Renata Jabłońska¹, Robert Ślusarz¹, Agnieszka Królikowska¹,
Joanna Rosińczuk-Tonderys²
Oswestry
Disability Index as a Tool to Determine Agility
of the Patients After Surgical Treatment
of Intervertebral Disk Discopathy
Kwestionariusz Oswestry jako narzędzie oceny sprawności chorych
po chirurgicznym leczeniu przepukliny krążka międzykręgowego
1 Department of Neurological and Neurosurgical Nursing Collegium Medicum in Bydgoszcz,
Nicolaus Copernicus University in Torun, Poland
² Department of Nervous Diseases, Wroclaw Medical University, Poland
Abstract
Background. The Oswestry Disability Index is the most commonly used scale to determine the agility of patients with intervertebral disk discopathy of the spinal column. This tool includes daily-life problems, important during near-surgical times to individual functioning of the patients.
Objectives. To carry out an estimation of agility of the examined patients after performing operational treatment of lumbar or cervical discopathy.
Material and Methods. Evaluations have been performed on a group of 188 patients, operated on because of lum-bar or cervical discopathy of the spinal column, by the Neurosurgery Department of University Hospital number 2 in Bydgoszcz. A prospective plan of examination with a three-time estimation was carried out using the Oswestry
Disability Index. Gathered material was statistically edited to verify the hypothesis at the level of significance of p < 0.05.
Results. In individual estimations, the number of people who have a minimal handicap was increasing – it increased by 6.4% and after that by 41.3% (p < 0.05). The greatest improvement was seen in the extent of pain (decreased by 1.79 points), object lifting (decreased by 1.14 points), and travel (decreased by 1.09 points). In the case of lumbar discopathy, 73 of the examined (38.8%) before surgery qualified for group II. After the surgery, in the first estima-tion, there were 80 patients (42.6%) in this group, while in the third, the majority were qualified in group I (40%) and in group II (23.6%) (r = 0.5147, p < 0.05, i.s.). Significant improvement also happened in those examined with type C discopathy (r = 0.3767, p < 005).
Conclusions. 1. Before surgery, the majority of the examined shows a moderate handicap of functional compe-tence. 2. After neurosurgery, on the day of discharge, the functional state had minimally improved. Statistically significant improvement happened long after the treatment. 3. It was observed that improvement in the agility of the examined applies to the people with intervertebral disk discopathy at the cervical segment as well as lumbar of the spinal column (Adv Clin Exp Med 2011, 20, 3, 377–384).
Key words: discopathy, agility, Oswestry Disability Index.
Streszczenie
Wprowadzenie. Kwestionariusz Niepełnosprawności Oswestry jest najczęściej stosowaną skalą do oceny sprawno-ści pacjentów z przepukliną krążka międzykręgowego kręgosłupa. To narzędzie, które uwzględnia problemy życia codziennego, istotne w okresie okołooperacyjnym dla samodzielnego funkcjonowania pacjentów.
Cel pracy. Dokonanie oceny sprawności badanych po przeprowadzonym leczeniu operacyjnym dyskopatii lędź-wiowej lub szyjnej.
Materiał i metody. Badania przeprowadzono na Oddziale Neurochirurgii Szpitala Uniwersyteckiego nr 2 w Bydgoszczy na grupie 188 chorych, operowanych z powodu dyskopatii lędźwiowej lub szyjnej kręgosłupa. Zastosowano plan badań prospektywnych, z trzykrotną oceną w czasie, wykorzystując Kwestionariusz Niepełnosprawności Oswestry. Zgromadzony materiał opracowano statystycznie, weryfikując hipotezy na poziomie istotności p < 0,05.
Adv Clin Exp Med 2011, 20, 3, 377–384 ISSN 1230-025X
ORIGINAl PAPERS
The definition of intervertebral disc hernia is a broad notion covering various kinds and degrees of its dislocation and most often defined as a com-plex of structural changes as a consequence of dis-orders of the common element system which is made up of intervertebral discs and the spinal ca-nal [1, 2]. Two factors have a constant influence on the destruction of an intervertebral disc: everyday use and the aging process. The first one consists of biomechanical and tissular disc decomposition and it is mainly connected with water loss and dis-equilibrium in the synthesis of proteoglycans, with predominance of their decomposition. An inter-vertebral disc, along with age, gradually loses elas-ticity, springiness and resistance to burdens. The starting process of degeneration of collage fibers weakens the structures of the annulus fibrosus as well. As a result, the shock-absorbing and adap-tive abilities of the disc become greatly reduced. The aging process of the intervertebral disc is often caused by an excessive spine burden, congenital defects and also spine injuries which result from past diseases and trauma. It leads to a decrease in the intervertebral disc’s height, which destabilizes the whole motor segment and leads to the damage of its other elements [3–5].
