ARTICLE
Follow-up of a Randomized, Placebo-Controlled Trial
of Dexamethasone to Decrease the Duration of
Ventilator Dependency in Very Low Birth Weight
Infants: Neurodevelopmental Outcomes at 4 to 11
Years of Age
T. Michael O’Shea, MD, MPHa, Lisa K. Washburn, MDa, Patricia A. Nixon, PhDa,b, Donald J. Goldstein, PhDa
aDepartment of Pediatrics, School of Medicine, andbDepartment of Health and Exercise Science, Wake Forest University, Winston-Salem, North Carolina
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.High doses of dexamethasone reduce the risk of chronic lung disease
among premature infants but may increase the risk of developmental impair-ments. The objective of this study was to compare developmental outcomes beyond infancy for children who, as neonates, participated in a randomized trial of dexamethasone.
PATIENTS AND METHODS.One hundred eighteen children with birth weights ⬍1500 g
were randomly assigned at 15 to 25 days of life to a 42-day tapering course of dexamethasone or placebo. All 95 survivors were assessed by using standardized measures of developmental outcome at least once at or beyond 1 year of age, and 84 were examined at 4 to 11 years. For this follow-up study, the outcome of primary interest was death or major neurodevelopmental impairment, which was defined as cerebral palsy, cognitive impairment, or blindness.
RESULTS.On the basis of each child’s most recent follow-up, the rates of major
neurodevelopmental impairments were 40% for the dexamethasone group and 20% for the placebo group. The higher impairment rate for the dexamethasone group was mainly attributed to a higher prevalence of cerebral palsy. Rates of the composite outcome of death or major neurodevelopmental impairment were 47% and 41%, respectively.
CONCLUSION.A 42-day tapering course of dexamethasone, which was shown
previ-ously to decrease the risk of chronic lung disease in very low birth weight infants, does not increase the risk of the composite outcome of death or major neurode-velopmental impairment.
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-0486
doi:10.1542/peds.2007-0486
Key Words
bronchopulmonary dysplasia, chronic lung disease, dexamethasone, glucocorticoids
Abbreviations CLD— chronic lung disease DAS—Differential Abilities Scales VABS—Vineland Adaptive Behavioral Scales
WISC-III—Wechsler Intelligence Scale for Children, 3rd Edition
MDI—Mental Developmental Index OR— odds ratio
CI— confidence interval
Accepted for publication Jun 4, 2007
Address correspondence to T. Michael O’Shea, MD, MPH, Department of Pediatrics, Wake Forest University School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157. E-mail: [email protected]
G
LUCOCORTICOIDS HAVE BEENused for⬎30 years to treat premature infants with respiratory disease in an effort to decrease duration of ventilator dependency and risk of chronic lung disease (CLD).1One widely usedglucocorticoid, dexamethasone, improves pulmonary mechanics2–4 but has been associated with both acute
adverse effects, such as increased blood pressure5–7 and
slowing of growth,8–10 and long-term effects, such as
neurodevelopmental impairment.11,12 In view of these
risks, the American Academy of Pediatrics and Canadian Paediatric Society have advised against the use of post-natal steroids except in randomized trials or for the treatment of infants on maximal ventilatory and oxygen support.13
The evidence on which recommendations against postnatal steroids are based is limited by the high rates of contamination (treatment of infants randomly assigned to placebo with open-label steroids) in almost all trials5–7
and the small number of trial participants who have been studied beyond the neonatal period.11 Doses of
dexamethasone that have been associated with an in-creased risk of neurodevelopmental impairment are sev-eral-fold that which recently was shown to have bene-ficial effects on the lung.8 A recent meta-analysis14
suggested that the beneficial effects of dexamethasone outweigh the risk among infants at high risk (⬎55%) of CLD.
The objective of this study was to study the effect of dexamethasone on neurodevelopmental outcomes be-yond infancy on the basis of data collected on partici-pants in a randomized trial of a 42-day tapering course of dexamethasone.15
METHODS
This research was approved by the institutional review boards of Wake Forest University Health Sciences and Forsyth Medical Center.
Study Participants
The children who participated in this study were, as neonates, enrolled in a randomized placebo-controlled trial of a 42-day tapering course of dexamethasone, as reported previously.15 The infants were enrolled
be-tween April 1992 and May 1995 and met the following criteria: (1) birth weight of⬍1501 g; (2) age between 15 and 25 days; (3)⬍10% decrease in ventilator settings for the previous 24 hours and fraction of inspired oxygen
ⱖ0.3; (4) no clinical signs of sepsis; and (5) echocardi-ography results that indicate the absence of a patent ductus arteriosus. The rate of contamination (ie, treat-ment with dexamethasone of patients who were ran-domly assigned to placebo) was zero. The effects of dexa-methasone on the duration of ventilator dependency and developmental outcomes at an adjusted age of 1 year have been reported.15,16When surviving study
par-ticipants were 4 to 6 years of age, and again when they
were 8 to 11 years of age, we attempted to schedule a follow-up assessment. Written informed consent was obtained from the parents before randomization and at the follow-up visits, and written assent was obtained from the children at 8 to 11 years of age.
