Amiodarone
Therapy
Effects
on Childhood
Thyroid
Function
D. CoIm Costigan, MB, BCh, FRCP(C),
F. John Holland, MB, BCh, MRCP, FRCP(C),
Denis
Daneman,
MB, BCh, FRCP(C), Peter S. Hesslein, MD,Michael Vogel, MD, and Graham Ellis, PhD, MRC Path
From the Divisions of Endocrinology and Cardiology, Departments of Pediatrics and Clinical Chemistry, The Hospital for Sick Children, University of Toronto School of Medicine, Toronto
ABSTRACT. Thyroid function was systematically
evalu-ated in 15 consecutive children (mean age 13.7 years, range 0.5 to 19.5 years) before and serially during
treat-ment with amiodarone (Cordarone), a potent
antiar-rhythmic agent. Amiodarone is known to affect thyroid homeostasis by competitive inhibition of
5’-monodeio-dinase, which converts L-thyroxine (T4) to triiodothyro-nine (T3) and reverse T3 (rT3) to 3,3’-diodothyronine
(T2), and also by the direct effects of its high iodine
content (37% by weight). Clinical and/or biochemical evidence of hypothyroidism occurred in three patients,
two of whom required treatment with L-thyroxine. An
additional patient had persistent hyperthyroxinemia but
no clinical evidence of hyperthyroidism. Results from the
patients who remained euthyroid showed characteristic alterations in serum thyroid function tests. These in-cluded significant increases in serum T4, rT3, basal thy-roid-stimulating hormone and thyroid-stimulating hor-mone response to thyrotropin-releasing hormone testing. These changes were considered to be compensatory ad-justments by the pituitary-thyroid axis to competitive inhibition of5’-monodeiodinase by the amiodarone.
Rou-tine screening of thyroid function is needed to allow early
detection of hypothyroidism when these compensations fail to occur. Pediatrics 1986;77:703-708; arrziodarone, thyroid function.
Amiodarone hydrochloride, is a khellin derivative recently introduced to North America.’ It is a
p0-tent antiarrhythmic agent both in adults and
chil-dren.2’3 Amiodarone has a chemical structure
simi-Received for publication April 12, 1985; accepted July 12, 1985. Presented, in part, at the VIIth International Congress of En-docrinology, Quebec City, Canada, June 1984.
Reprint requests to (F.J.H.) The Hospital for Sick Children, 555 University Aye, Toronto, Canada M50 1X8.
PEDIATRICS (ISSN 0031 4005). Copyright © 1986 by the
American Academy of Pediatrics.
lar to L-thyroxine (Fig 1) and contains 37% organic iodine by weight. The high content of iodine alone (400 mg of amiodarone contains 150 mg of iodine,
equivalent to 24 drops of Lugol’s iodine) may cause
either hypo- or hyperthyroidism in certain
suscep-tible individuals.4’5 In addition amiodarone acts as
a competitive inhibitor of5’-monodeiodinase which
catalyzes the conversion of L-thyroxine (T4) to tn-iodothynonine (T3) and the conversion of the
mac-tive reverse tniiodothyronine (nT3) to 3,3’-diodo-thynonine (T2).6’7
Interference with normal thyroid hormone
ho-meostasis may profoundly affect young children
during critical stages of brain and somatic devel-opment. Therefore, we have evaluated thyroid func-tion, growth, and development in all children
treated with amiodarone since its introduction to
the Hospital for Sick Children, Toronto, in July 1981.
PATIENTS AND METHODS
All children (nine boys and six girls) who received
amiodarone HC1 (Cordarone) had life-threatening cardiac arrhythmias that were refractory to or un-suitable for other modes oftherapy (Table 1). Their
ages ranged from 0.5 to 19.5 years with a mean of
13.7 years. Eight patients had complex congenital
heart disease and seven had structurally normal
hearts. The focus of the arrhythmia was atnial in
six, ventricular in four, or combined in five patients. Six patients had previously required one or more direct current cardioversions.
amiodarone. Pituitary-thyroid function was
as-sessed prior to starting amiodarone therapy, at 1
and 3 months, and every 3 months thereafter. This was done by complete physical examination and by measurement of serum T4, thyroid-stimulating hor-mone (TSH), T3, T3 resin uptake (T3RU), and rT3.