Spine ailments, including those caused by in-tervertebral disc hernia, owing to the universality of its occurrence, have taken on the characteristics of an epidemic [6–8]. An exploration of the problems connected with a dominating symptom of discopa-thy – like pain – should not concentrate only on the views associated with diagnosis and treatment. With the long duration of spine disease processes, psychomotor disorders are connected in the form of the deterioration of control keeping correct pos-ture as well as a decrease in the level of physical and social functioning [9–11]. Thus, a significant prob-lem, often omitted in the specialist literature, is the issue of the patients’ disability or ability.
The term disability covers many functional
limitations with particular consideration of barriers in performing basic everyday-life activities such as: moving, reaching various things, physical fitness,
seeing, hearing, the necessity of using care, holding urine, communicating, and the retention of cogni-tive and behavioral functions [12]. The assessment scale most often used for the ability of patients with intervertebral disc hernia is the Oswestry Disability Index. This tool, which takes into account everyday-life problems, is crucial in the perioperative period for the self-reliant functioning of patients.
The aim of this study was to assess the agil-ity of the examined after operational treatment of lumbar or cervical discopathy was conducted.
Material and Methods
The study was conducted at the Neurosurgery Department of University Hospital number 2 in Bydgoszcz on a group of 188 patients. A prospec-tive plan of examination with a three-time assess-ment was used (assessassess-ment 1, assessassess-ment 2, and assessment 3). Only patients with a diagnosis of lumbar and spinal or cervical discopathy were qualified for the studies. The next criterion involv-ing patients in the research was the performance of one procedure of discectomy in each of them. The research did not include patients who were discharged from the department earlier or later than the 7th day after the operation and those who were subjected to conservative therapy. On this basis, 188 patients were included in the study and subjected to assessment 1 and 2. In assessment 3, due to refusals (failure to return the survey), 140 patients took part.
People qualified to the study were character-ized by taking into account the following features: age, sex, place of residence, kind of work per-formed, clinical diagnosis and operation level. De-tailed data is presented in Table1.
In the study, a standardized research tool, the Oswestry Disability Index, was used [13, 14]. For assessment of the limitation of agility (disability) caused by pain ailments of the lumbar part of the spine, the ODI scale (Oswestry Disabillity Index) is used, whereas for determining disability due to
Wyniki. W poszczególnych ocenach wzrastała liczba osób, które mają minimalne upośledzenie – wzrost o 6,4%, a następnie o 41,3% (p < 0,05). Największą poprawę zaobserwowano w zakresie bólu (spadek o 1,79 pkt.), podno-szenia przedmiotów (spadek o 1,14 pkt.) oraz podróży (spadek o 1,09 pkt.). W przypadku dyskopatii lędźwiowej 73 badanych (38,8%) przed zabiegiem zakwalifikowało się do II grupy. Po zabiegu, w ocenie 1, w grupie tej znalazło się 80 chorych (42,6%), a w ocenie 3. większość znalazła się w grupie I (40%) oraz w grupie II (23,6%) (r = 0,5147, p < 0,05 i.s). Istotna poprawa nastąpiła także u badanych z dyskopatią C (r = 0,3767; p < 0,05).
Wnioski. 1. Przed zabiegiem chirurgicznym większość badanych charakteryzuje się umiarkowanym upośledzeniem wydolności funkcjonalnej. 2. Po leczeniu neurochirurgicznym, w dniu wypisu ze szpitala, stan funkcjonalny popra-wia się minimalnie. Znacząca statystycznie poprawa nastąpiła w późnym okresie po przeprowadzonym leczeniu. 3. Zaobserwowana poprawa sprawności badanych dotyczy zarówno osób z przepukliną krążka międzykręgowego odcinka szyjnego, jak i lędźwiowego kręgosłupa (Adv Clin Exp Med 2011, 20, 3, 377–384).
pain ailments of the cervical part of spine, the NDI scale (Neck Disabillity Index) is used.
