P
IOTRW
ÓJCICKI1, 2, M
ARIUSZW
YSOCKI2Postmastectomy Breast Reconstruction
with Autologous Tissue – Pedicled Flaps. Part I
Rekonstrukcje piersi po mastektomii tkankami własnymi
– płaty uszypułowane. Część I
1Department of Plastic Surgery, Wroclaw Medical University, Poland
2Department of Plastic Surgery, Specialist Medical Center, Polanica Zdroj, Poland
Adv Clin Exp Med 2009, 18, 6, 649–655 ISSN 1230–025X
REVIEWS
© Copyright by Wroclaw Medical University
Abstract
Breast cancer is the most common tumor afflicting women. Breast loss is a dramatic experience triggering profound trauma. Contemporary operating techniques provide women with the opportunity for effective rehabilitation and a return to regular functioning in society. This paper presents the current state of the art concerning breast recon− struction with autologous tissue with application of the pedicled transverse rectus abdominis myocutaneous (TRAM) flap and the latissimus dorsi myocutaneous island flap (Adv Clin Exp Med 2009, 18, 6, 649–655).
Key words:breast reconstruction, pedicled flaps, breast cancer.
Streszczenie
Rak sutka jest najczęstszym nowotworem u kobiet. Utrata piersi jest tragicznym wydarzeniem wywołującym głęboki uraz psychiczny. Współczesne techniki operacyjne rekonstrukcji piersi stwarzają kobietom szansę na skuteczną rehabilitację i powrót do normalnego funkcjonowania psychospołecznego. W pracy przedstawiono aktu− alny stan wiedzy dotyczący rekonstrukcji piersi tkankami własnymi z zastosowaniem uszypułowanego płata skórno−mięśniowego z mięśnia prostego brzucha (TRAM) oraz płata skórno−mięśniowego z mięśnia najszerszego grzbietu (LD) (Adv Clin Exp Med 2009, 18, 6, 649–655).
Słowa kluczowe:rekonstrukcje piersi, płaty uszypułowane, rak piersi.
Growing breasts in young girls are a sign of puberty, and subsequently the most significant fea− ture distinguishing a woman’s silhouette. Their shape and size are associated with gracefulness, attractiveness, and sex appeal. Breast cancer is the most common tumor from which women suffer. Breast loss is a dramatic experience bearing trau− matic consequences. The breast is a symbol of femininity, beauty, and motherhood, hence mas− tectomy can result in psychological and aesthetic disturbances. The indications for reconstructive surgery are both aesthetic and psychological in nature, and its favorable impact on psychosocial functioning is unquestionable [1, 2]. Breast recon− struction aims not only at minimizing disfigure− ment, but foremost improving self−esteem.
Immediate or Delayed
Reconstruction?
In many hospitals, immediate postmastectomy reconstruction has become a standard procedure in the treatment of patients with breast cancer. Such a course of action allows achieving defined bene− fits. According to some authors it enables obtain− ing a better aesthetic result, avoiding a secondary reconstructive procedure on scar tissues and thus diminishing the risk of early complications, but primarily it promises doubtless psychological ben− efits [3].
The essential problem with regard to immedi− ate reconstruction is the effect of complementary radiotherapy on tissues of the reconstructed breast. Radiation has an unfavorable influence on recon− struction results when using alloplastic implants, and the frequency of occurrence of third− and fourth−degree pericapsular contracture may rise to 100% [4]. The high rate of complications and poor aesthetic result requires a secondary procedure applying tissue flaps in 47.5% of women [4, 5]. What is more, the application of autologous tis− sues most often results in delayed complications following radiotherapy compared with patients not subjected to radiation [3, 6, 7]. The consequences of irradiation are adipose tissue necrosis, callosity, hyperpigmentation, and shrinkage of both the flap and skin, which in 78% of patients leads to breast asymmetry [6]. Therefore in patients who, due to the stage of illness, are to receive complementary radiotherapy, postponement of reconstruction ought to be taken into consideration [3, 6, 7].
