Case Report
Clear cell variant of diffuse large B-cell lymphoma: a
case report and review of the literature
Yongjie Xue1, Qiulan Wang2, Xuejiao He1
1Department of Pathology, San Ai Tang Hospital, Lanzhou, China; 2Clinical College, Gansu University of Chinese Tranditional Medicine, Lanzhou, China
Received April 12, 2015; Accepted May 27, 2015; Epub June 1, 2015; Published June 15, 2015
Abstract: Diffuse large B cell lymphoma (DLBCL) is a diffuse proliferation of large neoplastic B lymphoid cells with nuclear size equal to or exceeding that of normal macrophage nuclei. The DLBCL morphological variants are centro-blastic, immunocentro-blastic, T-cell- and histiocyte-rich, anaplastic, plasmacentro-blastic, anaplastic lymphoma kinase-positive, and primary mediastinal large B-cell lymphoma (PMBCL). These histopathologically-recognized morphological vari-ants respond differently to treatment and have distinct prognoses. We report a case of a 43-year-old patient who presented pain in the lower abdomen that had begun four months prior. Ultrasound-guided biopsy revealed epi-thelial cell features and a partial alveolar growth pattern. We discovered large diffuse areas comprising large cells with slightly irregular nuclei and very clear cytoplasm. These features were similar to those of clear cell carcinoma in renal tissue, suggesting the possibility of an epithelial neoplasm. To test this possibility, immunohistochemistry for cluster designation markers was performed, but the diffuse areas were found to be positive only for CD45. Additional immunohistochemistry was performed, and the diffuse areas were found to be positive for CD20, CD79a, P53, and Mum-1. Based on these characteristics, a diagnosis of a clear cell variant of DLBCL was made, and the pa-tient was treated with chemotherapy. Precise histological diagnosis is crucial for clinical management and ultimately for patient survival. There has been one additional report of a case of clear cell DLBCL, in outside the mediastinum. The features we identified can be used to define a new subtype of DLBCL. The expression of P53 and Mum-1 sug -gest a poor prognosis.
Keywords: Diffuse large B-cell lymphoma, retroperitoneal, CD45, CD20, clear cell, morphology, newly defined enti -ties
Introduction
Diffuse large B cell lymphoma (DLBCL), a sub-type of non-Hodgkin’s lymphoma (NHL), is the most common type of lymphoid tumor world-wide, accounting for 30%-40% of adult NHLs, according to the World Health Organization’s (WHO) classification of neoplastic diseases of hematopoietic and lymphoid tissues [1]. DLBCL exhibits striking heterogeneity at the clinical, genetic, and molecular levels [2]. The tumor may arise as a primary tumor or as a result of the progression and transformation of a less aggressive lymphoma [3-5].
This heterogeneous group of lymphoid neo-plasms is characterized by diverse spectra of clinical and morphological features [5], res- ponses to therapy, and survival [6-9]. In
We present a case of primary DLBCL with clear cell morphology in the retroperitoneal space, with a review of the literature. According to the results of immunohistochemistry (IHC), the patient presents non- germinal center B cell-like (non-GCB) DLBCL, suggesting a poor pro- gnosis.
Case presentation
[image:2.612.90.379.75.404.2]The patient was a 43-year-old woman who pre-sented with the chief complaint of painful swell-ing in the lower abdominals. She was admitted to the hospital due to complaints of fatigue, diz-ziness and intermittent lower abdominal pain without obvious incentives. Symptoms had begun 5 months before admittance and had
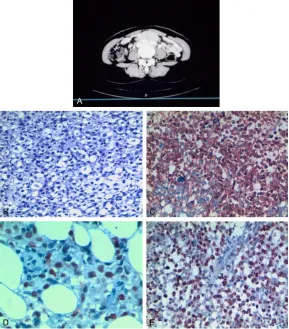
Figure 1. A. Computed tomography (CT) images. soft tissue mass beneath the lower and medial peritoneum. B. H&E staining. Sheets of large cells with abundant clear cytoplasm and with distinct cell boundaries. Nuclei were oval or irregular in shape and were deeply stained. Original magnification, × 200. C. Immunohistochemical staining. CD20+ expressed positivity. Original magnification, × 200. D. Immunohistochemical staining. Mum-1+ expressed
Cell nuclei positiviy; original magnification, × 400. E. Immunohistochemical stainig Ki-67+ expressed a high proliferation index (Ki-67 staining, 70%), Original magnification × 200.
