Biologic Behavior and Clinical Outcome of 25 Dogs with Canine
Appendicular Chondrosarcoma Treated by Amputation: A
Veterinary Society of Surgical Oncology Retrospective Study
JAMES P. FARESE,DVM, Diplomate ACVS, JOLLE KIRPENSTEIJN,DVM, PhD, Diplomate ACVS, & ECVS, MARJA KIK,DVM, PhD, Diplomate Vet Path, NICHOLAS J. BACON,Vet MB, Diplomate ACVS, Diplomate ECVS, SUZANNE SHELLY WALTMAN,DVM, Diplomate ACVIM (Oncology), BERNARD SEGUIN,DVM Diplomate ACVS, MICHAEL KENT,DVM, Diplomate ACVIM (Oncology) & ACVR (Radiation Oncology), JULIUS LIPTAK,BVSc, MVetClinStud, FACVSc Diplomate
ACVS & ECVS, ROD STRAW, BVSc, Diplomate ACVS, M(A)ACVSc, MYRON N. CHANG,PhD, YANG JIANG, and STEPHEN J. WITHROW,DVM, Diplomate ACVS & ACVIM (Oncology)
Objective—To characterize biologic behavior, clinical outcome, and effect of histologic grade on prognosis for dogs with appendicular chondrosarcoma treated by amputation alone.
Study Design—Case series.
Animals—Dogs (n¼25) with appendicular chondrosarcoma.
Methods—Medical records were searched to identify dogs with appendicular chondrosarcoma treated by limb amputation alone. Information recorded included signalment, anatomic location, radiographic appearance, and development of metastasis. Histopathologic diagnosis was confirmed and graded (1, 2, or 3). Survival curves were generated by the Kaplan–Meier method and the association between covariates (gender, age, weight, and tumor grade) and survival were evaluated using the univariate proportional hazards model.
Results—Histopathology slides were available for 25 dogs. Rates of pulmonary metastasis were as follows: grade 1–0%, grade 2–31%, and grade 3–50%. Overall median survival time (MST) was 979 days. Age, weight, and sex were not significantly associated with survival (P¼.16; .33; and .31, respectively). Survival was significantly associated with tumor grade (P¼.008), with dogs with tumor grade of 1, 2, and 3 having MSTs of 6, 2.7, and 0.9 years, respectively.
Conclusion—Canine appendicular chondrosarcoma can be treated effectively with amputation alone. Low to intermediate grade chondrosarcoma has a good prognosis, whereas high-grade tumors appear to behave aggressively.
Clinical Relevance—The overall prognosis for appendicular chondrosarcoma is better than that of appendicular osteosarcoma treated by amputation alone or in combination with chemotherapy.
rCopyright 2009 by The American College of Veterinary Surgeons
Work was performed at the University of Florida, College of Veterinary Medicine and Utrecht University, Utrecht, the Netherlands. Presented in part at the annual meeting of the Veterinary Cancer Society, Seattle, WA, October 18–20, 2008.
Corresponding author: James P. Farese, DVM, Diplomate ACVS, Department of Small Animal Clinical Sciences, College of Veterinary Medicine, University of Florida, Gainesville, 2015 SW 16th Ave. FL 32610-0126. E-mail: [email protected]fl.edu.
Submitted December 2008; Accepted May 2009
From the College of Veterinary Medicine, University of Florida, Gainesville, FL; the Faculty of Veterinary Medicine, Utrecht University, The Netherlands; the Southwest Veterinary Oncology, Glendale, AZ; the Oregon Cancer Center for Animals, College of Veterinary Medicine, Oregon State University, Corvallis, OR; the School of Veterinary Medicine, University of California–Davis, Davis, CA; the Alta Vista Animal Hospital, Ottawa, Canada; the Australian Animal Cancer Foundation, Brisbane Veterinary Specialist Centre, Brisbane, Australia; the Division of Biostatistics, College of Medicine, University of Florida, Gainesville, FL; and the Animal Cancer Center, Colorado State University, Fort Collins, CO.