The questions included in the survey concern the performing of everyday activities and were se-lected from a few experimental surveys as the most significant for problems of people suffering from spinalgia. Each question contains six responses. Each subsequent response corresponds to a larger degree of disability.
The responses to the questions made it possi-ble to classify how limited the patient’s function-ing is while performfunction-ing particular activities. The responses are arranged from 0 to 5. The overall result is presented on a 0–50 point scale. It is multiplied by two and expressed as a percentage [13, 14]. The results obtained make it possible to distinguish five groups of disability [13, 14]:
– Group I – 0–20% – minimal disability. In this group, patients do not require treatment but only education concerning the correct techniques of sitting, lifting, diet and physical efficiency;
– Group II– 20–40% – moderate disability. In
this group, more severe pain occurs. Patients tend to be periodically unfit for work. The condition of the spine requires treatment to improve;
– Group III – 40–60% – serious disability. Pain is a serious problem, patients require some detailed examination;
– Group IV – 60–80% – full disability. Pain disrupts all aspects of the patient’s life. Proper treatment is required;
– Group V – 80–100% – invalidity. Patients are immobilized in bed. Their objective state can only be estimated by a detailed and exact clinical examination.
The calculations were made with the use of the computer program called Microsoft Excel, a part of Microsoft Office, and the program Sta-tistica 6.0. In the staSta-tistical analysis, quantitative and value statistics were used as well as methods of statistical description: the measure of position x and measure of differentiation SD, the test of
independence χ2 and Spearman’s
nonparamet-ric test. A significance level of the value p < 0.05 was accepted as statistically characteristic in the study.
A condition for completing the study was the obtaining of a positive opinion from the Biotic Commission at Collegium Medicum in Bydgoszcz on the concept of the presented study.
Table 1. Characteristics of the examined group
Tabela 1. Charakterystyka grupy badanej
Feature examined
(Badana cecha) N %
Sex
(Płeć) femalemale 98 90 52.147.9
Age – years
(Wiek – lata) 10–1920–29 30–39 40–49 50–59 60–69 70–79
0 18 46 58 52 12 2
0 9.6 24.5 30.9 27.7 6.4 1.1 Place of residence
(Miejsce zamieszkania) villagecity 55133 29.370.7
Kind of work
(Rodzaj pracy) physicalintellectual 94 41 69.630.4
Clinical diagnosis
(Rozpoznanie kliniczne) lumbar discopathycervical discopathy 140 48 74.525.5 Operation level
(Poziom operacji) C3 – C4C4 – C5 C5 – C6 C6 –C7 l1 – l2 l2 – l3 l3 – l4 l4 – l5 l5 – S1
3 9 28 8 1 4 4 62 69
Results
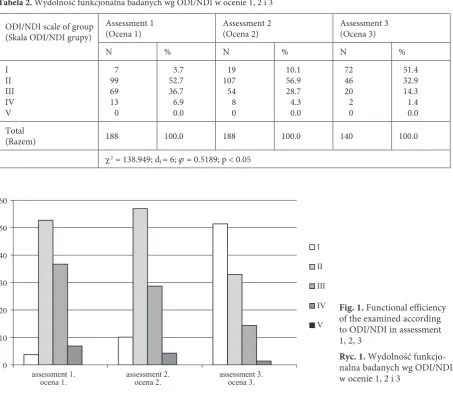
In the assessment of the examined according to ODI or NDI, it was noticed that in particular assessments, the number of people with minimal handicap increased – an increase of 6.4% in rela-tion to assessment 1, and then by another 41.3%. Among the examined, there were no people who would be classified as full disability (p < 0.05) (Ta-ble 2, Fig. 1).
Next, particular ODI/NDI categories were analyzed (Tables 3, 4).
Pain intensification – at first a definite, favor-able decrease of the mean by 2.3%, and then an increase of 0.51%. General pain intensification fa-vorably fell by an average of 1.79%.