Pedicled Flaps
Anatomical research conducted in the 1970s resulted in the description of numerous muscle and fasciocutaneous flaps, of which the latissimus dorsi flap and the TRAM flap were determined to be the best for breast reconstruction. These flaps constituted the fundamental methods of breast reconstruction until the development of microsurgical techniques.
Latissimus Dorsi Myocutaneous
Island Flap
The latissimus dorsi (LD flap) is a type V flap according to the Mathes and Nahai classification. Proximal attachments through the posterior lamina of the lumbodorsal fascia begin on the spinous processes of the six inferior thoracic vertebra, the basilar vertebra, the sacral crest, and the posterior
part of the iliac bone crest. Distal attachment is found on the crest of the smaller tubercle of the humerus. The dominant vascular pedicle consists of thoracodorsal vessels, the final branch of the subscapular vessels, entering the muscle approxi− mately 10 cm beneath the axillary apex. The first mention of applying an LD flap in breast recon− struction dates back to 1906 [8]. It was forgotten for seventy years, but in 1976 it was promoted by Olivari [8] and applied in breast reconstruction by Mühlbauer and Olbrich [10] as well as Schneider [11]. It established its reputation due to its excel− lent blood supply and easy dissection (Fig. 1). One can distinguish two types of latissimus dorsi flaps in breast reconstruction: the standard LD flap and the so−called extended latissimus dorsi flap (ELD), containing an additional amount of fat tissue. In exceptional cases a standard flap suffices on its own for breast reconstruction.
In reconstructing small breasts, an adequate volume is obtained by harvesting the whole mus− cle, holding it, and suturing into two or three lay− ers beneath the skin island. In principle, however, due to insufficient tissue material, this flap serves as a supplement to the skin envelope of the recon− structed breast and creates a space for implant placement. The shape, size, and location of the skin island on the back is individually planned depending on the postmastectomy scar and the volume of skin loss. It is important to create a sub− mammary fold after flap transfer approximately 1–2.5 cm lower in relation to the contralateral sub− mammary fold due to the tendency of upward dis− location of the flap with a prosthesis [12–14]. This prevents a subsequent too high, asymmetric posi− tioning of the reconstructed breast.
Much attention was also devoted to the course of action with thoracodorsal nerve and brachial muscle attachment. Although some authors report the occurrence of fasciculation, the preservation of muscle innervation prevents its secondary atrophy and a loss of flap volume [15–17]. Opinions on dealing with brachial muscle attachment are divid− ed. It is believed that leaving the attachment pre− vents excessive tension in the pedicle and possible vascular complications; nevertheless, it simultane− ously results in a feeling of discomfort in 61.3% of patients in the axillary area, defined as “carrying a book”. Cutting the brachial muscle attachment reduces the occurrence of this phenomenon in 10.3% of patients [18].
mulation of transudate fluid in 9–10% of cases which requires long−term drainage, especially in obese patients [14, 19, 20]. Total flap necrosis appears very rarely due to the good blood supply and may be a consequence of pedicle rotation or tension. A complication connected with the pros− thesis is capsular contracture, which contributes to a change in breast consistency, progressive asym− metry, and, in extreme cases, pain discomfort. The incidence of second−degree contracture according to the Becker classification (prosthesis palpable, but soft) varies within the limits 24–57%, whereas third− and fourth−degree (prosthesis visible, hard, deformed) is between 2.3–30% [13, 14, 19]. Changes occurring around the prosthesis area most often cause approximately 31% of patients [20] to undergo capsulotomy already in the phase of nipple reconstruction [19, 20].
