seroreversion of 7-12 months107-109 and an estimated 1%-2% of HEU US and European infants do not serorevert until 15 months of age109. In developing countries, however, there is a lack of data on
age17. Maternal antibodies decline slowly throughout the first year of life in the postpartum period with a half-life of 28 to 30 days in non-breastfed infants13,15-17. However, there are minimal data on the
persistence of maternal antibodies in breastfed populations. Of the studies describing persistence of maternal antibodies, three of the studies were in industrialized countries among non-breastfeeding populations107-109 and three studies occurred prior to the WHO guidelines changing that encouraged breastfeeding for HIV-pregnant/lactating women and were among non-breastfeeding populations13,15,17,73. There were two studies which examined a mixed population of breastfeeding and non-breastfeeding HIV positive women, although the percentage of breastfeeding women was not provided1516. Only one study describing seroreversion documented the percentage of breastfeeding HIV positive women but this percentage was very low at 4%110.
Postpartum factors affecting waning of placentally-acquired antibodies
After birth, IgA becomes the predominant antibody class transferred through colostrum and breast milk111. In addition, maternally-acquired IgG decay during the postpartum period, with the most rapid waning occurring before 9 months of age. During the first few days after delivery, colostrum is the predominant form of nutrition given to an infant and contains many protective properties, including antiviral and immunological substances. The immunoglobulin content, particularly IgG , in colostrum is much higher than that in breast milk111. Contributions of IgM and IgG are produced but in minuscule quantities112-116. Over 92%-95% of IgG is transferred in utero while the remaining 5%-8% is transferred mainly through colostrum from day 0 to day 6 and in very small quantities thereafter through breast milk113-116. Breast milk antibodies do not enter the infant circulation in substantial amounts and, of the five immunoglobulin classes, the most significant transfer is IgA. Although the relationship between antibody decay during the postpartum period and a myriad of maternal and infant characteristics have been examined, the most significant contributors consistently noted in the literature are infant age and maternal IgG concentrations.
antibody positive to mumps or rubella while 9% were antibody positive to measles117. Similarly, other studies have found the concentration of passively-acquired IgG for measles, mumps, and rubella decreased rapidly within the first six months of life118 and the concentration of pertussis-specific IgG decreased rapidly within the first two months of life119.
Other than infant age, very few infant-related characteristics have been identified that impact waning of placentally-transferred antibodies. A study among rural Bangladeshi infants found measles-specific antibody concentrations decreased with age and the child’s length, weight, gestational age, and
parity were not associated120. Similarly, a Congolese study found age was the only factor influencing decay of measles antibody, even after adjusting for infant gender, birth weight, weight-for-age, maternal age, and parity121.
Maternal IgG concentrations. Maternal IgG concentrations not only affect the transfer of antibodies in utero but also impact the clearance of antibodies in infants after delivery87,94,95,120,122-124. Elevated maternal IgG concentration reduces transplacental efficiency for the infant, resulting in lower infant IgG levels acquired in utero. Thus, the rate of infant antibody decay after delivery is faster among infants born to women with elevated IgG concentrations than infants born to women with lower IgG concentrations.
ART therapy. Mean time to seroreversion seems to be shorter in studies performed earlier in the HIV epidemic, particularly, before the usage of PMTCT or ART. An analysis on 3 MTCT prevention trials in Malawi found that infants born from 1989 to 1996 had a significantly shorter time to
was 3 months longer than the median ages seen in Malawi during the same time period, again indicating ART treatment could delay clearance of antibodies since ART usage was higher in the US than Malawi16.
Although historical data, as noted above, seems to suggest maternal ART contributes to seroreversion delays, to date there have been no studies to explicitly evaluate how ART/HAART affects the time of seroreversion in infants. A small case analysis of 14 infants less than 12 months who initiated ART therapy in rural India observed that the majority of these infants did not develop sufficient
antibodies for detection on rapid test due to ART128. However, this paper did not provide what type of rapid test was used, the number of tests performed per time period, and the ages of the children.
Other factors complicating the utility of rapid tests.Another risk factor contributing to time to seroreversion is birth weight as children with higher birth weights were more likely to serorevert at a younger age16. Gender, gestational age, mother’s clinical stage of AIDS, breastfeeding status, and child’s health history have not been found to be associated with time to seroreversion16,109.
