ARTICLE
Differences in Infant and Parent Behaviors During
Routine Bed Sharing Compared With Cot Sleeping in
the Home Setting
Sally A. Baddock, PhDa, Barbara C. Galland, PhDa, David P. G. Bolton, MRCP, PhDb, Sheila M. Williams, DScc, Barry J. Taylor, MBChB, FRACPa
aDepartments of Women’s and Children’s Health andcPreventive and Social Medicine, Dunedin School of Medicine, andbDepartment of Physiology, Otago School of
Medical Sciences, University of Otago, Dunedin, New Zealand
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVES.To observe the behavior of infants sleeping in the natural physical environment of home, comparing the 2 different sleep practices of bed sharing and cot sleeping quantifying to factors that have been identified as potential risks or benefits.
METHODS.Forty routine bed-sharing infants, aged 5–27 weeks were matched for age and season of study with 40 routine cot-sleeping infants. Overnight video and physiologic data of bed-share infants and cot-sleep infants were recorded in the infants’ own homes. Sleep time, sleep position, movements, feeding, blanket height, parental checks, and time out of the bed or cot were logged.
RESULTS.The total sleep time was similar in both groups (bed-sharing median: 8.6 hours; cot-sleeping median: 8.2 hours). Bed-sharing infants spent most time in the side position (median: 5.7 hours, 66% of sleep time) and most commonly woke at the end of sleep in this position, whereas cot-sleeping infants most commonly slept supine (median: 7.5 hours, 100%) and woke at the end of sleep in the supine position. Prone sleep was uncommon in both groups. Head covering above the eyes occurred in 22 bed-sharing infants and 1 cot-sleeping infant. Five of these bed-sharing infants were head covered at final waking time, but the cot-sleeping infant was not. Bed-sharing parents looked at or touched their infant more often (median: 11 vs 4 times per night) but did not always fully wake to do so. Movement episodes were shorter in the bed-sharing group as was total movement time (37 vs 50 minutes respectively), whereas feeding was 3.7 times more frequent in the bed-sharing group than the cot-sleeping group.
CONCLUSIONS.Bed-share infants without known risk factors for sudden infant death syndrome (SIDS) experience increased maternal touching and looking, increased breastfeeding, and faster and more frequent maternal responses. This high level of interaction is unlikely to occur if maternal arousal is impaired, for example, by alcohol or overtiredness. Increased head covering and side sleep position occur during bed-sharing, but whether these factors increase the risk of SIDS, as they do in cot sleeping, requires further investigation.
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-1636
doi:10.1542/peds.2005-1636
Key Words
cosleeping, SIDS, breastfeeding, sleep
Abbreviation
SIDS—sudden infant death syndrome
Accepted for publication Oct 17, 2005
Address correspondence to Barry Taylor, MBChB, FRACP, Department of Women’s and Children’s Health, University of Otago, PO Box 913, Dunedin, New Zealand. E-mail: barry. [email protected]
M
ANY GROUPS VALUE bed sharing, whether as a traditional practice, a positive parenting choice,or a way of coping with the demands of an infant.1–3
These varied motivations lead to considerable
heteroge-neity with regard to the actual practices involved.2,4–6The
practice is relatively common in the United Kingdom7
and has become more common in Western countries in
the last 10 years, for example, the United States,8
Nor-way,9and the Netherlands.10 This is in part coincident
with the promotion of breastfeeding.9Many advantages
have been documented, for example, increased
breast-feeding,11,12increased mother-infant interactions,12 and
increased infant arousals.12 However, bed sharing has
also been identified as a risk factor for sudden infant death syndrome (SIDS) in combination with maternal
smoking,13–15 alcohol consumption,14,15 maternal
over-tiredness,14excessive or soft bedding,16bed sharing with
someone other than parents,17 and younger infant
age.14,15,18 There may also be separate risks associated
with sleeping in an adult bed without adults, similar to
those identified with sleeping in any unusual place.14
The recent policy statement of the American Academy of Pediatrics did not target these risk factors but
recom-mended against bed sharing during sleep.19There are a
number of postulated mechanisms for this increased risk but little research to provide evidence for them in the bed-share situation.
There is a need to identify benefits and risks to the infant and parent(s) to understand the ways bed sharing could be made safer for all infants. The change away from the prone sleep position has been very successful in
many cultures at reducing the SIDS rate,20but changes
to other potentially modifiable factors have met with
limited success.15,21It may be more realistic and of more
benefit to families that value bed sharing to identify ways to make it safer rather than increase guilt about what is a common and, for many cultures, a valued child-care practice.
When trying to assess the risks or benefits of bed sharing, cot sleeping is often taken as the norm; how-ever, within many cultures, bed sharing is the norm or
has historically been so.22 It is important to identify
normative data for bed sharing rather than treating the 2 environments as if they are the same. Three groups have published findings from observational studies of infants
sleeping overnight in a bed-share situation.12,23,24These
studies have been in sleep laboratories with infants at low risk of SIDS using a crossover design so that infants act as their own controls. This, however, means that infants are asked to sleep nights in a situation that is not their usual practice. As far as we are aware, there are no published studies of overnight family behavior con-ducted in the home environment comparing bed sharing and infant cot sleep.
The aim of this study, therefore, was to observe and document the behavior of families sleeping in their
home environment, comparing the 2 different sleep practices of bed sharing and cot sleeping. This was to identify the differences between groups in regard to sleep time, sleep position, movements, feeding, blanket height, and parental checks, which may contribute to the mechanisms underlying risks and benefits identified from epidemiologic data.
