ContentslistsavailableatScienceDirect
Epidemics
jo u r n al h om ep ag e :w w w . e l s e v i e r . c o m / l o c a t e / e p i d e m i c s
Gender
asymmetry
in
concurrent
partnerships
and
HIV
prevalence
Ka
Yin
Leung
a,b,∗,
Kimberly
A.
Powers
c,
Mirjam
Kretzschmar
b,daUtrechtUniversity,POBox80010,3508TAUtrecht,TheNetherlands
bUniversityMedicalCenterUtrecht,POBox85500,3508GAUtrecht,TheNetherlands
cTheUniversityofNorthCarolinaatChapelHill,2105DMcGavran-GreenbergHall,CampusBox7435,ChapelHill,NC27599-7435,USA dNationalInstituteofPublicHealthandtheEnvironment,POBox1,3720BABilthoven,TheNetherlands
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30June2016
Receivedinrevisedform8January2017
Accepted15January2017
Availableonline20January2017
Keywords:
Concurrency
Genderasymmetry
Polygyny
HIVprevalence
Mathematicalmodel
a
b
s
t
r
a
c
t
ThestructureofthesexualnetworkofapopulationplaysanessentialroleinthetransmissionofHIV. Concurrentpartnerships,i.e.partnershipsthatoverlapintime,areimportantindeterminingthisnetwork structure.Menandwomenmaydifferintheirconcurrentbehavior,e.g.inthecaseofpolygynywhere womenaremonogamouswhilemenmayhaveconcurrentpartnerships.Polygynyhasbeenshown empir-icallytobenegativelyassociatedwithHIVprevalence,buttheepidemiologicalimpactsofotherforms ofgender-asymmetricconcurrencyhavenotbeenformallyexplored.Hereweinvestigatehowgender asymmetryinconcurrency,includingpolygyny,canaffectthediseasedynamics.Weuseamodelfora dynamicnetworkwhereindividualsmayhaveconcurrentpartners.Themaximumpossiblenumberof simultaneouspartnershipscandifferformenandwomen,e.g.inthecaseofpolygyny.Wecontrolfor meanpartnershipduration,meanlifetimenumberofpartners,meandegree,andsexuallyactivelifespan. Weassesstheeffectsofgenderasymmetryinconcurrencyontwoepidemicphasequantities(R0andthe
contributionoftheacuteHIVstagetoR0)andontheendemicHIVprevalence.Wefindthatgender
asym-metryinconcurrentpartnershipsisassociatedwithlowerlevelsofallthreeepidemiologicalquantities, especiallyinthepolygynouscase.Thiseffectondiseasetransmissioncanbeattributedtochangesin networkstructure,whereincreasingasymmetryleadstodecreasingnetworkconnectivity.
©2017TheAuthor(s).PublishedbyElsevierB.V.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Sexualbehaviorplaysanessentialroleinthetransmissionof HIVandothersexuallytransmittedinfections(STIs)ina popula-tion.Thereislargediversityinsexualbehavior,leadingtovarying risksofacquiringor transmittinginfection.Somebehavior pre-dominantlyinfluencestransmissibilityandsusceptibility,suchas condomuse.Otherbehavior,suchasconcurrency,influencesthe populationnetworkstructure.
WhetherconcurrentpartnershipsaredrivingHIVepidemicsin sub-SaharanAfricahasbeendiscussedanddebatedforalmost20 years(e.g.MorrisandKretzschmar,2000;HalperinandEpstein, 2004;LurieandRosenthal,2010;MahandHalperin,2010;Sawers and Stillwaggon, 2010; Kretzschmar et al., 2010; Epstein and Morris, 2011; Goodreau, 2011; Boily et al., 2011; Reniers and Watkins, 2010; Kretzschmar and Caraël, 2012). The biological
∗Correspondingauthor.Presentaddress:DepartmentofMathematics,Stockholm University,10691Stockholm,Sweden.