obvious invasion in the vertebral body. The mass had a CT value of 44.0 HM, a maximum area of 5.28 cm × 4.27 cm, and unclear bound-aries with the surrounding tissues. When enhanced scanning was performed, arterial phase enhancement was not obvious and the CT value was approximately 48.9 HM. The intra-peritoneal lymph node was not enlarged. Plain film X-rays of the anteroposterior and lateral chest were normal without mediastinal enlarge-ment. CT inspection revealed no masses in liver, kidney, lung, adrenal gland and brain. B ultrasound examination showed a homoge-neous and relatively hypo-echoic area with a size of 6.2 cm × 3.5 cm around the abdominal aorta, behind the peritoneum and in front of the vertebral column. This area presented clear boundaries, a fairly regular shape, and regular internal echo. Blood routine examination, liver function testing, and biochemical testing found no abnormalities. B ultrasound-guided tumor puncture was performed two days after the patient was admitted to our hospital. A gray-white tissue with a length of 2 cm and a diam-eter of 2 mm was extracted. Conventional sec-tioning showed relatively homogeneous trans-parent cells that were analogous to renal clear cell carcinoma of medium size. Most cells were irregularly polygonal or ovoid in shape, with dis-tinct cell boundaries and clear cytoplasm (Figure 1B). Nuclei were oval or irregular in shape and were deeply stained. Large nucleoli were observed in some of the nuclei. Massive necrosis accounted for 15% of the tumor tis-sue. A small number of fat cells were found in the tumor tissue without obvious interfibrillar substance. The preliminary consideration was an epithelial mesenchyme-derived malignant tu- mor. To test this possibility, IHC was carried out using antibodies for vimentin, Syn, CD34, CD117, S-100, HMB45, CKpan, CKlow, and CD45. CD45 was strongly expressed, but the tissue was negative for the rest of the epitheli-um and mesenchyme antibodies, suggesting that the tumor was not an epithelial mesen-chyme-derived malignant tumor. Next, retroper-itoneal lymphoma was considered, and a sec-ond round of IHC staining was performed. Antibodies were selected for their roles in the diagnosis and classification of lymphoma. Strong positive labeling was observed for CD20 (Figure 1C) and CD79a (+++) as well as for P53 and MUM-1 (++) (Figure 1D). In addition, appro- ximately 70% of nuclei were positive for KI67 (Figure 1E). The tissue was negative for CD10,
CD21, CD30, Bcl-2, bcl-6, CD3 and ALK. Based on these characteristics, we diagnosed the tumor as a clear cell variant of DLBCL, non-GCB type. R-CHOP was chosen as the clinical thera-peutic protocol.
Discussion
DLBCL is a moderately to highly malignant B cell-derived tumor with significant heterogene-ity. This heterogeneity is present not only in its complex and diverse clinical manifestations, histological features [4], immune phenotypes, and genetic characteristics, but also in the inconsistent responses of DLBCL patients to treatment and their different prognoses [5, 13, 14]. In the WHO classifications of 2001 and 2008 [15, 16], variants of DLBCL were defined according to the belief that they represent dis-tinct clinico-pathologic entities [17]. As such, the pathomorphological changes found in tumors can be used for diagnostic purposes and to guide treatment. In the case we present-ed, the tumor cell morphology was different from that of common variants of DLBCL. Instead, the transparent and lightly stained tumor cell cytoplasm gave the initial impression that the condition was metastatic clear cell car-cinoma or another clear cell tumor. This case suggests that the heterogeneity of DLBCL is greater than previously thought, as tumor cells can have morphological changes outside of those present in more common variants of DLBCL. Such differences in morphology pres-ent a great challenge for pathological diagno-sis. Had no IHC techniques been applied, the pathological diagnosis in this case would have been incorrect. In pathological and differential tumor diagnosis, a variation of DLBCL should be considered after epithelial and mesenchy-mal tumors are excluded by IHC. This case emphasizes that correct pathological diagnosis requires the use of several pathological tech-niques, especially IHC.