rCopyright 2009 by The American College of Veterinary Surgeons
0161-3499/09
doi:10.1111/j.1532-950X.2009.00606.x
INTRODUCTION
C
HONDROSARCOMA IS the second most com-mon primary bone tumor in both dogs and humans, and accounts for 5–10% of reported cases.1–6Reported anatomic locations for chondrosarcoma in dogs include the nasal cavity, axial skeleton (e.g., rib, facial bones), appendicular skeleton and extraskeletal sites such as the mammary gland.4,6–8Chondrosarcoma is generally con-sidered moderately metastatic,1 with rates ranging from 18% to 60% and reported sites including the lungs, pleura, mediastinum, pericardium, lymph nodes, bone, liver, kidney, adrenal gland, and eyes.1,4,6,7,9 In 1 study tumor location rather than histologic grade was consid-ered prognostic, with tumors of the facial bones, nasal turbinates and extremities having prolonged survival when compared with those located in the rib.8In a more recent study, histologic grade was prognostic for sur-vival.7 Chemotherapy has not been shown to prolong survival in either dogs or humans and is typically not recommended after surgical excision in either species.7,10 Several reports of skeletal chondrosarcomas have in-cluded a number of appendicular cases.6–9The reported survival times for dogs treated with surgery alone (typ-ically amputation) varied widely: Obradovich et al9 re-ported a median survival time (MST) 163 days (n¼7), Popovitch et al6reported a MST 540 days (n¼5), and Waltman et al7 reported a mean survival time of 2618 days (n¼13, 10 of which were treated by amputation and 3 were untreated). Such discrepancies make it difficult to predict survival accurately. Our purpose with a retro-spective, multi-institutional study was to identify a greater number of dogs with appendicular chondrosar-coma treated with limb amputation alone to characterize biologic behavior, assess clinical outcome and determine effect of histologic grade on prognosis.MATERIALS AND METHODS Inclusion Criteria
Medical records (1995–2005) of all contributing institutions were searched to identify dogs with chondrosarcoma of the appendicular skeleton that were treated by limb amputation alone. Dogs that had adjunctive therapy (e.g., chemotherapy or radiation therapy) or did not have 6 weeks of follow-up information were excluded. Only dogs with a confirmed histo-logic diagnosis of chondrosarcoma on tissue sections collected from the amputated limb were included.
Data Retrieved
Information recorded included: age, weight, sex, breed, bone affected, location within the bone (i.e., proximal, middle, or distal), preoperative serum alkaline phosphates levels,
ra-diographic appearance (i.e., proliferative, lytic, or mixed), de-tails about preoperative biopsy, level of amputation, development of metastasis (anatomic location and number of days detected postamputation) and overall survival.
Histopathology
Hematoxylin and eosin (H&E)-stained slides were evalu-ated and graded by a single pathologist (M.K.), without having knowledge of the corresponding clinical history, radiologic in-terpretations, or gross pathologic findings. A grading scale was adapted from a previous human chondrosarcoma grading scale11,12and grade was determined by assessing the following features: matrix production, architecture, degree of pleiomorp-hism, cellularity, necrosis, and mitosis. Each descriptive feature was assigned a numerical value of 0, 1, 2, or 3, with 0 indicating not observed and 1, 2, and 3 indicating increasing presence. Mitosis was assessed by counting the number of mitotic fig-ures/10 high-power fields (HPF). Values for each category were then summed (including the number of mitotic figures/10 HPF) and each case was assigned a grade according to the following scale: Grade I—total histologic scoreo6 and mito-sis 0–1 or total histologic score 7 and mitomito-sis¼0; Grade II— total histologic score 7–10 and mitosis¼1 or 2; and Grade III—total histologic score 11–16 or mitosis¼3.
Data Analysis
Survival time was defined as the interval between amputa-tion and death. Cause of death was classified as chondrosar-coma or nonchondrosarchondrosar-coma related. Dogs with unknown causes of death were presumed to have died from chondro-sarcoma. For the purposes of survival calculations, dogs that died as a result of their chondrosarcoma were considered completed events and dogs that died of other causes other than chondrosarcoma, or were still alive at the time of last contact, were censored. Survival curves were generated by the Kaplan– Meier method. Association between covariates (gender, age, weight, and tumor grade) and survival were evaluated using both univariate and multivariate proportional hazards models. Rate of pulmonary metastasis was compared by Fisher’s exact test. All data were analyzed using statistical software (SAS version 9.1.3 software, SAS Institute, Cary, NC).