Breast reconstruction with an LD flap without implant enables modifications which augment its volume. The first flap containing an additional
amount of adipose tissue from the lumbar area was suggested by Hokin in 1983 [21]. To increase ELD flap volume one uses fat tissue harvested with the skin island, the adipose layer covering the whole muscle surface, and the scapular area above the superior−medial edge of the latissimus dorsi, tissue located forward from the latissimus dorsi, as well as tissue above the iliac crest, defined as “love han− dles” [22]. This permits breast reconstruction with− out the necessity of using implants [23]. The amount of fat tissue from the back is evaluated with a simple test: grabbing the skin into a fold, the so− called “pinch test”. Tissue thickness exceeding 2–2.5 cm is generally sufficient for breast recon− struction without a prosthesis [24]. To achieve good breast projection and simultaneously create an aesthetic scar at the donor site, the skin island is shaped in a crescent opening upwards which, after flap transfer, is formed into the shape of an asym− metric “U”. During flap preparation it is significant to leave the subcutaneous vascular plexus by pre−
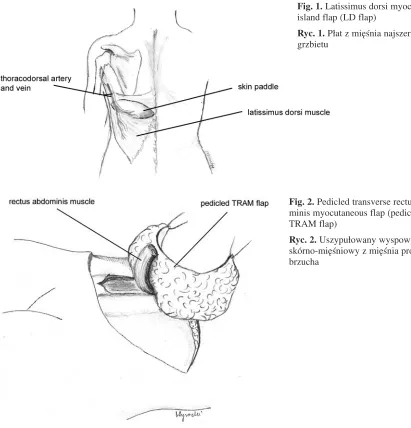
Fig. 1. Latissimus dorsi myocutaneous island flap (LD flap)
Ryc. 1. Płat z mięśnia najszerszego grzbietu
Fig. 2.Pedicled transverse rectus abdo− minis myocutaneous flap (pedicled TRAM flap)
serving an about one−centimeter layer of adipose tissue [22, 24]. The volume of the reconstructed breast ought to exceed the size of a healthy breast by approximately 15–30%, which ensures symme− try after the phase of spontaneous flap shrinkage (approximately 5–6 months) [22, 25].
The most common complication following reconstruction with an ELD flap, which appears on average in 60–76% of patients, including obese women, is accumulation of transudate fluid [17, 22, 25], which requires long drainage and evacua− tion of formed seromas. Reconstruction with the aid of an ELD flap is a reliable method which excellently reproduces the anterior axial fold and subclavicular part of the breast [24]. This method facilitates the reconstruction of a breast with an approximate volume 300–400 ml in patients with normal body weight, 600–800 ml in women with overweight, and even 1200–1500 ml in obese patients [22].
Transverse Rectus Abdominis
Myocutaneous flap
Single Pedicled TRAM Flap
A pedicled TRAM flap consists of a horizon− tal cutaneous island and the rectus abdominis mus− cle which, with the superior epigastric vessels entering the muscle, constitute the pedicle of the flap. The fusiform island containing skin, subcuta− neous tissue, subcutaneous and superficial fascia, as well as a marginal fragment of the anterior rec− tus abdominis muscle sheath is located horizontal− ly on the long axis on the abdomen. Its superior limit is the umbilicus, inferior the pubic mound, and lateral the anterior−superior iliac spine. A myocutaneous pedicled flap based on the rectus abdominis muscle was introduced by Robbins in 1979 [26]. It was modified as the TRAM flap, sug− gested and propagated by Hartrampf et al. in 1982 [27] (Fig. 2).
The blood supply of the abdominal walls comes from the superior and inferior epigastric vessels, inferior superficial epigastric vessels, superficial iliac circumflex vessels, intercostal vessels from VIII to XII, and the superficial pudendal vessels [28]. The abdominal area is pro− vided by the first four mentioned vessels. The ves− sels of the pedicled TRAM flap constitute the superior epigarstic vessels, whereas the vessels of the free flap constitute the inferior epigastric ves− sels. The dominant artery providing the TRAM flap is the inferior epigastric artery from the exter− nal iliac artery. Running along the posterior sur− face of the rectus abdominis muscle, it enters it at various levels and, after making two or three per−
forators in the paraumbilical area, it joins at half length between the umbilicus and xiphoid process through the “choke vessels” [29] with the superior epigastric artery [30]. Moon and Taylor [31] proved the existence of three types of junctions between the superior and inferior epigastric arter− ies. In the first type (29%) the junction appears between single vessels, in the second (57%) the inferior epigastric artery divides into two branches at the level of the arcuate line before joining, and in the third (14%) into three branches. This system facilitates reconstruction with a pedicled flap on the superior epigastric artery. Arranged in two rows, medial and lateral, musculocutaneous and fasciocutaneous perforators combine the epigastric vessels with the flap’s subcutaneous plexus. Their greater number appears in the paraumbilical area and they play a decisive role in blood supply [31].
