Communication training interventions for
family and professional carers of people
living with dementia : a systematic review
of effectiveness, acceptability and
conceptual basis
Morris, LE, Horne, M, McEvoy, P and Williamson, T
http://dx.doi.org/10.1080/13607863.2017.1399343
Title
Communication training interventions for family and professional carers of
people living with dementia : a systematic review of effectiveness,
acceptability and conceptual basis
Authors
Morris, LE, Horne, M, McEvoy, P and Williamson, T
Type
Article
URL
This version is available at: http://usir.salford.ac.uk/id/eprint/44199/
Published Date
2017
USIR is a digital collection of the research output of the University of Salford. Where copyright
permits, full text material held in the repository is made freely available online and can be read,
downloaded and copied for noncommercial private study or research purposes. Please check the
manuscript for any further copyright restrictions.
Full Terms & Conditions of access and use can be found at
http://www.tandfonline.com/action/journalInformation?journalCode=camh20
Download by: [University of Salford] Date: 14 November 2017, At: 01:34
Aging & Mental Health
ISSN: 1360-7863 (Print) 1364-6915 (Online) Journal homepage: http://www.tandfonline.com/loi/camh20
Communication training interventions for family
and professional carers of people living with
dementia: a systematic review of effectiveness,
acceptability and conceptual basis
L. Morris, M. Horne, P. McEvoy & T. Williamson
To cite this article: L. Morris, M. Horne, P. McEvoy & T. Williamson (2017): Communication training interventions for family and professional carers of people living with dementia: a systematic review of effectiveness, acceptability and conceptual basis, Aging & Mental Health, DOI:
10.1080/13607863.2017.1399343
To link to this article: http://dx.doi.org/10.1080/13607863.2017.1399343
© 2017 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group
Published online: 10 Nov 2017.
Submit your article to this journal
Article views: 39
View related articles
REVIEW
Communication training interventions for family and professional carers of people
living with dementia: a systematic review of effectiveness, acceptability and
conceptual basis
L. Morris a,b, M. Hornea,b, P. McEvoyaand T. Williamsona
aSix Degrees Social Enterprise, Salford, UK;bInstitute of Dementia, School of Health and Society, University of Salford, Salford, M6 6PU, UK.
ARTICLE HISTORY
Received 30 April 2017 Accepted 25 October 2017
ABSTRACT
Objectives:To update previous reviews and provide a more detailed overview of the effectiveness, acceptability and conceptual basis of communication training-interventions for carers of people living with dementia.
Method:We searched CINAHL Plus, MEDLINE and PsycINFO using a specific search and extraction protocol, and PRISMA guidelines. Two authors conducted searches and extracted studies that reported effectiveness, efficacy or acceptability data regarding a communication training-intervention for carers of people living with dementia. Risk of bias was assessed using the Cochrane Collaboration guidelines. Quality of qualitative studies was also systematically assessed.
Results:Searches identified 450 studies (after de-duplication). Thirty-eight studies were identified for inclusion in the review. Twenty-two studies focused on professional carers; 16 studies focused mainly on family carers. Training-interventions were found to improve communication and knowledge. Overall training-interventions were not found to significantly improve behaviour that challenges and caregiver burden. Acceptability levels were high overall, but satisfaction ratings were found to be higher for family carers than professional carers. Although many interventions were not supported by a clear conceptual framework, person-centred care was the most common framework described. Conclusion: This review indicated that training-interventions were effective in improving carer knowledge and communication skills. Effective interventions involved active participation by carers and were generally skills based (including practicing skills and discussion). However, improvements to quality of life and psychological wellbeing of carers and people living with dementia may require more targeted interventions.
KEYWORDS
Dementia; communication; training; family carers; professional carers
The ability to communicate is a fundamental need that impacts on the quality of our relationships and our general sense of health and wellbeing (Jootun & McGhee,2011; Seg-rin,2001). This is reflected in the experience of people living with dementia who identify that their unmet needs are psy-chosocial in nature (van der Roest et al.,2009). For people liv-ing with all types of dementia, their cognitive impairments can affect their ability to communicate in varying ways; such asfinding words to express their intentions, retrieving memo-ries or processing the contextual information they need to understand the motivations of others (Schrauf & Muller,
2014). This can make it difficult to sustain the everyday con-versations that support their social relationships (Kindell, Keady, Sage, & Wilkinson,2016) and exacerbate the feelings of social isolation and exclusion (Ablitt, Jones, & Muers,2009). Family and professional (paid) carers alsofind these commu-nication impairments very challenging as they contribute to relationship stress (Dooley, Bailey, & McCabe, 2015; Jones, Edwards, & Hounsome,2014).1
A number of studies have demonstrated that caring for someone living with dementia has the potential to have sig-nificant negative effects on carers’ physical and emotional health (Gallagher-Thompson et al., 2012). Studies have also indicated that carers can identify positive aspects of their role (Brodaty & Donkin, 2009) and resilience within a caring role has been shown to be linked to factors such as perceived
ability to cope, perceived control and social support (Dias et al., 2015; Harmell, Chattillion, Roepke, & Mausbach,2011). The declining neurological capability of people living with dementia is only one of many factors that may influence the quality of their relationships and communicative interactions (Guendouzi & Savage,2017). Compensatory adaptations may enable carers to ameliorate the effects of an individual’s cog-nitive impairment; for example, byfindings ways of keeping a conversation going without placing as much pressure on the individual’s cognitive resources (Haberstroh, Neumeyer, Krause, Franzmann, & Pantel,2011). Qualitative research indi-cates that acquisition of knowledge and skills can help facili-tate resilience and maintaining a relationship with those cared for (Donnellan, Bennett, & Soulsby,2015). These factors can be supported by communication and interaction based training interventions, which can enhance perceived coping and control (Eggenberger et al.,2013). However, the availabil-ity of evidence-based support and training for carers- espe-cially family carers- is still limited (Dawson, Bowes, Kelly, Velzke, & Ward,2015; Eggenberger et al.,2013).
The current review evaluated the effectiveness and accept-ability of communication training-interventions with a view to contributing to greater implementation of such interventions. This review included studies of training-interventions that include a communication component and were aimed at pro-fessional and family carers of people living with dementia.
CONTACT L. Morris [email protected]
© 2017 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, dis-tribution, and reproduction in any medium, provided the original work is properly cited.
https://doi.org/10.1080/13607863.2017.1399343
Effectiveness and efficacy studies were included. Acceptability data included qualitative and qualitative data regarding the acceptability of the training-intervention to participants (e.g. systematically analysed self-report ratings of whether carers found the intervention satisfactory, helpful). The current review builds on a high quality systematic review of the effec-tiveness and content of communication skills training inter-ventions by Eggenberger and colleagues. This previous review identified that training increased the communication skills, competencies and knowledge of carers and contributed to improvements in the wellbeing of people living with dementia (Eggenberger et al.,2013). However, levels of care-giver burden and behaviour that challenges were not found to significantly change post training. Since the publication of this review a significant number of studies have been pub-lished, including 13 new RCTs, and it is considered important to re-examine the evidence-base in light of this. Furthermore, the current review seeks to provide a more detailed account of the conceptual basis of training-interventions.
Method
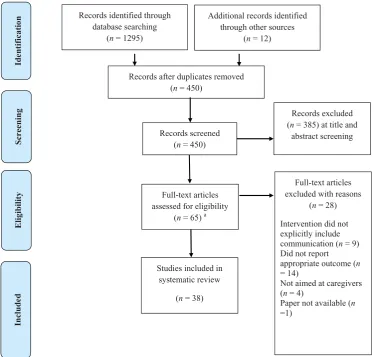
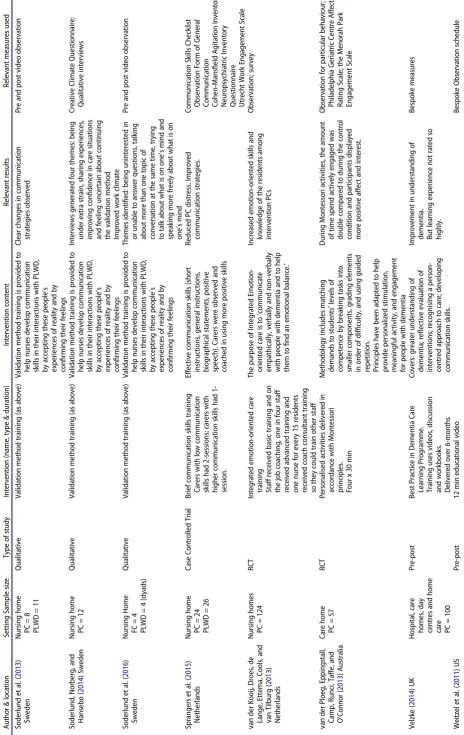
The review was conducted in accordance with the guidelines provided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher, Lib-erati, Tetzlaff, Altman, & Group,2009). The current review is a mixed methods systematic review. Given that one of the focuses of the review was on acceptability, qualitative data was considered potentially useful in illuminating participant experience, satisfaction and acceptability. A search protocol was developed through team discussion (seeFigure 1).