RESULTS
Twenty-seven dogs met the inclusion criteria; however, 2 cases previously diagnosed as chondrosarcoma were reclassified as chondroblastic osteosarcomas and were therefore excluded, resulting in a total of 25 cases. Eight cases were previously included in the study by Waltman et al7 Mean age was 6.58 years (range, 1.8–12 years). Mean weight was 30.5 kg (range, 7–52 kg). There were 14 females (2 intact, 12 spayed) and 11 males (2 intact, 9 neutered). Breeds included 4 mixed breed dogs, 2 Golden Retrievers, 4 Bernese mountain dogs, 2 Doberman Pinsc-hers, 2 Australian cattle dogs and 1 each of Rottweiler,
English Springer Spaniel, Labrador Retriever, Belgian Shepherd, Irish Wolfhound, Maltese, Lhasa Apso, Irish Setter, Greyhound, Cocker Spaniel, and Great Pyrenees. Serum alkaline phosphatase levels were available for 10 dogs and were normal in 8. Of the 2 outside the ref-erence range, 1 was below normal (3; institution refref-erence interval, 5–131 IU/L) and the other was elevated (142; institution reference interval, 17–86 IU/L). Ten tumors were located in the tibia (6 proximal, 4 distal), 5 in the femur (2 proximal, 3 distal), 4 in the humerus (3
prox-imal, 1 distal), 2 in the ulna (both distal), 1 in metacarpals II and III, 1 in the carpus, 1 in the proximal aspect of the radius, and 1 in the calcaneus. When radiographs were available for review, pathologic changes were observed osteolytic (7 dogs), osteoproliferative (2 dogs), or a mixed process (6 dogs; Figs 1 and 2).
Information regarding preoperative biopsy was avail-able for 12 of the confirmed chondrosarcomas; however, none of these samples were available for re-evaluation by our pathologist. In 8 of these cases, chondrosarcoma was Fig 1. Craniocaudal (A) and mediolateral (B) radiographic projections of a proximal tibial chondrosarcoma from a 9-year-old, male intact 35 kg Irish Setter.
Fig 2. Craniocaudal (A) and mediolateral (B) radiographic projections of a distal humeral chondrosarcoma from an 8.8-year-old, female spayed 7 kg Lhasa Apso. Note lytic changes extending from distal humeral metaphysis to the proximal olecranon.
initially diagnosed. In the other 4 cases a different diagno-sis was initially made (2 as chondroma, 1 focal chondro-dysplasia, and 1 bone marrow fibrosis). One of the tumors diagnosed as chondrosarcoma preoperatively was also subjectively graded by the initial pathologist. This case, which was given a low preoperative grade, was considered a grade 2 chondrosarcoma in our study. This dog was alive at the time of this report at 550 days.
The primary tumor was treated by amputation in all dogs. One dog was treated by partial pelvectomy (i.e., ace-tabulectomy) because of proximity of the tumor to the coxofemoral joint (originated in the greater trochanter of the femur). Eight dogs were still alive at the time of writing. Six dogs died of unknown causes and 5 died from unrelated conditions, including splenic hemangiosarcoma (1), pros-tatic adenocarcinoma suspected (1), renal failure (1), and 2 euthanatized for other geriatric problems. Pulmonary me-tastasis was diagnosed radiographically in 7/25 (28%) dogs and 2 of these had confirmation of pulmonary metastasis by necropsy (no other abnormalities were noted). Time to radiographic evidence of metastasis from the time of am-putation was reported in 4/7 dogs with pulmonary metas-tasis. For these 4 dogs, the number of days to detection of metastasis and survival time, respectively, were as follows: 191 and 252 days, 325 and 387 days (still alive at the time of this report with pulmonary hypertrophic osteopathy), 453 and 455 days, and 712 and 723 days. For the other 3 dogs, the radiographic diagnosis of pulmonary metastasis and euthanasia occurred on the same day. There was no ev-idence of local recurrence in any of the cases.
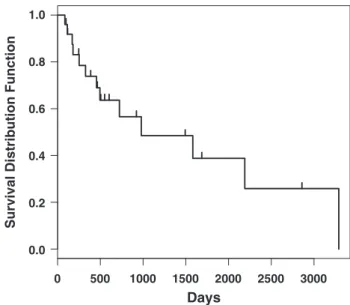
Histopathology slides created from the amputated spec-imens were available for 25 dogs: 6 (24%) were grade 1; 13 (52%) grade 2; and 6 (24%) grade 3 tumors. The rates of pulmonary metastasis were as follows: grade 1–0%, grade 2–31%, and grade 3–50%. The difference in rate of pul-monary metastasis between dogs with tumor grade 1, 2, or 3 was not statistically significant (P¼.18). Two of the 6 grade 3 tumors died of unknown causes at 85 and 171 days. Overall MST was 979 days (2.7 years, Fig 3). From univariate analysis, age, weight, and sex were not signifi-cantly associated with survival (P¼.16, .33, and 0.31, re-spectively). Survival was significantly associated with tumor grade (P¼.008), with dogs with tumor grade of 1, 2, and 3 having MSTs of 6, 2.7, and 0.9 years, respec-tively (Fig 4). By multivariate analysis with survival as the dependent variable and with age, weight, sex, and tumor grade as independent variables, only tumor grade was sig-nificantly associated with survival (P¼.039).