Neonatal Data
Data from the neonatal period (eg, cranial ultrasound findings) were collected by a research nurse who re-viewed medical charts without knowledge of treatment-group assignment. CLD was defined as use of supple-mental oxygen at 36 weeks’ postmenstrual age.17Small
for gestational age was defined as birth weight less than the gender-specific 10th percentile for gestational age.18
Cranial ultrasounds were obtained at least once, be-tween 7 and 14 days of life, and most infants had at least 1 additional ultrasound examination before discharge. A major cranial ultrasound abnormality was defined as (1) subependymal or intraventricular hemorrhage with post-hemorrhagic hydrocephalus requiring placement of a shunt, (2) persistent but nonprogressive ventricular di-latation, or (3) intraparenchymal echodensity or echolu-cency in the periventricular white matter on the basis of the last ultrasound obtained during the neonatal hospi-talization.19,20
Cerebral Palsy
Data about developmental outcomes were collected pro-spectively at visits that occurred at an adjusted age of⬃1 year, 4 to 6 years of age, and 8 to 11 years of age. Parents, children, and follow-up examiners were not aware of the children’s randomization assignment. As described previously,16 cerebral palsy was diagnosed at
an adjusted age of 1 year if a child had abnormality of muscle tone and posture with impaired motor function on the basis of an examination performed by a develop-mental pediatrician or a neonatologist with experience in neurodevelopmental follow-up. Cerebral palsy was diagnosed at 4 to 6 years if the child had neuromotor abnormality on the basis of a neurologic examination by a nurse with specialized training in neurodevelopmental follow-up and the parent reported that the child was receiving therapies for cerebral palsy. The parent was interviewed again at the 8- to 11-year visit as to whether a diagnosis of cerebral palsy had ever been made.
Intelligence and Academic Achievement
At the 4- to 6-year visit, a child psychologist assessed the children by using the Differential Abilities Scales (DAS),21 the Kaufman Survey of Early Academic and
Language Skills,22and the Vineland Adaptive Behavioral
Scales (VABS).23At the 8- to 11-year visit, a child
psy-chologist assessed the children by using the Wechsler Individual Achievement Tests,24 the Wechsler
Intelli-gence Scale for Children, 3rd Edition (WISC-III),25 and
Definition of Major Neurodevelopmental Impairment
For 45 dexamethasone-treated children and 37 placebo-treated children who underwent intelligence testing at 4 to 6 and/or 8 to 11 years, a major neurodevelopmental impairment was defined as either cerebral palsy at 4 to 6 years of age or mental retardation at last follow-up. Mental retardation was defined as an IQ of⬍70 (on the DAS at 4 – 6 years or the WISC-III at 8 –11 years) and a VABS composite score of ⬍70.26For 5 dexamethasone
recipients and 6 placebo recipients, the diagnosis of men-tal retardation was based on testing at 4 to 6 years; for 40 dexamethasone recipients and 31 placebo recipients, this diagnosis was based on testing at 8 to 11 years. Five dexamethasone-treated and 8 placebo-treated children did not undergo intelligence testing. When comparing the 2 treatment groups with respect to the rate of major neurodevelopmental impairment, we performed analy-ses that both excluded and included those children who did not undergo intelligence testing. For the latter, we classified children who did not undergo intelligence test-ing as havtest-ing a major neurodevelopmental impairment if they were blind, had cerebral palsy at the most recent visit, or a Bayley Mental Developmental Index (MDI) of
⬍70 for adjusted age.
Data Analysis
Group comparisons were performed with the Wilcoxon rank-sum test for continuous variables. Exact P values for 2⫻2 contingency tables, odds ratios (ORs), and 95% confidence intervals (CIs) were computed by using StatXact (Cytel Software Corporation, Cambridge, MA). For all other analyses, SAS was used (SAS Institute, Inc, Cary, NC). APvalue of⬍.05 was used to define statis-tical significance.
Sample-Size Considerations
The sample size for the randomized trial from which this study was derived was selected to provide 80% power to detect what we considered was a clinically significant decrease in the duration of ventilator dependency. Given the frequency among placebo recipients of death or major developmental impairment observed by Yeh et al12 (35%), the sample size we selected (118 infants)
provided slightly more than 80% power to detect a halving or doubling of the risk of the composite outcome of death or major neurodevelopmental impairment among dexamethasone recipients.
RESULTS
Characteristics of the Children
Figure 1 is a participant-flow diagram. Ninety-five ran-domly assigned children survived to an adjusted age of 1 year, and all survivors were examined at least once at or beyond an adjusted age of 1 year. In Table 1, we sum-marize the sources of follow-up information that were
used to classify infants with respect to the presence or absence of cerebral palsy, cognitive impairment, and major developmental impairment. In Table 2, the at-tributes of 11 infants who were not seen after 1 year adjusted age are compared with those of the 84 infants who were seen after 1 year. Among survivors, a greater proportion of dexamethasone-treated children were ex-posed to antenatal steroids (P⫽.02), but no other group differences were statistically significant.