In the topography of the abdominal flap, four vascular territories (angiosomes, I−IV), that divide the skin island horizontally to the long axis are dis− tinguished. Zones I and II refer to the central flap part, although zone I is located on the side of the vascular pedicle. Zones III and IV concern the external flap parts and, analogous to zone III, refers to the same side as the vascular pedicle.
In the originally suggested technique, the pedicle was located on the side of the reconstruct− ed breast [27]; however, due to the fear of exces− sive pedicle folding and blood perfusion deteriora− tion, an oppositely pedicled flap was applied. However, it was indicated that in these flaps a sig− nificantly greater venous pressure and lower per− fusion pressure occur than in ipsilateral flaps, which is interpreted as excessive pedicle tension obstructing blood flow [32–34]. On the strength of numerous studies, the opinion predominates that less ipsilateral pedicle tension enables easier mod− eling of the reconstructed breast and, moreover, the transfer of a thicker paraumbilical flap part to the inferior part of the reconstructed breast ensures a better aesthetic result. The application of con− tralateral pedicled flaps causes removal of the medial part of the submammary fold, a bulge in the area of the xiphoid process, and a too acute breast protrusion from the chest [32–34].
patients with an aggravating medical history to approximately 6.6–7.5% [40, 42–44]. Alternative to ligation of the inferior epigastric vessels is ele− vating the skin island 7 to 10 days before flap transfer. This procedure decreases the risk of par− tial flap necrosis to 3.6% [45].
Double Pedicle TRAM Flaps
To improve blood perfusion of the skin island, especially in zone IV, flaps containing two superi− or epigastric arteries and so−called “supercharged” [46] and “turbocharged” [47] TRAM flaps are used. Suggested in 1985 [48], the flap based on two pedicles containing both rectus abdominis muscles was not highly recognized due to substan− tial deformation of the abdominal wall and diffi− culties with unrestrained dislocation of the flap and with formation of the reconstructed breast [49]. In the “supercharged” TRAM flap, the sec− ond pedicle constitutes superficial or deep arteries and inferior epigastric veins [50, 51] that are anas− tomosed with recipient vessels. The preferred recipient vessels are those of the axillary fossa, particularly thoracodorsal vessels and internal mammary vessels and those of the circumflex scapula. The success of this specific operating technique is mainly dependent on the availability and quality of the recipient vessels.
The “turbocharged” flap does not demand recipient vessels and improvement in blood flow is achieved by the formation of a loop out of inferior epigastric vessels. Inferior epigastric vessels pre− pared on both sides are anastomosed with one another. Thanks to the loop opposite the major
vascular pedicle, the flap area receives extra per− fusion. Reverse pulsating blood outflow from the inferior epigastric artery with a minimal diastolic pressure of 50 mm Hg provides appropriate blood flow through the formed loop [47].