A
thyroid-releasing hormone (TRH) stimulationtest (TRH 200 tg/1.73 m2 ofbody surface area) was
performed before amiodarone treatment was
started, at 3 months after, and then every 6 months for the duration of the study. Thyroid antibodies (antimicrosomal, antithyroglobulin) were measured
Amiodarone QJCO_(OCCHN5 4H9 Thyroxine FF4) L I ,NH2 COOH CM \\ \1I NM
HO_<)_O_(_CH2_CH CM-CH ,NH
COOH COOH
3,5,3-Trilodothyronine 3,3’,5’.Triiodothyronine
cr3). ., N,1
/“
(reverse T3)I I
HOQ- O-()- CM2-CH ,NH2
COOH 3,3’-Diiodothyronine
(T2)
Fig 1. Structural similarity of amiodarone to thyroid
hormone (T4) and its metabolites.
before the start of amiodarone therapy. Standard
commercial radioimmunoassay kits were used to measure serum T4, T3RU, T3, rT3, and TSH. The
ranges of normal values established for children in
this laboratory are: T4, 65 to 165 nmol/L (5.0 to 12.8 ig/dL); T3RU, 0.25 to 0.35 tg/dL; T3, 1.4 to
3.4 nmol/L (90 to 220 ng/dL); TSH, <10 mULL; max TSH post-TRH, <30 mU/L.
RESULTS
Amiodarone Requirements and Cardiac
Responses
Amiodarone dosage varied depending on the
types, persistence, and severity of the arrhythmia
and body size. The mean (±SEM) loading dose for the older children 6 to 19.5 years of age was 16.3 ± 1.7 mg/kg/d and the maintenance dose was 7.5 ±
1.2 mg/kg/d. Because of persistent dysrrhythmias
the three youngest patients (0.5, 0.9, and 4.9 years of age) required higher loading (39.2 to 63.2 mg/kg! d) and maintenance (9.8 to 27.4 mg/kg/d) dosages.
Thirteen patients had a satisfactory response to
amiodarone: there was a prompt abolition of the
arrhythmia in eight, and delayed abolition or
im-proved control occurred in five. Two patients had to discontinue the drug, one because of ventricular fibrillation, which developed during treatment of atrial flutter, and one because of a transient rash.
Two patients died during treatment due to the underlying cardiac disease. Three patients have
been able to discontinue amiodarone therapy, two
after 1 month and one after 11.5 months. The
TABLE 1. Clinical Data of Childr en Recei ving Amiodarone Hydroch bride Therapy*
Patient
No.
Age at Onset of
Treatment (yr)
Sex Diagnosis Duration of
Treatment 1 2t 3t 4 5 6 7 8t 9 10 11:1: 12 13 14 15 7.5 0.9 12.8 4.9 0.5 6.4 13.7 17.4 19.6 14 15.9 15 14.2 18.3 14.4 M F M F M F M F M
M
M M F F M TGA,aI vtSingle ventricle, a!
TOF,svt
Myocarditis EFE, svt
TGA,af
TGA,
svt, vt svtWPW,svt
Cardiomyopathy, vt
TGA, svt, a1 vt
TAPV,svt DORy, vt Cardiomyopathy, vt 42mo 11.5 mo 41 mo imo 1mo 21 mo 4d 32 mo 3Omo 28mo 1.5 mo 6 mo 22mo 19 mo 6 mo
a Abbreviations used are: TGA, transposition ofthe great arteries; WPW,
Wolf-Parkinson-White syndrome; TAPV, total anamolous pulmonary venous drainage; DORV, double outlet right ventricle; TOF, tetralogy of Fallot; EFE, endocardial fibroelastosis; af, atrial
flutter, vt, ventricular tachycardia; svt, supraventricular tachycardia. t Hypothyroidism developed.
Asymptomatic com-pensated
hypothy-roidism
No therapy
Asymptomatic corn-pensated hypothy-roidism
L-Thyroxine 75 ig/d
Normalized remainder have been on amiodarone for periods of
6 to 42 months.
Thyroid Evaluation
All but one patient (patient 9, Table 1) had
normal thyroid hormone concentrations prior to starting amiodarone therapy. Patient 9 had a lower serum T3 concentration (0.31 nmol/L) but normal T4 and TSH. The T3 returned to normal with improvement in his clinical status (“euthyroid sick
syndrome”).7 Two patients (No. 8 and No. 10) had
positive thyroid antimicrosomal and
antithyroglob-ulin antibody titers.