Self-dependence – at first an unfavorable in-crease of 0.7% of the average result, and then a de-crease of 1.12%. General self-dependence (favor-ably) fell by 0.42%.
lifting objects – at first an unfavorable in-crease of 0.4%, and then a dein-crease of 1.54%. In total, a favorable decrease of 1.14%.
Walking – a decrease of 0.1%, then another decrease of 0.53%. In total, a favorable decrease of the mean by 0.63%.
Sitting – at first the mean remains unchanged, but less favorable due to standard deviation. It is not as close to the mean as in assessment 1. Next, a decrease of 0.83%. A total decrease of 0.83%.
Standing – at first a decrease of 0.2%, and then a decrease by another 0.43%. A total decrease of 0.63%.
Sleeping – at first a decrease of 0.6%, and then an increase of 0.09%. In total, a favorable decrease of 0.51%.
Social life – at first a decrease of 0.1%, and then a decrease of 0.88%. A total decrease of 0.98%.
Sexual activity – at first a decrease of 0.4%, and next an increase of 0.08%. A total decrease of 0.32%.
Travel – at first an increase of 0.4%, and next a decrease of 1.49%. A total decrease of 1.09%.
The means in the categories of pain intensi-fication, lifting objects and travel fell in the most favorable way. The differences turned out to be statistically significant.
Table 2. Functional efficiency of the examined according to ODI/NDI in assessment 1, 2, 3
Tabela 2. Wydolność funkcjonalna badanych wg ODI/NDI w ocenie 1, 2 i 3
ODI/NDI scale of group (Skala ODI/NDI grupy)
Assessment 1
(Ocena 1) Assessment 2(Ocena 2) Assessment 3(Ocena 3)
N % N % N %
I II III IV V
7 99 69 13 0
3.7 52.7 36.7 6.9 0.0
19 107 54 8 0
10.1 56.9 28.7 4.3 0.0
72 46 20 2 0
51.4 32.9 14.3 1.4 0.0 Total
(Razem) 188 100.0 188 100.0 140 100.0
χ2 = 138.949; df = 6; ϕ = 0.5189; p < 0.05
Fig. 1. Functional efficiency of the examined according to ODI/NDI in assessment 1, 2, 3
Ryc. 1. Wydolność funkcjo-nalna badanych wg ODI/NDI w ocenie 1, 2 i 3
0 10 20 30 40 50 60
assessment 1.
ocena 1. assessment 2.ocena 2. assessment 3.ocena 3.
I
II
III
IV
Table 3. Average ODI/NDI in particular categories and assessments
Tabela 3. Średnie ODI/NDI w poszczególnych kategoriach i ocenach
Assessment
(Ocena) ODI/NDI Scale kategories(Skala ODI/NDI kategorie) N x– SD min max
1. A B C D E F G H I J 188 188 188 188 188 188 188 188 188 188 3.1 1.6 2.9 1.6 2.0 2.2 1.4 2.2 1.0 2.3 1.159 0.934 1.011 1.028 1.051 0.934 0.777 0.973 1.017 1.003 0 0 0 0 0 0 0 0 0 0 5 4 5 5 5 5 4 5 5 4 2. A B C D E F G H I J 188 188 188 188 188 188 188 188 188 188 0.8 2.3 3.3 1.5 2.0 2.0 0.8 2.1 0.6 2.7 0.981 1.030 1.053 1.167 1.158 1.011 0.764 1.067 0.921 1.015 0 0 1 0 0 0 0 0 0 0 5 5 5 5 5 5 3 5 5 5 3. A B C D E F G H I J 140 140 140 140 140 140 140 140 140 140 1.31 1.18 1.76 0.97 1.17 1.57 0.89 1.22 0.68 1.21 1.257 0.850 1.244 1.045 0.913 1.073 0.895 0.989 0.771 0.942 0 0 0 0 0 0 0 0 0 0 5 4 5 5 3 5 5 4 4 4
Tabela 4. ODI/NDI kategorie – zależności statystyczne
Table 4. ODI/NDI categories – statistical dependences
ODI/NDI Scale Categories (Skala ODI/NDI kategorie)
Assessment 1
(Ocena 1) Assessment 2(Ocena 2) Assessment 3(Ocena 3) r p
N x– SD N x– SD N x– SD
A B C D E F G H I J 188 188 188 188 188 188 188 188 188 188 3.1 1.6 2.9 1.6 2.0 2.2 1.4 2.2 1.0 2.3 1.159 0.934 1.011 1.028 1.051 0.934 0.777 0.973 1.017 1.003 188 188 188 188 188 188 188 188 188 188 0.8 2.3 3.3 1.5 2.0 2.0 0.8 2.1 0.6 2.7 0.981 1.030 1.053 1.167 1.158 1.011 0.764 1.067 0.921 1.015 140 140 140 140 140 140 140 140 139 140 1.31 1.18 1.76 0.97 1.17 1.57 0.89 1.22 0.68 1.21 1.257 0.850 1.244 1.045 0.913 1.073 0.895 0.989 0.771 0.942 0.5654 0.3347 0.4721 0.1557 0.1798 0.0943 0.2365 0.3074 0.0582 0.4770 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05
Another issue analyzed was the determination of the influence of clinical diagnosis on the assess-ment of functional efficiency obtained in the three measurements (Table 5).