Cerebral Palsy
Among 78 children not classified as having cerebral palsy at an adjusted age of 1 year, 2 (1 dexamethasone and 1 placebo) were determined to have cerebral palsy at 4 to 6 years of age, 9 (2 dexamethasone and 7 placebo) were not examined after 1 year adjusted age, 61 (31 dexamethasone and 30 placebo) were classified as not having cerebral palsy when examined at 4 to 6 years of age, and an additional 6 children (2 dexamethasone and 4 placebo) were free from cerebral palsy at 8 to 11 years of age, based on parent report. One dexamethasone-treated child, who was previously reported as lost to follow-up16 and whose medical chart was subsequently
found, had been diagnosed with cerebral palsy at the 1-year follow-up. Among the 16 children (13 dexameth-asone and 3 placebo) who were classified at 1 year of age as having cerebral palsy, 15 continued to exhibit signs of cerebral palsy, based on examinations performed at a minimum of 30 months of age, but 1 dexamethasone-treated child did not. One dexamethasone-dexamethasone-treated child, who was not examined at 1 year adjusted age or 4 to 6 years of age but returned for follow-up at 10.3 years of age, was classified as not having cerebral palsy, based on parent report. Thus, at the most recent follow-up (as presented in Table 1), 13 of 50 dexamethasone-treated children had cerebral palsy (12 diagnosed at 1 year and 1 diagnosed at 4 – 6 years) compared with 4 of 45 place-bo-treated children (3 diagnosed at 1 year and 1 diag-nosed at 4 – 6 years) (OR: 3.6; 95% CI: 1.1–12.0; P ⫽
.03). This association is weaker if we exclude 15 children (4 dexamethasone and 11 placebo) who were free from cerebral palsy at 1 year but were not examined at 4 to 6 years and 1 child (dexamethasone-treated) who was seen only at 9 years (13 of 45 dexamethasone versus 4 of 34 placebo; OR: 3.0; 95% CI: 0.9 –10.4;P⫽.07).
had not undergone orthopedic surgery for cerebral palsy. Another child (dexamethasone recipient) was classified as having mild cerebral palsy at 1 year but had not been seen after that age. A fifth child with mild cerebral palsy at 1 year showed no signs of cerebral palsy at 4 to 6 years. Thus, at least 4, and possibly 5, dexa-methasone recipients could reasonably be classified as having mild cerebral palsy. Two of these children had mental retardation, but the other 3 had no major im-pairment other than cerebral palsy. Thirteen children (9 dexamethasone and 4 placebo) were classified as having moderate-to-severe cerebral palsy at 1 year and/or had a VABS motor subscale score of⬍55 (ie, 3 SDs below the mean) and/or have undergone orthopedic surgery for cerebral palsy. On this basis we regard them as having moderate-to-severe cerebral palsy.
Intelligence, Preacademic Skills, and Academic Achievement Testing
Intelligence testing was performed successfully on 82 of 84 study participants who returned for follow-up
eval-uation at 4 to 6 and/or 8 to 11 years of age. In each group 1 child who had significantly delayed mental develop-ment at 1 year of age would not cooperate for intelli-gence testing at 4 to 6 or 8 to 11 years. One placebo-treated child with severe visual impairment was tested only for verbal IQ. The results of intelligence and aca-demic achievement testing on the remaining 81 partic-ipants are presented in Tables 3 and 4. Although median scores for the majority of measures tended to be higher in the dexamethasone-treated children, no statistically significant treatment-group differences were found. At the latest follow-up, children in the dexamethasone-treated group had a median IQ of 90 (5th and 95th percentiles: 48 and 113), and those in the placebo group had a median IQ of 84 (5th and 95th percentiles: 44 and 111) (P ⫽ .5, Wilcoxon rank-sum test). Inclusion of information about the child who had only verbal IQ measured decreased the median IQ for the placebo-treated children to 83 (at latest follow-up). Among those children tested at 4 to 6 or 8 to 11 years, mental retar-dation was detected in 8 (18%) of 45
dexamethasone-FIGURE 1
treated children and 4 (11%) of 37 placebo-treated chil-dren (OR: 1.8; 95% CI: 0.5– 6.5). If the untestable children are classified as mentally retarded, an OR of 1.6 (95% CI: 0.5–5.3) is obtained.
Major Neurodevelopmental Impairment
Excluding the 13 children who did not undergo intelli-gence testing at either 4 to 6 or 8 to 11 years, the rates of major neurodevelopmental impairments were 36% (16 of 45) and 14% (5 of 37) in the dexamethasone and placebo groups, respectively (OR: 4.1; 95% CI: 1.3–12.5;
P ⫽ .01). Including all children, and based on each child’s most recent follow-up, the rates of major neuro-developmental impairments were 40% (20 of 50) and 20% (9 of 45) in the dexamethasone and placebo groups, respectively (OR: 2.7; 95% CI: 1.1– 6.7;P⫽.04). Similar proportions had cerebral palsy and cognitive im-pairment (dexamethasone: 8%; placebo: 7%), and sim-ilar proportions had cognitive impairment without cere-bral palsy (dexamethasone: 14%; placebo: 11%). Thus, the higher risk of neurodevelopmental impairment among the dexamethasone-treated children was attrib-utable largely to the greater proportion with cerebral palsy but without cognitive impairment (dexametha-sone: 18%; placebo: 2%). Rates of the composite
out-come of death or major neurodevelopmental impair-ment were 47% (27 of 57) and 41% (25 of 61), respectively (OR: 1.3; 95% CI: 0.6 –2.7;P⫽.5).
Adaptive Development
Table 5 summarizes the results of parent-reported adap-tive behavior. Within domains, median scores were sim-ilar at 4 to 6 and 8 to 11 years of age. Comparing the dexamethasone and placebo groups, no statistically sig-nificant results were found. The medians for both groups were ⬃1 SD below the mean in the normative sample (ie, 100).
DISCUSSION
The primary finding from this follow-up of the random-ized trial is that a 42-day course of dexamethasone, initiated in weeks 3 to 4 of life in very low birth weight infants, did not increase the rate of the composite out-come of death or major neurodevelopmental impair-ment. These findings are consistent with observations made on the study participants at 1 year adjusted age, when dexamethasone was associated with a higher rate of cerebral palsy but not a higher rate of the composite outcome of death or cerebral palsy.