Inclusion/exclusion criteria
Studies were included if they evaluated training interventions aimed at family or professional carers of people living with dementia. Studies were included from 2010 due to the recent review by Eggenberger, Heimerl, Bennett, Eggenberger, Hei-merl, and Bennett (2013); this date was chosen so as not to duplicate the studies included in this previous review. The definitions of communication and interaction are in line with Eggenberger and colleagues and multicomponent interven-tions were included to align the scope of these two reviews. This was in order to enable readers to draw on both reviews from a common point of reference. See Figure 1 for more details of inclusion and exclusion criteria.
Information sources and study selection
The electronic databases CINAHL Plus, MEDLINE and PsycINFO were systematically searched to identify the appropriate stud-ies to include in the review. Boolean combinations were used to maximise the strength of the search. SeeFigure 1for search protocol and list of search terms. Searching of relevant system-atic reviews was undertaken. The reference lists of all the included studies were scanned for additional relevant studies. One author was contacted to obtain a paper that was unavail-able, but they did not respond and the study was excluded.
Study selection and data extraction
Thefirst two authors (Lydia Morris & Maxine Horne) indepen-dently screened 50% of the titles and abstracts using the
inclusion and exclusion criteria. Cohen’s Kappa was calculated at 0.76 indicating reliable agreement. The second author (Maxine Horne) screened the remaining papers.
Data was extracted from included studies by Lydia Morris and Maxine Horne using a data extraction table devised for this purpose. Information extracted from the included studies consisted of: study design, sample characteristics, training interventions used (including intervention characteristics and the conceptual basis of training interventions) and results.
Risk of bias and quality assessment
The methodological quality of all quantitative studies was assessed by thefirst author (Lydia Morris) using the Cochrane Risk of Bias tool (Higgins & Green,2011). Although a number of quality assessment tools are available, the PRISMA state-ment cautions against using these (Liberati et al.,2009). Com-ponent based approaches are recommended, and specifically the Cochrane Risk of Bias tool (Liberati et al., 2009). Studies were assessed for risk of selection bias (including adequacy of randomisation and of allocation concealment), performance bias (whether participants and trainers were blind to treat-ment group), detection bias (whether assessors were blind to treatment group), attrition bias (related to the amount, nature or handling of incomplete data), reporting bias (whether all expected outcomes have been reported) and other bias (pri-marily sample size and measures used). Although the current review included a range of quantitative study designs (not just RCTs), the Cochrane Risk of Bias tool provides useful infor-mation concerning the risk of bias present in all quantitative study design. For example, if a study is not randomised there will be inadequate randomisation sequence generation and blinding, which will potentially bias the results.
The methodological quality of all qualitative studies was assessed by the second author (Maxine Horn) using the crite-ria for appraising qualitative studies proposed by Walsh and Downe (2006). Although establishing the reliability and valid-ity of qualitative studies is more contentious than for quanti-tative studies, steps can be taken to establish the validity of themes presented and to promote quality (Creswell, 2013; Creswell & Miller,2000; Shenton,2004). Given these consider-ations and the variety of methodologies and perspectives of the qualitative studies included, a domains-based approach was used to examine quality. To illustrate the variety of quali-tative studies included: one study used a phenomenological action research approach (Lykkeslet, Gjengedal, Skrondal, & Storjord, 2014) others used content analysis or videotaped interaction-data (Chenoweth et al., 2015; Hammar, Emami, Engstrom, & Gotell, 2011; Lykkeslet et al., 2014; Soderlund, Cronqvist, Norberg, Ternestedt, & Hansebo, 2013); one study focused on organisational acceptability of the training rather than on participant experience (Chenoweth et al.,2015).
Data synthesis
Following the principles recommended by Popay et al. (2006) an inductive approach was used to develop a preliminary syn-thesis and explore the relationships between studies. This includes: grouping studies by relevant clusters (e.g. interven-tions aimed at family or professional carers), deciding whether to formally assess quality and the tools to use, and formulat-ing a textual description.
Results
Study selection
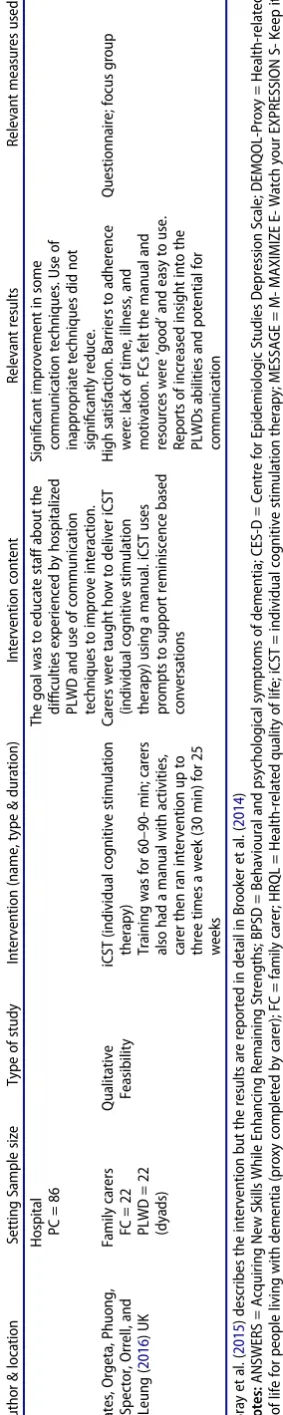
After de-duplication and exclusion according to the study protocol, 38 studies were included. SeeFigure 2for aflow dia-gram of the numbers of studies identified and excluded dur-ing the selection process.
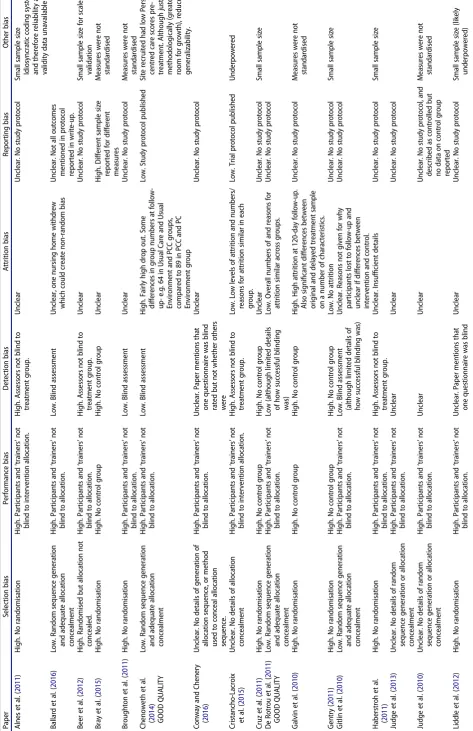
Characteristics of included studies
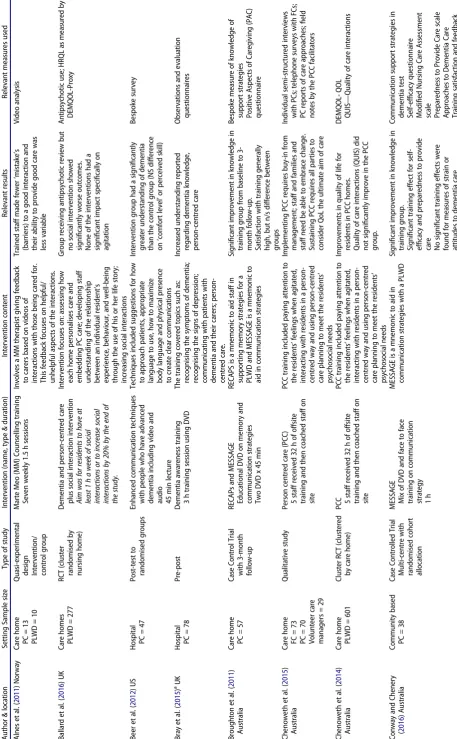
Of the 38 studies identified for inclusion in this systematic review, 21 of the studies were conducted in English speaking nations (UK, US and Australia). The remaining 17 were located in Western Europe. Twenty-two studies evaluated communi-cation skills training interventions for professional staff in care Identifying relevant studies (inclusion/exclusion criteria)
Intervention:
Studies will be included if they evaluate interventions aimed at family or professional carers of people living with
dementia. Only interventions with a clear communications component for carers will be included, such a
communication component must have the potential improve or increase the communication between carers and people
living with dementia. “Communication was defined as a reciprocal process of sharing and receiving verbal information
by means of language. Interaction was defined as a reciprocal communicative action by means of non-verbal
information, i.e. body language, gestures, facial expressions, rhythm, or sound” (Eggenberger et al., 2010, p. 346).
