19
Int J Res Med. 2014; 3(2);19-26 e ISSN:2320-2742 p ISSN: 2320-2734Evaluation of wound dehiscence of midline laparotomy wounds on comparing
continuous interlocking and interrupted X-suturing methods of closure
Osman B. Belim
1*, Krunal Gohil
21,2
Associate Professor,Department of General Surgery, Medical College, Baroda
INTRODUCTION
Wound dehiscence carries with it a substantial morbidity. In addition there is an increase in the cost of care both in terms of increased hospital stay, nursing and manpower cost in managing the burst and its complications. Many patients in India have a poor nutritional status and the presentation of patients with peritonitis is often delayed in the emergency. This makes the problem of wound dehiscence more common1 and graver in our setting as compared to the West. Out of numerous etiological factors causing wound dehiscence, the technique of closure of abdomen and the sutures used are most important.1 Numerous studies have been conducted evaluating a variety of closure techniques and suture materials.2-4 The current opinion in the West centers around mass closure versus layered closer of the abdomen in both emergency and elective settings, as there is no *Corresponding Author
Dr. Osman B. Belim,
Associate Prof. Department of Gen. Surgery Medical College, Baroda
Email:- [email protected]
significant difference reported between the two, in most studies.5-13 While the choice may not be so important in elective patients who are nutritionally adequate, do not have any risk factor for dehiscence and are well prepared for surgery, however it may prove crucial in emergency patients who often have multiple risk factors for developing dehiscence14 and the strangulation of the sheath is the proverbial last straw in precipitating wound failure. A new “Interrupted „X‟ technique” was developed to circumvent the problem of cutting out effect of a continuous suture. Here, its clinical usefulness is tested in a randomized trial of midline laparotomy wound closure.
MATERIALS AND METHODS
Randomized study was conducted on 134 patients(87 male and 47 female) of midline vertical laparotomy wounds carried out in surgical ward of Sir Sayajirao General Hospital Baroda from August‟ 2009 to September „2010. Amongst which 94patients (71 male and 23 female)underwent emergency laparotomy out of which 54 patient‟s abdomen were closed by continuous interlocking and 40 patients by interrupted „X‟ arm suturing.
ORIGINAL ARTICLE
ABSTRACT
BACKGROUND: The quest for the best closure technique for abdominal incisions continues. The surgeon‟s Endeavour is to eliminate consequences of wound failure and wound dehiscence in the acute form, and incisional hernia as the late manifestation. To achieve this goal, several modifications in opening the abdomen and closing the wound have been tried. There are many studies in the literature comparing various methods of wound closure, with conflicting results. Three meta-analyses of these studies have been performed, which have been successful in resolving many of the issues. A Meta-analysis done in1981,favors interrupted method of closer over continuous closure technique; while a meta-analysis conducted in 1992 comparing continuous versus interrupted closure method favors continuous method. A third meta-analysis in1986, has not found any significant difference between these two methods. However, there is still no consensus over continuous versus interrupted methods of wound
closure. MATERIALS AND METHODS: 134 cases of midline laparotomy done in Surgical ward of Sir
Sayajirao General Hospital, Baroda from August‟2009 to September‟2010 were included in this study to analyze the incidence, risk and co-morbid factors of Burst abdomen amongst the two methods of sheath closure viz: continuous interlocking v/s interrupted x-suture method. RESULTS: In emergency group, 25.9% burst were in continuous interlocking and 5% in X suturing, a significant difference. In elective group, bursts were 4.7% in continuous and 0% in X arm, not significant. For age& sex in both groups and other co morbid factors in emergency group, no significant difference was found amongst two methods but relative risk of bursts were higher
in continuous interlocking. CONCLUSION: In emergency setting, incidence of burst can be reduced
using„X‟closure in presence of all predictors of dehiscence. In cases of elective surgeries, continuous interlocking closure gives satisfactory results.