fre-quently invades adjacent structures and repre-sents bulky disease [20]. PMBCL is morphologi-cally heterogeneous, but is mainly composed of large cells with abundant, clear cytoplasm and round to ovoid nuclei. Diagnosis is further com-plicated by the occasional presence of Reed-Sternberg like cells, which raises the suspicion of classical Hodgkin lymphoma (CHL) [20]. We excluded a diagnosis of PMBCL when IHC showed the tumor cells were negative for the PMBCL marker CD30. A diagnosis of systemic DLBCL with secondary mediastinal involvement also had to be excluded. Dissemination outside the mediastinum commonly occurs in cases of relapse and involves extranodal sites such as the kidney, liver, adrenal glands, or central ner-vous system [20].
The patient in this case was free from respira-tory symptoms, and CT examination showed no tumor in the mediastinum, kidney, liver, adrenal glands, or central nervous system. In addition, IHC showed the tumor was negative for CD30. Based on these characteristics, the lesion was not considered to originate from the mediasti-num, but was instead considered a retroperito-neal primary lesion. The diagnosis as a clear cell variant is indicative of a very significant morphological variation of DLBCL.
Gene expression profile (GEP) studies have confirmed that DLBCL can be divided into sub-types according to its gene signature. These subtypes include germinal center B-cell (GCB) or GCB-like, activated B-cell (ABC) or ABC-like, and type 3 DLBCL [21, 22]. In addition to their specific gene signatures, these DLBCL sub-types are associated with different molecular signaling pathways and clinical outcomes [23, 24]. Patients with GCB-DLBCL have significant-ly better overall survival than those with ABC-DLBCL [25, 26]. Because GEP is expensive and not readily available in routine practice, several algorithms [27, 28] have been proposed in recent years as alternative diagnostic tools for GEP. These algorithms have been based on IHC staining or tissue microarray analysis, which is a surrogate for GEP analysis [27, 28].
According to the Hans [9, 13] classification standard, the case we presented belonged to the non-GCB subtype of DLBCL due to the IHC staining results, which showed the tumor was negative for Bcl-2, Bcl-6, and CD10, and posi-tive for Mum-1. This indicates a poor prognosis.
We performed a search of the literature world-wide and found a case reported by Suzana Manxhuka-Kerliu in 2011 [4]. Both this patient and the one in our case are at middle age and are pathologically typed as non-GCB.
Conclusion
Based on our IHC findings, we diagnosed the present case as a clear cell variant of DLBCL of activated cell type, post-germinal center cell origin. Clear cell morphology is atypical of DLBCL, and may represent an otherwise unspecified variant of DLBCL. Our patient is alive and undergoing R-CHOP chemotherapy treatment. Due to time restrictions, the treat-ment has not been completed and further observation is required.
Disclosure of conflict of interest None.
Address correspondence to: Dr. Yongjie Xue, Depart- ment of Pathology, San Ai Tang Hospital, 74 South Jingning Road, Lanzhou 730030, Gansu, P.R. China. Tel: +86-13919765305; Fax: +86-9318150897; E-mail: [email protected]
References
[1] Menon MP, Pittaluga S, Jaffe ES. The Histologi-cal and BiologiHistologi-cal Spectrum of Diffuse Large B-cell Lymphoma in the WHO Classification. Cancer J 2012; 18: 411-420.
[2] Abramson JS, Shipp MA. Advances in the biol-ogy and therapy of diffuse large B-cell lympho-ma: moving toward a molecularly targeted ap-proach. Blood 2005; 106: 1164-1174. [3] De Paepe P, Achten R, Verhoef G, Wlodarska I,
Stul M, Vanhentenrijk V, Praet M, De Wolf-Peeters C. Large cleaved and immunoblastic lymphoma may represent two distinct clinico-pathologic entities within the group of diffuse large B-cell lymphomas. J Clin Oncol 2005; 23: 7060-7068.