E-mailaddresses:[email protected](K.Y.Leung),[email protected]
(K.A.Powers),[email protected](M.Kretzschmar).
explanationbehindanimportantroleforconcurrencyis plausi-ble:inthesettingofserialmonogamy,anewlyinfectedindividual istypicallystillinapartnershiponlywithhis/herinfectorduring theacutephaseofHIV,i.e.theelevatedinfectiousnessinthefirst fewweeks/monthsimmediatelyafterinfection.Incontrast,when partnershipsoverlapintime,newlyinfectedindividualscan trans-mitinfectiontotheirsusceptiblepartnersinthisacutephase.It hasbeenhypothesizedandshownthroughmathematicalmodeling (Eatonetal.,2011)thattheinteractionbetweenacute infectious-nessand concurrentpartnershipscouldpotentially enhancethe spreadofHIVinthepopulation.
Someformsofconcurrencysuchaspolygyny(menmayhave multiple partners at a time while women are monogamous) naturallyleadtogenderasymmetry inconcurrentbehavior. An ecologicalstudyof34countriesinsub-SaharanAfricasuggested that thisformof concurrencyis negativelycorrelated withHIV prevalence in the population (Reniers and Watkins, 2010). A recentmodelingstudy(Reniersetal.,2015)comparingpolygyny togender-symmetricconcurrencyalsoconcludedthatpolygyny is associated withlower HIV prevalence. Besidespolygyny and gender-symmetricconcurrency,however,thereisabroadrange ofconcurrencypatternsexistinginpopulations.Inparticular,men
http://dx.doi.org/10.1016/j.epidem.2017.01.003
areoftenfoundtoreportmoreconcurrentpartnersthanwomen, butwomenmayalsohavemorethanonepartneratatime(Morris andKretzschmar,2000;Glynnetal.,2012;Maughan-Brown,2013). Itisnotstraightforwardtopredicthowthis‘intermediate’typeof asymmetricconcurrencymightaffectpopulation-levelHIV trans-mission. We therefore sought to assess through mathematical modelinghowvaryingtypesofgenderasymmetryinconcurrent partnerships–includingpolygyny–affectHIVdiseasedynamicsin apopulation.
AsmostHIVepidemicsinsub-SaharanAfricaarenowendemic, our main aim is to study the relationship between gender-asymmetricconcurrencyandendemicprevalence.Moreover,we studythebasicreproductionnumberR0andtherelative contribu-tionoftheacutestageofHIVtoR0.Howdoesgenderasymmetry affectthepopulationprevalence; aremoreasymmetric popula-tionsassociatedwithlowerlevelsofHIVprevalence(asfoundin
ReniersandWatkins,2010)?Inthisstudyweareinterestedinthe qualitativebehaviorandwedonotattempttomakeany quantita-tivepredictionsaboutdiseaseprevalence.Weuseamathematical modelforthespreadofHIVonadynamicsexualnetworkfora het-erosexualpopulationwherewecontrolforsexuallyactivelifetime, meanpartnershipduration,meandegree,andmeanlifetime num-berofpartners.Toparameterizethemodelweuseexistingdataon sexualbehaviorfromastudypopulationinMalawiandpublished estimatesofHIVinfectivityandnaturalhistoryparameters. Differ-entscenariosinthemaximumnumberofsimultaneouspartners areinvestigated.
2. Methods
2.1. Model
Weusea mathematical modeltostudytheeffect ofgender asymmetryinconcurrencyontransmissiondynamicsinthe pop-ulation.Tothis end, we usea previously introducedmodel for infectiondynamicsonadynamicnetworkthattakesintoaccount partnership formation and separation as well as demographic turnover(Leungetal.,2012,2015).Generalanalyticalresultsfor thespreadofinfectionsonnetworkshavemainlybeenforstatic networks(e.g.Diekmannetal.,1998;BallandNeal,2008;House andKeeling,2011;Miller etal.,2012).Early exceptionsaree.g.
Altmann(1995)andVolzandMeyers(2007)whoconsiderdisease transmissionondynamicnetworkswithoutdemographicturnover. Ourmodel,whichtakesintoaccountbothpartnershipchangesand demographicchanges,canbeseenasageneralizationofpair forma-tionmodelsthatdescribesequentiallymonogamouspopulations (whichwerefirstintroducedinepidemiologybyDietzandHadeler, 1988).