Keywords: Laparotomy wound dehiscence, burst abdomen, continuous interlocking method and X suturing
20
Int J Res Med. 2014; 3(2);19-26 e ISSN:2320-2742 p ISSN: 2320-2734 While 40 patients (16 male and 24 female)underwent elective laparotomy out of which 24 patient‟s abdomen were closed by continuous interlocking and 16 patients by interrupted „X‟ arm suturing. The patients‟ of age < 18 years, previous laparotomy cases and patients who died before developing wound dehiscence have been excluded from this study. All patients were given explanation of the study and signed a written consent form. They were randomized to undergo either continuous interlock or interrupted closure of the laparotomy incision. The randomization codes determined by a table of random numbers were kept in sealed numbered envelopes which were opened once a patient was deemed suitable for inclusion in the study. Continuous interlocking closure: It is performed using No.1 Prolene suture (Polypropylene; Ethicon), care being taken to place each bite 1.5 to 2 cm from the linea alba edge and successive bites being 1 cm from each other. The edges of line alba were gently approximated without strangulation with an attempt to keep a suture to wound length ratio of 4:1
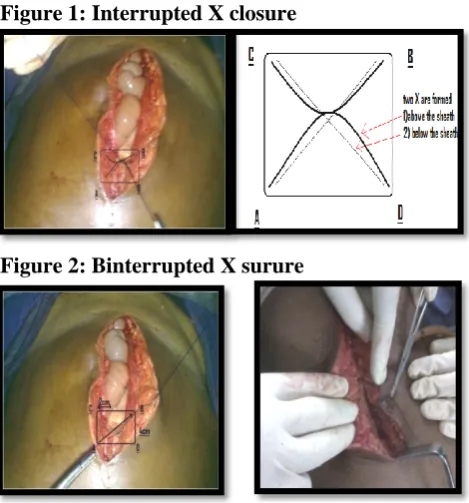
Figure 1: Interrupted X closure
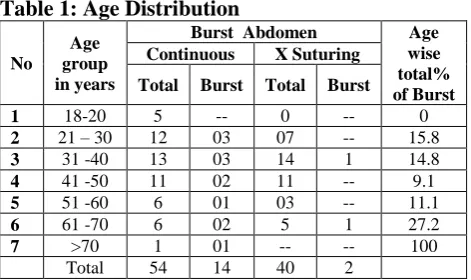
Figure 2: Binterrupted X surure
It is performed by using No. 1prolene suture, Imagine four points on linea alba edges: A, B, C, D each point is 2 cm away from linea alba edge and distance between A-C or B-D is 4 cm.Large bite is taken outside-in, 2 cm from the cut edge of linea alba. The needle emerges on the other side from inside out diagonally 2 cm from the edge and 4 cm above or below the first bite. This strand is crossed or looped around the free end of suture, so needle end of suture will be at “C” point and free end will be at “D” point, continued outside-in diagonally at 90 degree to the first diagonal. Continued outside-in, diagonally at 90 degree to the first diagonal. The
two ends were tied just tight enough to approximate the edges of linea alba taking care not to include bowel or omentum between the edges. The next X- suture is placed 1 cm away from the previous one. This creates two X like crosses-one on the surface and another deep to linea alba.
Mathematical considerations of stresses on abdominal wall.
21
Int J Res Med. 2014; 3(2);19-26 e ISSN:2320-2742 p ISSN: 2320-2734 abdominal girth >2 centimeter), Cough, Jaundice(S.bilirubin>2mg%). RESULTS
A total 134 patients were evaluated in this study. Amongst his 94 patients were of emergency laparotomy group, while 40 patients of elective laparotomy group. The following results were observed as follows:
Table for comparing abdominal dehiscence
Continuous interlocking
X suturing P value
Relative risk
% Burst total %Burst total
Emergency
Group 25.91 54 5 40 0.01
5.2
Elective
Group 4.1 24 0 16
Emergency Setting
Method Burst No Burst Total
Continuous locking 14 40 54
X suturing 2 38 40
Total 16 78 94
In emergency setting, out of 94 patients, in 54 patient‟s continuous interlocking method of suturing and in 40 patients X suturing method were applied after randomized distribution. In this study, 14 out of 54 wound dehiscence in continuous group and only 2 patients out of 40 in X suturing group had developed dehiscence. In emergency group, 25.9% bursts were present amongst continuous group and only 5% in X suturing. Thus in X suturing method chances of burst reduces approximately 5 times lesser than that of continuous interlocking method in this study.