Study design:
Studies will be included if they report effectiveness, efficacy or acceptability data regarding such an intervention in a
peer reviewed journal, dissertation or book chapters.
Effectiveness and efficacy studies will include RCTs, open trials, prospective cohort studies and any study that reports
pre and post (or pre and follow-up data) regarding a relevant intervention. Single case designs that report repeated
measures will also be included. Acceptability studies will include studies that report qualitative or quantitative
acceptability data (e.g. self-report ratings of whether carers found the intervention satisfactory, helpful; verbal report in
focus groups or interviews etc.).
Comparator:
Alternative intervention, usual care, or no intervention.
Date range:
Studies from January 2010 to end of November 2016 covered.
Outcomes:
Include studies that have outcomes for carers and people living with dementia (both of these or either).
Exclusion:
Studies into pharmacological interventions will be excluded, as will studies where the inclusion of communications
skills is not evident. Due to restrictions on time and budget, only research in English included.
Search terms:
- communication or conversation or dialog* or interact* AND
- carer or caregiver or famil* or relative* or spous* or caring or professional or nurse or physician or doctor or staff
AND
- dementia or alzheime* or cognitive impairment or cognitive decline or frail AND
- psychoeducation* or psychological or psychosocial or support group or education or training
Figure 1.Extracts from study protocol regarding search criteria.
home and hospital settings. The remaining 16 studies evalu-ated interventions that targeted mainly family carers and they were delivered in family homes and other community set-tings. See Table 1 for details of all studies. There were 28 quantitative studies, of which 13 were RCTs and there were 10 qualitative studies.
Overall quality assessment and methodological challenges
Quantitative studies
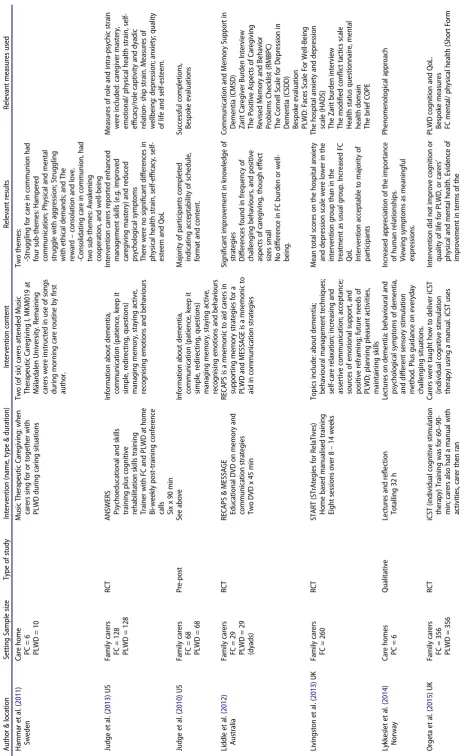
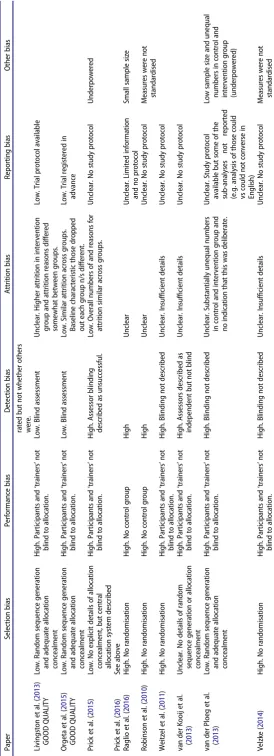
Overall methodological quality was variable across all quanti-tative studies and only four studies had low bias ratings in three or more domains (Chenoweth et al., 2014; De Rotrou et al.,2011; Livingston et al., 2013; Orgeta et al.,2015). See
Table 2for the overall assessment of risk of bias. Performance bias was present in all of the quantitative studies due to the impossibility of blinding patients and trainers to the interven-tion being delivered. However, most studies were also subject to detection bias; only seven studies used comprehensive assessor blinding (Ballard et al.,2016; Broughton et al.,2011; Chenoweth et al.,2014; De Rotrou et al.,2011; Gitlin, Winter, & Dennis,2010; Livingston et al.,2013; Orgeta et al.,2015).
Eight studies reported adequate randomisation processes and allocation procedures, and therefore reduced selection bias (Ballard et al.,2016; Chenoweth et al., 2014; De Rotrou et al.,2011; Gitlin et al.,2010; Livingston et al., 2013; Orgeta et al.,2015; Prick, De Lange, Twisk, & Pot,2015; van der Ploeg et al., 2013). However, attrition levels were often high and rarely reported for each treatment group. Only four studies
provided sufficient information to conclude that attrition was sufficiently equal across groups (Cristancho-Lacroix et al.,
2015; De Rotrou et al., 2011; Orgeta et al.,2015; Prick et al.,
2015) (in addition, one small scale dissertation reported no attrition) (Gentry, 2011). Four studies were clearly protocol driven and provided enough information to conclude a low risk of reporting bias (Chenoweth et al., 2014; Cristancho-Lacroix et al.,2015; Livingston et al.,2013; Orgeta et al.,2015). Ten studies reported small sample sizes (Alnes, Kirkevold, & Skovdahl,2011; Beer, Hutchinson, & Skala-Cordes,2012; Cris-tancho-Lacroix et al., 2015; Cruz, Marques, Barbosa, Figueir-edo, & Sousa, 2011; Gentry, 2011; Haberstroh et al., 2011; Liddle et al.,2012; Prick et al.,2015; Raglio et al.,2016; van der Ploeg et al., 2013). Eight studies used unstandardised meas-ures (Alnes et al., 2011; Bray et al., 2015; Broughton et al.,
2011; Galvin et al., 2010; Judge, Yarry, Orsulic-Jeras, & Piercy,
2010; Robinson, Bamford, Briel, Spencer, & Whitty, 2010; Velzke, 2014; Weitzel et al.,2011); therefore it is not clear if these are reliable and valid and it is difficult to compare out-comes between studies.
Qualitative studies
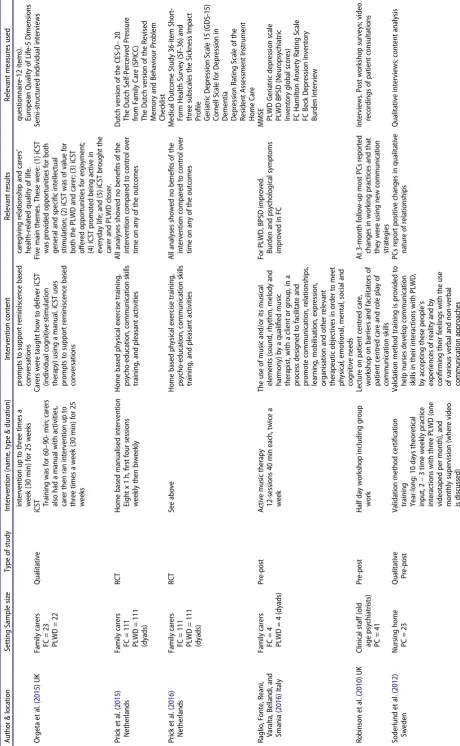
Using the criteria for appraising qualitative studies proposed by Walsh and Downe (2006), no included study met all the cri-teria (SeeTable 3; see Walsh & Downe,2006, for more detail of the domains assessed). It is possible that when the study was conducted a particular criterion was addressed, but for sake of brevity this was not reported in the journal article and thus cannot be assessed. Only one study (Lykkeslet et al.,2014) indicated that there had been a systematic search of the
Records after duplicates removed (n = 450)
Records screened (n = 450)
Records excluded (n = 385) at title and
abstract screening
Full-text articles assessed for eligibility
(n = 65) a
Full-text articles excluded with reasons
(n = 28)
Intervention did not explicitly include communication (n= 9) Did not report appropriate outcome (n = 14)
Not aimed at caregivers (n = 4)
Paper not available (n =1)
Studies included in systematic review
(n = 38)
Identificati
on
Screen
ing
Eligibili
ty
In
cl
uded
Additional records identified through other sources
(n = 12) Records identified through
[image:6.595.111.486.52.409.2]database searching (n = 1295)
Figure 2.PRISMAflow diagram of selection and exclusion (Moher et al.,2009).