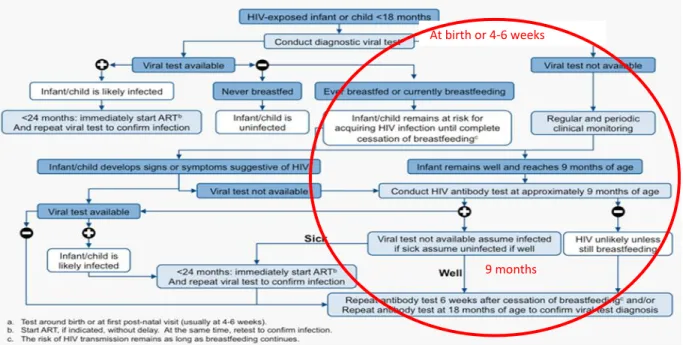
2.6 Current recommended HIV testing algorithms for HIV-exposed infants with a negative 4-6 week virological test
Currently, there are three main HIV testing algorithms used worldwide: 1) the 2010 WHO recommendations on the diagnosis of HIV infection in infants and children (Figure 5); 2) the CDC testing algorithm for HIV-exposed infants in settings with ART, PCR availability, and resources permit either replacement feeding or two tests per infant; and 3) the CDC testing algorithm in settings without widespread ART, limited resources for virological testing, and where most women breastfeed. WHO Recommendations
Figure 5 describes the current WHO early infant HIV testing algorithm27. The group of interest given the current breastfeeding guidelines (see Section B.3), is represented in the red circle. Infants that tested negative on the 4-6 week virological test and continued to be breastfeed remain at risk for acquiring HIV until cessation of breastfeeding occurs. According to the WHO algorithm, after a negative
suggestive of HIV occur prior to 9 months. The following two scenarios could ensue among breastfeeding infants who tested negative on a virological test at age 4 to 6 weeks:
Scenario 1: Infants who remain well are to receive an HIV antibody test beginning at 9 months of age. If the antibody test at 9 months is negative the child is assumed uninfected. A repeat antibody test is to be given six weeks after the cessation of breastfeeding and/or at 18 months of age.
Scenario 2: If infants develop signs or symptoms suggestive of HIV between 4-6 weeks and 9 months, they are to be given a virological test. If a viral test is not available, an HIV antibody test is to be performed at 9 months.
Figure 4. WHO early infant HIV testing algorithm
The testing algorithm in both scenarios recommend sparse HIV testing of HEU infants during the time between the 4-6 week virological test and 18 months of age or cessation of breastfeeding unless the infant is sick, in which it may be too late. Between age 4-6 weeks and 9 months of age, no testing is recommended unless the child is sick. This time period is approximately 7 months. A test is
recommended at 9 months of age and then again 6 weeks after cessation of breastfeeding or until 18 months of age. This second risk period after age 9 months is approximately 2-9 months depending on
At birth or 4-6 weeks
when the child weans. The entire risk period from the 4-6 week virological test to the cessation of breastfeeding is 11 to 16 months. It is not adequate enough to ensure early initiation of ART if the child does become infected through breastfeeding to simply test HIV-exposed infants a few times during the breastfeeding risk period. Another pitfall of the algorithm is that the algorithm does not describe what tests or combination of rapid tests to use at any timepoint. As previously discussed (Section B.4), these tests have widely different performances when used among infant populations in resource limited settings. CDC testing algorithm for HIV-exposed infants in settings with ART, PCR availability, and resources permitting either replacement feeding or two tests per infant 129
The only recommendation for an HEU infant who is younger than 9 months is to conduct PCR virological testing. If the HEU infant is 9 months of age or older, a rapid HIV antibody test is to be conducted. If the rapid test is positive, a PCR should be conducted. If the rapid test is negative and the infant has not been breastfed within the last 6 weeks, the child is considered HIV negative. If the rapid test is negative and the infant has been breastfed within the last 6 weeks, the infant is “probably” not infected but is still at risk and a repeat rapid test should be conducted 6 weeks after cessation of
breastfeeding. Similar to the WHO EID testing recommendations, there is no information regarding what test to use and the frequency of and accuracy of each test. Additionally, testing occurs infrequently during the breastfeeding exposure period, placing the HEU infant at risk of late diagnosis.
CDC testing algorithm in settings without widespread ART, limited resources for virological testing, and where most women breastfeed129
Similar to the WHO EID testing recommendations and the CDC testing algorithm for settings with ART, PCR availability, and resources permitting either replacement feeding or two tests per infant, there is no information regarding what test to use and the frequency for each test. Additionally, testing occurs even more infrequently than the other testing algorithms during the breastfeeding exposure period, placing the HEU infant at risk of late diagnosis. Given increasing access to virologic testing for EID, the utility of this algorithm is outdated for most settings. Nonetheless, testing recommendations are briefly outlined.