[4] Nayak PB, Desai D, Pandit S, Rai N. Centro-blastic variant of diffuse large B-cell lympho-ma: Case report and review of literature. J Oral Maxillo Pathol 2013; 17: 261-265.
[5] Martelli M, Ferreri AJ, Agostinelli C, Di Rocco A, Pfreundschuh M, Pileri SA. Diffuse large B-cell lymphoma. Crit Rev Oncol Hematol 2013; 87: 146-171.
B-cell lymphoma (DLBCL). Blood 2003; 101: 4279-4284.
[7] Carbone A, Gloghini A, Kwong YL, Younes A. Diffuse large B cell lymphoma: using patho-logic and molecular biomarkers to define sub -groups for novel therapy. Ann Hematol 2014; 93: 1263-1277.
[8] Gurbuxani S, Anastasi J, Hyjek E. Diffuse large B-cell lymphoma-more than a diffuse collec-tion of large b cells: An entity in search of a meaningful classification. Arch Pathol Lab Med 2009; 133: 1121-1134.
[9] Hans CP, Weisenburger DD, Greiner TC, Gas-coyne RD, Delabie J, Ott G, Müller-Hermelink HK, Campo E, Braziel RM, Jaffe ES, Pan Z, Farinha P, Smith LM, Falini B, Banham AH, Ros-enwald A, Staudt LM, Connors JM, Armitage JO, Chan WC. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue mi-croarray. Blood 2004; 103: 275-282.
[10] Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. Blood 2011; 117: 5019-5032.
[11] Rosenwald A, Wright G, Chan WC, Connors JM, Campo E, Fisher RI, Gascoyne RD, Muller-Her-melink HK, Smeland EB, Giltnane JM, Hurt EM, Zhao H, Averett L, Yang L, Wilson WH, Jaffe ES, Simon R, Klausner RD, Powell J, Duffey PL, Longo DL, Greiner TC, Weisenburger DD, Sanger WG, Dave BJ, Lynch JC, Vose J, Armit-age JO, Montserrat E, López-Guillermo A, Gro-gan TM, Miller TP, LeBlanc M, Ott G, Kvaloy S, Delabie J, Holte H, Krajci P, Stokke T, Staudt LM; Lymphoma/Leukemia Molecular Profiling Project. The use of molecular profiling to pre -dict survival after chemotherapy for diffuse large-B-cell lymphoma. N Engl J Med 2002; 346: 1937-1947.
[12] Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW. WHO classification of tumours of haematopoietic and lymphoid tissues, 4th edition. IARC, Lyon. [13] Cultrera JL, Dalia SM. Diffuse Large B-Cell
Lym-phoma: Current Strategies and Future Direc-tions. Cancer Control 2012; 19: 204-213. [14] Dominis M, Dzebro S, Gasparov S, Pesut A,
Ku-sec R. Diffuse large B-cell lymphoma and its variants. Croat Med J 2002; 43: 535-540. [15] Gatter KC, Warnke RA. Diffuse large B-cell
lym-phoma. In Pathology Genetics of Tumours of Haematopoietic and Lymphoid Tissues: IARC WHO Classification of Tumours. Volume 3. 3th edition. In: Jaffe ES, Harris NL, Stein H, Vard-iman JW, editors. Lyon, France: IARC Press; 2001. pp. 171-174.
[16] Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW. In
WHO Classification of Tumours of Haema-topoietic and Lymphoid Tissues (IARC WHO Classification of Tumours). Volume 2. 4 edi -tion. Geneva: World Health Organization; 2008.
[17] Terada T. Diffuse large B-cell lymphoma of non-germinal center B-cell type of the heart in an immunocompetent woman: an autopsy case. Med Oncol 2011; 28: 201-210.