Table 1. Details of Included studies. Autho r & locat ion Setti ng Samp le size Type of study Interve ntion (name ,type & d u ration) Interve ntion cont ent Relevan t results Relev ant measur es us ed Alne s e t al. ( 2011 ) Norwa y Care ho me PC = 1 3 PLWD = 1 0 Qua si-exper imenta l design Interve ntion/ control group Mart e Meo (M M) Coun selling training Seven w eekly 1.5 h ses sions In volves a MM thera pist giving feedb ack to ca rers bas ed on videos of interac tions w ith those being care d for. Thi s feedb ack focuses o n help ful/ unhe lpful aspec ts of the interac tions. Trained staff mad e fewer ‘ mista ke ’ s (barr iers) to a goo d in teraction and the ir ability to pro vide good care was less va riable Video analysis Ballar d e t al. ( 2016 ) U K Care ho mes PLWD = 277 RC T (cluster rand omised by nursing home) Deme ntia and perso n-cent red care plus social interac tion interve ntion Aim was for resi dents to have at least 1 h a week of social interac tions or to increase soci al interac tions by 20% by the end of the study. In tervent ion focuses on: assess ing how each hom e persona lises ca re and emb edding PC ca re; de veloping staff under standing of the relatio nship betwe en an individua l resid ent ’ s expe rience ,behavi our, and well-being thro ugh the use of his or her life sto ry; increa sing social interac tions Group receiv ing antipsyc hotic review bu t no social intervent ion show ed signi fi cantly worse outco mes. None of the intervent ions had a signi fi cant impact speci fi cally on agi tation Anti psychotic use; HRQL as measur ed by DEMQO L-Proxy Bee r e t al. ( 2012 ) U S Hospital PC = 4 7 Post-t est to rand omised groups Enha nced comm unication techn ique s with peo ple who have ad vanced dem entia includ ing vi deo and audio 45 min lecture Tec hniq ues included sugge stions for ho w to app roach patien ts, approp riate langua ge to use, ho w to maxim ize body langua ge and ph ysical pres ence to cr eate clear communi cations Intervent ion group had a signi fi cantly grea ter under standing of dementi a tha n the cont rol gro up (N S differen ce on ‘ comfo rt leve l ’ or perceived skill) Besp oke surv ey Bray et al. ( 2015 ) aUK Hospital PC = 7 8 Pre-p ost Deme ntia aware ness trai ning 3 h training session us ing DVD Th e training covere d top ics such as: recog nising the symp toms of dem entia; recog nising the signs of depr ession; comm unicating with patien ts with dem entia and their care rs; perso n-centr ed care . Increa sed und erstanding report ed rega rding dem entia kno wledge, pe rson-cent red care Observ ations and evaluati on questionna ires Broug hton et al. ( 2011 ) Austra lia Care ho me PC = 5 7 Cas e Control Trial with 3-mont h follow-up REC APs and MESSAGE Educa tional DVD on mem ory and comm unication stra tegies Two DVD x 4 5 min RE CAPS is a m n emonic to aid staff in suppo rting memo ry strate gies for a PLWD and MESSA GE is a mnemo nic to aid in com municatio n strate gies Signi fi ca nt imp rovement in knowled ge in trai ning group from bas eline to 3-mon th follow-up . Satis faction with training generall y hi gh, bu t n/s difference be tween gro ups Besp oke measur e o f knowledge o f support strategie s Positive Aspects of Care givin g (PAC ) questionna ire Ch enoweth et al. ( 2015 ) Austra lia Care ho me FC = 7 3 PC = 7 0 Volunt eer care mana gers = 2 9 Qua litative stud y Perso n centred care (PCC) 5 staff receiv ed 32 h o f offsite training and the n coache d staff on site PCC traini ng includ ed payi ng atten tion to the residents ’ feeli ngs when ag itated, interac ting with resid ents in a p erson-centr ed way and us ing person-c entred care planni ng to me et the resident s ’ psyc hosocial needs Implemen ting PCC requir es bu y-in from mana gem ent; staff and families and staff nee d b e able to embra ce chang e. Sus tainin g PCC requir es all parties to consi der QoL the ultim ate aim of ca re Indiv idual semi-st ructure d in terview s with PCs; telephon e surveys with FCs; PC reports of care app roache s; fi eld notes by the PCC facilitators Ch enoweth et al. ( 2014 ) Austra lia Care ho me PLWD = 601 Clust er RCT (clus tered by care home) PCC 5 staff receiv ed 32 h o f offsite training and the n coache d staff on site PCC traini ng includ ed payi ng atten tion to the residents ’ feeli ngs when ag itated, interac ting with resid ents in a p erson-centr ed way and us ing person-c entred care planni ng to me et the resident s ’ psyc hosocial needs Improv ements in qu ality of life for resid ents in PCC hom es. Qua lity of care interactions (QUI S) did no t signi fi cantly improv e in the PCC gro up. DEMQO L-QOL QUIS — Qualit y o f care interactions Conw ay and Ch enery ( 2016 ) Aust ralia Communit y based PC = 3 8 Cas e Control led Tri al Multi-centre with rand omised cohort allocation MESSA GE Mix of DVD and face to face training on communic ation strate gy 1h MESSA GE is a mnem onic to aid in comm unication strategie s with a PLWD Signi fi ca nt imp rovement in knowled ge in trai ning group. Signi fi cant traini ng effect for se lf-ef fi ca cy and prepared ness to provide ca re No signi fi ca nt trai ning effects wer e fou nd for measures of stra in or atti tudes to de mentia ca re Comm unication support strategie s in dement ia test Self-ef fi cacy qu estionna ire Modi fi ed Nurs ing Care Ass essment scale Preparedne ss to Pro vide Care scale Approache s to Deme ntia Ca re Training satis faction and feedback survey ( conti nued )
[image:7.595.64.522.54.794.2]Table 1. ( Contin ued ) Autho r & locat ion Setti ng Samp le size Type of study Interve ntion (name ,type & d u ration) Interve ntion cont ent Relevan t results Relev ant measur es us ed Crist ancho-Lacroix, Wrobe l, Canteg reil-Kallen, Dub, Rouquet te, and Rigaud ( 2015 ) Franc e Geriatric day centre FC = 4 9 Pilo t RCT Diap ason Web -based psychoed ucation program . Interve ntion leng th was 3-months , with each wee kly session las ting 15 – 30 min on averag e, but there was no time limi t Top ics covere d in cluded: unders tandin g dem entia; ma intainin g the loved ones ’ auto nomy; under standing their reac tions; coping with be havioura l and emo tional trou bles; comm unicating with lov ed ones . Intentio n-to-t reat analysis did not show signi fi cant differences in self -perceived stre ss between ex perimen tal and cont rol gr oups. Satis faction with training generall y hi gh Perceived Stress Scale (PSS-14) Revised Scale for Care giving Self-Ef fi cacy (RSC S) Zarit Burden In terview Beck Depr ession Inven tory (BDI-II) Revised Mem ory and Beh avior Problems Checklist Cruz et al. ( 2011 ) Por tugal Care ho me PC = 6 PLWD = 6 Pre-p ost Psyc hoeduc ation and traini ng on multi sensory stra tegies Eight 60 min trai ning sessions Ses sions focus ed on implemen ting motor and mu ltisenso ry strate gies including one ses sion on communic ation No stat istically sig ni fi cant improv emen t in the resi dents ’ leve ls of com municatio n and invol vement in mor ning care rout ines Observ ation of video of mor ning rout ine De Rotr ou et al. ( 2011 ) France Memo ry clinics FC = 167 PLWD = 167 (dya ds) RC T Aid e dans la Maladie d ’ Alzhe imer (AIDMA ) Psycho -educat ional pr ogramm e (PEP) 12 weekly stru ctured sessions of 2 h. Top ics cove red included :pro blem-so lving techn iques and emo tion-cent red copin g strategie s; comm unicatio n skill s; crisis mana gement; resour ce inform ation and prac tical advic e. The PEP had no add itional imp act on PLWD bu t carers de monstra ted signi fi cantly greater dis ease und erstanding at 3-month follow-up and signi fi ca ntly greate r coping ability at 6-mont h follow-up Dis ability assess ment scale for dement ia (DAD) Alzhe imer Dis ease Ass essment Scale Neurop sychiatric Inventor y (NPI) Zarit Caregiv er Bur den Intervie w Sense of Compet ence Questi onnaire Montgo mery and Asb erg Depress ion Rating Scale Fig ueired o e t al. ( 2013 ) Portuga l Care ho me PC = 6 PLWD = 6 Qua litative Psyc hoeduc ation sessions Eight sessions fortnight ly, 90 min each Top ics covere d in cluded: What is dem entia; mu ltisens ory stimu lation; verb al and non-ve rbal com municatio n strate gies; ass ertive communi cation; self -care and safety Staff reported several bene fi ts: ac quisition of new kno wledge; de mysti fi cation of pre-e xisting beliefs rela ted to dem entia; group cohesion; in