During amiodarone therapy, in two children (No.
2 and No. 8) primary hypothyroidism developed, necessitating L-thyroxine replacement, and in a third (No. 3) mild compensated hypothyroidism
(T4, 75 nmol/L, TSH 12.1 mU/L) (Table 2). An illustrative case history is presented below.
Patient 2
A 10-month-old girl presented with congestive cardiac failure and a tachyarrhythmia. She had a normal
pen-natal and developmental history. Her ECG showed
yen-tnicular tachycardia with intermittent sinus capture. This arrhythmia was refractory to treatment with lidocaine, procainamide, and propranolol. Electrophysiologic stud-ies during cardiac catheterization revealed an automatic ectopic focus in the left ventricle of a structurally normal heart. Loading doses of amiodarone (54.8 mg/kg) for seven days and phenytoin treatment terminated the yen-tricular tachycardia. Despite serum phenytoin levels
within the therapeutic range, reduction of the dosage of
amiodarone below 27 mg/kg/d led to recurrence of the
ventricular tachycardia. Her pre-amiodarone T4 was 73.4
nmol/L and TSH 2.4 mU/L. Test results for thyroid
antibodies were negative. Initially, her thyroid function
was monitored with only serial T4 and T3RU estimations. T4 was 122 and 92.6 nmol/L at 2 and 6 weeks, respec-tively. After 18 weeks of therapy, no developmental ad-vancement in speech or motor skills had occurred. On
examination, there was neither a palpable goiter nor somatic features of hypothyroidism. Serum T4 was 50
nmol/L (normal, 65 to 165 nmol/L), TSH was 53.9 mU/
L,
and T3 was 2.2 nmol/L. Bone age was normal. A week later, she exhibited phenytoin toxicity. Her serum T3 had decreased to 1.1 nmol/L, and her serum rT3 was 1,488 g/dL. Twenty-four-hour cardiac monitoring docu-mented continuous sinus rhythm for the first time sincediagnosis. Phenytoin treatment was discontinued, and
serum levels were undetectable within four days. Four days later, ventricular tachycardia returned but again reverted to bigeminy on the reintroduction of phenytoin. Formal psychologic testing confirmed the 3- to 4-month delay in overall development (Griffith’s mental
develop-ment scale, general quotient 82). She was begun on L-thyroxine therapy, 50 zg/d, and the dosage was increased very slowly in increments of 12.5 g to a maximum of 75
ig/d (10 tg/kg) when her TSH response to TRH returned to normal (mar TSH, 21.2 mULL). At that time, her
serum thyroxine level was 92 nmol/L, T3 was 1.7 nmol/
L, and TSH was 2.7 mUlL. Developmental catch-up was documented during the following 6 months by repeat
psychologic assessment (Griffith’s general quotient 98). Sinus rhythm returned, and her antiarrhythmic drugs were sequentially discontinued without incident after
11.5 months of therapy. L-Thyroxine was withdrawn gradually during the subsequent 2 months. Eighteen
TABLE 2.
Three Patients in Whom Hypothyroidism Developed During Amiodarone TherapyPatient No. 2 3 8
Sex F M F
Age (yr) 0.9 12.8 17.4
Thyroid function at start of Normal Normal Normal
treatment
Thyroid antibodies Negative Negative Positive
At development of hypothyroidism
Duration of treatment (mo) 5 8 3
Thyroxine (normal 65-165 50 75 72.1
nmol/L)
Thyroid-stimulating hormone 53.9 12.1 39
(normal <10 mU/L)
Mar
Thyroid-stimulating 38.5hormone (normal <30 mUlL)
Tniidothyronine (normal 1.4-3.4 2.2 2.4 1.6
nmol/L)
Reverse triidothyronine 1,488 750 420
(normal 80-250 g/L)
Comments Clinical hypothyroidism,
with developmental
delay
L-Thyroxme 75 ig/d
Clinically and biochemi-cally normalized
160-SERUM
120-THYROXINE nMolIL
80-
40-3.5.
3.0 SERUM
T3nMol/L 2.5
2.0
1.5#{149}
SERUM
REVERSE
T, iig/L
SERUM T.S.H. mUJL
600
500
400
300-200.
100-
A-
30-::
I ***
5-months later, she remains clinically and biochemically euthryoid.