In the case of l-S discopathy, most of the
most respondents were in group I (40%) and in group II (23.6%). A reclassification occurred which proves the improvement of functional efficiency of the examined in assessment 3. It is a statistically significant difference; r = 0.5147, p < 0.05. Among the examined with this diagnosis, there was no one in group V.
Analyzing the results obtained from the exam-ined with a diagnosis of cervical discopathy, a sim-ilar dependence was noticed: the majority (13.8%) in assessment 1 qualified to group II. As after op-erations, in assessment 2, a similar number of re-spondents belonged to group II (14.4%). In assess-ment 3 though, the majority (11.1%) qualified to group I (11.1%) and to group II (9.3%). This data shows an increasing improvement as time goes on; this difference is characteristic on the average level r = 0.3767, (p < 0.05). like in the case of l-S dis-copathy in the group mentioned above, there were no people from group V.
Discussion
Maintenance of functional efficiency is the main task in the care of patients with discopathy [15]. It is the loss of functional efficiency which causes the occurrence of disability, has an influ-ence on the decreasing of the quality of life and a significant increase of the social and economic costs. Moreover, disability is an important com-ponent of the assessment of a patient’s condition, coming directly from him and being a valuable supplement of the assessment of disease activity by a doctor [16, 17]. Assessment of patients’ func-tional state is often used as an objective efficiency method of therapeutic processes [10, 17–20]. In the available literature, one can find several dif-ferent scales which describe treatment efficiency
from the perspective of the degree of functional handicap [10, 13, 14, 21, 22]. Some examples may be as follows: the Short Form Health Survey SF-36, the Prolo Functional Economic Outcome Rating Scale, Roland’s survey and the Oswestry low Back Pain Disability Questionnaire. They have received a positive review due to their usefulness in the as-sessment of patients with rachialgia since they take into account objective and subjective factors char-acteristic for this affection [10].
An analysis of the efficiency state of the exam-ined, including mainly the assessment of the ca-pabilities to perform basic everyday-life activities, was made with the use of the Oswestry Question-naire (ODI/NDI).
In the initial study, patients reported a decrease in the functional state to an average degree – 52.7% of the examined had a moderate handicap and 36.7% a serious handicap. This state significantly improved after the procedure; in particular assess-ments, the number of people who had a minimal handicap increased by 6.4% in relation to assess-ment 1, and then by another 41.3%. This improve-ment concerned both patients with l-S and C dis-copathy. This data corresponds to results found in the literature. An average ODI indicator for the group of the examined with l-S discopathy was: 55 before the operation and 36 after the procedure in Häkkinen et al. [23], 50 before the operation and 20.5 after the procedure in Strőmqvist et al. [24], 56.7 before the operation and 12 after the proce-dure in Ryang et al. [25]. Whereas the average NDI indicator for the group of the examined with C dis-copathy was: 25 before the operation and 11 after the procedure in Godlewski et al. [26] and 60 before the operation and 29 after in Steinmetz et al. [27].