METHODS
Two groups of infants were studied: 40 bed-sharing in-fants and 40 cot-sleeping inin-fants. The sleep practice cri-teria was that bed-sharing infants regularly slept in the parental bed for a minimum of 5 hours per night whereas cot-sleeping infants regularly slept in a cot or
bassinette in the parental bedroomⱖ5 hours per night.
None of the infants reported prenatal or postnatal com-plications (questionnaire). Bed-sharing infants were re-cruited through local postnatal groups and media adver-tising. Cot-sleeping infants matched for age and season of study were recruited from the local maternity ward. Infants were aged 0 – 6 months with 13 infant pairs aged 0 –12.9 weeks, 15 pairs aged 13–19.9 weeks, and 12 pairs
aged 20 –27 weeks. All of the infants were at⬎37 weeks’
gestation (except 2 infants in each group who were 28 and 32 weeks’ gestation). The age of the 4 premature infants was adjusted to be consistent with 40 weeks’ gestation. There were 14 pairs of studies in the winter compared with 8 to 10 studies in each of the other seasons. The study was approved by the Southern Re-gional Health Authority Ethics Committee, New Zealand (protocol 97/04/036). Informed consent was obtained from the parent(s) of all of the infants studied.
Protocol
Infants were monitored over 2 consecutive nights in their own home. The first night involved video recording only, and the second involved video and physiologic recording. The physiologic recordings involved place-ment of electrodes for recording raw electrocardiogram, oxygen saturation and heart rate, abdominal and chest movements of respiratory pattern, nasal airflow, shin
and rectal temperature, and CO2near the infant’s face.
The details of these recordings have been described
pre-viously.25Infants were set up and recordings started by
reflect light off the ceiling on to the recording area. The camera was connected to an analog video recorder (Panasonic AG-TL700) set to “long play” that allowed 15 hours of recording on a 3-hour videotape.
Video Analysis
Analysis of the video data for sleep time, sleep position, movements, feeding, blanket height, and parental checks was based on observations on the second night, allowing synchronization with physiologic recordings. Custom-developed computer software was used to log all of the significant events into a database with time code for correlation with the physiologic readings. C Video software (Envisionology, San Francisco, CA) and a connecting cable were used to link the time counter from the video player with a key command on the computer. The database (File Maker Pro 2.0; Claris Cor-poration, Santa Clara, CA) was customized to provide a file for each major behavior category and subcategory. The start and finish times and code for each event were logged in the database using computer key commands. The video counter was calibrated with the real time digitized on the recording tape. Although tapes were recorded as long play, they were viewed at normal tape speed.
Off-line logging of data started from when the infant was asleep. Sleep was identified from the video and defined as starting after the infant was settled for 2 minutes. Start and stop times for behavioral categories listed here were logged into the database from this start time until the final waking of the infant in the morning. Subcategories for sleep position were: side, prone, and supine; for blanket height: below chin, chin to eyes, and above eyes; for parental checks: father look, father touch, mother look, and mother touch; for infant move-ments: small movement, posture change (trunk or gross body movement), response to parent (any infant move-ment that occurred after movemove-ment by the adjacent adult), feeding, and time out of the cot. Sleep and awake periods were identified from the video. If the infant awoke during sleep and returned to a settled state within 2 minutes, this period was included as sleep.
Awaken-ings that lasted for⬎2 minutes were described as awake.
Study time was defined from when the infant was first asleep, regardless of the presence of an adult, until the infant woke in the morning. Sleep time was the accu-mulation of the infant sleep periods during the study time. Sleep efficiency was expressed as the percentage of total sleep time/total study time.
Statistical Analyses
Based on studies of high-risk behavior in cot-sleeping
infants,26 it was predicted that 50% of bed-sharing and
20% of cot-sleeping infants were likely to experience a potentially dangerous event. Two samples of 40, using
the 5% level of significance, have 80% power to show this difference between groups.
Although bed-share and cot-sleep infants were matched for age and season of study, data for both members of 4 pairs were not available. Data were, there-fore, analyzed as 2 groups, and regression analysis, ad-justing for infant age and season, was used to take the matching into account. Medians and interquartile ranges are presented to describe the data. A Kruskal-Wallis test, Poisson or negative binomial regression, to account for the overdispersion in the data, or linear regression based on log transformation values were used to compare the 2 groups for the behavior variables. Results, where ap-propriate, are presented as the risk ratios and 95% con-fidence intervals.
RESULTS
As shown in Table 1, bed-sharing and cot-sleeping in-fants were comparable with regard to gestational age, birth weight, male:female ratio, age at study, and weight at study. All of the bed-sharing infants and 35 of 40 cot-sleeping infants were breastfed. The age of the mother and the proportion of mothers educated to ter-tiary level were similar between the groups. A small number in both groups were identified as Maori, indig-enous New Zealanders. Maternal smoking was more common in the cot group (25%) compared with the bed-sharing group (8%). Maternal alcohol consumption was minimal in all, ranging from “rarely” to 3 glasses of wine or beer per week, with 17 of 40 bed sharers and 15 of 40 mothers of cot sleepers reporting no alcohol con-sumption during or after pregnancy. The practice of bed sharing was reported to be adopted by mothers because of factors such as the ease of breastfeeding, the provision of a close and secure environment for the infant, a more settled infant, and a natural environment.