Inthispaper,weextendedthemodelofLeungetal.(2012,2015)
toaheterosexualpopulationwitha1:1sexratioandatwo-stage infectiousdisease.Concurrentpartnershipsaremodeledby allow-ingamaximumnumberofpartnersthatanindividualcanhaveat thesametime;wecallthisnumberthepartnershipcapacity.We assumethattherearetwopartnershipcapacitiesnmandnfformen
andwomeninthepopulation,respectively,andwevariedthese valuesacrossmodelscenarios(whileholdingthevaluesofnmand
nffixedacrossindividualswithinascenario).Newlyinfected
indi-vidualsareinthefirstphaseofinfectionandthenprogresstothe chronicphaseafteranexponentiallydistributedamountoftime. Aninfectiousindividualremainsinfectiousfortherestofhisorher sexuallyactivelife.Werefertothefirstandsecondphaseof infec-tionastheacuteandchronicphase,respectively.Theacutephaseis characterizedbyahighertransmissionratethanthechronicphase. Thenetworkstructureisstableovertime,whichleadsto sta-bledegree distributionsfor menand women(the degreeof an individualisthenumberofpartnersthatheorshehas).Themean
degreewaskeptconstantthroughoutthisstudy.However,the spe-cificlinkswithinthenetworkaredynamicintimeduetoindividuals formingnewpartnershipsandseparatingfromexistingpartners duringthecourseoftheirlife.Furthermore,thereisdemographic flowdue toindividuals enteringandleavingthesexuallyactive population.Infectionisassumedtohavenoimpactonpartnership formationorseparationnoronmortality.
Themodelisdeterministicinnature.Itisfullycharacterized byasetofparameterscomprisingsexualbehaviorandinfection parameters.Individualsarecharacterizedbysex-specific behav-ioralparameters;seeSections2.2and 2.3.We assumethatthe infectionparameters(i.e.transmissionratesanddisease progres-sion)donotdependongender(Hughesetal.,2012;Powersetal., 2008;Quinnetal.,2000).
Concurrencyismeasuredusingthepartnership-based concur-rencyindex(MorrisandKretzschmar,1997;Leung etal.,2012; LeungandKretzschmar,2015).Itmeasuresthemeannumberof additionalpartnersofanindividualinarandomlychosen partner-shipandcanbeexpressedintermsofthemeanandvarianceof adegreedistribution.Herewedistinguishbetweenconcurrency indicesmP andfPformenandwomen,respectively,andthe
con-currencyindexpopulP forthepopulationasawhole.Wevarythe gendersymmetryofconcurrencyinthepopulationbyvaryingnf
andnm.
Wehavepreviouslyderivedexplicitexpressionsforthedegree distributions,partnership-basedconcurrencyindices,basic repro-ductionnumberR0,and relativecontributionof theacutestage toR0intermsofmodelparameters(Leungetal.,2012,2015).The endemicprevalenceischaracterizedimplicitlyassolutionofafixed pointproblemthatcanbecomputednumerically.
Amoredetailedandtechnicaldescriptionofthemodelcanbe foundinAppendixAofthesupplementarydata.
2.2. Scenarios
ThroughoutthisstudywekeepmeanpartnershipdurationdP, sexuallyactivelifespan ¯L,andmeanlifetimenumberofpartners ¯
inthepopulationfixed.Thisalsomeansthatmeandegreeinthe populationisfixed(Eq.(A.2)inAppendixAofthesupplementary data).Thescenariosaredefinedbyvaryingthesex-specific quan-titiesnm,nf,Lf,andLm(whichalsovariesfandm,Eq.(A.1)in
AppendixA.1ofthesupplementarydata).
Wefocusongenderasymmetryinthemaximumnumberof partnersmenandwomenmayhaveatthesametime,i.e.in partner-shipcapacitiesnfandnm.Meanpartnershipcapacityisfixedacross
scenariosat ¯n=(nf+nm)/2=4.Theextremesaretheasymmetric
polygynous situation (nf, nm)=(1, 7) (i.e. women are
monoga-mous)andthesymmetricsituation(nf,nm)=(4,4).Notethat,since
infectionparametersaregenderindependent,asymmetryinthe oppositedirection((nf,nm)=(7,1)etc.)isautomaticallyincluded
byswitchingtheroleofmalesandfemalesintheresults.