When we initiated a randomized trial of dexametha-sone, we expected that by decreasing the risk of CLD, dexamethasone would also decrease the risk of adverse neurodevelopment outcomes. Despite finding that dexa-methasone reduced the risk of CLD15and improved
pul-monary function during childhood,27this treatment did
not improve neurodevelopmental outcome.16 These
findings are consistent with the results of all randomized trials of postnatal steroids, except one,28,29with regard to
the finding that dexamethasone reduces CLD risk5–7but
has no effect on neurodevelopmental outcome.11 It is
possible that dexamethasone has indirect beneficial ef-fect on neurodevelopmental outcome mediated by its salutary effect on the lung, which is offset by a direct detrimental effect on brain development. Dexametha-sone has been associated with reduced brain growth in animals30 and impaired head growth9,31 and neurologic
and cognitive impairment12,32in humans.
The inclusion criteria and the intervention used in the current study were based on an earlier trial by Cum-mings et al,28 and the follow-up of both trials did not
detect an adverse effect of dexamethasone on the com-posite outcome of death or major developmental impair-ment. Using a lower dose, begun at a mean age of 8 hours, Yeh et al12,33observed a decreased risk of CLD and
increased risk of the composite outcome of death or neurodevelopmental impairment. This disagreement among the 3 studies could be attributable to the more-than-twofold-higher risk of CLD among controls in our study15and that of Cummings et al,28as compared with
controls in the study by Yeh et al.12,33Our study provides
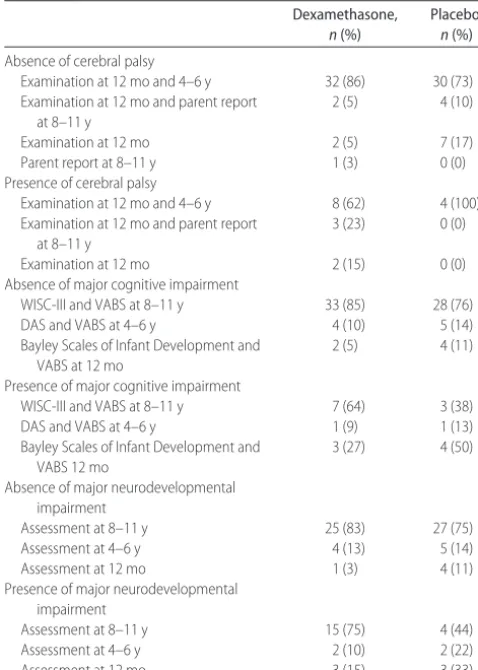
support for the conclusion of Doyle et al14that among TABLE 1 Sources of Follow-up Information
Dexamethasone, n(%)
Placebo, n(%)
Absence of cerebral palsy
Examination at 12 mo and 4–6 y 32 (86) 30 (73) Examination at 12 mo and parent report
at 8–11 y
2 (5) 4 (10)
Examination at 12 mo 2 (5) 7 (17)
Parent report at 8–11 y 1 (3) 0 (0)
Presence of cerebral palsy
Examination at 12 mo and 4–6 y 8 (62) 4 (100) Examination at 12 mo and parent report
at 8–11 y
3 (23) 0 (0)
Examination at 12 mo 2 (15) 0 (0)
Absence of major cognitive impairment
WISC-III and VABS at 8–11 y 33 (85) 28 (76)
DAS and VABS at 4–6 y 4 (10) 5 (14)
Bayley Scales of Infant Development and VABS at 12 mo
2 (5) 4 (11)
Presence of major cognitive impairment
WISC-III and VABS at 8–11 y 7 (64) 3 (38)
DAS and VABS at 4–6 y 1 (9) 1 (13)
Bayley Scales of Infant Development and VABS 12 mo
3 (27) 4 (50)
Absence of major neurodevelopmental impairment
Assessment at 8–11 y 25 (83) 27 (75)
Assessment at 4–6 y 4 (13) 5 (14)
Assessment at 12 mo 1 (3) 4 (11)
Presence of major neurodevelopmental impairment
Assessment at 8–11 y 15 (75) 4 (44)
Assessment at 4–6 y 2 (10) 2 (22)
infants whose baseline risk of CLD exceeds⬃55%, the beneficial effect of dexamethasone on neurodevelop-mental outcome (associated with CLD risk reduction) may outweigh the direct hazardous effect on brain de-velopment.
In studies by Romagnoli et al,34in which the rate of
CLD among controls was 68%, and the Collaborative Dexamethasone Trial Group,35 in which home oxygen
use was approximately one half of the rate of our con-trols, no difference was found in either mortality or neurodevelopmental impairment. However, in both
studies, a high rate (43% and 52%) of contamination (ie, treatment of infants randomly assigned to placebo with open-label steroids) could have attenuated group differences.