2.7 Significance of the proposed project: The intersection of the current PMTCT structure, current EID testing algorithms, and 2010 WHO breastfeeding recommendations
Current testing algorithms do not adequately describe how to optimally follow HEU infants, including what specific rapid test to use and when to administer the test, during the time between the 4-6 week virological tests through the cessation of breastfeeding. Given the effectiveness of early ARV initiation, it is unacceptable to test an infant only a few times during the high risk period of repeated exposure through breastfeeding or to wait until the child develops symptoms suggestive of HIV..
Highlighting the need for updated testing algorithms further are the recent changes in
breastfeeding guidelines. The duration of breastfeeding will increase an infant’s recurrent exposure to HIV over a longer period of time, which will increase the proportion of infant HIV acquired during the breastfeeding period, especially given that this risk period is not adequately captured in the current PMTCT structure. Studies evaluating rapid tests performance in resource poor settings among
breastfeeding populations are especially important now that women will breastfeed for longer periods of time, increasing the risk of postnatal infection through exposure of HIV via breast milk.
CHAPTER 3: DESCRIPTION OF THE STUDY POPULATION AND DATA COLLECTION
3.1 Study setting
The data used for this study came from a community-based cohort study examining the effects of HIV on pediatric neurodevelopment. The study was conducted at two healthcare centers in the Blantyre region of Malawi between May 2008 and March 2012. Both clinics have PMTCT programs which provide HIV counseling and testing of all pregnant women, and offered nevirapine treatment for prevention of mother to child transmission of HIV.
In Malawi an estimated 57,000 (13%) pregnant women and 90,000 children were living with AIDS in 200866. In 2010, Malawi was one of the 21 African priority countries targeted in the Global Plan to reduce MTCT of HIV to less than 5%, increase PMTCT services, and provide more widespread distribution of ARV therapy18. Since then, new HIV infections among infants have been reduced by 50% in seven of the Global Plan’s priority countries, including Malawi1. Despite these significant advances, Malawi continues to have one of the highest rates of HIV positive women who did not receive effective ARV regimens. In 2012, an estimated 69%-77% of HIV positive women did not receive ARVs while 50% of women globally did not receive their ARVs19.
women reported breastfeeding after 6 months131. In the study population, 78% of HIV positive women were breastfeeding at 6 months, 52% at 9 months, and 36% at 12 months.
3.2 Study population
Study population for the parent study
Inclusion criteria for the parent study included infants born to mothers greater than 15 years of age and included both HIV positive and HIV negative mothers. Exclusion criteria included mothers with active maternal alcohol or drug abuse or maternal chronic illness other than AIDS. All children, without congenital malformations or severe chronic illness, who were born to HIV infected mothers at the two participating health centers were screened for HIV infection at 4-6 weeks of age after appropriate HIV counseling and obtaining oral consent.
Study population for the proposed study
Of the 556 children enrolled in the parent study, 96 perinatally infected infants, 170 children were born to HIV negative mothers, and 290 children born to HIV positive mothers. Children enrolled in the proposed study were eligible for inclusion if they were born to an HIV infected mother, had a negative PCR test at 4 to 6 weeks of age, and had a Determine or Unigold rapid test performed after 4 to 6 weeks of age. Rapid testing in the parent study began 9 months after the start of the study and children without any rapid testing before this 9 month period were excluded. Children were also excluded if they had a rapid test performed but the type of rapid test (Determine or Unigold) was not collected. The final dataset for the proposed study includes 121 children born to an HIV positive mother and were deemed HIV negative at 4 to 6 weeks by PCR.