In Elective Surgery
Method Burst No Burst Total
Continuous locking 1 23 24
X suturing 0 16 16
Total 1 39 40
Now in 40 patients of elective laparotomy group, 24 in continuous interlocking method and 16 were in „X‟ suturing method, after randomization. Amongst these laparotomies, only single patient of continuous arm group had developed burst. No patient in X suturing method had developed wound dehiscence.Applying statistical analysis on this data; Chi-square test=0.616 DF=1 And 25.9% bursts were present amongst continuous group and only 5% in X suturing. So, P=0.01 suggest significant difference was found amongst these two methods of closure.(P<0.05) So the impression is that, in emergency group X suturing is more effective than continuous method, while in elective surgeries continuous method gives comparable result. In this study youngest patient‟s age is 20 year and oldest patient age is 75 year. In emergency group, in continuous interlocking method mean age group was 38.5 + 16.5; and in interrupted X suturing method mean age group was 39.6+16.4. While in elective group, in continuous interlocking method
mean age group was 41.2+ 14.8; and in interrupted X suturing group mean age was 40.8 + 15.2. In both this group, for age distribution p value is > 0.05, so not significant. The predictors were mainly studied in emergency laparotomies, as they were eliminated before doing planned /elective laparotomy.
1). Age and Sex Distribution Table 1: Age Distribution
No
Age group in years
Burst Abdomen Age
wise total% of Burst Continuous X Suturing
Total Burst Total Burst
1 18-20 5 -- 0 -- 0
2 21 – 30 12 03 07 -- 15.8
3 31 -40 13 03 14 1 14.8
4 41 -50 11 02 11 -- 9.1
5 51 -60 6 01 03 -- 11.1
6 61 -70 6 02 5 1 27.2
7 >70 1 01 -- -- 100
Total 54 14 40 2
In this study youngest patient is 20 years old and oldest patient age is 75 years. In emergency group, in continuous interlocking method mean age group was 38.5 + 16.5; and in interrupted X suturing method mean age group was 39.6+16.4. While in elective group, in continuous interlocking method mean age group was 41.2+ 14.8; and in interrupted X suturing group mean age was 40.8 + 15.2. In both this group, for age distribution p value is > 0.05, so not significant. The only burst which was noticed in elective group was of 65 years of age. In emergency laparotomies, maximum burst-27.2% was observed in 61-70 year. Amongst this age group 2/6 patients in continuous arm and 1/5 patients in „X „suturing arm had developed burst. Distribution of patients in this age group in both the methods is almost same (P= 0.5, >0.05 so not significant) [in > 70 year age group only single patient was there who had burst ,so not taken in to consideration] (b) Sex distribution : The next table (table-2) shows the sex distribution of the patients of my study.
Table 2: Sex Distribution
Sex Burst No Burst Total
Male C(n= 43) X(n=28)
11 1
32 27
71
Female C(n=11) X(n=12)
03 1
8 11
23
Total 16 78 94
22
Int J Res Med. 2014; 3(2);19-26 e ISSN:2320-2742 p ISSN: 2320-2734 continuous method and 1/12 wound dehiscencewere noted. For emergency group, RR=0.97. No significant difference in wound dehiscence in this study.
2). Burst abdomen and anemia
Method Anemic (n=35) Non Anemic
(n=19) Total
Burst No Burst Burst No Burst
C 13 22 1 18 54
Method Anemic (n=32) Non Anemic
(n=8) Total
Burst No Burst Burst No Burst
X 2 30 0 8 40
Out of total 94 emergency laparotomies total 67 patients were found to be anemic. Amongst them, 13/35 wound dehiscence in continuous suturing and 2/32 wound dehiscence were noted in X suturing methods. For distribution of anemia in both groups, applying chi-square test, P=0.10 (>0.05), no significant difference was found. Thus in both the methods almost equal amount of anemic patients were present. Comparing the risk of burst between these two methods of suturing, relative risk, RR~6, that is 6 times higher chances of burst in anemic patient in continuous interlocking method group. In rest of the non anemic patients in both the methods, only 1wound dehiscence out of 19 in continuous suturing and none wound dehiscence in X suturing methods were noted.