The principal objective of reconstructive pro− cedures in postmastectomy patients is the recon− struction of a natural−looking symmetric breast with a nipple−areola complex. The treatment of ”Amazons” is a compound issue of surgical, onco− logical, and psychological nature. It is extremely essential to inform the patient about every aspect of treatment in an objective manner. Such an approach guarantees avoidance of disappointment and unrealistic expectations. Cooperation of the oncology surgeon and plastic surgeon permits an immediate mastectomy and reconstructive opera− tion. Even if a two−staged treatment is scheduled, the cooperation allows for more economical skin removal, smaller scars, and less burdensome and arduous treatment for the patient. The implemen− tation of pedicled flaps substantially improved breast reconstructive possibilities and contributed to the achievement of good treatment results in comparison with those obtained by applications of tubular flaps, free skin grafts, or local flaps. The latissimus dorsi flap is generally applied to form a suitable tissue cover to implant a breast prosthe− sis. Very seldom, selected cases allow for breast reconstruction without the use of implants. The pedicled TRAM flap has been the method of choice for many years in breast reconstruction. The progress in microsurgical techniques and the development of fasciocutaneous and myocuta− neous flaps provoked the more frequent use of free tissue flaps in breast reconstructive operations.
References
[1] Keith DJ, Walker MB, Walker LG, Heys SD, Sarkar TK, Hutcheon AW, Eremin O:Women who wish breast reconstruction: characteristics, fears, and hopes. Plast Reconstr Surg 2003, 111, 1051–1056.
[2] Brandberg Y, Malm M, Blomqvist L:A prospective and randomized study, “SVEA”, comparing effect of three methods for delayed breast reconstruction on quality of life, patient−defined problem areas of life, and cosmetic results. Plast Reconstr Surg 2000, 105, 66–74.
[3] Tran NV, Chang DW, Gupta A, Kroll SS, Robb GL:Comparison of immediate and delayed free TRAM flap breast reconstruction in patients receiving postmastectomy radiation therapy. Plast Reconstr Surg 2001, 108, 78–82.
[4] Vanderweyer E, Deraemaecker R:Radiation therapy after immediate breast reconstruction with implants. Plast Reconstr Surg 2000, 106, 56–58.
[5] Spear SL, Onyewu C: Staged breast reconstruction with saline−filled implants in the irradiated breast: recent trends and therapeutic implications. Plast Reconstr Surg 2000, 105, 930–942.
[6] Tran NV, Evans GRD, Kroll SS, Baldwin BJ, Miller MJ, Reece GP, Robb GL: Postoperative adjuvant irradi− ation: effect on transverse rectus abdominis muscle flap breast reconstruction. Plast Reconstr Surg 2000, 106, 313–317.
[7] Rogers NE, Allen RJ:Radiation effect on breast reconstruction with the deep inferior epigastric perforator flap. Plast Reconstr Surg 2002, 109, 1919–1924.
[8] Maxwell GP:Iginio Tansini and the origin of the latissimus dorsi musculocutaneous flap. Plast Reconstr Surg 1980, 65, 686–692.
[10] Mühlbauer W, Olbrisch R: The latissimus dorsi myocutaneous flap for breast reconstruction. Chirurgica Plastica 1977, 4, 27.
[11] Schneider WJ, Hill HL, Brown RG: Latissimus dorsi myocutaneous flap for breast reconstruction. Br J Plast Surg 1977, 30, 277–281.
[12] Wolf LE, Biggs TM:Aesthetic refinements in the use of the latissimus dorsi flap in breast reconstruction. Plast Reconstr Surg 1982, 69, 788–793.
[13] Tschopp H: Evaluation of long−term results in breast reconstruction using the latissimus dorsi flap. Ann Plast Surg 1991, 26, 328–340.
[14] Smith BK, Cohen BE, Biggs TM, Suber J:Simultaneous bilateral breast reconstruction using latissimus dorsi myocutaneous flaps: a retrospective review of an institutional experience. Plast Reconstr Surg 2001, 108, 1174–1181.
[15] Towpik E: Rekonstrukcja sutka po mastektomii wyspowym płatem z mięśnia najszerszego grzbietu bez endo− protezy. Pol Tyg Lek 1988, 18, 1058–1063.
[16] Towpik E, Różycki−Gerlach W: Breast reconstruction using latissimus dorsi island flap without an endoprosthe− sis. Eur J Surg Oncol 1992, 18, 53–55.