In particular categories of the ODI/NDI ques-tionnaire, various results were obtained which show a heterogeneous influence of individual
ac-Table 5. Functional efficiency of the examined according to ODI/NDI and clinical diagnosis in assessment 1, 2, 3
Tabela 5. Wydolność funkcjonalna badanych wg ODI/NDI a rozpoznanie kliniczne w ocenie 1, 2 i 3
ODI/NDI Scale Groups
(Skala ODI/NDI grupy)
Assessment 1
(Ocena 1) Assessment 2(Ocena 2) Assessment 3(Ocena 3)
l–S C l–S C l–S C
N % N % N % N % N % N %
I II III IV V
3 73 54 10 0
1.6 38.8 28.7 5.3 0.0
4 26 15 3 0
2.1 13.8 8.0 1.6 0.0
13 80 41 6 0
6.9 42.6 21.8 3.2 0.0
6 27 13 2 0
3.2 14.4 6.9 1.1 0.0
56 33 17 0 0
40.0 23.6 12.1 0.0 0.0
16 13 3 2 0
11.4 9.3 2.1 1.4 0.0 Total
(Razem) 140 74.5 48 25.5 140 74.5 48 26 106 75.7 34 24.3
tivities on the functional state of patients with dis-copathy. Before the operation the largest percent-age of replies showing a significant limitation in the scope of the assessed function was obtained in the questions concerning pain intensification and lifting objects. After 1 week following the proce-dure, from the estimated everyday-life activities, the biggest influence on the decrease in general comfort was given as a handicap in the scope of lifting objects and self-dependence. On the other hand, after a 6-month period, the examined also associated the decrease in life comfort with lifting objects and the occurrence of spinalgia during the states of standing and concentration. However, it is worth noting that in the late period after the procedure conducted, a significant improvement occurred in every discussed activity, firstly in the scope of considerable weakening of pain ailments. In the studies by Häkkinen et al. [23], the patients associated most problems with pain, social life, walking and standing. In the studies by Radzisze-wski [10], who analyzed a group of patients treated surgically and non-invasively, the change of
func-tional state – referring to the initial study – was observed to a greater extent in the group of pa-tients who had received surgery. A significant im-provement of functional efficiency, observed after the operative procedure in a direct and brief study, was decreased in a remote study. Similar data has also been presented by other authors [23–25, 27].
It should be added that the ability to perform everyday housework activities does not always mean a comparable degree of physical fitness since, to a large extent, it depends on the degree of work arrangement or technical facilities owned [10].
The authors concluded that before the op-erative procedure, most of the examined showed a moderate handicap of functional efficiency. After neurosurgical treatment, on the day of dis-charge from the hospital, the functional state un-derwent a minimal improvement. Statistically sig-nificant improvement occurred in the late period after the conducted treatment. Patients’ efficiency improved the most in the category of pain inten-sification. The problem is still the issue of lifting objects and standing or concentration.
References
Morton M:
[1] Zespoły bólowe kręgosłupa. Przew lek 2008, 5, 45–52.
Kim PK, Branch ChL:
[2] The lumbar degenerative disc: confusion, mechanics, management. Clin Neurosurg 2006, 53, 28–25.
Żytkowski A, Sosnowski S, Wrodycka B:
[3] Etiopatogeneza choroby zwyrodnieniowej kręgosłupa. Pol Merk lek 2006, 21, 125, 498–501.
Dziak A:
[4] Bóle i dysfunkcje kręgosłupa. Med Sport, Kraków 2007.
Luoma K, Riihimaki H, Luukkonen R, Raininko R, Viikari-Juntura E, Lamminen A:
[5] low back pain relation to
lumbar disc degeneration. Spine 2000, 25, 4, 487–492.
Ahmed M, Modic MT:
[6] Neck and low back pain: neuroimaging. Neurol Clin 2007, 25, 439–471.
Borenstein DG:
[7] Epidemiology, etiology diagnostics evaluation, and treatment of low back pain. Curr Opin Rheumatol 2001, 13, 2, 128–134.
Milewska D, Ryglewicz D:
[8] Epidemiologia bólów kręgosłupa. In: Neurologiczne powikłania niedomogi kręgosłupa. Eds.: Mazur R, Podemski R, Książkiewicz B. Via Medica, Gdańsk 2003, 31.
Hamberg-van Reenen HH, Ariëns GA, Blatter BM, Mechelen W:
[9] A systematic review of the relation between
physical capacity and future low back and neck/shoulder pain. Pain 2007, 130, 1–2, 93–107.