3). Burst and Malnutrition
Method Malnutrition (n=46) Non Malnutrition (n=8) Total
Burst No Burst Burst No Burst
C 13 33 1 7 54
Method Malnutrition (n=36) Non Malnutrition (n=4) Total
Burst No Burst Burst No Burst
X 2 34 0 4 40
Total 82 patients were found malnourished in emergency setting out of 94 patients. Amongst them, 13/46 wound dehiscence in continuous method and 2/36 patients in X suturing group had developed wound dehiscence. For distribution of malnutrition in both groups, P=0.4 (>0.05), which is not significant. Calculating the risk of burst in malnourished patients comparing the two methods, RR~5, malnourish patient is having 5 times higher chance of burst in continuous arm group , in this study. In rest of the adequately nourished patients, only single burst was noted out of 8 patients in continuous interlocking method and no wound dehiscence in interrupted X suturing.
4). Burst and Diabetes
Method Diabetes (n=2) Non Diabetes
(n=52) Total
Burst No Burst Burst No Burst
C 1 1 12 39 54
Method Diabetes (n=5) Non Diabetes
(n=35) Total
Burst No Burst Burst No Burst
X 1 4 1 34 40
Only 7 patients out of 94 were diabetic in emergency group. Amongst them, 1/2 in continuous method and 1/4 wound dehiscence in X suturing methods were noted. For diabetic patients distribution in both the methods, P=0.10, so no significant difference.As we have only 7 diabetic patients in our study group, the statistical analysis amongst them is not possible.
5). Burst and Jaundice
Method Jaundice (n=1) Non Jaundice
(n=53) Total
Burst No Burst Burst No Burst
C 0 1 14 39 54
Method Jaundice (n=2) Non Jaundice
(n=38) Total
Burst No Burst Burst No Burst
X 0 2 2 36 40
Only 3 patients were having jaundice out of 94. And none of them had developed burst. For jaundice distribution, 1 out of 54 patients in continuous and 2 out of 40 patients in X suturing were having jaundice. P=0.3(>0.05) which is not significant. Here also only 3 jaundiced patients in study group so statistical analysis is not applied.
6). Burst abdomen and Intra abdominal sepsis
Method Pyoperitoneum (n=25)
Non Pyoperitoneum
(n=29)
Total
Burst No Burst Burst No Burst
C 12 13 2 27 54
Method Pyoperitoneum (n=27)
Non Pyoperitoneum
(n=13)
Total
Burst No Burst Burst No Burst
X 2 25 0 13 40
In this study, out of 94 patients 52 laparotomy cases were having pyoperitoneum as intra operative finding. Amongst them 12/25 wound dehiscence in continuous method and 2/27 wound dehiscence in X suturing method were noted. For pyoperitoneum distribution in both the groups, P=0.12(>0.05).No significant difference for its distribution in both the groups was found. For comparison of both the methods in pyoperitoneum cases, RR~6, thus 6 times higher risk of burst in continuous arm group. While in 42 laparotomies without pyoperitoneum, 2 /29 wound dehiscence in continuous locking method were noted and no wound dehiscence in interrupted X suturing group.
7). Burst abdomen and abdominal distension
Method Distension (n=30) Non Distension
(n=24) Total
Burst No Burst Burst No Burst
C 14 16 0 24 54
Method Distension (n=23) Non Distension
(n=17) Total
Burst No Burst Burst No Burst
X 2 21 0 17 40
23
Int J Res Med. 2014; 3(2);19-26 e ISSN:2320-2742 p ISSN: 2320-2734 abdominal distention in both suturing method,P=0.13(>0.05), which is not significant. Thus in this study, All the cases of dehiscence of the abdominal wound had abdominal distension. Comparing the two methods in post operative abdominal distention cases, RR~5, thus X suturing here also is an effective method in preventing burst. In rest of post operative 41 patients without abdominal distention none have developed wound dehiscence in both the methods of closer.