[17] Clough KB, Louis−Sylvestre C, Fitoussi A, Couturaud B, Nos C: Donor site sequelae after autologous breast reconstruction with an extended latissimus dorsi flap. Plast Reconstr Surg 2002, 109, 1904–1910.
[18] Gerber B, Krause A, Reimer T, Müller H, Friese K: Breast reconstruction with latissimus dorsi flap: improved aesthetic results after transection of its humeral insertion. Plast Reconstr Surg 1999, 103, 1876–1881.
[19] De Mey A, Lejour M, Declety A, Meythiaz AM: Late results and current indications of latissimus dorsi breast reconstructions. Br J Plast Surg 1991, 44, 1–4.
[20] Moore T, Farrell L: Latissimus dorsi myocutaneous flap for breast reconstruction: long−term results. Plast Reconstr Surg 1992, 89, 666–671.
[21] Hokin JAB:Mastectomy reconstruction without a prosthetic implant. Plast Reconstr Surg 1983, 72, 810–818.
[22] Delay E, Gounot N, Bouillot A, Zlatoff P, Rivoire M:Autologous latissimus breast reconstruction: a 3−year clin− ical experience with 100 patients. Plast Reconstr Surg 1998, 102, 1461–1478.
[23] Chang DW, Youssef A, Cha S, Reece GP: Autologous breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg 2002, 110, 751–759.
[24] Mc Craw JB, Papp C, Edwards A, Mc Mellin A:The autogenous latissimus breast reconstruction. Clin Plast Surg 1994, 21, 279–288.
[25] Menke H, Erkens M, Olbrisch RR: Evolving concepts in breast reconstruction with latissimus dorsi flaps: results and follow−up of 121 consecutive patients. Ann Plast Surg 2001, 47, 107–114.
[26] Robbins TH: Rectus abdominis myocutaneous flap for breast reconstruction. Aust N Z J Surg 1979, 49, 527–530.
[27] Hartrampf CR, Shceflan M, Black PW: Breast reconstruction with a transverse abdominal island flap. Plast Reconstr Surg 1982, 69, 216–224.
[28] Hartrampf CR Jr, Anton MA, Breid JT: Breast reconstruction with the transverse abdominal island (TRAM) flap. In: Georgiade Plastic, Maxillofacial and Reconstructive Surgery. Eds.: Georgiadae GS, Riefkohl R, Levin LS. Williams & Wilkins, Baltimore, Philadelphia, London, Paris, Bangkok, Hong Kong, Munich, Sydney, Tokyo, Wrocław 1997, 3rded., 786–797.
[29] Taylor GI, Palmer JH:The vascular territories (angiosomes) of the body. Experimental study and clinical appli− cations. Br J Plast Surg 1987, 40, 113–141.
[30] Cormac GC, Lamberty BGH: The Arterial Anatomy of Skin Flaps. Churchill Livingstone, Edinburgh, London 1986, 266–271.
[31] Moon HK, Taylor GI: The vascular anatomy of rectus abdominis musculocutaneous flaps based on deep superi− or epigastric system. Plast Reconstr Surg 1988, 82, 815–829.
[32] Clugston PA, Lennox PA, Thompson RP: Intraoperative vascular monitoring of ipsilateral vs. contralateral TRAM flaps. Ann Plast Surg 1998, 41, 623–628.
[33] Clugston PA, Gingrass MK, Azurin D, Fisher J, Maxwell GP: Ipsilateral Pedicled TRAM flaps: The safer alternative? Plast Reconstr Surg 2000, 105, 77–82.
[34] Olding M, Emory RE, Barrett WL: Preferential use of the ipsilateral pedicle in TRAM flap breast reconstruc− tion. Ann Plast Surg 1998, 40, 349–353.
[35] Padubidri AN, Yetman R, Browne E, Lucas A, Papay F, Larive B, Zins J: Complications of postmastectomy breast reconstruction in smokers, ex−smokers, and non−smokers. Plast Reconstr Surg 2001, 107, 342–349.