Several limitations of our study should be noted. Re-lated to the diagnosis of cerebral palsy, 9 trial partici-pants who were classified as not having cerebral palsy were examined only at 1 year adjusted age, when milder cerebral palsy might not have been detected. In addition, examinations at 4 to 6 years were performed by a nurse, rather than a pediatrician, and she may have failed to identify mild cases. Because the examiners were not aware of randomization assignment, we would expect underascertainment to be nondifferential with respect to randomization group, thereby attenuating associations between dexamethasone and the risk of cerebral palsy.36 TABLE 2 Randomly Assigned Trial Survivors Examined at 4 to 6 and/or 8 to 11 Years of Age and Those
Not Examined After 1 Year of Age
Attribute Examined at 4–11 y Not examined at 4–11 y
Dexamethasone (n⫽46)
Placebo (n⫽38)
Dexamethasone (n⫽4)
Placebo (n⫽7)
Birth weight, kg 758 (530–1050) 784 (515–1267) 730 (500–801) 760 (683–939) Gestational age, wk 25 (23–28) 26 (24–29) 25 (24–28) 25 (24–27)
Small for gestational age 4 (9) 4 (11) 1 (25) 0 (0)
White race 30 (65) 20 (53) 3 (75) 3 (43)
Male gender 21 (46) 19 (50) 3 (75) 4 (57)
Antenatal steroidsa 18 (39) 6 (16) 1 (25) 1 (14)
Home oxygen 13 (28) 16 (42) 1 (25) 5 (71)
Major CUS abnormalityb 9 (20) 5 (13) 1 (25) 0 (0)
Maternal educationc
Less than high school 9 (21) 6 (16) 1 (25) 3 (43)
High school 19 (45) 22 (58) 0 (0) 2 (29)
More than high school 14 (33) 10 (26) 3 (75) 2 (29)
Data are presented as median (5th–95th percentiles) or number of individuals with the attribute (group percentage in parentheses). All group comparisons were not statistically significant except as specifically noted. CUS indicates cranial ultrasound.
aDexamethasone recipients were more likely to have been exposed to antenatal steroids (P⫽.02).
bMajor abnormality on cranial ultrasound refers to posthemorrhagic hydrocephalus, persistent ventricular enlargement, or persistent intrapa-renchymal echodensity/echolucency.
cData about maternal education were missing for 4 dexamethasone-treated infants.
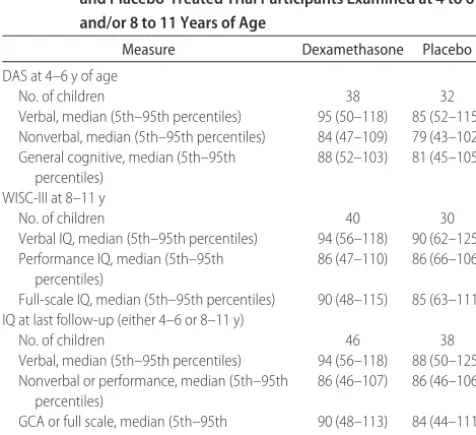
TABLE 3 Comparison of Intelligence Scores for Dexamethasone-and Placebo-Treated Trial Participants Examined at 4 to 6 and/or 8 to 11 Years of Age
Measure Dexamethasone Placebo
DAS at 4–6 y of age
No. of children 38 32
Verbal, median (5th–95th percentiles) 95 (50–118) 85 (52–115) Nonverbal, median (5th–95th percentiles) 84 (47–109) 79 (43–102) General cognitive, median (5th–95th
percentiles)
88 (52–103) 81 (45–105)
WISC-III at 8–11 y
No. of children 40 30
Verbal IQ, median (5th–95th percentiles) 94 (56–118) 90 (62–125) Performance IQ, median (5th–95th
percentiles)
86 (47–110) 86 (66–106)
Full-scale IQ, median (5th–95th percentiles) 90 (48–115) 85 (63–111) IQ at last follow-up (either 4–6 or 8–11 y)
No. of children 46 38
Verbal, median (5th–95th percentiles) 94 (56–118) 88 (50–125) Nonverbal or performance, median (5th–95th
percentiles)
86 (46–107) 86 (46–106)
GCA or full scale, median (5th–95th percentiles)
90 (48–113) 84 (44–111)
No group differences were statistically significant. GCA indicates general cognitive assessment.
TABLE 4 Comparison of Dexamethasone- and Placebo-Treated Trial
Participants for Preacademic Skills at 4 to 6 Years and Academic Skills at 8 to 11 Years
Measure Dexamethasone Placebo
K-SEALS at 4–6 y of age
Vocabulary 99 (58–113) 89 (55–110)
Numbers, letters, words 94 (69–122) 96 (55–111)
EALC 98 (60–121) 89 (52–106)
Expressive skills 97 (65–121) 91 (52–106) Receptive skills 97 (61–116) 90 (55–112)
Number skills 90 (72–112) 86 (55–100)
Letters and words 91 (74–133) 88 (55–105) WIAT at 8–11 y of age
Reading 97 (59–126) 92 (65–117)
Spelling 98 (64–120) 97 (67–118)
Math 92 (55–121) 92 (64–126)
A second limitation is that 15% of the trial partici-pants did not undergo cognitive testing. Most studies37–39
of the bias resulting from loss to follow-up among high-risk neonatal cohorts have suggested that the result of this bias is an underestimation of the rate of impairment. In the current study, the lost-to-follow-up rate was somewhat higher among placebo-treated children (16% vs 8%), and the resultant bias might account, at least to a small degree, for the somewhat lower rate of mental retardation in that group (11% vs 18%). On the other hand, all trial participants were evaluated at or beyond 1 year adjusted age; thus, the issue that may be more relevant than lost-to-follow-up bias is the degree to which an evaluation at 1 year adjusted age is a valid predictor of major neurodevelopmental impairment during childhood. In the current study 11 children were not seen after 1 year adjusted age. Four of them were judged to have a major impairment at 1 year (a blind child in each group and 2 children with cerebral palsy in the dexamethasone group). Our decision to classify the other 7 children as free from major neurodevelopmental impairment was based on their not having cerebral palsy, a Bayley MDI of⬍70, or blindness at 1 year and studies by Hack et al40 and Roth et al,41who examined
very preterm infants at both 12 to 20 months and at 8 years. In the former study,40only 3 of (2.7%) 112
chil-dren with a Bayley MDI in the reference range at 20 months were found to have an IQ of⬍70 at school age, and only 3 (1.8%) of 163 who were free from cerebral palsy at 20 months were classified as having cerebral palsy at school age. Roth et al41reported that 1 (0.6%) of
164 children who were free from a major impairment at 1 year of age were found to have a major impairment at 8 years of age.