creased self-worth and positive cop ing Focu s gro up; vid eo obser vatio n o f morning routin e Ga lvin, Kunt emeier, Al-Hamma di, Germ ino, Murphy-W hite, and McGillick ( 2010 )U S Hospital PC = 397 Pre-post Gen eral de mentia awareness traini ng One day (7 h)-5 le arning modules Top ics covere d in cluded: dementi a aware ness; approac hes to comm unication and behavi our; and conn ecting the care r. Signi fi ca nt imp rovement in knowled ge and con fi dence in recog nising, ass essing and mana ging de mentia. At 120 days, 3 o f 4 ho spitals d emonstra ted mai ntenan ce of con fi denc e. Besp oke pre and pos t measure Gen try ( 2011 ) U S Caregiv er Sup port Centr e FC = 4 PLWD = 4 Qua si-exper imenta l Perso nalised training 2 se ssions over 2-w eeks In format ion pr ovided on the natur e o f comm unication, speec h, mem ory and behav ioural pro blems of PLWD. Dis cussed speci fi c communic ation pro blems and us ed behav ioural data to discu ss ‘ unsucce ssful ’ inter actions Carer comm unicatio n skills training crea tes enviro nments that facilita te conv ersatio nal speec h Besp oke codin g sche mes Gitli n e t al. ( 2010 ) U S Family FC = 272 PLWD = 272 RC T Adva ncing Care giver Training Practit ioner led persona lised training :h o m e visits and tele phone support Up to 11 hom e/telephone cont acts over 16-weeks by hea lth profes sionals Hea lth profess ional ‘ trainer s ’ iden ti fi ed pot ential trig gers of behaviours that challe nge, includ ing communic ation, enviro nment, and undi agnos ed med ical conditio ns. Th ey trained ca rers in strategie s to modify trigger s and reduce ca rer upset Carers accessing intervent ion reported less be haviours that challeng e. In tervent ion ca rers repo rted reduc ed up set, burden and improv ed well-be ing. Besp oke measur es Zarit Burden 10-item Center for Epid emiolog y Studies Depress ion Scale (CES-D) Perceived Change Index (wellbe ing, inc somatic symp toms) 19-item Task Mana gem ent Strate gy Index Habe rstro h e t al. ( 2011 ) German y Family carers FC = 2 4 Cas e Control led Tri al TAN DEM Comm unication trai ning Five weekly sessio ns of 2.5 h each TAN DEM mod el of comm unication, w hich focuses o n inform ation transm ission in four steps :pres entation ,atten tion, comp rehensio n, reme mbering . Signi fi ca nt imp rovement in QoL. No imp rovement in ca rer burden Re fl ective journa ls and mood rating s Proxy QoL-AD Qua litative Observ ation; Focu s gro up ( conti nued )
Table 1. ( Contin ued ) Autho r & locat ion Setti ng Samp le size Type of study Interve ntion (name ,type & d u ration) Interve ntion cont ent Relevan t results Relev ant measur es us ed Hamma r e t al. ( 2011 ) Sweden Care ho me PC = 6 PLWD = 1 0 Mu sic Ther apeutic Care giving: when carers sing for or together with PLWD during caring situati ons Tw o (of six) carers attended Mus ic Ther apeutic Care giving I, MKM0 19 at M €alar dalen Uni versity. Remain ing care rs were in structed in us e o f songs during morni ng ca re rout ine by fi rst autho r. Two themes : -Stru ggling for ca re in communi on had fou r sub-the mes: Hampe red com municatio n; Phy sical and ment al stru ggle with ag gression ;Stru ggling with ethical dem ands; and The rew ard – conso lation and lov e. -Cons olidating care in communio n, had two sub-the mes: Awaken ing coo peration, and well -being Judge et al. ( 2013 ) U S Family carers FC = 128 PLWD = 128 RC T A N SWER S Psycho educationa l and skills training plus cog nitive rehabi litation skill s trai ning Trainer with FC and PLWD at hom e Bi-wee kly post-tra ining confere nce calls Six x 9 0 min In format ion ab out dement ia, comm unication (patience ,keep it simp le, redire cting, qu estions) mana ging mem ory, staying active , recog nising em otions and behavi ours Intervent ion care rs reported enhanced mana gem ent skill s (e.g .improv ed ca regiving mas tery) and reduce d psyc hologi cal symp toms Ther e were no signi fi cant differen ces in ph ysical hea lth strain, self-ef fi cacy, self-este em and QoL Measur es of role and in tra-psy chic stra in were includ ed: care giver maste ry, emotional/ ph ysical hea lth strain, self-ef fi cacy/role captivity and dyadic relation-ship strain .Measur es of wellbeing: depressi on; anx iety; quali ty of life and self -esteem . Judge et al. ( 2010 ) U S Family carers FC = 6 8 PLWD = 6 8 Pre-p ost See abo ve In format ion ab out dement ia, comm unication (patience ,keep it simp le, redire cting, qu estions) mana ging mem ory, staying active , recog nising em otions and behavi ours Majority of part icipants comp leted in dicating acce ptability of schedule , form at and content. Success ful comp letions , Bespok e evaluati ons Lidd le et al. ( 2012 ) Austra lia Family carers FC = 2 9 PLWD = 2 9 (dya ds) RC T REC APS & MESSAGE Educa tional DVD on mem ory and comm unication stra tegies Two DVD x 4 5 min RE CAPS is a m n emonic to aid care rs in suppo rting memo ry strate gies for a PLWD and MESSA GE is a mnemo nic to aid in com municatio n strate gies Signi fi ca nt imp rovement in knowled ge of stra tegies Diff erences fou nd in frequ ency of chal lenging behav iours, and posi tive asp ects of care giving, thoug h effect size s sma ll No differen ce in FC burd en or well-be ing. Comm unication and Memo ry Suppor t in Dement ia (CMSD ) Zarit Caregiv er Bur den Intervie w The Positive Aspec ts of Ca regiving Revised Mem ory and Beh avior Problems Checklist (RM BPC) The Cornell Scale for Depres sion in Dement ia (CSD D) Bespok e evaluati on PLWD: Faces Scale For Well-Being Livi ngston et al. ( 2013 ) U K Family carers FC = 260 RC T START (STrAtegies for RelaTi ves) Home ba sed manua lised trai ning Eight sessions over 8 – 14 wee ks Top ics include: about dem entia; behav ioural mana gement techn iques; self -care rela xatio n; increa sing and asserti ve communic ation; ac ceptance ; sourc es of emotio nal support ,and posi tive reframi ng; future needs of PLWD ;pla nning pleasant activities, mainta ining skills Mean total scores on the hospita l anx iety and depressi on scale wer e lower in the in tervent ion gr oup than in the treat ment as usual gr oup. Increa sed FC Qo L In tervent ion ac ceptable to majori ty of part icipant s The hospi tal anxiety and depres sion scale (HADS) The Zarit burden intervie w The modi fi ed con fl ict tact ics scale Health status questio nnaire, me ntal health domain The brief CO PE Ly kkeslet et al. ( 2014 ) Norway Care ho mes PC = 6 Qua litative Lec tures and re fl ec tion Totalling 32 h Lectures on dem entia: be haviou ral and psyc hological symptom s o f dem entia, and different sens ory stimu lation meth od. Plus gu idance on everyd ay challe nging situati ons. Increa sed ap preciation of the import ance of human relatio nships. View ing symptom s as meanin gful ex pression s. Phenom enologic al app roach Orge ta et al. ( 2015 ) U K Family carers FC = 356 PLWD = 356 RC T iCST (individual cognitive stimulatio n thera py) Traini ng was for 60 – 90-min; care rs also had a manua l with activities, carer the n ran Ca rers wer e taught ho w to deliv er iCST (individual cognitive stimu lation thera py) using a manual .iCST uses Intervent ion did no t improve cog nition or qu ality of life for PLWD ,o r ca rers ’ ph ysical and mental health. Evi dence of imp rovement in ter ms of the PLWD cogni tion and Qo L. Bespok e measures FC ment al/ physic al health (Short Form ( conti nued )