Total Sleep Time and Sleep Efficiency
The total study time was similar between groups (bed sharing: median, 9.7 hours [interquartile range: 8.8 – 10.2 hours]; cot-sleeping: median, 9.0 [interquartile range: 8.7–10.2]). The total sleep time, as determined by video observation, was also similar (bed sharing: me-dian, 8.6 hours [interquartile range: 7.8 –9.4]; cot-sleep-ing: median, 8.2 [interquartile range: 7.4 –9.0]). Conse-quently, sleep efficiency was similar between groups (bed sharing: median, 90.7% [interquartile range: 87.1– 94.6]; cot-sleeping: median, 87.1 [interquartile range: 84.1–96.2]).
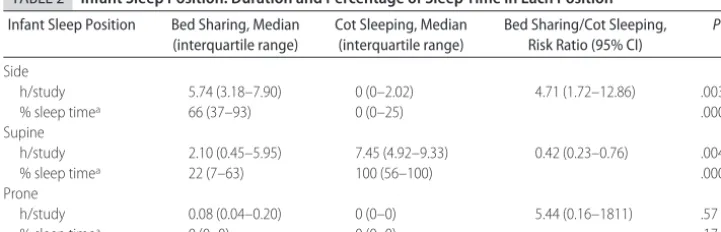
Infant Sleep Position
most commonly slept supine (median: 7.5 hours, 100% sleep time). The median time spent prone was not sig-nificantly different. At the end of the final sleep period, a similar distribution of sleep positions was observed. Bed-sharing infants were most commonly on their side (side: 23 infants; supine: 13; prone: 2), whereas cot-sleeping infants were commonly supine (side: 4 infants; supine: 33; prone: 2). The pattern of prone sleep varied between the 2 groups: 5 bed-sharing infants (aged 7, 8, 10, 22, and 23 weeks) spent some time prone (3.0, 3.5, 2.3, 2.2, and 1.6 hours, respectively), and 2 cot-sleeping infants (aged 8 and 25 weeks) slept the entire night in the prone position (8.9 and 10.2 hours, respectively).
Blanket Height Relative to Infant
Results for blanket height are shown in Table 3. Infants in both groups spent most of the night sleeping with the blankets below the level of the chin (bed-sharing dian: 7.1 hours [82% of sleep time]; cot-sleeping me-dian: 8.1 hours [100% of sleep time]). Bed-sharing
in-fants spent significantly more time than cot inin-fants with the blankets partially over the face (to the eyes) or with blankets above the eyes. Head-covering events (ie, blan-kets above the eyes) occurred in 22 bed-sharing infants and 1 cot-sleeping infant. At final awakening time, 5 of these bed-share infants had their head covered. The last head-covering incident for the cot-sleep infant finished 4 hours before final waking.
Parental Checks
When mothers in both groups checked their infant, it usually involved touching rather than just looking at the infant. Table 4 shows that there was no significant dif-ference in the amount of time bed-sharing mothers spent checking their infant compared with mothers of cot-sleeping infants. Fathers/partners rarely checked the infants (data not shown), but when all of the looks and touches by both parents were combined, bed-sharing parents checked their infant a median of 11 times com-pared with 4 checks by the parents of the cot-sleeping
TABLE 1 Infant and Maternal Group Characteristics
Study Group Bed Sharing
(n⫽40)
Cot Sleeping (n⫽40)
P
Infant characteristics
Study age, wka 15.3 (9.9–20.4) 16.5 (10.0–21.0) .93
Birth weight, ga 3615 (3190–4100) 3595 (3310–3965) .86
Gestation, wka 40.5 (39.0–41.0) 40 (39.0–41.0)b .62
Study weight, ga 6450 (5605–7755) 6720 (5700–7590)b .84
Sex (female)c 17 (43) 18 (45) .90
Breastfedd 40 (100) 35 (88) .05
Maternal characteristics (n)
Smoking at mid-trimesterd(38) 3 (8) 10 (25) .06
Tertiary educationde(26) 23 (88) 25 (96) .31
Ethnicityc(40)
Maori 4 (10) 7 (18)
European 31 (78) 23 (58) .18
Other 5 (13) 10 (25)
Data are median (interquartile range) orn(%).
aKruskal-Wallis test. bData missing from 1 infant. c2test.
dFisher’s exact test.
eTertiary refers to any post– high school education.
TABLE 2 Infant Sleep Position: Duration and Percentage of Sleep Time in Each Position
Infant Sleep Position Bed Sharing, Median (interquartile range)
Cot Sleeping, Median (interquartile range)
Bed Sharing/Cot Sleeping, Risk Ratio (95% CI)
P
Side
h/study 5.74 (3.18–7.90) 0 (0–2.02) 4.71 (1.72–12.86) .003
% sleep timea 66 (37–93) 0 (0–25) .0001
Supine
h/study 2.10 (0.45–5.95) 7.45 (4.92–9.33) 0.42 (0.23–0.76) .004
% sleep timea 22 (7–63) 100 (56–100) .0001
Prone
h/study 0.08 (0.04–0.20) 0 (0–0) 5.44 (0.16–1811) .57
% sleep timea 0 (0–0) 0 (0–0) .17
Adjusted for age, season of study, and total sleep time. CI indicates confidence interval.
infants (P⬍.0001). When considering individuals, there were extreme examples, for example, parents in 1 bed-sharing study checked their infant 53 times. These were predominantly brief touches by the mother. Observa-tions indicated that the bed-sharing parents did not al-ways wake fully to check their infant, and small patting movements, in what seemed to be drowsy sleep, were common.
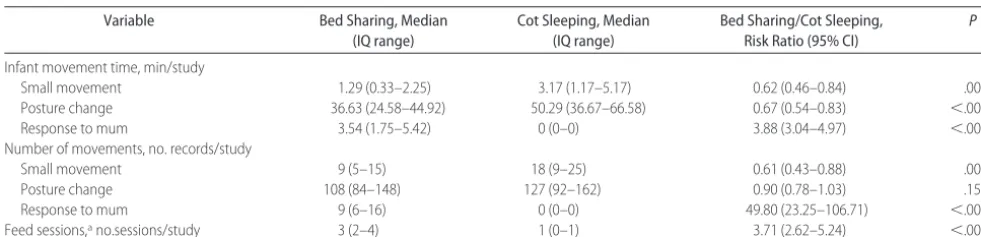
Infant Movements
Table 5 shows that the most common type of movement recorded in both groups through the night was posture change. Bed-sharing infants spent significantly less time in posture change movements compared with cot-sleep-ing infants (37 vs 50 minutes, respectively). However, the number of posture change records was similar for both groups, suggesting that individual periods of pos-ture change movement through the night were shorter for bed-sharing infants. There were significantly fewer small movements (brief hand movements) by the bed-sharing infants, and they occurred for less total time, whereas responses to mother were more frequent and lasted for longer total time. Feeding was 3.7 times more frequent in the bed-sharing group than the cot-sleeping group.
DISCUSSION
This study clearly demonstrated different behaviors of both the infant and parents when comparing bed-shar-ing and cot-sleepbed-shar-ing practices. Although the cot was usually immediately adjacent to the parents’ bed, the presence of the infant in the adult bed for bed-share
studies resulted in very different behaviors. The study showed that regular bed-share infants engaged in more feeding and more infant-mother interactions than cot-sleep infants, side cot-sleeping position was more common during sleep and at final waking in bed-share infants, and prone sleeping position, although rare, occurred for short intervals in bed-share infants, whereas it lasted all night for 2 cot infants. Incidents where the bedding or clothing covered the infant’s head were more common in the bed-sharing situation both during the night and on final waking.
Previous smaller studies comparing the same practices have been conducted mainly in the laboratory
set-ting,23,27although attempts have been made to make the
environment as home-like as possible. These studies used a crossover design that showed that, for many behaviors, the largest difference was recorded for regular bed sharers on their bed-share night compared with
regular cot-sleepers on their cot-sleep night.23,27This
em-phasizes the importance of observing infants in their regular sleep arrangement, as in this study. The present study supports the observations from laboratory studies that bed-share infants engage in more feeding episodes and are checked by their mother more frequently than
cot-sleeping infants.23,28–30Mothers often identified ease
of breastfeeding as a reason for bed sharing. Population studies also support an association between bed sharing
and breastfeeding31 and an association with
breastfeed-ing persistbreastfeed-ing to an older infant age.32Several large
ep-idemiologic studies have shown a small but significant
protective effect of breastfeeding against SIDS;17,33–36
however, this has not been shown in some others.37,38
TABLE 4 Parental Checking (looking and/or touching): Total Duration and Number of Checks for Bed-Sharing and Cot-Sleeping Infants
Parental Checks Bed Sharing, Median (interquartile range)
Cot Sleeping, Median (interquartile range)
Bed Sharing/Cot Sleeping, Risk Ratio (95% CI)
P
Time mother touching, min/study 4.59 (2.58–12.25) 1.54 (0.25–3.67) 2.07 (0.99–4.55) .07 No. parental checks, no./study 11 (7–25) 4 (2–6) 3.35 (2.45–4.59) ⬍.0001
Adjusted for age, season of study, and total sleep time. CI indicates confidence interval. Negative binomial regression TABLE 3 Blanket Height Relative to the Infant’s Face: Duration and Percentage of Sleep Time at
Different Blanket Heights
Blanket Height Bed Sharing, Median (interquartile range)
Cot Sleeping, Median (interquartile range)
Bed Sharing/Cot Sleeping, Risk Ratio (95% CI)
P
Below chin
h/study 7.10 (5.66–9.18) 8.10 (7.28–9.42) 0.88 (0.86–0.90) ⬍.0001
% sleep timea 82 (62–99) 100 (100–100) .0001
To eyes
h/study 0.83 (0–2.20) 0 (0–0) 3.12 (2.89–3.37) .0001
% sleep timea 10 (0–26) 0 (0–0) .0001
Above eyes
h/study 0.20 (0–1.03) 0 (0–0) 17.06 (13.45–21.63) .0001
% sleep timea 2 (0–10) 0 (0–0) .0001
Adjusted for age, season of study, and total sleep time. CI indicates confidence interval.
Concern has been raised regarding the possibility of accidental asphyxiation from mothers falling asleep
breastfeeding while lying down.39 No instances were
noted where the mother was in a position that might have resulted in mechanical obstruction of the airways,
and no oxygen desaturation events ⬍90% with head
covered (data not given) or any increase in rectal
tem-perature outside the reference range was observed.25
The reason we videoed 2 nights was to establish whether there was any difference in behavior because of “first-night effect” or the presence of the sensors on the
infant. Using Bland-Altman plots,40we found no
signif-icant difference on key behavioral indices, such as sleep time, number of infant movements per hour, feeds, and sleep position, suggesting that attachment of the sensors did not have a significant effect on sleep behavior.
Although there is no direct evidence that increased maternal checking reduces SIDS, mothers in this study
and others2,23,41,42report an emotional benefit from bed
sharing, because they can easily check their infant. Mothers have also been observed to actively check and
modify infant temperature by rearranging bedding.43
Room sharing compared with infant sleeping in a
sepa-rate room is protective against SIDS14,15,44 and may be
related to increased maternal checks. It is likely that the dramatic reduction in the multivariate relative risk for infants not sharing the room and prone from 16.99 (95% CI: 10.43–27.69) to 3.28 (95% CI: 2.06 –5.23) for
infants sharing the room and prone44 is explained by
increased awareness and checking of infants while they are asleep. In our study, whereas bed-share parents checked their infant more often, many of these checks were brief, involving minimal disruption to the mother’s
sleep. These findings are confirmed by Mosko et al,45
who reported that total sleep time of mothers was not decreased on bed-share nights compared with infant cot-sleep nights and that maternal awakenings were for shorter duration on the bed-share nights. It is likely that greater arousal and more disruption to maternal sleep
would be needed to check an infant in a cot, even if it was nearby.
The risks and/or benefits associated with increased waking have been debated. In adults and children, sleep fragmentation is associated with many negative effects, such as increasing the frequency and duration of
ob-structive sleep apnea46and increasing the arousal
thresh-old.47,48However, none of these studies have been
con-ducted on breastfeeding women. It is not known whether the multiple, brief, drowsy awakenings through the night during bed sharing would have more or less impact on the mother than the few, full awakenings required to attend to an infant in the cot. Interestingly, mothers in this study, as in others, report “increased sleep” as a reason to bed share, along with “having a more settled infant.” Studies investigating the effect of mild sleep deprivation on infants report a possible
in-creased propensity to upper airway obstruction49,50and
changes in autonomic control of cardiac function.51
However, it is likely that experimentally induced sleep deprivation has different physiologic manifestations from infant-initiated awakenings through the night as-sociated with breastfeeding.
The finding in this study that the side sleep position was the most common sleep position for bed-share
in-fants is in agreement with Ball’s findings.30 However,
whereas bed-share infants had significant periods of side
sleep in laboratory-based studies,23,52the supine position
was predominant. The increased instrumentation for re-cording electroencephalogram, electro-oculogram, and electromyogram in these 2 studies might have affected the position mothers placed their infant to sleep (Helen Ball, PhD, written communication, 2002). The side sleep position has been identified as increasing the risk of
SIDS,15,53 reportedly associated with the tendency of
side-sleep infants to roll prone.15However, the evidence
for this has been established from infants sleeping in a cot. There is no data to establish the risk of this position during bed-share sleep. In our study, 12 cot-sleep infants
TABLE 5 Infant Movements and Feeding Sessions: Total Duration and Number of Movement Records for Bed-Sharing and Cot-Sleeping Infants
Variable Bed Sharing, Median
(IQ range)
Cot Sleeping, Median (IQ range)
Bed Sharing/Cot Sleeping, Risk Ratio (95% CI)
P
Infant movement time, min/study
Small movement 1.29 (0.33–2.25) 3.17 (1.17–5.17) 0.62 (0.46–0.84) .002
Posture change 36.63 (24.58–44.92) 50.29 (36.67–66.58) 0.67 (0.54–0.83) ⬍.0001
Response to mum 3.54 (1.75–5.42) 0 (0–0) 3.88 (3.04–4.97) ⬍.0001
Number of movements, no. records/study
Small movement 9 (5–15) 18 (9–25) 0.61 (0.43–0.88) .007
Posture change 108 (84–148) 127 (92–162) 0.90 (0.78–1.03) .15
Response to mum 9 (6–16) 0 (0–0) 49.80 (23.25–106.71) ⬍.0001
Feed sessions,ano.sessions/study 3 (2–4) 1 (0–1) 3.71 (2.62–5.24) ⬍.0001
Adjusted for age and season of study. CI indicates confidence interval. Movement time was analyzed using regression on log transformation of the data. Movement records were analyzed using Poisson regression.
aAny feeding recommenced within 30 minutes was coded as 1 session. Cot infants were not in view when feeding, thus, feeding sessions were equated with removal from the cot. This may have
spent some time sleeping on their side, but none were observed to roll to the prone position. All 38 of the bed-share infants slept some time on their side, and 1 infant, aged 23 weeks, was observed to roll to the prone position when the mother moved away from the infant. A characteristic sleep position of mother and breastfed infant that seems to prevent rolling has been described: mother sleeping in a lateral position, facing the infant, with her knees drawn up under the infant feet and the
mother’s arm positioned above the infant’s head.54,55
This was observed in our study, but it was not universal, despite all of our mothers being breastfeeders.
Head covering by blankets occurred more often in the bed-share group, a finding also observed by Ball (Helen Ball, PhD, written communication, 2002) but not
re-ported by others. Young23 found no instances of head
and body completely covered by bedding. This may re-flect a difference in home monitoring compared with the sleep laboratory, where arguably parents are more re-laxed and more likely to engage in usual practices. Whether this behavior places these infants at risk is another question. Being found with head covered has been reported in several studies as increasing the risk of SIDS (odds ratio: 12.5; 95% confidence interval: 6.47–
24.1).15 Although head covering was common among
the bed-share infants in this study, only a quarter of infants with head-covering episodes during the night ended up with head covered at the end of sleep. Bedding tended to be moved on and off infants more often during the natural course of sleep through the night. This may help explain why bed-share infants are found with the head covered at the end of sleep less often than cot-sleep
infants.56Infants in the present study often stayed
(with-out significant movement) in the head-covered position for long periods of time (eg, 3.5 hours by 1 infant), suggesting they were not uncomfortable. Our previous studies suggest that the risk of significant rebreathing into bedding depends on the type and thickness of
cov-ering,57,58as well as the ability of the infant to mount
both a respiratory and arousal response. Because infants of smoking mothers may well be the infants least likely
to respond to this stress,59–61 the large interaction
be-tween smoking and bed sharing noted in epidemiologic studies may be explained by poor responsiveness to this particular occurrence during bed-sharing sleep.
Bed-share infants in this study had a different pattern of movements than the cot infants. Although there were the same numbers of posture change episodes in both groups, episodes were shorter in the bed-share group, resulting in a highly significant, reduced total posture change time. The presence of the mother, often touching or cradling the infant during sleep, may also have brought rapid reassurance to the bed-share infant and reduced nonawake movement episodes and, conse-quently, reduced stress experienced by infants.
It would seem that the bed-share infants in this study
were at low risk of SIDS, because there were very few maternal smokers, all of the infants in the bed-sharing group were breastfed, most mothers had some form of tertiary education, and families actively chose to bed share because of perceived advantages to themselves and their infant. The findings may be quite different in bed-sharing families where many SIDS risk factors are
prev-alent13,17,62and breastfeeding is not common.
Although this study has identified potential hazards that may be encountered during bed sharing, for exam-ple, head covering, it has also identified many potential benefits, for example, increased parental checks. This was not a surprising finding, because in many societies around the world, bed sharing is the preferred sleep arrangement. It is only relatively recently that white societies have moved to a solitary sleep arrangement, where conditioning infants to sleep through the night
without waking is a goal valued by society.63 However,
there is a growing trend among whites to choose to bed
share as a parenting style.7–9
This study has highlighted many factors that seem to be common to both bed-sharing and cot-sleep infants but in fact vary in important ways because of the differ-ent physical environmdiffer-ents and the presence of adults. Thus, risk factors identified for infants sleeping in a cot, for example, side sleep, may not be directly applicable to bed-sharing infants and require investigation by epide-miologic studies using cases and controls in the bed-share environment. Secondly, the benefits of bed sharing, for example, increased maternal checking, breastfeeding, and faster and more frequent maternal responses, rely on the mother’s ability to arouse, at least partially, and respond to the infant through the night. Mothers impaired, for example, by alcohol or extreme overtiredness, may not be able to respond appropriately, thus stressing the importance of a healthy, nonimpaired mother in the bed-share partnership.
ACKNOWLEDGMENTS
We thank Charrissa Makowharemahihi and Amanda Phillips for research assistance, Christine Rimene for advice on cultural aspects, Paul Bennington and Gordon Yau for assistance with customising the database for video logging, and the families that participated in the study.
This study was supported by a grant from the Health Research Council of New Zealand.
REFERENCES
1. McKenna JJ, Mosko S. Evolution and infant sleep - an exper-imental study of infant-parent co-sleeping and its implications for SIDS.Acta Paediatr.1993;82:31–36
2. Baddock SA, Day HF, Rimene CR, Moala AF, Taylor BJ, Day RR. Bedsharing practices of different cultural groups. 6th SIDS International Conference. Auckland, New Zealand; 2000 3. Ball HL, Hooker E, Kelly PJ. Where will the baby sleep?
cosleeping with their newborn infants. Am Anthropol. 1999; 101:143–151
4. Tuohy PG, Smale P, Clements M. Ethnic differences in parent/ infant co-sleeping practices in New Zealand.NZ Med J.1998; 111:364 –366
5. Latz S, Wolf AW, Lozoff B. Cosleeping in context: sleep prac-tices and problems in young children in Japan and the United States.Arch Pediatr Adolesc Med.1999;153:339 –346
6. Nelson EA, Chan PH. Child care practices and cot death in Hong Kong.NZ Med J.1996;109:144 –146
7. Blair PS, Ball HL. The prevalence and characteristics associated with parent-infant bed-sharing in England. Arch Dis Child.
2004;89:1106 –1110
8. Willinger M, Ko CW, Hoffman HJ, Kessler RC, Corwin MJ. National Infant Sleep Position Study. Trends in infant bed sharing in the United States, 1993–2000: the National Infant Sleep Position Study.Arch Pediatr Adolesc Med.2003;157:43– 49 9. Arnestad M, Andersen M, Vege A, Rognum TO. Changes in the epidemiological pattern of sudden infant death syndrome in southeast Norway, 1984 –1998: Implications for future preven-tion and research.Arch Dis Child.2001;85:108 –115
10. De Jonge GA, Hoogenboezem J. Epidemiology of 25 years of crib death (sudden infant death syndrome) in the Netherlands; incidence of crib death and prevalence of risk factors in 1980 –2004 [abstract]. Ned Tijdschr Geneeskd, 2005;149: 1273–1278
11. Ball, HL, Breastfeeding, bed-sharing and infant sleep. Birth,
2003. 30:181–188
12. McKenna J, Mosko S, Richard C, et al. Experimental studies of infant-parent co-sleeping—mutual physiological and behav-ioral influences and their relevance to SIDS (Sudden Infant Death Syndrome).Early Hum Dev.1994;38:187–201
13. Scragg R, Mitchell EA, Taylor BJ, et al. Bed sharing, smoking, and alcohol in the sudden infant death syndrome. New Zea-land Cot Death Study Group.BMJ.1993;307:1312–1318 14. Blair P, Fleming P, Smith I, et al. Babies sleeping with parents:
Case-control study of factors influencing the risk of the Sudden Infant Death Syndrome.BMJ.1999;319:1457–1462
15. Carpenter RG, Irgens LM, Blair PS, et al. Sudden unexplained infant death in 20 regions in Europe: case control study.Lancet.
2004;363:185–191
16. Flick L, White DK, Vemulapalli C, et al. Sleep position and the use of soft bedding during bed sharing among African Ameri-can infants at increased risk for sudden infant death syndrome.
J Pediatr.2001;138:338 –343
17. Hauck FR, Herman SM, Donovan M, et al. Sleep environment and the risk of sudden infant death syndrome in an urban population: the Chicago Infant Mortality Study. Pediatrics.
2003;111:1207–1214
18. Tappin D, Russell E, Brooke H. Bedsharing, roomsharing and sudden infant death syndrome in Scotland: a case-control study.J Pediatr.2005;147:32–37
19. American Academy of Pediatrics, Task Force on SIDS. The changing concept of Sudden Infant Death Syndrome: diagnos-tic coding shifts, controversies regarding the sleeping environ-ment, and new variables to consider in reducing risk.Pediatrics.
2005;116:1245–1255
20. Ponsonby AL, Dwyer T, Cochrane J. Population trends in sud-den infant death syndrome.Semin Perinat.2002;26:296 –305 21. Mitchell EA, Tuohy PG, Brunt JM, et al. Risk factors for sudden
infant death syndrome following the prevention campaign in New Zealand: a prospective study. Pediatrics. 1997;100: 835– 840
22. Barry H, Paxson LM. Infancy and early childhood: cross-cultural codes 2.Ethnology.1971;10:466 –508
23. Young J.Night-Time Behaviour and Interactions Between Mothers and Their Infants of Low Risk for SIDS: A Longitudinal Study of
Room-Sharing and Bedsharing [PhD thesis]. Bristol, United Kingdom: University of Bristol; 1999
24. Ball HL. Triadic bed-sharing and infant temperature.Child Care Health Dev.2002;28:55–58
25. Baddock SA, Galland BC, Beckers MGS, Taylor BJ, Bolton DPG. Bedsharing and the infant’s thermal environment in the home setting.Arch Dis Child.2004;89:1111–1116
26. Waters KA, Gonzalez A, Jean C, Morielli A, Brouillette RT. Face-straight-down and face-near-straight-down positions in healthy, prone-sleeping infants.J Pediatrs.1996;128:616 – 625 27. Richard CA, Mosko SS, McKenna JJ. Apnea and periodic breathing in bed-sharing and solitary sleeping infants.J Appl Physiol.1998;84:1374 –1380
28. McKenna JJ, Mosko SS, Richard CA. Bedsharing promotes breastfeeding.Pediatrics.1997;100:214 –219
29. Pollard K, Fleming P, Young J, Sawczenko A, Blair P. Night-time non-nutritive sucking in infants aged 1 to 5 months: relationship with infant state, breastfeeding, and bed-sharing versus room-sharing.Early Hum Dev.1999;56:185–204 30. Ball HL. Parent-infant bed-sharing behaviour: effects of feeding
type, and presence of father.Human Nature.2006; In press 31. McCoy RC, Hunt CE, Lesko SM, et al. Frequency of bed sharing
and its relationship to breastfeeding. J Devel Behav Pediatr.
2004;25:141–149
32. Vogel A, Hutchison BL, Mitchell EA. Factors associated with the duration of breastfeeding. Acta Paediatr. 1999;88: 1320 –1326
33. Hoffman HJ, Hillman LS. Epidemiology of the sudden infant death syndrome: maternal, neonatal, and postneonatal risk factors.Clin Perinatol.1992;19:717–737
34. Ford RP, Taylor BJ, Mitchell EA, et al. Breastfeeding and the risk of sudden infant death syndrome.Int J Epidemiol.1993;22: 885– 890
35. Andersen M, Arnestad M, Rognum TO, Vege A. Crib death in the eastern regions of Norway 1984 –1992. A survey of risk factors.Tidssk Nor Laegeforen.1995;115:34 –37
36. McVea KL, Turner PD, Peppler DK. The role of breastfeeding in sudden infant death syndrome.J Hum Lact.2000;16:13–20 37. Ponsonby AL, Dwyer T, Kasl SV, Cochrane JA. The Tasmanian
SIDS Case-Control Study: Univariable and multivariable risk factor analysis.Paediatr Perinat Epidemiol.1995;9:256 –272 38. Fleming PJ, Blair PS, Bacon C, et al. Environment of infants
during sleep and risk of the sudden infant death syndrome: results of 1993–5 case-control study for confidential inquiry into stillbirths and deaths in infancy. CESDI Regional Coordi-nators and Researchers.BMJ.1996;313:191–195
39. Byard RW. Is breast feeding in bed always a safe practice?J Paediatr Child Health.1998;34:418 – 419
40. Bland JM, Altman DG. Statistical methods for assessing agree-ment between two methods of clinical measureagree-ment.Lancet.