[18] Martelli M, Ferreri AJ, Agostinelli C, Di Rocco A, Pfreundschuh M, Pileri SA. Diffuse large B-cell lymphoma. Crit Rev Oncol Hematol 2013; 87: 146-171.
[19] Martelli M, Ferreri AJ, Johnson P. Primary medi-astinal large B-cell lymphoma. Critical Reviews in Oncology/Hematology 2008; 68: 256-263. [20] Gaulard P, Harris NL, Pileri S, Kutok JL, Stein H,
Kovrigina AM. Primary mediastinal, (thymic) large B-cell lymphoma. Arch Pathol Lab Med 2011; 135: 194-198.
[21] Rosenwald A, Wright G, Chan WC, Connors JM, Campo E, Fisher RI, Gascoyne RD, Muller-Her-melink HK, Smeland EB, Giltnane JM, Hurt EM, Zhao H, Averett L, Yang L, Wilson WH, Jaffe ES, Simon R, Klausner RD, Powell J, Duffey PL, Longo DL, Greiner TC, Weisenburger DD, Sanger WG, Dave BJ, Lynch JC, Vose J, Armit-age JO, Montserrat E, López-Guillermo A, Gro-gan TM, Miller TP, LeBlanc M, Ott G, Kvaloy S, Delabie J, Holte H, Krajci P, Stokke T, Staudt LM; Lymphoma/Leukemia Molecular Profiling Project. The use of molecular profiling to pre -dict survival after chemotherapy for diffuse large-B cell lymphoma. N Engl J Med 2002; 346: 1937-1947.
[22] Wright G, Tan B, Rosenwald A, Hurt EH, Wiest-ner A, Staudt LM. A gene expression based method to diagnose clinically distinct sub-groups of diffuse large B cell lymphoma. Proc Natl Acad Sci U S A 2003; 100: 9991-9996. [23] Alizadeh AA, Eisen MB, Davis RE, Ma C, Lossos
IS, Rosenwald A, Boldrick JC, Sabet H, Tran T, Yu X, Powell JI, Yang L, Marti GE, Moore T, Hud-son J Jr, Lu L, Lewis DB, Tibshirani R, Sherlock G, Chan WC, Greiner TC, Weisenburger DD, Ar-mitage JO, Warnke R, Levy R, Wilson W, Grever MR, Byrd JC, Botstein D, Brown PO, Staudt LM. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature 2000; 403: 503-511.
Project. The use of molecular profiling to pre -dict survival after chemotherapy for diffuse large-B-cell lymphoma. N Engl J Med 2002; 346: 1937-1947.
[25] Song Y, Cao Z, Li L, Zhang HT, Zhang X. Blimp-1 protein and Hans classification on prognosis of diffuse large B-cell lymphoma and their inter-relation. Chin J Cancer 2010; 29: 781-786. [26] Wilson WH, Hernandez-Ilizaliturri FJ, Dunleavy
K, Little RF, O’Connor OA. Novel disease tar-gets and management approaches for diffuse large B cell lymphoma. Leuk Lymphoma 2010; 51: 1-10.
[27] Visco C, Li Y, Xu-Monette ZY, Miranda RN, Green TM, Li Y, Tzankov A, Wen W, Liu WM, Kahl BS, d’Amore ES, Montes-Moreno S, Dyb-kær K, Chiu A, Tam W, Orazi A, Zu Y, Bhagat G, Winter JN, Wang HY, O’Neill S, Dunphy CH, Hsi ED, Zhao XF, Go RS, Choi WW, Zhou F, Czader M, Tong J, Zhao X, van Krieken JH, Huang Q, Ai W, Etzell J, Ponzoni M, Ferreri AJ, Piris MA, Møller MB, Bueso-Ramos CE, Medeiros LJ, Wu L, Young KH. Comprehensive gene expression profiling and immunohistochemical studies support application of immunophenotypic al-gorithm for molecular subtype classification in diffuse large B-cell lymphoma: a report from the International DLBCL Rituximab-CHOP Con-sortium Program Study. Leukemia 2012; 26: 2103-2113.