MathematicalmodelsofheterosexualHIVtransmissionin sub-Saharan African settings commonly assume a sexually active populationbetween theages of 15 and 49 years (Eatonet al., 2012),correspondingtoanaveragesexuallyactivelifespan ¯Lof 35years.Differencesinthedurationofsexualactivitybysexare notwelldefined.Giventheuncertaintyinsexuallifespansformen andwomen,wemodeledthreescenarios:oneinwhichbothmen andwomenhadameansexuallifespanofLf=Lm=35years;onein
whichthesexuallyactivelifespanwasLf=33yearsforwomenand Lm=37yearsformen;andoneinwhichthesexuallyactive lifes-panwasLm=33yearsformenandLf=37yearsforwomen.Larger
Table1
The12differentscenarios.Correspondinglifetimenumberofpartnersaref=3.3
andm=3.7forLf=33years,Lm=37years,f=3.5=mforLf=35=Lmyears,and f=3.7andm=3.3forLf=37years,Lm=33years,seealsoSection2.3.
Lf=33years Lf=35years Lf=37years,
Lm=37years Lm=35years Lm=33years
(nf,nm)=(1,7) A1 A2 A3
(nf,nm)=(2,6) B1 B2 B3
(nf,nm)=(3,5) C1 C2 C3
(nf,nm)=(4,4) D1 D2 D3
Together,genderasymmetryinpartnershipcapacitiesand sex-uallyactivelifespansgiverisetotwelvedifferentscenarios;these aresummarizedinTable1.
2.3. Parameterizationofthemodel
Meanpartnershipdurationisbasedonself-reporteddataon steadypartnershipdurationcollectedinastudyofacuteHIV detec-tionstrategiesandlongitudinalHIVviraldynamicsatanSTIclinicin Lilongwe,Malawi.Samplingstrategiesandstudyprocedureshave beendescribedpreviously(Fiscusetal.,2007;Pilcheretal.,2007; Powersetal.,2007,2011a,b).Asourmodelassumesaconstant part-nershipdissolutionrate,wecalculatedtheslopeofalinearcurve fittedtothe reportedduration ofsteady partnerships(indays) onthex-axisandthe–ln(partnershipsurvival)onthey-axis,see AppendixBofthesupplementarydata.Weestimatedaweighted meanpartnershipdurationdPof3.92yearsacrossmenandwomen astheinverseofthisslope.
Sinceweareinterestedinqualitativebehaviorandwedonot aimtomakeanyquantitativepredictionsaboutdiseaseprevalence inthisstudy,themeanlifetimenumberofpartners ¯iscalibratedto anendemicHIVprevalenceofaround13%forscenariosB2andC2, correspondingtoestimatedHIVprevalenceinMalawiin2010(DHS Program,2010).Thisleadstoameanlifetimenumberofpartners ¯
=3.5.Consistencybetweenmeanlifetimenumberofpartners andsexuallifespanthendeterminesthemeanlifetimenumberof partnersm andffor menandwomen, thesearefoundbelow Table1(seealsoEq.(A.1)inAppendixA.1ofthesupplementary data).
Notethatourchoiceofkeepingmeansexualbehavior param-eters constant also leads toa constant mean degree acrossall scenarios, which isthe samefor menand women (Eq.(A.2)in Appendix A.1 ofthe supplementarydata). Variance, and there-foretheconcurrencyindex,doesdifferacrossthescenarios;see Section3.1fordetailsandadiscussion.
Infectionischaracterizedbythetransmissionratesˇ1,ˇ2and duration oftheacute phase dA (Table2).We letˇ1=2.76/year,
dA=2.9months,andˇ2=0.106/year(Hollingsworthetal.,2008). InAppendixC.3ofthesupplementarydataweconducted sensitiv-ityanalysisusinginfectivityparameterestimatesfromadifferent,
Table2
Modelparametersandvalues.Variationaroundtheparametervaluesareaddressed inthesensitivityanalysisinAppendixCofthesupplementarydata.
Parameter Description Estimate
nm Partnershipcapacityformen Varied(seeTable1)
nf Partnershipcapacityforwomen Varied(seeTable1)
dP Meanpartnershipduration 3.92years
Lf Sexuallyactivelifespanforwomen Varied(seeTable1)
Lm Sexuallyactivelifespanformen Varied(seeTable1)
¯
L=1
2(Lf+Lm) Sexuallyactivelifespan 35years
f Meanlifetimenumberofpartnersfor
women
Varied(seeTable1)
m Meanlifetimenumberofpartnersfor
men
Varied(seeTable1)
¯
=1
2(f+m) Meanlifetimenumberofpartners 3.5
ˇ1 Transmissionrateacutephase 2.76/year
dA Durationacutephase 2.9months
ˇ2 Transmissionratechronicphase 0.106/year
morerecentlypublishedstudy(Bellanetal.,2015).InBellanetal. (2015)amuchlowertransmissionratefortheacutestageof infec-tionwasestimatedbutahighertransmissionrateforthechronic stageofinfection(yieldingacomparabletotalinfectivity). Qualita-tively,thisdidnotchangeourconclusions.