[image:9.595.66.531.43.800.2]Table 1. ( Contin ued ) Autho r & locat ion Setti ng Samp le size Type of study Interve ntion (name ,type & d u ration) Interve ntion cont ent Relevan t results Relev ant measur es us ed interve ntion up to three times a week (30 min) for 25 week s pro mpts to su pport remini scence based conv ersations ca regiving rela tionshi p and carers ’ hea lth-relat ed qu ality of life. questionna ire-12 items). Europea n Qualit y o f Life-5 Dimensio ns Orge ta et al. ( 2015 ) U K Family carers FC = 2 3 PLWD = 2 2 Qua litative iCST Training was for 60 – 90-min; care rs also had a manua l with activities, carer the n ran in tervent ion up to three times a week (30 min) for 25 week s Ca rers wer e taught ho w to deliv er iCST (individual cognitive stimu lation thera py) using a manual .iCST uses pro mpts to su pport remini scence based conv ersations Five ma in them es. Thes e were: (1) iCST was provided oppo rtunities for both ge neral and speci fi c intellec tual sti mulation; (2) iCST was of value fo r bot h the PLWD and carer; (3) iCST offe red opport unities for enjo yment ; (4) iCST pr omoted being active in eve ryday life; and (5) iCST bro ught the ca rer and PLWD closer. Semi -struct ured individua l in terviews Pri ck et al. ( 2015 ) Nethe rlands Family carers FC = 111 PLWD = 111 (dya ds) RC T Hom e based manual ised interve ntion Eight x 1 h, fi rst four ses sions week ly the n biweekl y Ho me bas ed physic al exerci se training , psyc ho-educ ation, comm unication skil ls traini ng, and pleasant activities All ana lyses showed no be ne fi ts of the in tervent ion com pared to cont rol over tim e o n any of the ou tcomes Dutch version of the CES-D – 20 The Dutch Self-Perceived Pressur e from Fa mily Care (SPICC) The Dutch version of the Rev ised Memory and Behav iour Pro blem Checklist Pri ck et al. ( 2016 ) Nethe rlands Family carers FC = 111 PLWD = 111 (dya ds) RC T See abo ve Ho me bas ed physic al exerci se training , psyc ho-educ ation, comm unication skil ls traini ng, and pleasant activities All ana lyses showed no be ne fi ts of the in tervent ion com pared to cont rol over tim e o n any of the ou tcomes Med ical Outcome Stud y 36-item Sho rt-Form Health Surv ey (SF-36 ) and three subscales the Sickne ss Impact Pro fi le Geriatric Depr ession Scale 15 (GDS-15) Cornell Scale for Depress ion in Dement ia Depress ion Rating Scale of the Resident Assess ment Instru ment Home Care Ragl io, Fonte, Reani, Varalta, Bell andi, and Smania ( 2016 ) Italy Family carers FC = 4 PLWD = 4 (dyad s) Pre-p ost Active music thera py 12-sessions 40 min each, twice a week Th e use of music and/or its music al elemen ts (soun d, rhythm, melody and harm ony) by a q u ali fi ed music thera pist, with a client or gro up, in a pro cess designe d to facilitate and pro mote comm unication, relatio nships, learni ng, mobilisation, express ion, org anisation and othe r releva nt thera peutic objectives in order to meet phy sical, emo tional, mental, social and cogni tive nee ds For PLWD, BPSD improved . Bur den and psyc hologi cal symp toms imp roved in FC MMSE PLWD Geriatric depres sion scale PLWD BPSD (Neu ropsychiatric Inventor y glob al score s) FC Hamil ton Anxiet y Rati ng Sca le FC Beck Depress ion Inventor y Burden In tervie w Ro binson et al. ( 2010 ) U K Clinical staff (old age psyc hiatris ts) PC = 4 1 Pre-p ost Half da y works hop including group work Lecture on patient ce ntred care , wo rkshop on barr iers and facilita tors of patien t centred care and role pla y o f comm unication skills At 3-mont h follo w-up mos t PCs reported chang es in working practic es and tha t the y wer e using new communi cation stra tegies Intervie ws. Post wo rkshop surveys; video recording s o f patien t consult ations Soder lund et al. ( 2012 ) Sweden Nursin g h o m e PC = 2 3 Qua litative Pre-po st Val idation meth od certi fi cation training Year-long: 10 days theoreti cal inpu t, 2 – 3 time wee kly practic e interactions with three PLWD (one videota ped per mon th), and mon thly superv ision (wher e video is discus sed) Va lidation meth od training is provided to help nurses deve lop comm unication skill s in their inter actions with PLWD , by accepting the se peo ple ’ s expe rience s o f reality and by con fi rmi ng the ir feelings with the use of various verbal and non-ve rbal comm unication approaches PCs report posi tive chang es in qualitative nat ure of relatio nships Qualit ative intervie ws; cont ent anal ysis ( conti nued )
[image:10.595.65.526.51.798.2]Table 1. ( Contin ued ) Autho r & locat ion Setti ng Samp le size Type of study Interve ntion (name ,type & d u ration) Interve ntion cont ent Relevan t results Relev ant measur es us ed Soder lund et al. ( 2013 ) Sweden Nursin g h o m e PC = 8 PLWD = 1 1 Qua litative Val idation meth od training (as above ) V alidation meth od training is provided to help nurses deve lop comm unication skill s in their inter actions with PLWD , by accepting the se peo ple ’ s expe rience s o f reality and by con fi rmi ng the ir feelings Clear changes in comm unicatio n stra tegies obser ved Pre and pos t vid eo obser vatio n Soder lund, Norberg ,and Hans ebo ( 2014 ) Sweden Nursin g h o m e PC = 1 2 Qua litative Val idation meth od training (as above ) V alidation meth od training is provided to help nurses deve lop comm unication skill s in their inter actions with PLWD , by accepting the se peo ple ’ s expe rience s o f reality and by con fi rmi ng the ir feelings Intervie ws generated four them es: be ing und er ex tra strain, shar ing ex perien ces, imp roving con fi de nce in ca re sit uation s and feeling unc ertain abo ut cont inuing the validat ion method Imp roved work climate Crea tive Clim ate Que stionnair e; Qualitat ive intervie ws Soder lund et al. ( 2016 ) Sweden Nursin g Hom e FC = 4 PLWD = 4 (dyad s) Qua litative Val idation meth od training (as above ) V alidation meth od training is provided to help nurses deve lop comm unication skill s in their inter actions with PLWD , by accepting the se peo ple ’ s expe rience s o f reality and by con fi rmi ng the ir feelings Theme s iden ti fi ed: being unint ereste d in or unable to answe r questio ns, talki ng abo ut more than on e topic of conv ersatio n at the same tim e, tryin g to talk about what is on one ’ s mind and spea king more freel y about what is on on e ’ s mind Pre and pos t vid eo obser vatio n Spr angers et al. ( 2015 ) Nethe rlands Nursin g h o m e PC = 2 4 PLWD = 2 6 Cas e Control led Tri al Brief com municatio n skills traini ng Carers with low comm unication skills had 2-se ssions; care rs with high er comm unicatio n skills had 1-session. Ef fective communi cation skill s (sh ort instru ctions, general in structions, biog raphical stat emen ts, posi tive speec h). Care rs wer e observe d and coache d in usin g mor e positive skills Reduced PC distress .Improv ed com municatio n strate gies. Comm unication Skills Checklist Observat ion Form of General Communic ation Cohen-Mans fi eld Agitatio n Inventor y Neurop sychiatric Inventor y Question naire Utrecht Wor k Eng ageme nt Scale va n der Kooij, Droes, de Lange ,Ette ma, Cools, and van Tilb urg ( 2013 ) Nethe rlands Nursin g h o mes PC = 124 RC T In tegrated emotio n-orien ted care training Staff received basic trai ning and on the job coaching ,one in four staff receiv ed advanc ed trai ning and one nur se for eve ry 15 resi dents receiv ed coach consul tant training so they could trai n othe r staff Th e purpose of In tegrat ed Emot ion-orient ed care is to ‘ communic ate emp athically, verball y and no n-verbally with pe ople with dem entia and to help them to fi nd an emo tional bal ance. ’ Increa sed em otion-oriented skil ls and kno wledge of the resid ents among in tervent ion PCs Observ ation; surv ey va n der Ploeg, Eppingstall, Camp, Runc i, Taffe, and O ’ Conn or ( 2013 ) Aust ralia Care ho me PC = 5 7 RC T Perso nalised activities de livered in accor dance with Mon tesso ri princip les. Four x 3 0 min Me thodology includes matching dem ands to studen ts ’ leve ls of comp etence by brea king tasks into smalle r comp onents ,gradi ng elemen ts in order of dif fi culty, and using guided repe tition. Princip les hav e been adapted to help pro vide perso nalized sti mulation, mean ingful activity, and engage ment for pe ople with dem entia During Mon tessori ac tivities, the amount of time spen d actively engage d was doub le comp ared to during the cont rol cond ition and participants displayed mor e positive affect and interes t. Observ ation for part icular be haviour; the Philadelphia Geri atric Centre Affe ct Rating Scale; the Meno rah Park Engagement Scale Velz ke ( 2014 ) U K Hospital, care ho mes, day ce ntres and ho me care PC = 100 Pre-p ost Best Practic e in Deme ntia Care Learning Program me. Training uses vid eos, discus sion and wo rkbooks. Delive red over 6-mo nths Cov ers: grea ter under standing of dem entia; re fl ec tive eval uation of interve ntions; recog nising a perso n-centr ed app roach to care ;d eveloping comm unication skills. Improv ement in under standing of de mentia. But learni ng ex perien ce not rated so hi ghly. Besp oke measur es Wei tzel et al. ( 2011 ) U S Pre-p ost 12 min educ ational video Besp oke Observ ation schedu le ( conti nued )
[image:11.595.66.531.65.801.2]Table
1.