8). Burst abdomen and Coughing
Method Cough (n=27) Non Cough (n=27) Total
Burst No Burst Burst No Burst
C 12 15 2 25 54
Method Cough (n=24) Non Cough (n=16) Total
Burst No Burst Burst No Burst
X 2 22 0 16 40
Out of 94 patients 51 patients were having post operative coughing, and 12/27 wound dehiscence in continuous suturing and 2/22 wound dehiscence in X suturing method were noted. For cough distribution in two groups, P=0.33 (>0.05), which is not significant. Risk of developing burst RR~5, 5 times higher chances of burst in continuous suturing method. In rest of 43 laparotomies without post operative coughing, only 2/27 wound dehiscence were noted in continuous method.
Other Findings :
Post op day Number of brust %
1 -- --
2 -- --
3 1 5.8
4 2 11.7
5 7 41.7
6 4 23.5
7 2 11.7
>7 1(elective lap.) 5.8
Up to 4 weeks 17 100
[For both emergency and elective group]: Most number of bursts abdomen in this study were observed: 5th post operative day (43.7%), followed by 6th post operative day 23.5%.
Time and suture utilized in both the methods :
Continuous
Locking X Suturing
Average wound
length 15.5cm 15.3cm
Time utilized for
10 cm wound 6.3 min 6.4 min
[For average wound length: it is the length of wound which is closed by single full length suture material (70 cm), where full length single or more than one suture material utilized in each group. And 2nd is average time utilized for closer of 10 cm length wound in each group.]
So no significant difference in time and material utilized for closer in both the methods. Operative Details The specific details of each operative procedure were noted in the form of: Operative indication
Length of the laparotomy incision (in centimeter)
Intra operative findings (eg; absence or presence of intra peritoneal sepsis)
Procedure done
Length of the wound (linea Alba) closed by single suture material in each method (where full length 1 or more sutures are utilized) Time utilized for 10 cm length wound closer and total time for wound closer in both the methods (in minutes)
Post-Operative Surveillance
Post operative patients routine blood investigations, patients weight in kilogram and height in meter was noted. Respiratory system evaluation was done.
Base line abdominal girth was noted after patient had been shifted in surgical wards at the umbilical level. Followed by daily 8 am, 3 pm and 8 pm abdominal girth monitoring.
In this study, a burst was considered present, when intestine, omentum or other viscera were seen in the abdominal wound. For that daily wound examination was done in the morning at 8 am. In the post-operative period the wounds were observed daily until discharge and subsequently in the outpatient department at least weekly after discharge for one month. The End point of the study was considered on the day when patient has developed burst. DISCUSSION
The present study is a Randomized study of 140 cases of midline vertical laparotomy wounds carried out in the Department of General Surgery, Sir Sayajirao General Hospital & Baroda Medical College during a period of 13 months from 1stAugust 2009 to 30th September 2010. A total of 140 cases of mid line vertical laparotomies are taken in this study. Amongst these, 6 patients had expired just after laparotomy before developing wound dehiscence, so these cases have been excluded. So 134 patients were evaluated in this study. Amongst which 94 patients were of emergency laparotomy cases, while 40 patients were of elective laparotomy cases. In emergency group 71 male and 23 female patients and in elective group 16 male and rest 14 patients were female.
24
Int J Res Med. 2014; 3(2);19-26 e ISSN:2320-2742 p ISSN: 2320-2734 age distribution p value is > 0.05, so not significant.The maximum number of burst-27.2% were observed in 61-70 years of age group. Amongst the patients who had abdominal dehiscence, the average age group was 45.6 years with the range of 22 years to 75 years. Studies have shown that advanced age (more than 50-65 years) is associated with increased incidence of burst abdomen. Moreover advanced age is associated with co-morbid illnesses which in itself increase the risk. There were a total of 100 patients in emergency group and 110 in elective laparotomy group. The average age of the total sample was 38.06 with a median age of 32 and a standard deviation of 15.209. The age range was from 18 years to 75 years. One patient died soon after the operation. In the study, by Srivastavet al, Fifty-four patients were randomized into the continuous arm and 46 to the interrupted arm. The average age of the patients in the continuous arm was 36.37 years and in the interrupted arm it was 40.09 years. Nine abdominal wound dehiscence were noted in the emergency group. Their average age was 34.4 years with a range of 26 to 61 years. (b) Sex Distribution: In our study, 12 out of 71 males (16.9%) and 4 out of 23 females (17.3%) patients had developed burst, with RR=0.97. In elective group the only patient who has developed burst was 65 year male patient. In emergency group, out of 71 males, 11/43 wound dehiscence in continuous method and 1/28 wound dehiscence were noted. While out of 23 females, 3/11 wound dehiscence in continuous method and 1/12 wound dehiscence were noted. In study, which was conducted in AIIMS, by Dr.Srivastav et al, 5 out of 75 males(6.67%) and 4 out of 25 females(16%) had developed burst in it.