[36] Schusterman MA, Kroll SS, Weldon ME: Immediate breast reconstruction: why the free TRAM over the con− ventional TRAM flap? Plast Reconstr Surg 1992, 90, 255–261.
[37] Kroll SS:Bilateral breast reconstruction in very thin patients with extended free TRAM flaps. Br J Plast Surg 1998, 51, 535–537.
[38] Baldwin BJ, Schusterman MA, Miller MJ, Kroll SS, Wang BG:Bilateral breast reconstruction: conventional versus free TRAM. Plast Reconstr Surg 1994, 93, 1410–1416.
[39] Moran SL, Serletti JM:Outcome comparison between free and pedicled TRAM flap breast reconstruction in obese patient. Plast Reconstr Surg 2001, 108, 1954–1960.
[41] Scheufler O, Andersin R, Kirch A, Banzer D, Vaubel E: Clinical results of TRAM flap delay by selective embolization of the deep inferior epigastric arteries. Plast Reconstr Surg 2000, 105, 1320–1329.
[42] Hudson DA: The surgically delayed unipedicled TRAM flap for breast reconstruction. Ann Plast Surg 1996, 36, 238–242.
[43] Jensen JA, Handel N, Silverstein MJ, Waisman J, Gierson ED:Extended skin island delay of the unipedicle TRAM flap: experience in 35 patients. Plast Reconstr Surg 1995, 96, 1341–1345.
[44] Ribuffo D, Muratori L, Antoniadou K, Fanini F, Martelli E, Martini M, Messineo D, Trinci M, Scuderi N:
A hemodynamic approach to clinical results in the TRAM flap after selective delay. Plast Reconstr Surg 1997, 99, 1706–1714.
[45] Towpik E, Mazur S, Witwicki T, Tchorzewska H, Jackiewicz P:Elevating the Island: The Simplest Method of Delaying the TRAM Flap. Ann Plast Surg 2000, 45, 240–243.
[46] Harashina T, Sone K, Inoue T, Fukuzumi S, Enomoto K:Augmentation of circulation of pedicled transverse rectus abdominis musculocutaneous flaps by microvascular surgery. Br J Plast Surg 1987, 40, 367–370.
[47] Semple JL: Retrograde microvascular augmentation (turbocharging) of a single−pedicle TRAM flap through a deep inferior epigastric arterial and venous loop. Plast Reconstr Surg 1994, 93, 109–117.
[48] Ishii CH Jr, Bostwick J 3rd, Raine TJ, Coleman JJ 3rd, Hester TR:Double−pedicle transverse rectus abdo− minis myocutaneous flap for unilateral breast and chest wall reconstruction. Plast Reconstr Surg 1985, 76, 901–907.
[49] Wagner DS, Michelow BJ, Hartrampf CR Jr:Double−pedicle TRAM flap for unilateral breast reconstruction. Plast Reconstr Surg 1991, 88, 987–997.
[50] Towpik E, Witwicki T, Mazur S, Kułakowski A: Natychmiastowa rekonstrukcja piersi uszypułowanym płatem TRAM z mikrozespoleniem naczyń nabrzusznych dolnych i piersiowo−grzbietowych. Nowotwory 1998, 48, 57–62.
[51] Witwicki T, Towpik E, Mazur S, Tchórzewska H, Jackiewicz P, Nagadowska M, Chmielewski R: Ocena wczesnych wyników rekonstrukcji piersi uszypułowanym wyspowym płatem z mięśnia prostego brzucha z dodatkowym mikrozespoleniem naczyń nabrzusznych dolnych. Pol Przeg Chir 2000, 72, 799–805.
Address for correspondence:
Piotr WójcickiJana Pawła II 2 57−320 Polanica Zdrój Poland
Tel.: +48 74 862 11 59
E−mail: [email protected]
Conflict of interest: None declared