Radziszewski KR:
[10] Stan funkcjonalny pacjentów z dyskopatią kręgosłupa lędźwiowego leczonych wyłącznie zacho-wawczo bądź operowanych. Wiad lek 2008, 61, 1–3, 23–29.
Banbury P, Feenan K, Allcock N:
[11] Experiences of analgesic use in patients with low back pain. Br J Nurs 2008, 17, 19, 1215–1218.
Barnes C, Mercer G:
[12] Niepełnosprawność. SIC, Warszawa 2008.
Fairbank JC, Couper J, Davies JB, O’Brien JP:
[13] The Oswestry low back pain disability questionnaire. Physiotherapy 1980, 66, 8, 271–273.
Fairbank JC, Pynsent PB:
[14] The Oswestry Disability Index. Spine 2000, 25, 2940–2953.
Puolakka K, Ylinen J, Neva MH,
[15] Kautiainen H, Häkkinen A: Risk factors back pain-related loss of work time after surgery for lumbar disc herniation: a 5-year follow-up study. Eur Spine J 2008, 17, 3, 386–392.
Weiner BK:
[16] Difficult medical problems: on explanatory models and a pragmatic alternative. Med Hypotheses 2007, 68, 3, 474–479.
Kagaya H, Takahashi H, Sugawara K, Kuroda T, Takahama M:
[17] Quality of life assessment before and after lumbar disc surgery. J Orthop Sci 2005, 10, 5, 486–489.
Ferrara L
[18] , Triano JJ, Sohn MJ, Song E, Lee DD: A biomechanical assessment of disc pressures in the lumbosacral spine in response to external unloading forces. Spine J 2005, 5, 5, 548–553.
Jansson KA.
[19] , Németh G, Granath F, Blomqvist P: Health-related quality of life in patients before and after sur-gery for a herniated lumbar disc. J Bone Joint Surg Br 2005, 87, 7, 959–964.
Lisiński P, Małgowska M:
Rąpała A, Rąpała K, Lachowicz W:
[21] Metody badań klinicznych i skale ocen leczenia choroby dyskowej kręgosłupa ze szczególnym uwzględnieniem skali Oswestry. Ortop Traumatol Rehabil 2004, 6, 2, 149–154.
Jarmużek P, Owoc A, Wdowiak L:
[22] Choroba zwyrodnieniowa kręgosłupa jako problem społeczny. II. Charakter wykonywanej pracy a przebieg choroby. Zdrow Publ 2004, 114, 3, 307–311.
Häkkinen
[23] A, KautiainenH, Järvenpää S, Arkela-Kautiainen M, YlinenJ: Changes in the total Oswestry Index and its ten items in females and males pre- and post-surgery for lumbar disc herniation: a 1-year follow-up. Eur Spine J 2007, 16, 3, 347–352.
Strőmqvist F, Ahmad M, Hildingsson Ch, Jőnsson B, Strőmqvist B:
[24] Gender differences in lumbar disc
hernia-tion surgery. Acta Orthopaedica 2008, 79, 5, 643–649.
Ryang YM, Oertel MF, Mayfrank L, Gilsbach JM, Rohde V:
[25] Standard open microdiscectomy versus minimal
access trocar microdiscectomy: results of a prospective randomised study. Neurosurgery 2008, 62, 1, 174–182.
Godlewski B, Grochal M, Jekimov R, Wójcik R, Radek M, Radek A:
[26] Evaluation of outcome after surgical
treat-ment of cervical disc disease with Dero C – Disc Peek cages. Neurol Neurochir Pol 2007, 41, 4, 417–426.
Steinmetz MP
[27] , Patel R, Traynelis V, Resnick DK, Anderson PA: Cervical disc arthroplasty compared with fusion in a workers’ compensation population. Neurosurgery 2008, 63, 4, 741–747.
Address for correspondence:
Renata JabłońskaDepartment of Neurological and Neurosurgical Nursing
Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Torun Techników 3
85-094 Bydgoszcz Poland
Tel.: (+48 52) 585-21-93 ext. 233, (52) 585-21-94 E-mail: [email protected]
Conflict of interest: None declared