Male Female
Present study 16.9% 17.3%
Dr. Srivastav et al (2004)48 6.67% 16%
Prevalence in males is twice when compared to females in many reviews. But in our study no significant difference was found for sex distribution. (B) Burst abdomen and anemia: In this study out of total 94 emergency laparotomies total 67 patients were found to be anemic. Amongst them, 13/35(37.1%) wound dehiscence in continuous suturing and 2/32 (6.25%) wound dehiscence were noted in X suturing methods. For distribution of anemia in both groups, applying chi-square test, P=0.10(>0.05), no significant difference was found . Thus in both the methods almost equal amount of anemic patients were present. Comparing the risk of burst between these two methods of suturing, relative risk, RR~6, that is 6 times higher chances of burst in anemic patient in continuous interlocking method group. In rest of the non anemic patients in both the methods, only 1wound dehiscence out of 19 in continuous suturing and
25
Int J Res Med. 2014; 3(2);19-26 e ISSN:2320-2742 p ISSN: 2320-2734 were noted and no wound dehiscence in interruptedX suturing group. In this study 12 out of 25 patients in continuous group and 2 out of 27 patients in „X‟ suturing having pyoperitoneum have developed burst. RR~6. So X suturing is proved to be an effective method in this study in patient having pyoperitoneum. Study conducted in AIIMS, Srivastav et al shows RR~2. (G) Burst abdomen and abdominal distension (Increase in abdominal girth>2cm): Post operative abdominal distention was noticed in 53 patients out of 94 emergency laparptomies. Amongst them 14/30 wound dehiscence in continuous method and 2 / 23 wound dehiscence in X suturing method were present. For distribution of abdominal distention in both suturing method, P=0.13(>0.05), which is not significant. Thus in this study, all the cases of dehiscence of the abdominal wound had abdominal distension. Comparing the two methods in post operative abdominal distention cases, RR~5, thus X suturing here also is an effective method in preventing burst. In rest of post operative 41 patients without abdominal distention none have developed wound dehiscence in both the methods of closer. The study, conducted in AIIMS, Srivastavet al, had also abdominal distention in all burst cases, with RR~4. (H) Burst abdomen and Coughing: Out of 94 patients 51 patients were having post operative coughing, and 12/27 wound dehiscence in continuous suturing and 2/22 wound dehiscence in X suturing method were noted. For cough distribution in two groups=0.33(>0.05), which is not significant. Risk of developing burst RR~5, 5 times higher chances of burst in continuous suturing method. In rest of 43 laparotomies without post operative coughing, only 2/27 wound dehiscence were noted in continuous method. (I) Time and material utilized in both the method is almost same, no significant difference is noticed Other Studies: 1. Dr. AnuragSrivastav et al has conducted a
similar comparative study in AIIMS, Delhi, in department of surgery. Burst abdomen occurred in 1/46 = 2.17% in the interrupted „X‟ suturing group and in 8/54 = 14.8% in the continuous group.
2. In the second related study, by Dr.Mishra et al in 2002, Total 105 patients of > 11 years of age group, underwent either elective or emergency midline vertical laparotomies, were included in this study. In this study 6/53 (11.3%) wound dehiscence in „X‟ suturing and 14/52 (26.9%) wound dehiscence in continuous far and near suturing were noticed.(OR=0.347 ; p=0.042) but here in continuous arm group they have kept continuous far and near suturing as control group.