3.3 Data Collection for the parent study
Procedures
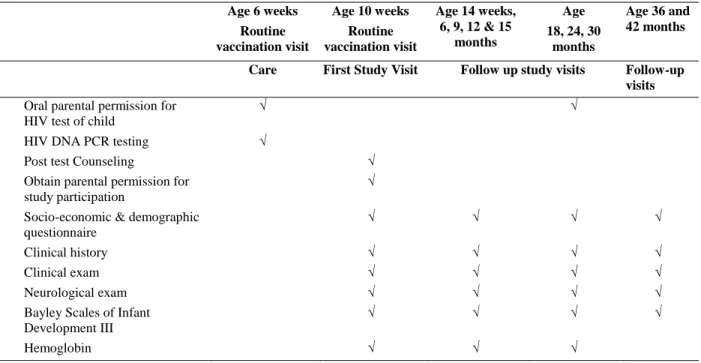
positive PCR result was sought through a second PCR or through HIV RNA viral load testing. Children enrolled in the study were asked to visit the clinic at 10 weeks and every 3 months between age 14 weeks and 18 months, and every 6 months between age 18 and 42 months. Blood was collected at all time points, unless HIV seroconversion was documented at one of these time point. At ages 14 weeks, 6, 9, 12 and 15 months blood was collected for storage for biomarkers and HIV DNA PCR testing. Blood was taken for hemoglobin at each visit.HIV rapid tests using Unigold® and Determine® test kits were performed at 6, 9, 12, 15, and 18 months.
Table 3. Procedures for HIV-exposed infants
Data collection procedures for the mother or primary caregiver, if no biological mother, are outlined in Table 4. Maternal or primary caregiver clinical history and sociodemographic information was collected at enrollment and updated at each follow-up visit. Sociodemographic data collected included marital status, level of education, employment status, caregiving responsibilities, members living in the household, household characteristics (i.e., toilet facilities, availability of electricity, building materials of the house and roof), assets and finances, utility of a mobile phone, and health of the child’s father.
Clinical history included ARV regimen, usage of nevirapine at birth (maternal and infant), co-morbidity
Age 6 weeks Routine vaccination visit
Age 10 weeks Routine vaccination visit
Age 14 weeks, 6, 9, 12 & 15
months
Age 18, 24, 30
months
Age 36 and 42 months
Care First Study Visit Follow up study visits Follow-up visits
Oral parental permission for HIV test of child
√ √
HIV DNA PCR testing √
Post test Counseling √
Obtain parental permission for study participation
√
Socio-economic & demographic questionnaire
√ √ √ √
Clinical history √ √ √ √
Clinical exam √ √ √ √
Neurological exam √ √ √ √
Bayley Scales of Infant Development III
√ √ √ √
assessment, disruptions in work due to illness, and hospitalizations. Changes in maternal/primary caregiver contact information, primary caregiver status and clinical history were updated throughout the follow-up period. Missed visit date and attempts to contact the primary caregiver were recorded as needed. Unscheduled visit dates, reason for the unscheduled visit, and diagnoses at the unscheduled visit were recorded as needed. Selected infant blood samples collected in the parent study were shipped from Malawi to the University of North Carolina at Chapel Hill (UNC).
Table 4. Procedures for HIV positive mothers or primary caregivers
Rapid test results for the parent study
There were 121 children that were followed from their 4-6 week negative PCR test. Table 5 describes the rapid testing that was completed on the 121 children from 2 months through 24 months. According, these children would return to the clinic for rapid testing every 3 months until 18 months of
Form Description Age 10 weeks
(Enrollment) Follow up Visits Unscheduled visits Used as needed Patient Contact Information Form
Used to record phone number, address and tracing permission
√ Update
Study Summary Sheet
Used to track dates of lab procedures and changes in HIV status
√ Update Update
Immunization Record Form
Used to record immunization history of the child
√ Update
Maternal Clinical History and Socio-demographics OR Primary Caregiver Clinical History and Socio-demographics
Form
Records information on the child’s home environment, health of the
caregiver and parents.
√
Clinical Form Records clinical history of the child, clinical examination, neurological
examination and AIDS staging
√ √
Primary Caregiver Clinical History and Socio-demographics
follow-up
Updates information on the caregiver’s health and the child’s
home environment
√
Change in Primary Caregiver
Used to record changes in primary caregiver if there is a change
√
Missed Visit Form Used to record information when a child misses a visit and attempts to contact the family and reschedule.
√
Unscheduled Visit Form
Used to record information about an unscheduled visit to the study clinic
√
ARV treatment Log Log to record treatment with ARVs √
Inactivation of Study Participation
Form
Used if a child discontinues the study or dies before the end of the study
age and then again at age 24 months. However, there were many times when the children were brought into the clinic earlier or later than these timepoints due to various reasons, such as missed visits or coming earlier/later to a scheduled appointment.
Throughout the follow-up period for each child at each timepoint, four scenarios could have occurred:
1) Both rapid tests were run and the results agreed between the two tests (DT+/UN+, DT-/UN-), 2) Both rapid tests were run but the results were discordant (DT-/UN+, DT+/UN-),
3) Only one rapid was conducted (DT- or +/UN missing, DT missing/UN- or +), and 4) Neither rapid test was conducted (DT missing, UN missing).