A third limitation of our study is that the sample size was modest, which limits the statistical power to detect small effects. For example, given the observed risks of death and major neurocognitive impairment among the children whom we studied, our sample of 118
individ-uals provided 80% power to detect relative risk reduc-tions of⬃55% for mortality and 40% for the combined outcome of mortality or a major neurocognitive impair-ment. Another limitation is that the dose of dexameth-asone used in our trial was higher than that used in more recent trials and in current clinical practice, which some-what limits the extent to which our findings apply to treatment with dexamethasone as currently used by cli-nicians.
Despite the limitations mentioned above, our study has implications for clinical researchers who are inter-ested in the prevention of CLD. Combining the results of the only 2 randomized trials15,28in which the risk of CLD
among controls was⬎70%, a prolonged course of dexa-methasone was used, and no crossover was allowed leads to the conclusion that dexamethasone is associated with significantly reduced odds for mortality (OR: 0.4; 95% CI: 0.18 – 0.96) and does not increase the risk of the composite outcome of death or major developmental impairment. In view of the potentially beneficial effects of dexamethasone on pulmonary outcomes and survival among infants at very high risk of CLD, more investiga-tion is needed of methods to identify such infants in the first 1 to 2 weeks of life.42Those methods then could be
used to increase the efficiency of future trials of dexa-methasone (and other glucocorticoids) to improve the outcome of infants at high risk for CLD. On the basis of the findings presented here and the pulmonary benefits observed with a much lower dose of dexamethasone,8
we conclude that additional trials of low-dose dexa-methasone (eg, 0.89 mg/kg cumulative dose over 10 days), and perhaps other glucocorticoids (eg, hydrocor-tisone), are warranted.
CONCLUSIONS
In addition to its implications for researchers, our study contributes important information about the long-term effects of dexamethasone treatment of preterm infants to decrease the risk of CLD, a morbidity that has been consistently associated with worse developmental out-come.43When given to infants at high risk of CLD, at the
doses used in our trial, dexamethasone decreases the duration of ventilator dependency and the risk of CLD and may also improve pulmonary function beyond in-fancy.27Although we report here a higher risk of major
neurodevelopmental impairment among dexametha-sone-treated children, this higher risk must be viewed in the context of a strong trend toward improved survival in this group and research that suggests that children with developmental impairments regard their quality of life as similar to that of children without such impair-ments.44A recommendation by the American Academy
of Pediatrics and the Canadian Paediatric Society is that “outside the context of a randomized, controlled trial, the use of corticosteroids should be limited to excep-tional clinical circumstances (eg, an infant on maximal
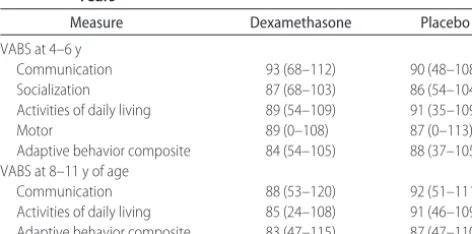
TABLE 5 Comparison of Dexamethasone- and Placebo-Treated
Participants for Adaptive Behavior at 4 to 6 and 8 to 11 Years
Measure Dexamethasone Placebo
VABS at 4–6 y
Communication 93 (68–112) 90 (48–108)
Socialization 87 (68–103) 86 (54–104)
Activities of daily living 89 (54–109) 91 (35–109)
Motor 89 (0–108) 87 (0–113)
Adaptive behavior composite 84 (54–105) 88 (37–105) VABS at 8–11 y of age
Communication 88 (53–120) 92 (51–111)
Activities of daily living 85 (24–108) 91 (46–109) Adaptive behavior composite 83 (47–115) 87 (47–110)
ventilatory and oxygen support).”13 In such
circum-stances, evidence presented here suggests that the like-lihood of death or a major neurodevelopmental impair-ment will not be increased as a result of treatimpair-ment with steroids.
ACKNOWLEDGMENTS
This research was supported by General Clinical Re-search Center of Wake Forest University Baptist Medical Center grant M01-RR07122, National Institutes of Health grant P01-HD047584, the Intramural Research Support Committee of Wake Forest Medical School, the Brenner Center for Child and Adolescent Health, and the North Carolina Department of Health and Human Services.
We thank Alice Scott, RN, Barbara Jackson, RN, BSN, Nancy Peters, RN, Debbie Allred, MA, Natalie Hall, MA, and the parents and children for their participation.
