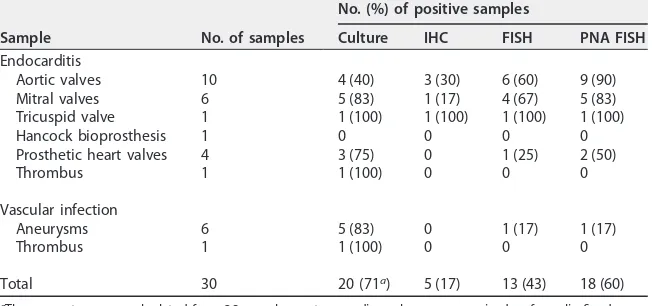
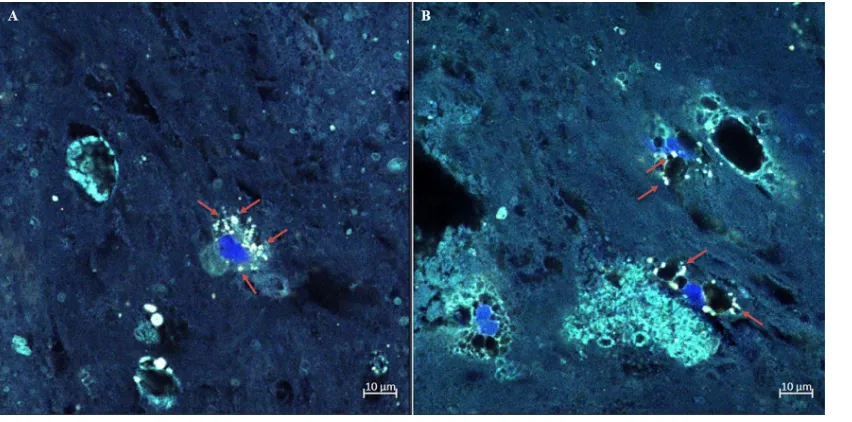
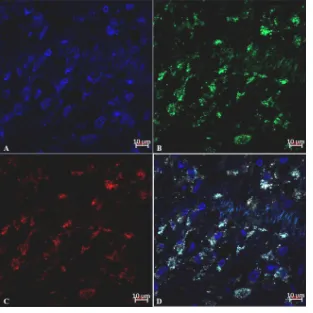
Fluorescence In Situ Hybridization (FISH) and Peptide Nucleic Acid Probe Based FISH for Diagnosis of Q Fever Endocarditis and Vascular Infections
Full text
Figure

Related documents
Because Toll-like receptors (TLRs) are involved in both innate and adaptive immune responses to a broad variety of antigens, the association between polymorphisms of TLRs and
The experiment was done until steady state condition was attained in the evaporator. The energy consumption of the system is measured using a digital
Results: The results indicated that Gd-BG scaffolds could promote the proliferation and osteogenic differentiation of human bone marrow-derived mesenchymal stem cells
Analysis of Cotton’s catechetical lectures and catechism on the church in 1634 indicate that he had not yet instituted relations of faith in Boston.. 52 John Davenport, A
The system is written in variations on the initial conditions for the Laskar system, and with its help the dependences of the problem parameter of the senior Lyapunov exponent and
From the above analysis, at present stage, China’s industry structure and employment structure evolution ac- cords with the general rules of modern economic development;
In our case to provide software quality assurance, we performed the testing process after solution phase to ensure that design and code meet the requirements
In this paper, we extend the Heisenberg uncertainty principle in FRFT domain for both discrete and conti- nuous cases for the ε -concentrated signals or the signals with