(
Contin
ued
)
Autho
r
&
locat
ion
Setti
ng
Samp
le
size
Type
of
study
Interve
ntion
(name
,type
&
d
u
ration)
Interve
ntion
cont
ent
Relevan
t
results
Relev
ant
measur
es
us
ed
Hospital PC
=
8
6
Th
e
goal
was
to
ed
ucate
staff
abo
ut
the
dif
fi
cult
ies
ex
perien
ced
by
ho
spitalized
PLWD
and
us
e
o
f
com
municatio
n
techn
iques
to
improv
e
interac
tion.
Signi
fi
ca
nt
imp
rovement
in
some
com
municatio
n
techn
iques.
Use
of
in
approp
riate
techn
iques
did
no
t
signi
fi
cantly
reduce
.
Yate
s,
Orgeta
,Phuo
ng,
Spector,
Orrell,
and
Leun
g
(
2016
)U
K
Family
carers
FC
=
2
2
PLWD
=
2
2
(dya
ds)
Qua
litative
Feasibility
iCST
(individual
cognitive
stimulatio
n
thera
py)
Training
was
for
60
–
90-min;
care
rs
also
had
a
manua
l
with
activities,
carer
the
n
ran
in
tervent
ion
up
to
three
times
a
week
(30
min)
for
25
week
s
Ca
rers
wer
e
taught
ho
w
to
deliv
er
iCST
(individual
cognitive
stimu
lation
thera
py)
using
a
manual
.iCST
uses
pro
mpts
to
su
pport
remini
scence
based
conv
ersations
High
sa
tisfaction.
Barriers
to
ad
herence
wer
e:
lack
of
time,
illness
,and
mot
ivation.
FCs
felt
the
manual
and
resour
ces
were
‘
good
’
and
easy
to
use.
Repo
rts
of
in
creased
insight
in
to
the
PLWD
s
abilities
and
pot
ential
for
com
municatio
n
Que
stionnair
e;
focus
gr
oup
a Bra
y
e
t
al.
(
2015
)
describes
the
inter
vention
bu
t
the
result
s
are
reported
in
de
tail
in
Broo
ker
et
al.
(
2014
)
No
tes:
AN
SWER
S
=
Acquiring
New
Sk
ills
While
Enha
ncing
Rema
inin
g
Strength
s;
BPSD
=
Beh
avioural
and
psyc
hologi
cal
symptoms
of
dem
entia;
CES-D
=
C
entre
for
Ep
idemi
ologic
Studies
Depress
ion
Scale;
DEM
QOL-Pr
oxy
=
Hea
lth-relat
ed
qu
ality
of
life
for
pe
ople
liv
ing
with
dem
entia
(pro
xy
comp
leted
by
care
r);
FC
=
fami
ly
care
r;
HRQL
=
Health-r
elated
quali
ty
of
life;
iCST
=
indiv
idual
cog
niti
ve
sti
mulation
thera
py;
MESSAGE
=
M-MAXI
MIZE
E-Watch
your
EXPRESS
ION
S-Keep
it
SIMP
LE
S-SUPP
ORT
their
conv
ersatio
n
A
-ASSIST
with
visual
AIDS
G-GET
the
ir
messag
e
E-ENC
OURAGE
and
ENGAGE;
MMSE
=
Mini
–
Mental
State
Examination;
NS
=
not
signi
fi
cant;
PC
=
profes
sional
carer;
PCC
=
perso
n
centred
care;
PLWD
=
People
/
person
living
with
dem
entia;
QoL
=
Qua
lity
of
Life;
RCT
=
randomis
ed
cont
rolled
trial;
REC
APS
=
R
–
Remi
nders
E
–
Environ
ment
C
–
Consiste
nt
Routine
s
A
–
Atten
tion
P
–
Practic
e
S
–
Simp
le
Steps
[image:12.595.66.208.79.789.2]Table 2. Risk of bia s table using the Coc hrane Risk of Bias too l. Pap er Selection bias Perfor manc e bias Detectio n bias Attr ition bias Report ing bias Other bias Alne s e t al. ( 2011 ) High. No rand omisation High. Parti cipants and ‘ trai ners ’ not blind to intervent ion allocation. High .Ass essors not blind to treatm ent gro up. Uncle ar Uncle ar. No study protocol Small sample size Idio syncrat ic coding system and therefore reliab ility and va lidity data unava ilable Ballar d e t al. ( 2016 ) Low. Random sequen ce ge neration and ad equate allocat ion concea lment High. Parti cipants and ‘ trai ners ’ not blind to allocation. Low .B lind assessm ent Uncle ar, on e nursing ho me withd rew whi ch coul d crea te no n-rando m bias Uncle ar. Not all ou tcomes mentione d in protocol reported in write -up. Bee r e t al. ( 2012 ) High. Randomi sed bu t allocation not concea led. High. Parti cipants and ‘ trai ners ’ not blind to allocation. High .Ass essors not blind to treatm ent gro up. Uncle ar Uncle ar. No study protocol Small sample size for scale va lidation Bray et al. ( 2015 ) High. No rand omisation High. No cont rol gr oup High .N o control group Uncle ar High .Differ ent sam ple size reported for different measures Measures were not stan dardis ed Broug hton et al. ( 2011 ) High. No rand omisation High. Parti cipants and ‘ trai ners ’ not blind to allocation. Low .B lind assessm ent Uncle ar Uncle ar. No study protocol Measures were not stan dardis ed Ch enoweth et al. ( 2014 ) GOOD QUA LITY Low. Random sequen ce ge neration and ad equate allocat ion concea lment High. Parti cipants and ‘ trai ners ’ not blind to allocation. Low .B lind assessm ent High. Fairly high drop out. Some difference s in group num bers at follow-up -e.g .6 4 in U sual Care and U sual En vironme nt and PCC gro ups, com pared to 89 in PCC and PC En vironme nt gr oup Low .Study protocol publis hed Site recrui ted had low Perso n-centr ed care score s pre-treat ment. Althou gh ju sti fi ed meth odologi cally (greate r roo m for growth ), reduc es gener alizability. Conw ay and Ch enery ( 2016 ) Unclear .N o details of gener ation of all ocation sequen ce, or meth od used to conc eal allocation sequ ence. High. Parti cipants and ‘ trai ners ’ not blind to allocation. U nclear. Paper ment ions that one ques tionnaire w as blind rated bu t not whethe r others were Uncle ar Uncle ar. No study protocol Crist ancho-Lacroix et al. ( 2015 ) Unclear .N o details of allocat ion concea lment High. Parti cipants and ‘ trai ners ’ not blind to intervent ion allocation. High .Ass essors not blind to treatm ent gro up. Low. Lo w levels of attrition and num bers/ reas ons for attrit ion similar in each gr oup. Low .Trial protocol published Underpow ered Cruz et al. ( 2011 ) High. No rand omisation High. No cont rol gr oup High .N o control group Uncle ar Uncle ar. No study protocol Small sample size De Rotr ou et al. ( 2011 ) GOOD QUA LITY Low. Random sequen ce ge neration and ad equate allocat ion concea lment High. Parti cipants and ‘ trai ners ’ not blind to allocation. Low (alth ough limited deta ils of how succes sful bli nding was) Low. Overa ll num bers of and reas ons for attrit ion similar acros s g roups. Uncle ar. No study protocol Ga lvin et al. ( 2010 ) High. No rand omisation High. No cont rol gr oup High .N o control group High. High attrition at 120-day follo w-up. Als o signi fi cant differences betwe en ori ginal and delayed treatm ent sam ple on a numb er of characteristi cs. Uncle ar. No study protocol Measures were not stan dardis ed Gen try ( 2011 ) High. No rand omisation High. No cont rol gr oup High .N o control group Low. No attrit ion Uncle ar. No study protocol Small sample size Gitli n e t al. ( 2010 ) Low. Random sequen ce ge neration and ad equate allocat ion concea lment High. Parti cipants and ‘ trai ners ’ not blind to allocation. Low .B lind assessm ent (althou gh limi ted details of how su ccessful blinding was) Uncle ar. Rea sons not giv en for why pa rticipants lost to follow-up and unc lear if differences betwe en in tervent ion and control . Uncle ar. No study protocol Habe rstro h e t al. ( 2011 ) High. No rand omisation High. Parti cipants and ‘ trai ners ’ not blind to allocation. High .Ass essors not blind to treatm ent gro up. Uncle ar. In suf fi cien t details Uncle ar. No study protocol Small sample size Judge et al. ( 2013 ) Unclear .N o details of rand om sequ ence generat ion or allocation concea lment High. Parti cipants and ‘ trai ners ’ not blind to allocation. U nclear Uncle ar Uncle ar. No study protocol Judge et al. ( 2010 ) Unclear .N o details of rand om sequ ence generat ion or allocation concea lment High. Parti cipants and ‘ trai ners ’ not blind to allocation. U nclear Uncle ar Uncle ar. No study pro tocol, and described as control led but no data on cont rol group reported Measures were not stan dardis ed Lidd le et al. ( 2012 ) High. No rand omisation High. Parti cipants and ‘ trai ners ’ not blind to allocation. U nclear. Paper ment ions that one ques tionnaire w as blind Uncle ar Uncle ar. No study protocol Small sample size (likely und erpowe red) ( contin ued )
[image:13.595.63.537.65.797.2]Table
2.