31
Table 5. Rapid test results for parent study during follow-up period
Collected data from parent study (n=737 rapid test results)
Missing data from parent study
(n=152 rapid test results)
Timepoint (month)
Results agree Results discrepant Determine missing, Unigold complete
Determine collected,
Unigold missing Timepoint
(month)
Missing both DT and UN
DT+/DT+ DT-/UN- DT+/UN- DT-/UN+ DT?/UN+ DT?/UN- DT+/UN? DT-/UN? DT?/UN?
2 0 0 0 0 0 0 0 0 2
3 0 0 1 0 0 3 0 0 3 37
4 0 0 0 0 0 0 0 0 4
6 6 34 27 1 0 18 1 0 6 11
7 0 0 1 0 0 0 0 0 7
8 0 0 1 0 0 0 0 0 8
9 2 39 22 0 0 10 0 1 9 8
10 0 0 0 0 0 2 0 0 10
12 2 43 1 0 1 7 0 7 12 12
15 1 34 0 0 0 4 0 17 15 4
18 2 29 1 0 0 5 1 22 18 2
21 1 2 0 0 0 0 0 2 21
22 0 1 0 0 0 0 0 0 22
24 0 19 0 0 0 3 4 27 24 2
>24 0 18 1 0 0 3 3 18 >24
Total DT 14 219 55 1 0 0 9 94 Missing
DT
76
Total UN 14 219 55 1 1 55 0 0 Missing
UN
76
Total tests 28 438 110 2 1 55 9 94 Total
missing
3.4 Data collection for proposed study
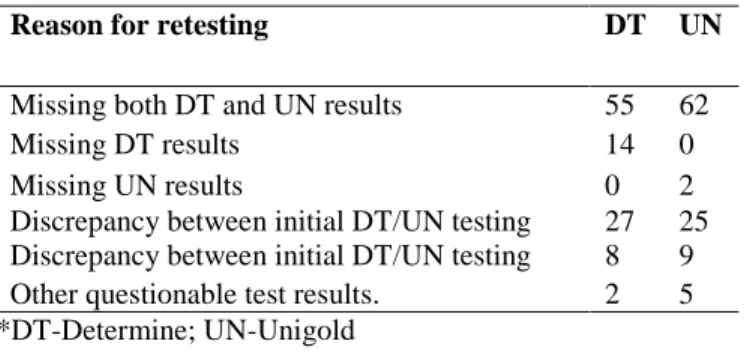
Per study protocol, children were scheduled to visit the study clinic at age 6, 9, 12, 15, 18, 21, and 24 months. However, data was collected when the mothers and children came for a visit, which was not always at the time of the scheduled appointment. Some children also missed scheduled visits, resulting in missing rapid test data for that timepoint. To address the issue of missing rapid test data and investigate the discordant results between Determine and Unigold results, we conducted 100 Determine and 100 Unigold rapid tests on a select group of stored samples. We prioritized samples according to the following criteria summarized in Table 6:
1. Obtain results that would provide us with the shortest seroreversion time.
Priority for testing of samples was given to earlier timepoints or timepoints that would result in a shorter seroreversion observation window. For example, if an infant was positive on both rapid tests at 3 months, did not have tests run at 6 months, and tested negative at 9 months, we wanted to obtain the test results at 6 months. The initial window to observe seroreversion would be 6 months (3 months to 9 months) while the second window with the new sample would be a shorter observation window of 3 months (3 months to 6 months).Of the 53 study visits in which Unigold was conducted but Determine was not, we obtained 14 Determine results. Of the 152 times in which Determine was collected and Unigold was not, we obtained 2 results. Of the times when both Determine and Unigold was missing, we obtained 55 Determine results and 62 Unigold results.
2. Investigate a sample of discordant rapid test results.
the two laboratory managers and the other reviewer that these faint results should be considered positive, per Unigold manufacturer instructions.
3. Investigate questionable test results.
There were occasions where an infant had a 6 negative test but had a 9 month positive rapid test. This would seem like a seroconversion but was not classified as one by study investigators throughout the follow-up period. We reran these tests at 6 months and found one to be positive and one to be negative.