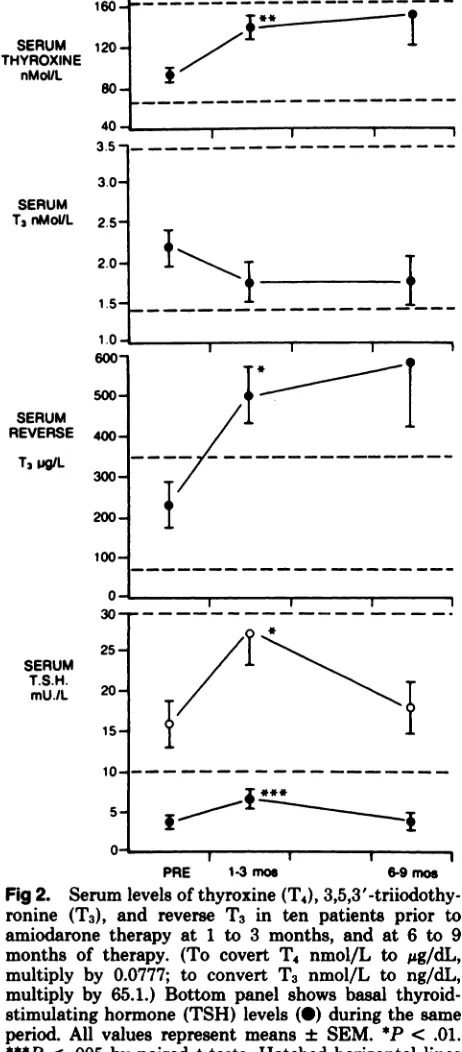
The 10 patients who remained euthyroid had normal growth and development with no clinical evidence of thyromegaly. The results of serial thy-roid function testing are shown in Fig 2. Within the first 3 months of starting amiodarone therapy, there was a significant increase in serum concen-trations of T4, rT3, TSH, and zmax TSH
post--
I I IK1
‘.v. . I I
--
I I IU. , I I
PRE 1-3rnoe 6-9moe
Fig 2. Serum levels of thyroxine (T4), 3,5,3’-tniiodothy-ronine (T3), and reverse T3 in ten patients prior to amiodarone therapy at 1 to 3 months, and at 6 to 9
months of therapy. (To covert T4 nmol/L to &g/dL,
multiply by 0.0777; to convert T3 nmol/L to ng/dL, multiply by 65.1.) Bottom panel shows basal thyroid-stimulating hormone (TSH) levels (#{149})during the same period. All values represent means ± SEM. *P < .01.
***P < .005 by paired t tests. Hatched horizontal lines indicate upper and lower range of normal for each test
(see text).
TRH
(P
< .01, .02, .05, and .05, respectively). T3 levels decreased but this change did not reach sta-tistical significance. These changes persisted during 6 or more months of amiodarone therapy. Occa-sional serum T4 levels were above normal. Onepatient (No. 6) had serum T4 concentrations (158
to 226 nmol/L) repeatedly above our normal range (65 to 165 nmol/L). She had no symptoms sugges-tive of hyperthyroidism, and her mean basal and
max TSH post-TRH were 3.5 and 21.4 mU/L,
respectively.
In the three patients in whom amiodarone treat-ment was discontinued (including patient 2), thy-roid function reverted to normal.