REFERENCES
1. Baden M, Bauer CR, Cole E, Klein G, Taeusch HW, Stern L. A controlled trial of hydrocortisone therapy in infants with re-spiratory distress syndrome.Pediatrics.1972;50:526 –534 2. Gladstone IM, Ehrenkranz RA, Jacobs HC. Pulmonary function
tests and fluid balance in neonates with chronic lung disease during dexamethasone treatment.Pediatrics.1989;84:1072–1076 3. Yoder MC Jr, Chua R, Tepper R. Effect of dexamethasone on pulmonary inflammation and pulmonary function of ventila-tor-dependent infants with bronchopulmonary dysplasia.Am Rev Respir Dis.1991;143:1044 –1048
4. Brundage KL, Mohsini KG, Froese AB, Walker CR, Fisher JT. Dexamethasone therapy for bronchopulmonary dysplasia: im-proved respiratory mechanics without adrenal suppression. Pe-diatr Pulmonol.1992;12:162–169
5. Halliday HL, Ehrenkranz RA, Doyle LW. Early postnatal (⬍96 hours) corticosteroids for preventing chronic lung disease in preterm infants.Cochrane Database Syst Rev.2003;(1):CD001146 6. Halliday HL, Ehrenkranz RA, Doyle LW. Moderately early (7–14 days) postnatal corticosteroids for chronic lung disease in preterm infants.Cochrane Database Syst Rev.2003;(1):CD001144 7. Halliday HL, Ehrenkranz RA, Doyle LW. Delayed (⬎3 weeks) postnatal corticosteroids for chronic lung disease in preterm infants.Cochrane Database Syst Rev.2003;(1):CD001145 8. Doyle LW, Davis PG, Morley CJ, McPhee A, Carlin JB.
Low-dose dexamethasone facilitates extubation among chronically ventilator-dependent infants: a multicenter, international, ran-domized, controlled trial.Pediatrics.2006;117:75– 83
9. Papile LA, Tyson JE, Stoll BJ, et al. A multicenter trial of two dexamethasone regimens in ventilator-dependent premature infants.N Engl J Med.1998;338:1112–1118
10. Anderson ME, Bednarek FJ, Dreyer G, et al. Early postnatal dexamethasone therapy for the prevention of chronic lung disease.Pediatrics.2001;108:741–748
11. Barrington KJ. The adverse neuro-developmental effects of postnatal steroids in the preterm infant: a systematic review of RCTs.BMC Pediatr.2001;1:1
12. Yeh TF, Lin YJ, Lin HC, et al. Outcomes at school age after postnatal dexamethasone therapy for lung disease of prema-turity.N Engl J Med.2004;350:1304 –1313
13. American Academy of Pediatrics, Committee on Fetus and Newborn. Postnatal corticosteroids to treat or prevent chronic lung disease in preterm infants.Pediatrics.2002;109:330 –338 14. Doyle LW, Halliday HL, Ehrenkranz RA, Davis PG, Sinclair JC.
Impact of postnatal systemic corticosteroids on mortality and cerebral palsy in preterm infants: effect modification by risk for chronic lung disease.Pediatrics.2005;115:655– 661
15. Kothadia JM, O’Shea TM, Roberts D, Auringer ST, Weaver RG III, Dillard RG. Randomized placebo-controlled trial of a 42-day tapering course of dexamethasone to reduce the duration of ventilator dependency in very low birth weight infants [published correction appears in Pediatrics. 2004;114:1746].
Pediatrics.1999;104:22–27
16. O’Shea TM, Kothadia JM, Klinepeter KL, et al. Randomized placebo-controlled trial of a 42-day tapering course of dexa-methasone to reduce the duration of ventilator dependency in very low birth weight infants: outcome of study participants at 1-year adjusted age.Pediatrics.1999;104:15–21
17. Shennan AT, Dunn MS, Ohlsson A, Lennox K, Hoskins EM. Abnormal pulmonary outcomes in premature infants: predic-tion from oxygen requirement in the neonatal-period. Pediat-rics.1988;82:527–532
18. Alexander GR, Himes JH, Kaufman RB, Mor J, Kogan M. A United States national reference for fetal growth.Obstet Gynecol.
1996;87:163–168
19. Stewart AL, Reynolds EO, Hope PL, et al. Probability of neu-rodevelopmental disorders estimated from ultrasound appear-ance of brains of very preterm infants.Dev Med Child Neurol.
1987;29:3–11
20. Paneth N. Classifying brain damage in preterm infants.J Pedi-atr.1999;134:527–529
21. Elliott CD.Differential Abilities Scales: Administration and Scoring Manual. San Antonio, TX: Psychological Corporation; 1990 22. Kaufman AS, Kaufman NL. Manual for the Kaufman Test of
Educational Achievement: Comprehensive Form. Circle Pines, MN: American Guidance Service; 1998
23. Sparrow SS, Balla DA, Cicchetti DV.Vineland Adaptive Behav-ioral Scales. Circle Pines, MN: American Guidance Service; 1984 24. Wechsler D.Wechsler Individual Achievement Test. San Antonio,
TX: Psychological Corporation; 1992
25. Wechsler D.Wechsler Intelligence Scale for Children. 3rd ed. New York, NY: Psychological Corporation; 1991
26. Grossman H, ed.Classification in Mental Retardation. Washing-ton, DC: American Association on Mental Deficiency; 1983 27. Nixon PA, Washburn LK, Schechter MS, O’Shea TM.
Fol-low-up study of a randomized controlled trial of postnatal dexamethasone therapy in very low birth weight infants: ef-fects on pulmonary outcomes at age 8 to 11 years.J Pediatr.
2007;150:345–350
28. Cummings JJ, D’Eugenio DB, Gross SJ. A controlled trial of dexamethasone in preterm infants at high risk for bronchopul-monary dysplasia.N Engl J Med.1989;320:1505–1510 29. Gross SJ, Anbar RD, Mettelman BB. Follow-up at 15 years of
preterm infants from a controlled trial of moderately early dexamethasone for the prevention of chronic lung disease.