ParametervaluesaresummarizedinTable2.Variationaround theparametervaluesareaddressedinthesensitivityanalysisin AppendixCofthesupplementarydata.
3. Results
ThethreedifferentsexuallyactivelifespancasesLf<Lm,Lf=Lm,
andLf>Lmleadtoverysimilarresultsfornetworkstructure,R0, andtherelativecontributionoftheacutephasetoR0.Therefore,in bothSections3.1and3.2,wefocusonthesexuallyactivelifespan caseLf=Lm,i.e.scenariosA2,B2,C2,andD2.InSection3.3all12
scenarios(definedinTable1)areconsidered.Asensitivityanalysis wascarriedoutinAppendixCofthesupplementarydata,which showsthattheresultspresentedinthissectionarequalitatively robusttovariationsinparametervalues.
3.1. Networkstructure
Astheoveralldegreedistributions(acrosswomenandmen)are verysimilaracrossscenariosB2,C2,andD2,weshowonlyscenarios A2andD2inFig.1.Ourdefinitionofscenariosleadstoaconstant meandegreeformenandwomenacrossall12scenariosanditis givenby ¯/Ld¯ P=0.39(notethatthisisindependentofgenderand partnershipcapacity).Thevarianceformenandwomendoesdiffer acrossthescenarios.VariancevaluesforscenariosA2,B2,C2,and D2aresummarizedinTable3(variancevaluesfortheothereight scenariosaresimilar).
Wefindthatthedegreedistributionformenissimilaracross allfourscenarios,illustratedbythetwomostextremescenarios
men women
7 6 5 4 3 2 1 0
number of partners
0 0.2 0.4 0.6
probability
Scenario A2
men women
7 6 5 4 3 2 1 0
number of partners
0 0.2 0.4 0.6
probability
Scenario D2
(a) (b)
Table3
Thedegreevarianceforwomen(f)andmen(m)forthescenariosA2,B2,C2,andD2 (Table1).Meandegreeis0.39forbothmenandwomenacrossallscenarios.
A2 B2 C2 D2
f m f m f m f m
0.24 0.38 0.32 0.37 0.35 0.37 0.36 0.36
A2andD2andthedegreevarianceinTable3.Thekeydifference acrossscenariosisinthedegreedistributionsforwomen:inA2, womenaremonogamousandcanhaveeitherzerooronepartner, whichisdistinctlydifferentfromscenariosB2,C2,andD2,where therearefractionsofwomenwithmorethanonepartneratatime. Thedegreedistributionformenandwomentogetherare impor-tantinmakingupthenetworkstructure,thisisillustratedbyFig.2. InFig.2networksforscenariosA2andD2arevisualizedby simu-latingcross-sectionsofthenetworksusingdegreedistributionsof
Fig.1.Networkstructureissignificantlydifferentinthetwo scenar-iosA2andD2.InscenarioD2,longer‘chains’ofpartnershipscanbe found,e.g.achainconsistingofsixindividuals.Thisisabsentin sce-narioA2wherewomenhaveatmostonepartneratatime(sochains consistofatmostthreeindividuals).NotethatFig.2represents snapshotsofonerandomlychosenpointintimeasthenetworks areevolvingintimewithpartnershipformationanddissolutionas wellasindividualsenteringandleavingthesexuallyactive popula-tion.Furthermore,singleindividualsareomittedfromthenetwork figurestobettershowthepartnerships.Finally,although partner-shipcapacitychoicesinprincipleallowformuchlargerconnected components,ourparametervaluesinthisstudyaresuchthatthis israrelythecase;thereisonlyaverysmallfractionofthe popula-tionwithmorethantwopartners(Fig.1).Nevertheless,thesmall proportionoflongerchainsintheD2networkresultin substan-tiallyhigherratesofdiseasetransmissioninthenon-polygynous scenarios(Sections3.2and3.3).