DISCUSSION
Amiodarone, a class III antiarrhythmic agent, is
being used increasingly in children with a wide
range of cardiac rhythm disorders. It prolongs the
duration of the action potential of all cardiac tissue by an as yet unknown mechanism.1 Our study is the first to assess prospectively the specific effects of amiodarone on thyroid function in children. We observed hypothyroidism in three of 15 patients #{149}1(20%), an incidence similar to the 22% incidence recently reported in amiodarone-treated adults also living in iodine-sufficient areas.5 We did not ob-serve hyperthyroidism, but one child had persistent asymptomatic hyperthyroxinemia. This latter ef-fect of the drug may have been mistaken for true
hyperthyroidism in earlier studies.8
The elevated serum T4, rT3, and TSH levels that we observed in the majority of our patients (10/13) during the first 3 months of amiodarone therapy #{149}1 are similar to the elevations seen both in adult
volunteers and patients.6’9’1#{176} These changes are thought to result primarily from amiodarone’s abil-ity to inhibit competitively the 5’-monodeiodinase enzyme in both of its allelic forms, thus inhibiting the conversion of T4 to T3 both peripherally (type
I)
and within the CNS (type II).5.6 The liver and kidney are responsible for peripheral conversion of plasma T4 to T3. However, in the CNS, this con-version (type II) is intracellular, and T3 so produced contributes much more than plasma T3 to the in-teraction with the nuclear T3 receptors, which is the final pathway of the thyroid hormone ef-fect.1#{176}’2Amiodarone’s inhibition of 5’-monodeio-dinase (type II) within the pituitary thyrotropes reduces intrapituitary T3 and results in increased TSH secretion and increased responsiveness toTRH. The normal thyroid responds to TSH by
we found the greatest increases in serum rT3 levels, as a result of increased diversion of T4 down this catabolic pathway (Fig 2). These findings persisted for the duration of treatment, supporting the find-ings of Martino et al.5 However, some previous data have suggested that such changes may be transient.6
The mechanism of amiodarone-induced hypothy-roidism is uncertain; the large iodine load may itself induce hypothyroidism in certain individuals.4 In normal individuals, the initial response to increased thyroid cell content of iodine is a direct suppression of thyroid hormone secretion (Wolff-Chaikoff ef-fect). Continued iodine administration (seven to 14 days) is accompanied by an autoregulatory decrease in iodine uptake by the thyroid cells, which allows thyroid hormone secretion to resume. However, continued suppression (iodine-induced hypothy-roidism) occurs in some individuals.4 Amiodarone,
by elevating serum TSH, may predispose to this
condition by continuing to stimulate iodine uptake.
Another risk factor for amiodarone-induced hy-pothyroidism is thyroiditis. In one series, as many as 50% of adult patients in whom this complication
developed had elevated antithyroid antibodies.’3
Patient 8 may illustrate the latter mechanism;
whereas, in patient 2, the very large iodine load due to a high dose of amiodarone was probably of prime
importance. Amiodarone withdrawal is effective in
reversing the hypothyroidism, but this is usually contraindicated becasuse of the serious cardiac sta-tus. We believe that treatment with T3 is not ad-visable because potentially acute elevations in serum T3 concentrations may aggravate cardiac function.” L-Thyroxine is, therefore, the treatment of choice.
In patient 2, amiodarone-induced
hypothyroid-ism presented with a 3-month history of
develop-mental arrest, in spite of a normal serum T3 level and without other somatic manifestations. We speculate that amiodarone, by inhibiting 5’-mono-deiodinase in the cerebral cortex of this child, may have accentuated this component of her hypothy-roidism. In the cerebral cortical cells of the euthy-roid rat, 75% of thyroid hormone action is depend-ent upon T3 that is derived locally from T4.’2”4 The activity of this enzyme increases in response to a declining nuclear T3 concentration, thus affording some CNS protection during development of hy-pothyroidism. Amiodarone, by its direct inhibition of this enzyme, may diminish this protection. Al-though chronic illness could have contributed to a decline in serum levels of T4, this child was clini-cally well with sinus rhythm and no congestive heart failure when hypothyroidism was first noted. Furthermore, prior to amiodarone therapy, when she was gravely ill, thyroid function was normal. It
is also unlikely that phenytoin treatment had a
significant impact on thyroxine metabolism be-cause its most prominent effects concern competi-tion for thyroxine-binding globulin and increased T4 to T3 conversion.7 In our patient, T3 resin uptake and serum T3 concentrations remained within the normal range, yet TSH levels became significantly elevated, findings inconsistent with the known
ac-tions of phenytoin.
In summary, we found that amiodarone treat-ment of cardiac arrhythmias in children is associ-ated with predictable responses in indices of pitui-tary-thyroid function that are similar to those re-ported in adults.6’9”#{176}Although the incidence of hy-pothyroidism in our study (20%) is similar to that recently reported in adults from similar iodine-sufficient areas,5 it is several-fold higher than that reported initially in amiodarone-treated children and adults.2’3 Our study is also in contrast to
pre-vious reports of a relatively higher prevalence of
hyperthyroidism than hypothyroidism.6’9”#{176} We rec-ommend thyroid function testing before and
seri-ally during amiodarone therapy. An increasing
serum TSH concentration in association with an unchanged or decreasing T4 concentration is a warning sign of possible thyroid decompensation. Careful follow-up of children on amiodarone treat-ment should detect thyroid decompensation before clinical symptoms supervene. This is particularly important in children younger than 1 year of age, during the period of rapid brain growth, in whom the initial symptoms may be due to cerebral cortical deficiency of T3. Frequency of monitoring should be greatest in this age group, but all amiodarone-treated patients should have T4, TSH, and T3 mea-sured often during the first year of treatment and subsequently as part of routine cardiologic assess-ment. If hypothyroidism occurs, L-thyroxine ther-apy should be introduced until such time as the amiodarone can be safely discontinued.