Pediatrics.2005;115:681– 687
30. Edwards HE, Burnham WM. The impact of corticosteroids on the developing animal.Pediatr Res.2001;50:433– 440 31. Murphy BP, Inder TE, Huppi PS, et al. Impaired cerebral
cor-tical gray matter growth after treatment with dexamethasone for neonatal chronic lung disease.Pediatrics.2001;107:217–221 32. Shinwell ES, Karplus M, Reich D, et al. Early postnatal dexa-methasone treatment and increased incidence of cerebral palsy.Arch Dis Child Fetal Neonatal Ed.2000;83:F177–F181 33. Yeh TF, Lin YJ, Hsieh WS, et al. Early postnatal
dexameth-asone therapy for the prevention of chronic lung disease in preterm infants with respiratory distress syndrome: a mul-ticenter clinical trial. Pediatrics. 1997;100(4). Available at: www.pediatrics.org/cgi/content/full/100/4/e3
pre-vention of chronic lung disease in preterm infants: a 3-year follow-up. Pediatrics. 2002;109(6). Available at: www. pediatrics.org/cgi/content/full/109/6/e85
35. Collaborative Dexamethasone Trial Group. Dexamethasone therapy in neonatal chronic lung disease: an international placebo-controlled trial.Pediatrics.1991;88:421– 427
36. O’Shea TM. Definition and classification of cerebral palsy: an epidemiologist perspective. Dev Med Child Neurol. 2007;49: 29 –30
37. Hille ETM, Elbertse L, Gravenhorst JB, Brand R, Verloove-Vanhorick SP; Dutch POPS-19 Collaborative Study Group. Nonresponse bias in a follow-up study of 19-year-old adoles-cents born as preterm infants.Pediatrics.2005;116(5). Available at: www.pediatrics.org/cgi/content/full/116/5/e662
38. Tin W, Fritz S, Wariyar U, Hey E. Outcome of very preterm birth: children reviewed with ease at 2 years differ from those followed up with difficulty.Arch Dis Child Fetal Neonatal Ed.
1998;79:F83–F87
39. Aylward GP, Hatcher RP, Stripp B, Gustafson NF, Leavitt LA.
Who goes and who stays: subject loss in a multicenter, longi-tudinal follow-up-study.J Dev Behav Pediatr.1985;6:3– 8 40. Hack M, Taylor HG, Drotar D, et al. Poor predictive validity of
the Bayley Scales of Infant Development for cognitive function of extremely low birth weight children at school age.Pediatrics.
2005;116:333–341
41. Roth SC, Baudin J, Pezzani-Goldsmith M, Townsend J, Reyn-olds EO, Stewart AL. Relation between neurodevelopmental status of very preterm infants at one and eight years.Dev Med Child Neurol.1994;36:1049 –1062
42. Bose CL, Laughon MM. Corticosteroids and chronic lung disease: time for another randomized, controlled trial. Pediat-rics.2005;115:794
43. Ehrenkranz RA, Walsh MC, Vohr BR, et al. Validation of the National Institutes of Health consensus definition of broncho-pulmonary dysplasia.Pediatrics.2005;116:1353–1360 44. Saigal S, Stoskopf B, Pinelli J, et al. Self-perceived
health-related quality of life of former extremely low birth weight infants at young adulthood.Pediatrics.2006;118:1140 –1148
THREE LEGAL PARENTS?
“Sometimes when the earth shudders it doesn’t make a sound. That’s what happened in Harrisburg, PA, recently. On April 30, a state Superior Court panel ruled that a child can have three legal parents. The case, Jacob v Shultz-Jacob, involved two lesbians who were the legal coparents of two children conceived with sperm donated by a friend. The panel held that the sperm donor and both women were all liable for child support. Arthur S. Leonard, a professor at New York Law School, observed, ‘I’m unaware of any other state appellate court that has found that a child has, simultaneously, three adults who are financially obligated to the child’s support and are also entitled to visitation.’ The case follows a similar decision handed down by a provincial court in Ontario in January. In what appeared to be the first ruling in any Western nation, the court ruled that a boy can legally have three parents. In that case the biological mother and father had parental rights and wished for the biological mother’s lesbian partner, who functions as the boy’s second mother, to have such rights as well. The idea of assigning children three legal parents is not limited to North America. In 2005, expert commis-sions in Australia and New Zealand proposed that sperm or egg donors be allowed to ‘opt in’ as a child’s third parent. That same year, scientists in Britain received state permission to create an embryo from the DNA of three adults, raising the real possibility that they all could be granted equal legal claims to the child if the embryo developed to term.”
Marquardt E.New York Times. July 16, 2007
DOI: 10.1542/peds.2007-0486
2007;120;594
Pediatrics
T. Michael O'Shea, Lisa K. Washburn, Patricia A. Nixon and Donald J. Goldstein
Infants: Neurodevelopmental Outcomes at 4 to 11 Years of Age
Decrease the Duration of Ventilator Dependency in Very Low Birth Weight
Follow-up of a Randomized, Placebo-Controlled Trial of Dexamethasone to
Services
Updated Information &
http://pediatrics.aappublications.org/content/120/3/594
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/120/3/594#BIBL
This article cites 32 articles, 17 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/pulmonology_sub Pulmonology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2007-0486
2007;120;594
Pediatrics
T. Michael O'Shea, Lisa K. Washburn, Patricia A. Nixon and Donald J. Goldstein
Infants: Neurodevelopmental Outcomes at 4 to 11 Years of Age
Decrease the Duration of Ventilator Dependency in Very Low Birth Weight
Follow-up of a Randomized, Placebo-Controlled Trial of Dexamethasone to
http://pediatrics.aappublications.org/content/120/3/594
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.