3. A randomized controlled trial by Dr.Mishra S
et al,in 2003, compares continuous mass closure and interrupted „X‟ suture with polypropylene in 240 patients undergoing emergency as well as elective laparotomy for gynecological procedures. They have noticed 1/160(0.62%) wound dehiscence in „X‟ suturing group and 11/80 (13.75%) burst in continuous arm group. (OR=0.039;p=0.0001)
Continuous Method
X Suture Method
Present study 25.9% 5%
DrSrivastav et al
(2004)48 14.8% 2.17%
Dr Mishra et al
(2002)40 26.9% 11.3%
Dr Mishra S et al
(2003)40 13.75% 0.62%
From this data, it can be concluded that interrupted X suturing is superior to continuous suturing of variety of configuration in preventing wound dehiscence
CONCLUSION
In emergency group, 25.9% burst were in continuous interlocking and 5% in X Suturing, a Significant difference. In elective group, bursts were 4.7% in continuous and 0% in X arm, not significant. For age& sex in both groups and others co morbid factors in emergency group, no significant difference were found amongst two methods but relative risk of bursts were higher in continuous interlocking. In emergency, burst can be reduced using„X‟closure and in presence of all predictors of dehiscence. In elective, Continuous interlocking closure gives satisfactory results. REFERENCES
1. Shukla HS, Kumar S, Misra MC, Naithani YP. Burst abdomen and suture material: a comparison of abdominal wound closure with monofilament nylon and chromic catgut. Indian J surg 1981;43:487-91
2. Dudley HAF. Layered and mass closure of the abdominal wall. Br J Surg 1970; 57:664-7. 3. Jenkins TPN. The burst abdominal wound: a
mechanical approach. Br J Surg 1976;63:873-6. 4. Jones TE, Newelle ET, Brubaker RE. The use
of alloy steel wire in closure of the abdominal wounds. SurgGynaecolObstet 1941; 72:1056-9. 5. Irvin TT. Wound repair. Closure of the
abdominal wound. Ann R CollSurg Eng1 1978; 60:224-6.
6. Ellis H, Bucknall TE, Cox PJ. Abdominal incisions and their closure. CurrProbSurg 1985; 22:1-51.
26
Int J Res Med. 2014; 3(2);19-26 e ISSN:2320-2742 p ISSN: 2320-2734 8. Singh A, Singh S, Dhaliwal US, Singh S.Technique of abdominal wall closure: a comparative study. Ind J Sur g 1981; 43:785-90.
9. Trimbos JB, Smit IB, Holm JP, Hermans J. A randomized clinical trial comparing two methods of fascia closure following midline laparotomy. Arch Surg 1992; 127; 1232-4. 10. McNeill PM, Surgerman HJ. Continuous
absorbable vs. interrupted no absorbable Facial closure. A prospective, randomized comparison. Arch Surg 1986;121:821-3.
11. Colombo M, Maggioni A, Parma G, Scalambrino S, Milani. A randomized comparison of continuous versus interrupted mass Closure of midline incisions in patients with gynecologic cancer. ObstetGynecol 1997; 89:684-9.
12. Br olin RE. Prospective randomized evaluation of midline fascial closure in gastric bariatric operations. Am J Surg 1996; 172: 328-331. 13. Choudhary SK, Choudhary SD, Mass closur e
versus layer closure of abdominal wound: a prospective clinical study. J Indian Med Assoc 1994; 92:229-32.
14. Niggebrugge AH, HansenBE, Trimbos JB, Van de Velde CJ, Zwaveling A, Mechnical Factors influencing the incidence of burst abdomen. Eur J Surg 1995; 161:655-61.
15. Zelen M. A new design for randomized clinical trials. N Engl J Med 1979; 300:1242-5.
16. Thomas GB, Finney RL. Vectors. In: Calculus and analytic geometry.6th edn. USA: Addison-Wesley Publishing Company Inc; 1993. pp. 697-58.
17. Shigley EJ, Mischke CR. Mechanical engineering design. 5th edn. New York: McGraw-Hill International; 1989. pp. 60 18. Bowen A: Postoperative wound disruption and
evisceration: An analysis of 34 cases with a review of literature. Am J Surg 1940; 47:3. 19. Poole GV Jr. Mechanical factors in abdominal
wound closure: the prevention of fascialdehiscence . Surgery, 1985; 97:631. 20. Webster C, Neumayer L, Smout R, et al.