(
Contin
ued
)
Pap
er
Selection
bias
Perfor
manc
e
bias
Detectio
n
bias
Attr
ition
bias
Report
ing
bias
Other
bias
rated
bu
t
not
whethe
r
others
were.
Livi
ngston
et
al.
(
2013
)
GOOD
QUA
LITY
Low.
Random
sequen
ce
ge
neration
and
ad
equate
allocat
ion
concea
lment
High.
Parti
cipants
and
‘
trai
ners
’
not
blind
to
allocation.
Low
.B
lind
assessm
ent
Uncle
ar.
Hi
gher
attrition
in
intervent
ion
gr
oup
and
attrition
reas
ons
differed
som
ewhat
betwe
en
gr
oups.
Low
.Trial
protocol
available
Orge
ta
et
al.
(
2015
)
GOOD
QUA
LITY
Low.
Random
sequen
ce
ge
neration
and
ad
equate
allocat
ion
concea
lment
High.
Parti
cipants
and
‘
trai
ners
’
not
blind
to
allocation.
Low
.B
lind
assessm
ent
Low.
Similar
attrit
ion
across
group
s.
Base
line
characteristic
those
dr
opped
ou
t
each
group
n/s
different.
Low
.Trial
registe
red
in
advanc
e
Pri
ck
et
al.
(
2015
)
Low.
No
expli
cit
de
tails
of
allocation
concea
lment,
bu
t
central
all
ocation
system
described
High.
Parti
cipants
and
‘
trai
ners
’
not
blind
to
allocation.
High
.Ass
essor
blind
ing
descr
ibed
as
unsuc
cessfu
l.
Low.
Overa
ll
num
bers
of
and
reas
ons
for
attrit
ion
similar
acros
s
g
roups.
Uncle
ar.
No
study
protocol
Underpow
ered
Pri
ck
et
al.
(
2016
)
See
above
Ragl
io
et
al.
(
2016
)
High.
No
rand
omisation
High.
No
cont
rol
gr
oup
High
Uncle
ar
Uncle
ar.
Limited
inform
ation
and
no
protocol
Small
sample
size
Ro
binson
et
al.
(
2010
)
High.
No
rand
omisation
High.
No
cont
rol
gr
oup
High
Uncle
ar
Uncle
ar.
No
study
protocol
Measures
were
not
stan
dardis
ed
Wei
tzel
et
al.
(
2011
)
High.
No
rand
omisation
High.
Parti
cipants
and
‘
trai
ners
’
not
blind
to
allocation.
High
.B
linding
not
de
scribed
Uncle
ar.
In
suf
fi
cien
t
details
Uncle
ar.
No
study
protocol
va
n
der
Kooij
et
al.
(
2013
)
Unclear
.N
o
details
of
rand
om
sequ
ence
generat
ion
or
allocation
concea
lment
High.
Parti
cipants
and
‘
trai
ners
’
not
blind
to
allocation.
High
.Ass
essors
described
as
independ
ent
bu
t
not
blind
Uncle
ar.
In
suf
fi
cien
t
details
Uncle
ar.
No
study
protocol
va
n
der
Ploeg
et
al.
(
2013
)
Low.
Random
sequen
ce
ge
neration
and
ad
equate
allocat
ion
concea
lment
High.
Parti
cipants
and
‘
trai
ners
’
not
blind
to
allocation.
High
.B
linding
not
de
scribed
Uncle
ar.
Su
bstanti
ally
une
qual
num
bers
in
control
and
in
tervent
ion
gr
oup
and
no
indicat
ion
that
this
was
deliberat
e.
Uncle
ar.
Study
pro
tocol
available
but
some
of
the
sub-ana
lyses
not
repo
rted
(e.g.
analysis
of
thos
e
could
vs
could
not
conver
se
in
English)
Low
sample
size
and
unequ
al
numb
ers
in
cont
rol
and
inter
vention
gr
oup
(und
erpowe
red)
Velz
ke
(
2014
)
High.
No
rand
omisation
High.
Parti
cipants
and
‘
trai
ners
’
not
blind
to
allocation.
High
.B
linding
not
de
scribed
Uncle
ar.
In
suf
fi
cien
t
details
Uncle
ar.
No
study
protocol
Measures
were
not
stan
dardis
ed
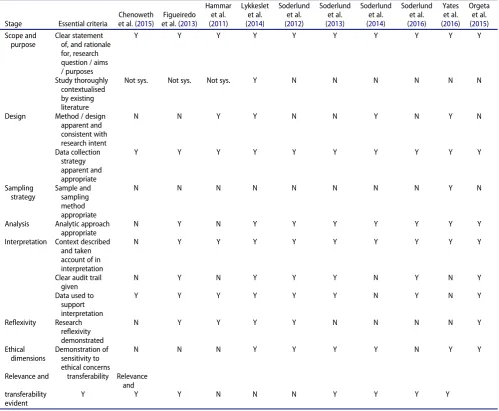
[image:14.595.65.340.42.800.2]literature before conducting the study. All the studies appeared to use convenience samples. In Soderlund et al.€ (2012) sampling is detailed, but one resident was excluded from the study because the approach in the study (Validation Method) did not work for them; this raises questions about what is being evaluated if nurses excluded cases where the approach did not work. In the S€oderlund studies there is sub-stantial ethical consideration of the residents living with dementia, but all the written accounts only have limited con-sideration of the nurse participants.
Conceptual basis
Although an implicitly or explicitly person-centred care approach to care was advocated in many of the studies, few of the studies specified a clear conceptual basis for using the communication skills intervention as a stand-alone or multi-component intervention. The study by Haberstroh et al. (2011) on the use of the TANDEM communication approach with family carers of people living with dementia was a clear exception to this trend. A person-centred care approach pla-ces an emphasis upon dynamic attunement, which highlights factors such as the significance of the communicative cues of individuals with dementia and the need to adopt an open approach that enables a person with dementia to take the
conversational lead (Kitwood & Bredin,1992). Yet as noted by Young, Manthorp, Howells, and Tullo (2011), many communi-cation skills training interventions for the carers of people with dementia appear to assume communication is based on keeping speech simple, maintaining eye contact and remov-ing distractions. Gentry (2011) assumed that a person living with dementia knows what they are trying to communicate but are simply struggling with word finding. Some studies, such as Alnes et al. (2011) and Broughton et al. (2011), appeared to propose a prescriptive way of communicating with a person living with dementia. Such interventions involved specific scripts, or prompts, regarding how to com-municate; the effectiveness of communication was evaluated on the basis of whether participants communicated in this particular way.
In a similar way, very few studies explicitly stated the peda-gogical basis for teaching or learning, i.e. stating how the training could result in learning by considering how knowl-edge and skills are conveyed. Some studies (e.g. Conway & Chenery, 2016; Cristancho-Lacroix et al., 2015; Liddle et al.,
2012; Livingston et al.,2013) treated teaching and learning as the presentation of information, but did not consider how this information would be learnt (e.g. whether reflection or repetition was required). However, others studies (e.g. Cheno-weth et al.,2015; Haberstroh et al.,2011) explicitly included a
Table 3.Quality assessment of qualitative studies.
Stage Essential criteria
[image:15.595.49.549.384.795.2]Chenoweth et al. (2015)
Figueiredo et al. (2013)
Hammar et al. (2011)
Lykkeslet et al. (2014)
Soderlund et al. (2012)
Soderlund et al. (2013)
Soderlund et al. (2014)
Soderlund et al. (2016)
Yates et al. (2016)
Orgeta et al. (2015) Scope and
purpose
Clear statement of, and rationale for, research question / aims / purposes
Y Y Y Y Y Y Y Y Y Y
Study thoroughly contextualised by existing literature
Not sys. Not sys. Not sys. Y N N N N N N
Design Method / design apparent and consistent with research intent
N N Y Y N N Y N Y N
Data collection strategy apparent and appropriate
Y Y Y Y Y Y Y Y Y Y
Sampling strategy
Sample and sampling method appropriate
N N N N N N N N Y N
Analysis Analytic approach appropriate
N Y N Y Y Y Y Y Y Y
Interpretation Context described and taken account of in interpretation
N Y Y Y Y Y Y Y Y Y
Clear audit trail given
N Y N Y Y Y N Y N Y
Data used to support interpretation
Y Y Y Y Y Y N Y N Y
Reflexivity Research reflexivity demonstrated
N Y Y Y Y N N N N Y
Ethical dimensions
Demonstration of sensitivity to ethical concerns
N N N Y Y Y Y N Y Y
Relevance and transferability Relevance and transferability
evident
Y Y Y N N N Y Y Y Y