ACKNOWLEDGMENTS
We thank Pam Goodwin for secretarial assistance and the Fellows in the endocrine division for assistance in
investigation of these patients.
ADDENDUM
Since completing this study, we have treated an
addi-tional ten patients with amiodarone; in two
hypothyroid-ism has developed. The incidence of hypothyroidism
re-mains 20% (five of 25).
REFERENCES
2. Rosenbaum MB: Clinical efficacy of amiodarone as an
an-tiarrhythmic agent. Am J Cardiol 1976;38:934-944
3. Coumel P, Fidelle J: Amiodarone in the treatment of cardiac
arrhythmias in children: One hundred thirty-five cases. Am
Heart J 1980;100:1063-1069
4. Ingbar SH, Woeber KA. The thyroid gland, in Williams RH (ad): Textbook of Endocrinology. Philadelphia, WB
Saun-ders, 1981, pp 138-139
5. Martino E, Safran M, Aghini-Lombardi F, et al:
Environ-mental iodine intake and thyroid dysfunction during chronic
amiodarone therapy. Ann Intern Med 1984;101:28-34 6. Melmed 5, Nademanee K, Reed AW, et al:
Hyperthyroxi-nemia with bradycardia and normal thyrotropin secretion
after chronic amiodarone administration. J Clin Endocrinol
Metab 1981;53:997-1001
7. Wartofsky L, Burman KD: Alterations in thyroid function
in patients with systemic illness: The “euthyroid sick
syn-drome.” Endocr Rev 1982;3:164-215
8. Jonckheer MH, Blockx P, Broeckaert I, et al: “Low T3
syndrome” in patients chronically treated with an
iodine-containing drug, amiodarone. Clin Endocrinol 1978;9:27-35
9. Burger A, Dinichert D, Nicod P, et al: Effect of amioda.rone on serum triiodothyronine, reverse triiodothyronine, thy-roxin, and thyrotropin. J Clin Invest 1976;58:255-259
10. Lambert MJ, Burger AG, Galazzi RL, et a!: Selective
in-creases in serum thyroxine (T4) due to iodinated inhibitors
of T4 monodeiodination indicative of hyperthyroidism. J Clin Endocrinol Metal, 1982;55:1058-1065
11. Larsen PR: Thyroid-pituitary interaction. New Engi J Med 1982;306:23-32
12. Larsen PR, Silva JE, Kaplan MM, et al: Thyroid hormone
metabolism in the brain. Proceedings of 7th International
Congress of Endocrinology, 1984, p 159
13. Chevigne-Brancart M, Vandalem JL: Thyroid function dun-ing and after amiodarone therapy, abstract no. 128.
Endo-crinology 1982;64:111
14. Crantz FR, Silva JE, Larsen PR: An analysis of sources and quantity of 3,5,3’-triiodothyronine specially bound to flu-clear receptors in rat cerebral cortex and cerebellum. En-docrinology 1982;110:367-375
SELECTIONIST ThEORY OF MENTAL DEVELOPMENT
Changeux argues that an unstimulated nervous system makes very large
numbers of random multiple connections which remain labile for various periods of time. Experience, i.e., stimulation of the nervous system, in this view, causes differential elimination of various of these multiple connections, leaving in place only those that form a coherent structure. In the absence of stimulation, random death of cells and rupture of connections will leave the pathways in a permanent state of disarray. That is why we can learn to speak only if we hear others speak, and why after a certain age such learning is impossible, as in the case of “wild children” who never acquire language. The analogy is to a photographic image in which certain silver grains are fixed by exposure to light, the remainder being washed out in the development process ...
Submitted by Student
From Lewontin RC: Darwin, Mendel and the Mind (Book Review of Changeux J-P. Neuronal Man: