Nine-Year Follow-up of a Home-Visitation Program:
A Randomized Trial
WHAT’S KNOWN ON THIS SUBJECT: A number of studies have shown that home-visiting interventions can improve outcomes for children being raised in families that face multiple adversities. It is less clear how well these benefits are sustained over long periods.
WHAT THIS STUDY ADDS: The current study shows that the Early Start program of home visitation has benefits in terms of reducing child abuse, increasing parental competence, and improving childhood behavioral adjustment for up to 9 years, suggesting long-term benefits of home visitation.
abstract
OBJECTIVE:To evaluate the extent to which a home-visitation program (Early Start) had benefits for child abuse, child behavior, and parental- and family-level benefits to the 9-year follow-up.
METHODS:A randomized controlled trial in which 220 families receiv-ing Early Start were contrasted with a control series of 223 families not receiving the program. Families were enrolled in the program for up to 5 years. Outcomes were assessed at 6 months, annually from 1 year to 6 years, and at 9 years after trial entry.
RESULTS: Comparisons between the Early Start and control series showed that families in the Early Start program showed significant (P,.05) benefits in reduced risk of hospital attendance for uninten-tional injury, lower risk of parent-reported harsh punishment, lower levels of physical punishment, higher parenting competence scores, and more positive child behavioral adjustment scores. Effect sizes (Cohen’s“d”) ranged from 0.13 to 0.29 (median = 0.25). There were no significant differences (allPvalues..05) between the Early Start and control series on a range of measures of parental behavior and family outcomes, including maternal depression, parental substance use, intimate partner violence, adverse economic outcomes, and life stress.
CONCLUSIONS:The Early Start program was associated with small to moderate benefits in a range of areas relating to child abuse, physical punishment, child behavior, and parenting competence. There was little evidence to suggest that the Early Start program had benefits that extended to the level of parents or family overall. Pediatrics 2013;131:297–303
AUTHORS:David M. Fergusson, PhD, Joseph M. Boden, PhD, and L. John Horwood, MSc
University of Otago, Christchurch School of Medicine and Health Sciences, Christchurch, New Zealand
KEY WORDS
home visitation, randomized controlled trial, child abuse, child health
ABBREVIATION
SDQ—Strengths and Difficulties Questionnaire
This trial has been registered with the Australian New Zealand Clinical Trials Registry (identifier ACTRN1605000352606). www.pediatrics.org/cgi/doi/10.1542/peds.2012-1612
doi:10.1542/peds.2012-1612
Accepted for publication Oct 16, 2012
Address correspondence to David Fergusson, PhD, Christchurch Health & Development Study, University of Otago, Christchurch School of Medicine & Health Sciences, PO Box 4345, Christchurch, New Zealand. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:Dr Fergusson is a member of the Board of Directors of Early Start; and Dr Boden and Mr Horwood have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:Funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation, and the New Zealand Lottery Grants Board.
multiple challenges are at increased risks of a range of adverse outcomes in later life,1–15 which has led to inter-ventions to mitigate the risks faced by children born into these environments. One approach to addressing these is-sues has been intensive home-visiting programs, which provide families with young children with support, mentor-ship, and assistance with child-rearing and related family issues. These pro-grams include the Nurse Family Part-nership,16,17Healthy Families America,18,19 Healthy Start,20,21 Early Head Start,22,23 the Comprehensive Child Development Program,24–26 and Early Start.27,28 All of these programs have been evaluated by using randomized control designs but
findings from these trials have been mixed, with some programs showing benefits and others failing to show benefits.29,30In a recent review, Howard and Brooks-Gunn30 found that home-visiting programs had reported
bene-fits for a number of outcomes, including child abuse, child health care, quality of home environment, parenting, parental depression, and childhood cognitive skills.
A previous article reported the out-comes of a randomized trial of the New Zealand Early Start program,27,28which provides intensive home visiting to families facing multiple challenges. Home visiting is provided by trained family support workers with qual-ifications in nursing, teaching, or allied disciplines. Outcomes at 36-month follow-up showed that children in the Early Start series had higher rates of general practitioner contact (P,.05), higher rates of well-child care (P , .05), lower rates of hospital attendance for unintentional injury (P,.01), lower rates of parentally reported child abuse (P,.01), greater use of preschool ed-ucation (P , .05), more positive and less punitive parenting (P,.05), and
found for a series of outcomes relating to parental and family circumstances, including maternal depression, family violence, parental substance use, family material conditions, family income, and welfare dependence.
This article reports an analysis of a 9-year follow-up of the Early Start and control families. The aims of this anal-ysis were to examine the extent to which
1. Gains made by the Early Start series in health, child abuse, parenting, and behavioral and related out-comes at 36 months were sustained over the 9-year follow-up period.
2. There was evidence of benefits for parental behavior or family circum-stances of Early Start over the 9-year follow-up period.
METHODS
Overview of Research Design
The evaluation of the Early Start pro-gram used a randomized control design in which the outcomes of 220 families enrolled in the program were com-pared with the outcomes of 223 control families. Assessments were made at baseline, 6 months, annually from 1 year to 6 years, and then at 9 years after trial enrollment. Sample size was de-termined by the availability of funding for services provided to the Early Start series. The study design had the ethical approval of the Canterbury Ethics Committee. No adverse effects of the intervention were observed.
Client Recruitment, Randomization, and Sample Retention
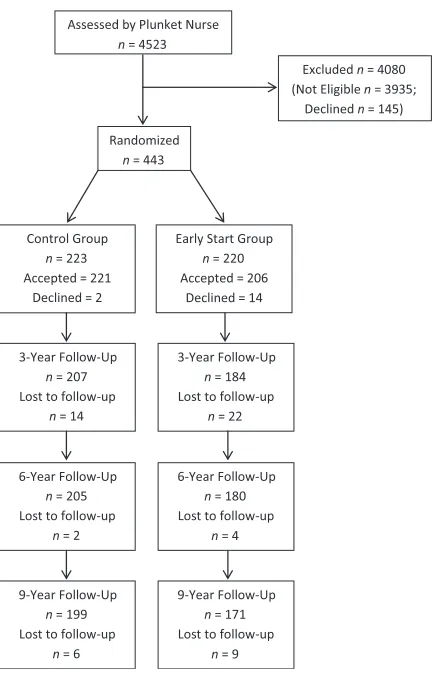
Trial recruitment took place over a 19-month period beginning in January 2000 during which Plunket nurses throughout the Christchurch area screened fam-ilies by using a procedure described in previous articles.27,31Figure 1 pro-vides a Consolidated Standards of
The figure shows that a total of 4523 families were seen by Plunket nurses. Of these families, 588 (13%) were deemed to be eligible for the trial on the basis of the screening criteria, and 443 (75%) agreed to participate.
At the point of referral to the trial, families were randomized to either Early Start or control series based on a computer-generated series of ran-dom numbers, and no blinding to as-signment was undertaken. Of the 443 families referred to the trial, 220 were assigned to the Early Start series and 223 to the control series. Families in the Early Start series were contacted by family support workers and invited to participate in the service, and were given an opportunity to try out the program for 1 month before actual enrollment. All families assigned to the Early Start service were studied, irre-spective of the result of the 1-month assessment. Control series families were contacted by survey interviewers and invited to participate, and paid NZD $50 per interview. Of those invited to participate in Early Start, 206 (96%) agreed to enter the service, whereas 221 (99%) in the control series agreed to participate in the trial. By 9 years, the drop-out rate in the Early Start group was 16% (35/220) compared with 11% (24/223) for the control group. At 9 years, 171 (78%) of the Early Start group was studied compared with 199 (89%) of the control group. These differences were statistically significant (P,.001) and largely attributable to the 14 fam-ilies who declined to enter Early Start and the trial.
Service Delivery
challenges, strengths, and resources; (2) development of a positive partner-ship between the family support worker and client; (3) collaborative problem solving to devise solutions to family challenges; (4) the provision of support, mentoring, and advice to assist client families to mobilize their strengths and resources; and (5) involvement with the family throughout the child’s preschool years. The Supplemental Information provides details of needs assessment, family support workers, client load, service goals, and service delivery principles.
Research Assessments
Participants in the trial were assessed at baseline, 6 months, annually from 1 year to 6 years, and at 9 years from trial enrollment, by using the following:
1. Client interviews. Client families were assessed on a structured in-terview administered in the clients’ homes by a trained survey inter-viewer. Interviews typically lasted between 45 minutes to an hour.
2. Medical record data. Parents were asked to give signed consent for the research group to access the hospital records for the child en-rolled in the study. More than 99% of parents provided this consent.
3. Teacher questionnaires. At 5, 6, and 9 years, teachers completed a ques-tionnaire about the child’s behav-ioral adjustment at school.
Measures Used in the Present Study
1. Hospital attendance for uninten-tional injury. Hospital attendance,
defined as attendance at an acci-dent and emergency department, or admission to a hospital, was obtained from local (Christchurch and the surrounding region) and national (New Zealand) hospital re-cords subject to the signed con-sent of the child’s parents. These records provided a complete list-ing of all hospital attendances for any study participant.
2. Harsh punishment/Parental use of physical punishment. Parents were interviewed on the Parent–Child
Con-flict Tactics Scale32 at each assess-ment from the 1- to 6-year follow-up and again at the 9-year follow-up. Two measures were constructed:
A measure of whether either parent used harsh or abusive punishment, which included shak-ing, hitting with an object, hitting with afist or kicking, grabbing by the neck/choking, hitting as hard as possible, burning/scalding, throwing/knocking down, and slapping on the head. A diversity score measure of the reported use of physical punish-ment, constructed by summing the number of different types of physical punishment methods reported by the parents over the follow-up periods of 1 to 3 years, 4 to 6 years, and 9 years.3. Parenting competence. This was mea-sured by the Parenting Scale,33a 30-item scale spanning a number of domains of parenting behaviors, in-cluding laxness of discipline, parental overreactions, and parental verbosity. Factor analysis showed that these items formed a unidimensional factor reflecting the extent of parenting competence.33 The scale reliability ranged froma= 0.82 to 0.83.
4. Child behavior (parent and teacher reports). Parent and teacher re-ports of child behavior problems
FIGURE 1
Consolidated Standards of Reporting Trials diagram of the screening, recruitment, and follow-up process for the Early Start program.
Difficulties Questionnaire (SDQ).34 The SDQ is a 30-item scale designed to assess a number of child behav-ior domains, including externalizing behaviors (conduct problems and hyperactivity/inattention) and inter-nalizing behaviors (emotionality and peer difficulties) during the 6 months before assessment. An overall score representing total
dif-ficulties was computed by summing the externalizing and internalizing behavior subscales; acoefficients for parent and teacher reports ranged from 0.70 to 0.85.
5. Maternal depression. This was assessed at the 5-, 6-, and 9-year follow-up by using questions from the Composite International Diag-nostic Inventory35measuring Diag-nostic and Statistical Manual of Mental Disorders, Fourth Edition36 symptoms of major depression. The measure of depressive symp-tomatology consisted of the total number of symptoms reported by participants in the 12 months be-fore each assessment point.
6. Parental substance use. This was assessed via 3 measures: (1) pa-rental cigarette smoking (for the month before assessment) at the 5-, 6-, and 9-year follow-up; (2) pa-rental alcohol problems, based on questions from the Composite In-ternational Diagnostic Inventory35 relating to Diagnostic and Statisti-cal Manual of Mental Disorders, Fourth Edition36 alcohol abuse/ dependence symptom criteria, in the 12 months before the 5-, 6-, and 9-year follow-up; and (3) pa-rental use of cannabis or other illicit drugs, since the previous as-sessment, at the 5-, 6-, and 9-year follow-up.
7. Family violence. Intimate partner violence was assessed for the 12
Conflict Tactics Scale.37This instru-ment measures the domains of minor psychological aggression, severe psychological aggression, minor physical assault, and severe physical assault.
8. Family economic circumstances. Family economic circumstances at the 5-, 6-, and 9-year follow-up were assessed via 3 measures: (1) whether either parent was in receipt of any welfare benefit at each point of as-sessment; (2) the total amount of debt reported by families at the time of each assessment; and (3) the number of hardship items en-dorsed by parents by using the Eco-nomic Living Standards Index.38
9. Family life stress. The family’s ex-posure to adverse life events in the previous 12 months was obtained at the 5-, 6-, and 9-year follow-up by using a 47-item questionnaire based on the Holmes and Rahe So-cial Readjustment Rating Scale.39
Statistical Analyses
The results in Tables 1 and 2 compare the Early Start and control series on outcomes assessed to 9 years, and summarize more extensive repeated measures data that are reported in the Supplemental Information. To test for differences between the Early Start and control groups, a unified analysis
measure:
fðYtÞ ¼B0þB1XþB2tþB3ðX:tÞ þ U ð1Þ
where Yt is the measure of the outcome Y observed at time t, X is a dichotomous variable representing treatment status (Early Start/control), and (X.t) is an in-teraction term. This model addresses 3 questions:
1. Treatment effects. The parameter B1 estimates the overall treatment difference in the outcome Y over the observation periods.
2. Time effects. The parameter B2 re-presents changes in the expected value of Y over time.
3. Time by treatment interaction. The parameter B3 represents the ex-tent to which any effects of treat-ment on the outcome Y varied with time.
This model was fitted by using population-averaged Generalized Esti-mating Equation methods. Effect sizes were obtained by computing Cohen’s d for the results pooled across the as-sessment periods. All tests of signifi -cance were 2-tailed.
To test for the multivariate effects of the intervention in Tables 1 and 2, multivariate tests of significance were conducted. The methods used are de-scribed in detail in the Supplemental Information.
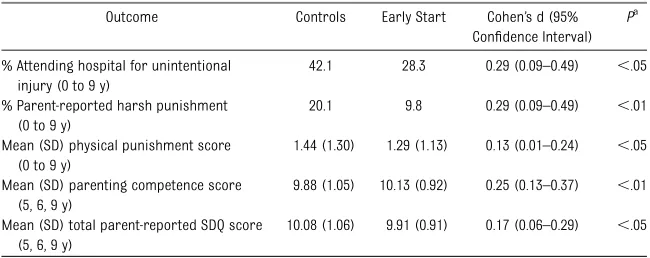
TABLE 1 Child Outcomes up to the 9-Year Follow-up
Outcome Controls Early Start Cohen’s d (95%
Confidence Interval)
Pa
% Attending hospital for unintentional injury (0 to 9 y)
42.1 28.3 0.29 (0.09–0.49) ,.05
% Parent-reported harsh punishment (0 to 9 y)
20.1 9.8 0.29 (0.09–0.49) ,.01
Mean (SD) physical punishment score (0 to 9 y)
1.44 (1.30) 1.29 (1.13) 0.13 (0.01–0.24) ,.05
Mean (SD) parenting competence score (5, 6, 9 y)
9.88 (1.05) 10.13 (0.92) 0.25 (0.13–0.37) ,.01
Mean (SD) total parent-reported SDQ score (5, 6, 9 y)
10.08 (1.06) 9.91 (0.91) 0.17 (0.06–0.29) ,.05
RESULTS
Child Outcomes up to the 9-Year Follow-up
Table 1 compares the Early Start and control series on measures assessed over the 9-year follow-up. In the inter-ests of brevity, this table reports the results to the 9-year follow-up. The Supplemental Information provides a more extensive account of the data on which Table 1 is based. The table shows that by the 9-year follow-up, children in the Early Start series had
1. Overall rates of hospital admission (28.3%) that were 33% lower than rates for the control series (42.1%; P,.05; d = 0.29).
2. Overall rates of parentally reported harsh punishment (9.8%) that were more than 50% lower than those for the control series (20.1%;P, .05; d = 0.29).
3. Pooled mean physical punishment scores (1.29) that were 0.13 SDs lower than those of the control se-ries (1.44;P,.05; d = 0.13).
4. Pooled mean parenting compe-tence scores (10.13) that were 0.25 SDs higher than those of the control series (9.88; P , .01; d = 0.25).
5. Pooled mean parentally reported total SDQ behavior scores (9.91) that were 0.17 SDs lower than the control series (10.08;P,.05; d = 0.17).
As shown in the Supplemental In-formation, for all comparisons there were no statistically significant treat-ment 3 time of measurement inter-actions. A multivariate regression analysis of the 5 outcomes showed that there was a statistically significant overall effect, X25= 22.56,P,.001.
The analysis in Table 1 was extended to consider teacher-reported measures of behavior over the period from 5 to 9 years. This analysis showed that there were no statistically significant differ-ences between the Early Start and control groups on teacher reports of overall SDQ scores.
Parental Behavior and Family Circumstances
Table 2 compares the Early Start and control groups on a series of measures of parent behavior and family circum-stances, including maternal depression, substance use, family violence, economic circumstances, and adverse life events assessed over the period from 5 to 9 years. In all cases, there were no signifi -cant differences (allPvalues..05) be-tween the Early Start and control groups. A multivariate regression analysis of the 5 outcomes showed that the joint effect of the 10 outcomes was statistically non-significant, X210= 6.30,P..70.
Analysis of Losses to Follow-up
As shown in Fig 1, losses to follow-up for the Early Start series (22%) were
substantially and significantly higher (P,.01) than losses to follow-up for the control series (11%). The principal reason for this was that 14 families randomized to Early Start declined to enter the service or participate in the evaluation.
To examine the effects of sample loss on trial validity, 2 analyses were con-ducted.
1. Comparison on baseline measures. The Early Start and control group members studied at the 9-year follow-up were compared on 35 measures assessed at the baseline assessment. These measures span-ned sociodemographic and ethnic background, economic circumstan-ces, maternal childhood disadvan-tage, maternal adjustment, and pregnancy and childbirth. This anal-ysis was extended to examine differ-ences between those who dropped out before the 9-year follow-up and those who did not drop out, in both the Early Start and control groups. In no case was a significant differ-ence observed between the treat-ment groups, or between those who dropped out before the 9-year follow-up and those who did not drop out, on the baseline measures (see Supplemental Information).
2. Imputation of missing data. In ad-dition, the data were reanalyzed by using a full intention-to-treat de-sign by imputing data for those participants not observed through-out the 9-year follow-up. This anal-ysis produced findings that were consistent with the analysis of the observed data in Table 1 (see Sup-plemental Information).
DISCUSSION
Thefindings of this 9-year assessment led to 3 general conclusions. First, significant benefits were observed for a number of child outcomes, includ-ing childhood hospital attendance for
TABLE 2 Parent and Family Outcomes From 5-Year to 9-Year Follow-up
Outcome Controls Early Start Pa
Mean (SD) depression symptoms 1.39 (2.97) 1.55 (3.12) ..20
% Reporting cigarette smoking 63.3 65.9 ..40
% Reporting alcohol problems 7.7 8.5 ..60
% Used cannabis/other illicit drugs 18.5 24.1 ,.10
Mean (SD) IPV victimization score 9.98 (0.84) 10.02 (1.15) ..60
Mean (SD) IPV perpetration score 9.99 (0.96) 10.01 (1.04) ..80
% Welfare dependent 56.8 59.5 ..50
Mean (SD) debt (in New Zealand dollars) 4492 (8524) 5248 (9140) ..20
Mean (SD) no. of hardship factors 3.46 (3.56) 3.52 (3.44) ..80
Mean (SD) adverse life events score 9.97 (0.98) 10.03 (1.02) ..40
IPV, intimate partner violence.
aTest of significance obtained from Generalized Estimating Equation model.
,
.05), punitive parenting (P,.05), pa-rental competence (P,.01), and pa-rentally reported child behavioral problems (P,.05). In all cases, tests of treatment3time of measurement interaction suggested that these ben-efits were sustained over the 9-year follow-up. Effect sizes (Cohen’s d) ranged from 0.13 to 0.29 with a median of 0.25.
Second, there was no evidence to sug-gest that Early Start had benefits for a range of parental behavior and family circumstances, including maternal de-pression, parental substance use, family violence, family income, family debt, and welfare dependence.
Third, the rate of sample attrition in the Early Start series was twice that of the control series. Tests of sample selection bias were conducted by (1) comparing the Early Start and control groups, and those observed and not observed at the 9-year follow-up on a series of 35 measures obtained at baseline; and (2) the use of imputation methods to pro-duce a full intention-to-treat analysis. Both approaches suggested that it was unlikely that differential sample
Thesefindings are consistent with the 36-month assessment27,31 and show that the child-related benefits of Early Start were sustained over the 9-year follow-up. As was the case with the 36-month follow-up, effect sizes were in the range of small to moderate. An important issue concerns the apparent failure of Early Start to produce change in parental behavior and family cir-cumstances. The reasons for this
finding are not clear; however, dis-cussions with Early Start staff suggest 3 reasons that conspired to reduce the effectiveness of the program in pro-ducing such changes. First, as refl ec-ted in the literature,40,41parents were often reluctant and resistant to seek treatment and advice for issues such as depression, substance abuse, and contraception. Second, the uptake of services was limited by the availability of services, in particular drug and al-cohol services. Finally, parents were often noncompliant with the advice with which they were provided, par-ticularly with budget advice. These 3 factors would appear to explain the reasons for the lack of success of Early
fi
and family-level change.
CONCLUSIONS
The results of this 9-year trial show that programs like Early Start can produce modest changes in outcomes relating to childhood well-being, including un-intentional injury, harsh discipline, parenting competence, and child be-havior; however, these benefits do not generalize to family-level change. In part, these results are likely to reflect the fact that Early Start, as well as other home-visiting programs with similar features, provide advice and mentor-ship but do not provide direct thera-peutic support. These considerations suggest that future directions in this area should involve the closer in-tegration of home-visiting services like Early Start into organizations providing health, educational, and behavioral support. Under ideal circumstances, home-visiting teams should be part of integrated organizations of medical practitioners, educationalists, and psy-chologists that provide integrated sys-tems of care and support for families facing multiple challenges.
REFERENCES
1. Farrington DP, Lambert S, West DJ. Criminal careers of two generations of family members in the Cambridge study in de-linquent development. Studies on Crime
and Crime Prevention. 1998;7(1):85–97
2. Heimer K. Socioeconomic status, subcul-tural definitions, and violent delinquency.
Social Forces. 1997;75(3):799–833
3. Lindstrom P. School violence: a multi-level perspective.Int Rev Victimol. 2000;8(2):141–58
4. Sourander A, Elonheimo H, Niemela S, et al. Childhood predictors of male criminality:
a prospective population-based follow-up study from age 8 to late adolescence. J Am Acad Child Adolesc Psychiatry. 2006;45 (5):578–586
5. Repetti RL, Taylor SE, Seeman TE. Risky
families: family social environments and
the mental and physical health of off-spring.Psychol Bull. 2002;128(2):330–366
6. Abdelrahman A, Rodriguez G, Ryan JA, French JF, Weinbaum D. The epidemiology
of substance use among middle school students: the impact of school, familial, community and individual risk factors.
J Child Adolesc Subst Abuse. 1998;8(1):55– 75
7. Brody GH, Stoneman Z, Flor D. Linking family processes and academic
compe-tence among rural African American youths.J Marriage Fam. 1995;57:567–579
8. Davis-Kean PE. The influence of parent education and family income on child
achievement: the indirect role of parental expectations and the home environment.
J Fam Psychol. 2005;19(2):294–304
9. De Civita M, Pagani L, Vitaro F, Tremblay RE. The role of maternal educational aspira-tions in mediating the risk of income
source on academic failure in children from persistently poor families.Child Youth
Serv Rev. 2004;26(8):749–769
10. Melby JN, Conger RD, Fang S-A, Wickrama
KAS, Conger KJ. Adolescent family experi-ences and educational attainment during
early adulthood. Dev Psychol. 2008;44(6): 1519–1536
11. Christoffersen MN, Poulsen HD, Nielsen A. Attempted suicide among young people:
risk factors in a prospective register-based study of Danish children born in 1966.Acta Psychiatr Scand. 2003;108(5):350–358
12. Gilman SE, Kawachi I, Fitzmaurice GM, Buka
the lifetime risk of major depression.Int J Epidemiol. 2002;31(2):359–367
13. Mcleod JD, Shanahan MJ. Trajectories of poverty and children’s mental health. J Health Soc Behav. 1996;37(3):207–220
14. Smart D, Hayes A, Sanson A, Toumbourou JW. Mental health and well-being of Aus-tralian adolescents: pathways to vulnera-bility and resilience. Int J Adolesc Med Health. 2007;19(3):263–268
15. Fergusson DM, Horwood LJ, Lynskey MT. The childhoods of multiple problem adolescents: a 15-year longitudinal study.J Child Psychol Psychiatry. 1994;35(6):1123–1140
16. Olds DL, Henderson CR Jr, Tatelbaum R, Chamberlin R. Improving the life-course development of socially disadvantaged mothers: a randomized trial of nurse home visitation.Am J Public Health. 1988;78(11): 1436–1445
17. Olds DL. Prenatal and infancy home visiting by nurses: from randomized trials to community replication.Prev Sci. 2002;3(3): 153–172
18. Daro D.Healthy Families America: A Guide for Evaluating Healthy Families America Efforts. Chicago, IL: National Committee to Prevent Child Abuse; 1994
19. Daro DA, Harding KA. Healthy Families America: using research to enhance prac-tice.Future Child. 1999;9(1):152–178
20. Duggan A, McFarlane E, Fuddy L, et al. Randomized trial of a statewide home vis-iting program: impact in preventing child abuse and neglect.Child Abuse Negl. 2004; 28(6):597–622
21. Duggan AK, McFarlane EC, Windham AM, et al. Evaluation of Hawaii’s Healthy Start Program. Future Child. 1999;9(1):66–90; discussion 177–178
22. Love JM, Kisker EE, Ross C, et al. The ef-fectiveness of early Head Start for 3-year-old children and their parents: lessons for
policy and programs.Dev Psychol. 2005;41 (6):885–901
23. Chazan-Cohen R, Ayoub C, Pan BA, et al. It takes time: impacts of early Head Start that lead to reductions in maternal depression two years later.Infant Ment Health J. 2007; 28(2):151–170
24. Goodson BD, Layzer JI, St. Pierre RG, Bernstein LS, Lopez M. Effectiveness of a comprehensive,five-year family support program for low-income children and their families:findings from the Comprehensive Child Development Program. Early Child Res Q. 2000;15(1):5–39
25. Anderson LM, Shinn C, Fullilove MT, et al; Task Force on Community Preventive Serv-ices. The effectiveness of early childhood development programs. A systematic review.
Am J Prev Med. 2003;24(suppl 3):32–46
26. St Pierre RG, Layzer JI. Using home visits for multiple purposes: the Comprehensive Child Development Program.Future Child. 1999;9(1):134–151
27. Fergusson DM, Grant H, Horwood LJ, Ridder EM. Randomized trial of the Early Start program of home visitation. Pediatrics. 2005;116(6). Available at: www.pediatrics. org/cgi/content/full/116/6/e803
28. Fergusson DM, Grant H, Horwood LJ, Ridder EM. Randomized trial of the Early Start pro-gram of home visitation: parent and family outcomes.Pediatrics. 2006;117(3):781–786
29. Gomby DS. Promise and limitations of home visitation.JAMA. 2000;284(11):1430–1431
30. Howard KS, Brooks-Gunn J. The role of home-visiting programs in preventing child abuse and neglect.Future Child. 2009;19(2): 119–146
31. Fergusson DM, Horwood LJ, Grant H, Ridder E. Early Start evaluation report. Christ-church: Early Start Project Ltd. Available at: www.otago.ac.nz/christchurch/otago014859. pdf. Accessed November 1, 2005
32. Straus MA, Hamby SL, Finkelhor D, Moore DW, Runyan D. Identification of child mal-treatment with the Parent-Child Conflict Tactics Scales: development and psycho-metric data for a national sample of American parents.Child Abuse Negl. 1998; 22(4):249–270
33. Arnold DS, O’Leary SG, Wolff LS, Acker MM. The Parenting Scale: a measure of dys-functional parenting in discipline sit-uations.Psychol Assess. 1993;5(2):137–144
34. Goodman R. The Strengths and Difficulties Questionnaire: a research note. J Child Psychol Psychiatry. 1997;38(5):581–586
35. World Health Organization. Composite In-ternational Diagnostic Interview (CIDI). Geneva, Switzerland: World Health Orga-nization; 1993
36. American Psychiatric Association. Di-agnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: Ameri-can Psychiatric Association; 1994
37. Straus MA, Hamby SL, Boney-McCoy S, Sugarman DB. The Revised Conflict Tactics Scales (CTS2). Development and pre-liminary psychometric data.J Fam Issues. 1996;17(3):283–316
38. Jensen J, Spittal M, Krishnan V.ELSI Short Form: User Manual for a Direct Measure of Living Standards. Wellington, New Zealand: Ministry of Social Development; 2005
39. Holmes TH, Rahe RH. The Social Readjust-ment Rating Scale.J Psychosom Res. 1967; 11(2):213–218
40. Morrissey-Kane E, Prinz RJ. Engagement in child and adolescent treatment: the role of parental cognitions and attributions. Clin Child Fam Psychol Rev. 1999;2(3):183–198
41. Gulliver A, Griffiths KM, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young peo-ple: a systematic review. BMC Psychiatry. 2010;10:113
DOI: 10.1542/peds.2012-1612 originally published online January 28, 2013;
2013;131;297
Pediatrics
Services
Updated Information &
http://pediatrics.aappublications.org/content/131/2/297
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/131/2/297#BIBL
This article cites 35 articles, 2 of which you can access for free at:
Subspecialty Collections
e_management_sub
http://www.aappublications.org/cgi/collection/administration:practic Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2012-1612 originally published online January 28, 2013;
2013;131;297
Pediatrics
David M. Fergusson, Joseph M. Boden and L. John Horwood
Nine-Year Follow-up of a Home-Visitation Program: A Randomized Trial
http://pediatrics.aappublications.org/content/131/2/297
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2013/01/23/peds.2012-1612.DCSupplemental
Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.