1986;1:307–310
41. Abel S, Park J, Tipene-Leach D, Finau S, Lennan M. Infant care practices in New Zealand: a cross-cultural qualitative study.Soc Sci Med.2001;53:1135–1148
42. Ball HL. Reasons to bed-share: why parents sleep with their infants.J Reprod Infant Psychol.2002;20:207–222
43. Sawczenko A, Galland BC, Young J, Ring W, Fleming PJ. Night time mother- infant interactive behaviour and physiology: a longitudinal comparison of room sharing versus bedsharing (“co-sleeping”).Pediatr Pulmonol.1995;20:341
44. Scragg RK, Mitchell EA, Stewart AW, et al. Infant room-sharing and prone sleep position in sudden infant death syn-drome. New Zealand Cot Death Study Group.Lancet.1996;347: 7–12
46. Guilleminault C. Sleep apnea syndromes: impact of sleep and sleep states.Sleep.1980;3:227–234
47. Roehrs T, Merlotti L, Petrucelli N, Stepanski E, Roth T. Exper-imental sleep fragmentation.Sleep.1994;17:438 – 443 48. Ferrara M, De Gennaro L, Casagrande M, Bertini A. Auditory
arousal thresholds after selective slow-wave sleep deprivation.
Clin Neurophysiol.1999;110:2148 –2152
49. Kahn A, Groswasser J, Sottiaux M, Rebuffat E, Franco P. Mechanisms of obstructive sleep apneas in infants.Biol Neonate.
1994;65:235–239
50. Thomas DA, Poole K, McArdle EK, et al. The effect of sleep deprivation on sleep states, breathing events, peripheral che-moresponsiveness and arousal propensity in healthy 3 month old infants.Eur Respir J.1996;9:932–938
51. Franco P, Seret N, Van Hees JN, Lanquart JP Jr, Groswasser J, Kahn A. Cardiac changes during sleep in sleep-deprived in-fants.Sleep.2003;26:845– 848
52. Richard C, Mosko S, McKenna J, Drummond S. Sleeping po-sition, orientation, and proximity in bedsharing infants and mothers.Sleep.1996;19:685– 690
53. Skadberg BT, Markestad T. Infant behaviour in response to a change in body position from side to prone during sleep.Eur J Pediatr.1996;155:1052–1056
54. Mosko S, Richard C, McKenna J, Drummond S, Mukai D. Maternal proximity and infant CO2 environment during bed-sharing and possible implications for SIDS research.Am J Phys Anthropol.1997;103:315–328
55. Ball HL. Differences in bed-sharing behaviour among
breast-feeding and non-breastbreast-feeding families. 7th SIDS International Conference. Florence, Italy; 2002
56. Blair P, Fleming D, Smith IJ, Ward Platt M. Are risk factors for SIDS infants found sharing the parental bed different from those found in the cot? 7th SIDS International Conference. Florence, Italy; 2002
57. Campbell AJ, Bolton DPG, Williams SM, Taylor BJ. A potential danger of bedclothes covering the face.Acta Paediatr.1996;85: 281–284
58. Campbell AJ, Taylor BJ, Bolton DPG. Comparison of two methods of determining asphyxial potential of infant bedding.
J Pediatr.1997;130:245–249
59. Lewis KW, Bosque EM. Deficient hypoxia awakening response in infants of smoking mothers: possible relationship to sudden infant death syndrome.J Pediatr.1995;127:691– 699
60. Campbell AJ, Galland BC, Bolton DPG, Taylor BJ, Sayers RM, Williams SM. Ventilatory responses to rebreathing in infants exposed to maternal smoking.Acta Paediatr.2001;90:793– 800 61. Hafstrom O, Milerad J, Asokan N, Poole SD, Sundell HW. Nicotine delays arousal during hypoxemia in lambs.Pediatr Res.
2000;47:646 – 652
62. Brenner RA, Simons-Morton BG, Bhaskar B, Revenis M, Das A, Clemens JD. Infant-parent bed sharing in an inner-city population.Arch Pediatr Adolesc Med.2003;157:33–39 63. Morelli GA, Rogoff B, Oppenheim D, Goldsmith D. Cultural
variation in infants’ sleeping arrangements: questions of inde-pendence.Dev Psychol.1992;28:604 – 613
A NEW SLEEPING SICKNESS IS HAUNTING HIGHWAYS
“With a tendency to stare zombie-like and run into stationary objects, a new species of impaired motorist is hitting the roads: the Ambien driver. Ambien, the nation’s best-selling prescription sleeping pill, is showing up with regu-larity as a factor in traffic arrests, sometimes involving drivers who later say they were sleep-driving and have no memory of taking the wheel after taking the drug. In some state toxicology laboratories Ambien makes the top 10 list of drugs found in impaired drivers. Wisconsin officials identified Ambien in the bloodstreams of 187 arrested drivers from 1999 to 2004. And as more people are taking the drug – 26.5 million prescriptions in this country last year – there are signs that Ambien-related driving arrests are on the rise.”
Saul S.New York Times. March 8, 2006
DOI: 10.1542/peds.2005-1636
2006;117;1599
Pediatrics
Barry J. Taylor
Sally A. Baddock, Barbara C. Galland, David P.G. Bolton, Sheila M. Williams and
Compared With Cot Sleeping in the Home Setting
Differences in Infant and Parent Behaviors During Routine Bed Sharing
Services
Updated Information &
http://pediatrics.aappublications.org/content/117/5/1599
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/117/5/1599#BIBL
This article cites 57 articles, 10 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/breastfeeding_sub Breastfeeding
http://www.aappublications.org/cgi/collection/sids_sub SIDS
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2005-1636
2006;117;1599
Pediatrics
Barry J. Taylor
Sally A. Baddock, Barbara C. Galland, David P.G. Bolton, Sheila M. Williams and
Compared With Cot Sleeping in the Home Setting
Differences in Infant and Parent Behaviors During Routine Bed Sharing
http://pediatrics.aappublications.org/content/117/5/1599
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.