Next,weconsiderthelevelofconcurrencyforthescenariosA2, B2,C2,andD2.Differentaspectsofconcurrency,suchasthemean numberofconcurrentpartnershipsandthemeandurationof over-lap,arecapturedbythedegreedistributioninthepopulation(Fig.1
andnetworkparameterssuchasthemeanpartnershipduration andlifetimenumberofpartners).Fromthedegreedistributions inFig.1,weobservethatonlysmallfractionsofmenandwomen haveconcurrentpartnerships,i.e.morethantwopartners,acrossall scenarios,andalargeproportionofthepopulationiswithoutany partner.Wecombinetheseaspectsofconcurrencyandmeasure thelevelofconcurrencywiththepartnership-basedconcurrency index(cf.MorrisandKretzschmar,1997;Leungetal.,2012;Leung
Fig.3. Theconcurrencyindexm P formen,
f
Pforwomen,and
popul
P forthe
popula-tion,inscenariosA2,B2,C2,andD2.
andKretzschmar,2015,seealsoAppendixAofthesupplementary data).TheresultsarepresentedinFig.3.
Notethatfemaleconcurrencyiszerofornf=1(monogamy)and
increasesfornf=2,3,4.Maleconcurrencyishighestinthemost
asymmetricscenarioA2anddecreaseswithmoresymmetric sce-narios.Similartothecaseforwomen,thisdecreaseinconcurrency iscausedbyadecreaseinthemaximumnumberofsimultaneous partnerships(nm=7,6, 5,4).Thedecreasein maleconcurrency isless thantheincreaseinfemaleconcurrency.Therefore, with increasingequalityofmenandwomeninthenumbersofpartners theymayhaveatthesametime,theoverallpopulation-level con-currencyindexpopulP increases,evenifaveragelifetimenumbers ofpartnersremainconstant.
3.2. R0andthecontributionoftheacutephasetoR0
ThebeginningoftheepidemicisstudiedbyconsideringR0and therelativecontributionoftheacutephasetoR0forscenariosA2, B2,C2,andD2inFig.4.R0 increaseswithincreasingsymmetry inthepopulation.InallfourscenariosR0isabovetheepidemic thresholdvalueone.
Transmissionofdiseaseduringtheprimaryphaseisstrongly determinedbyconcurrency(combineFig.3withFig.4).Onlyif concurrentpartnersareavailableduringtheprimaryphasecanthe infectionbetransmittedinthatphase,becauseseparationand find-inganewpartnerrequiresamuchlongertime.Inthepolygynous scenariothenetworkstructureismadeupofshortchainsof part-nerships(involvingamaximumofthreeindividuals,seealsoFig.2). Therefore,itisreasonablethatprimaryinfectionwillhavelittle impactinthepolygynousscenarioA2.Theacutephasedoesplaya
Scenario D2 Scenario A2
men women partnerships
) b ( )
a (
chronic phase acute phase
1.0% 10.9% 12.4% 12.7%
Fig.4.R0inthefourscenariosA2,B2,C2,andD2.Thedashedlinerepresentsthe
epidemicthresholdvalueofone.Thelightanddarkgreenindicatethefractionof
R0thatiscausedintheacuteandchronicphaseofinfection,respectively,whilethe
heightofthebarrepresentsR0.(Forinterpretationofthereferencestocolorinthis
figurelegend,thereaderisreferredtothewebversionofthisarticle.)
(n ,n )=(1,7)f m
(n ,n )=(2,6)f m
(n ,n )=(3,5)f m
(n ,n )=(4,4)f m
A1 B1 C1 D1
A2 B2 C2 D2
A3 B3 C3 D3
Fig.5.Theendemicprevalenceinthepopulationforthe12differentscenarios plot-tedasafunctionofsexuallyactivelifespanwithpartnershipcapacitiesfixed.The correspondingscenario(seeTable1)isdenotedforeachpointinthegraph.
significantroleintheotherthreescenarioswithacontributionof upto∼13%toR0.
3.3. Endemicprevalence
InFig.5populationHIVprevalenceisconsideredasafunction oftheconcurrencyandsexuallyactivelifespanscenarios.