Table 6. Summary of UNC rapid testing
After this first round of retesting, we received funding from the University of North Carolina Center for AIDS Research to test all available samples needed. This resulted in a total of 492 Determine and 504 Unigold tests conducted. We compared the population with missing data versus complete data, by timepoint and by test, for characteristics including infant factors (gender, breastfeeding, nevirapine at birth) and maternal factors (maternal age, marital status, education level, and socioeconomic variables). (see Appendix A). There were no factors consistently different between the two populations. We therefore concluded the missing data population was similar to the complete case population and proceeded with the missing data population for analyses.
Reason for retesting DT UN
Missing both DT and UN results 55 62
Missing DT results 14 0
Missing UN results 0 2
34
Table 7. Description of collected or missing rapid test data throughout follow-up, stratified by type of rapid test.
3m 6m 9m 12m 15m 18m Total
Collection site
DT UN DT UN DT UN DT UN DT UN DT UN DT UN
Malawi 1 1 66 66 63 62 52 52 56 56 57 57 295 294
UNC 75 76 31 39 29 29 35 38 20 17 7 11 197 210
Total 76 77 97 105 92 91 87 90 76 73 64 68 492 504
Total missing
45 (37%)
44 (36%)
25 (20%)
16 (13%)
29 (24%)
30 (25%)
34 (28%)
31 (26%)
45 (37%)
48 (40%)
57 (47%)
53 (44%)
234 (32%)
222 (31%)
CHAPTER 4: METHODS
4.1 Specific Aim 1
4.1.1 Study Sample and Data Collection
We collected data on the performance of Unigold® and Determine® rapid tests as part of a community-based cohort study examining the effects of HIV on neurodevelopment in infants receiving care at two healthcare centers in the Blantyre region of Malawi between May 2008 and March 2012. During that period, both clinics provided HIV counseling and testing to all pregnant women and offered single dose nevirapine or zidovudine treatment to women who were HIV infected. The study included infants born to HIV-positive mothers (age ≥ 15 years) who did not have a history of alcohol or drug abuse or chronic illness other than AIDS. For the analysis presented here, only children who were negative by HIV DNA PCR at the time of enrollment were included.
HIV DNA PCR testing using version 1.5 of the Amplicor HIV-1 DNA test kit (Roche, Basel, Switzerland) was performed at enrollment, which took place at approximately 6 weeks of age (median age 6.4 weeks, interquartile range [IQR] 4.3-15.1 weeks). Children were scheduled to visit the study clinic at age 10 weeks and every 3 months between age 14 weeks and 18 months. At all timepoints, clinical and sociodemographic information were collected, a fingerprick was performed for hemoglobin testing, dried blood spots were collected for storage for HIV DNA PCR assays, and a venous whole blood sample was taken for storage at ≤ -70 degrees Celsius. Confirmation of infant HIV infection detected by a
positive HIV DNA PCR result was done through a second HIV DNA PCR assay or a HIV RNA viral load assay.
collected at age 3 months. If data were missing at other timepoints due to failure to perform the rapid test at point-of-care or assay stock outs, rapid HIV tests were also performed on stored blood when available. Rapid testing on stored blood was conducted at a research laboratory at the University of North Carolina. Stored samples were thawed per manufacturer’s instructions, and both rapid tests were performed
simultaneously by a single operator. Weakly positive rapid tests results were reported as positive. The University of Malawi College of Medicine Research and Ethics Committee and the
University of North Carolina at Chapel Hill Institutional Review Board approved the study protocol. All mothers provided written informed consent and permission for participation of their infant.
4.1.2 Statistical Analysis
The 18-month cumulative incidence of infant HIV infection was estimated using an extension of the Kaplan-Meier estimator that allows for competing risks of death or loss to follow-up132 Sensitivity and specificity were estimated in a cross-sectional manner at each timepoint (3, 6, 9, 12, 15 and 18 months), separately for Determine and Unigold. A two-week window around each timepoint was used to define a visit. Data occurring outside of the two-week window were discarded. Sensitivity for each rapid test was estimated by the proportion of infants diagnosed as HIV infected by the rapid test among all infants with confirmed infection (by PCR) at the timepoint of interest. Specificity for each rapid test was estimated by the proportion of infants diagnosed as HIV negative by the rapid test among all infants with confirmed free of HIV infection (by PCR) at the timepoint of interest.
The positive predictive value (PPV) was estimated by the proportion of infants with confirmed HIV infection among all infants who tested positive on the rapid test. The negative predictive value (NPV) was estimated by the proportion of infants free of HIV infection among all infants who tested negative on the rapid tests. PPV and NPV were determined for a range of population infant HIV