DISCUSSION
There has been great discrepancy in the published MSTs for dogs with appendicular chondrosarcoma treated by amputation. Some studies have linked the
clinical outcome to that of canine appendicular osteosar-coma (OSA; Obradovich et al,9n¼7, MST¼163 days), whereas others have reported moderately higher (Popov-itch et al,6n¼5, MST¼540 days) or substantially higher survival times (Waltman et al,7mean survival time¼2618 days). We speculate that, given the higher number of cases in our study, the overall MST of 2.7 years (979 days) may better estimate the survival of dogs with
ap-0 0.0
Days
Survival Distribution Function
500 1000 1500 2000 2500 3000 0.2 0.4 0.6 0.8 1.0
Fig 3. Kaplan–Meier survival analysis for 25 dogs with appendicular chondrosarcoma treated with amputation alone. Overall median survival time is 2.7 years (979 days).
0 0.0
Days
Survival Distribution Function
0.2 0.4 0.6 0.8 1.0 500 1000 1500 2000 2500 3000 tumorgrade1 (n = 6) tumorgrade2 (n = 13) tumorgrade3 (n = 6)
Fig 4. Kaplan–Meier survival analysis of grade 1, grade 2, and grade 3 chondrosarcomas treated by amputation alone. The tumor grade was significantly associated with survival (P¼.008). The higher the tumor grade, the shorter the survival. Dogs with tumor grade of 1, 2, and 3 had median survival times of 6, 2.7, and 0.9 years, respectively.
pendicular chondrosarcoma treated by amputation alone. In our study, the rate of metastasis was 28% (7/25 dogs) and the lungs were the only documented anatomic site. This rate is in agreement with the 31% rate reported for long bone tumors by Waltman et al7(n¼13; 10 treated and 3 untreated); however, it is substantially lower than reported rates for dogs treated by amputation by Pop-ovitch et al6(60%; n¼5) and Obradovich et al9(57%; n¼7). We also speculate that our findings, and those reported by Waltman et al,7may better represent the rate of metastasis for appendicular chondrosarcoma given the higher number of cases in the more recent studies.
In humans, grading of chondrosarcomas is one of the most important prognostic predictors.11,12Grade I human chondrosarcomas are not typically metastatic, whereas 10–33% of grade II and 70% of grade III chondro-sarcomas metastasize. Six of the dogs in our study were diagnosed as grade 1, 13 as grade 2, and 6 as grade 3. The association between grade and metastasis in our dogs (grade 1–0%, grade 2–31%, and grade 3–50%) is similar to the association reported for human chondrosarcoma.
Two tumors in this study had been provisionally diag-nosed as chondrosarcoma, but were re-classified as chond-roblastic osteosarcoma by our pathologist and therefore excluded. Such disagreement, between histopathologic di-agnosis obtained preoperatively by needle core biopsies and the postoperative diagnosis based on the larger tissue specimen submitted after amputation, is common in the clinical setting. Given the apparent difference in MST between appendicular chondrosarcoma and appendicular osteosarcoma treated by amputation alone (2.7 years and 18–19 weeks,1respectively), it is important for clinicians to be aware of this possibility and to educate clients ac-cordingly. It is also possible that previous studies could have mistaken some chondroblastic osteosarcomas for chondrosarcomas and this may in part have accounted for the some of the shorter survival times.6,9
A preoperative biopsy was performed in 12 of the 25 dogs; however, none of these slides were made available to our pathologist. In 8 of these cases, a diagnosis of chondro-sarcoma was made. Thus, 66% of the preoperative di-agnoses agreed with the postoperative diagnosis. Preoperative diagnoses that did not agree with the postop-erative diagnosis tended benign in nature (e.g., chondroma). Although it cannot be determined from our retrospective study, we speculate that the discrepancy may be attributed to the small size of most preoperative biopsies.
We found that the tibia was the most commonly affected bone (10/25 [40%] dogs; 6 proximal, 4 distal), followed by the femur (5/25 [20%]) and humerus (4/25 [16%]). Unlike osteosarcoma, the radius was infrequently affected and the 1 documented case in our series was in the proximal aspect. Popovitch et al,6 found the femur most commonly affected, equally distributed between the
proximal and distal metaphyses. In the reports by Sylvestre et al8and Waltman et al7the tibia and humerus were the most commonly affected bones. Collectively, these studies and our study indicate that the proximal tibia is the most commonly affected bone, specifically the proximal aspect. Thus, it appears that the skeletal distri-bution differs from that of appendicular osteosarcoma, where the distal radius is the most common site.1
In our study, radiographic changes were observed osteolytic (7 dogs), osteoproliferative (2 dogs), or a mixed process (6 dogs; Fig 1). These observations are consistent with those reported where chondrosarcoma has been de-scribed to produce predominantly osteolytic changes or a mixed process.8,13 In 1 dog (Fig 2), the tumor caused osteolysis that extended across a joint, affecting the distal humerus and olecranon. Sylvestre et al8also reported an appendicular chondrosarcoma that crossed a joint. In that dog the tumor was located primarily in the proximal humerus and extended along the shoulder joint capsule into the distal scapula.
Our study has several limitations because of its retro-spective nature. First, inconsistent follow-up information and postoperative radiographic evaluation of the lungs do not allow consistent and complete assessment of time to metastasis and disease progression. Secondly, ne-cropsies were not performed in all dogs. This may have resulted in an underestimation of the frequency and lo-cation of metastatic disease. Other reported sites of me-tastasis include pleura, mediastinum, pericardium, lymph nodes, bone, eyes, kidneys, liver, and the adrenal gland.4,6–9Also, there were a number of dogs for which preoperative radiographs and serum alkaline phospha-tase concentrations, and preoperative biopsy samples were either not performed or not available.
We conclude that for dogs with canine appendicular chondrosarcoma, extended survival times are possible with amputation alone. Our data suggest that low to in-termediate grade chondrosarcoma carries a good prog-nosis, whereas high-grade tumors appear to behave aggressively. Future studies should evaluate whether postoperative chemotherapy provides a survival advan-tage over amputation alone, particularly with high-grade tumors. Clearly, the overall prognosis for appendicular chondrosarcoma is better than that of appendicular osteosarcoma treated by amputation alone or in combi-nation with chemotherapy.1
ACKNOWLEDGMENTS
The authors would like to thank Veterinary Society of Sur-gical Oncology (VSSO) members for support for this study, and especially Drs. Giorgio Romanelli, Paolo Buracco, Tara Britt, and Ralph Henderson for case submission.
REFERENCES
1. Dernell WS, Ehrhart NP, Straw RC, et al: Tumors of the skeletal system, in Withrow SJ, Vail DM (eds): Withrow & MacEwen’s Small Animal Clinical Oncology (ed 4). St. Louis, MO, Saunders, 2007, pp 540–582
2. Si-Kwang L: Tumors of bone and cartilage, in Bojrab MJ (ed): Disease mechanisms in small animal surgery (ed 2). Philadelphia, Pennsylvania, Lea & Febiger, 1993, pp 905 3. Brodey RS, McGrath JT, Reynolds H: A clinical and
radio-logical study of canine bone neoplasm’s. J Am Vet Med Assoc 134:53–71, 1959
4. Brodey RS, Misdorp W, Riser WH, et al: Canine skeletal chondrosarcoma: a clinicopathologic study of 35 cases. J Am Vet Med Assoc 165:68–78, 1974
5. Brodey RS, Sauer RM, Medway W: Canine bone neoplasms. J Am Vet Med Assoc 143:471–495, 1963
6. Popovitch CA, Weinstein MJ, Goldschmidt MH, et al: Chondrosarcoma: a retrospective study of 97 dogs (1987–1990). J Am Anim Hosp Assoc 30:81–85, 1994 7. Waltman SS, Seguin B, Cooper BJ, et al: Clinical outcome
of non-nasal chondrosarcoma in dogs: thirty-one cases (1986–2003). Vet Surg 36:266–271, 2007
8. Sylvestre AM, Brash ML, Atilola MAO, et al: A case series of 25 dogs with chondrosarcoma. Vet Comp Orthop Traumatol 5:13–17, 1992
9. Obradovich JE, Straw RC, Powers BE, et al: Canine chondrosarcoma: a clinicopathologic review of 55 cases (1983–1990).Proceedings Veterinary Cancer Society, 10th Annual Meeting, 1992, p 29 (abstract)
10. Malawer MM, Link MP, Donaldson SS: Sarcomas of the soft tissue and bone, in DeVita VT, Hellman S, Rosenberg SA (eds): Cancer: Principles and Practice of Oncology (ed 6). Philadelphia, PA, Lippincott, Williams & Wilkins, 2001, pp 1891–1930
11. Rozeman LB, Cleton-Jansen AM, Hogendoorn PCW: Pathology of primary malignant bone and cartilage tumors. Int Orthop 30:437–444, 2006
12. Evans, Ayala AG, Romsdahl MM: Prognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic grading. Cancer 40:818–831, 1977 13. Gibbs C, Denny HR, Lucke VM: The radiological features of
non-osteogenic malignant tumors of bone in the append-icular skeleton of the dog: a review of thirty-four cases. J Small Anim Pract 26:537–553, 1985