SimilartothequantitiesexploredinSections3.1and3.2,from theresultsinFig.5weconcludethatgenderasymmetryinsexually activelifespanshavelittleeffectonpopulationprevalence (com-paree.g.scenariosB1,B2,andB3toeachother,thesescenarioshave thesamegenderasymmetryinconcurrencybutdifferentsexually activelifespanscenarios).Moreover,weseethatgenderasymmetry inconcurrentpartnershipsdoeshaveanimportanteffecton popu-lationprevalence(comparee.g.scenariosA1,B1,C1,andD1toeach other,wheregenderasymmetryinconcurrentpartnershipis var-iedbutsexuallyactivelifespansarethesame).Inparticular,wefind
thatthepolygynoussettingAisassociatedwithmuchlowerlevels ofdiseaseprevalencecomparedtotheotherconcurrencysettings B,C,andD.Thisisconsistentwiththenetworkstructurein set-tingAcomparedtotheothersettings(seealsoFig.2).InsettingA, thelongestchainsofpartnershipsinvolveatmostthree individu-als(menhavingmorethanonepartner).Potentiallymuchlonger chainsofpartnershipscanbefoundintheothersettings(seeFig.2
fora simulatedcross-sectionofanetwork structurein scenario D2;scenariosB2andC2areinbetweenA2andD2intermsoftheir networkstructure).
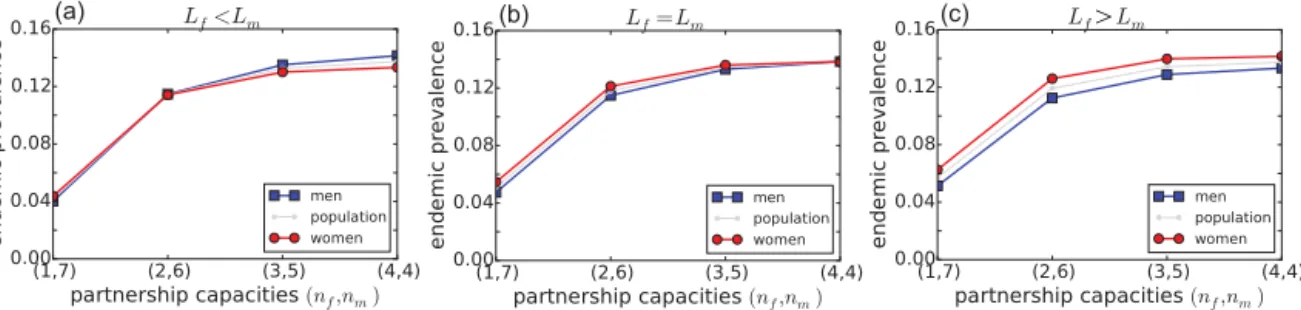
Weinvestigatethegenderasymmetryfurtherbyconsidering endemicprevalenceseparatelyformenandwomenasafunction ofpartnershipcapacityscenariosinFig.6.Thefactthatendemic prevalenceisinareasonablerange(DHSProgram,2010)isa con-sequenceofourparametervaluechoicefor ¯(recallSection2.3: wecalibrated¯toanendemicdiseaseprevalenceofaround13%in thepopulationforthescenariosB2andC2;seeFig.6).Ourinterest wasinthequalitativebehavior,inparticularweareinterestedin comparingtheendemicprevalencesofscenariosA2,B2,C2,and D2relativetoeachother.Wefindthat,qualitatively,gender asym-metryinpartnershipcapacityisassociated withlowerendemic prevalenceinthepopulation.Again,thisimpliesthatmoreequally distributedconcurrencybehaviorcanleadtohigher epidemiolog-icaloutcomes.
Next,thereisalsogenderasymmetryindiseaseprevalence.In
Fig.6(b)and(c)femaleprevalenceishigherthanmaleprevalence forallfourpartnershipcapacitycombinations.Wefindthatthe female-to-maleratioofHIVprevalencerangesfrom1inscenarioD2 (symmetricsexuallifespansandpartnershipcapacities)to1.22in scenarioA3(Lf>Lmandgreatestasymmetryinpartnership
capac-ities).ThisgenderratioislargestinFig.6(c).However,inFig.6(a) for(nf,nm)=(3,5),and(4,4),femaleprevalenceisslightlylower
thanmaleprevalence.Sensitivityanalysisshowsthatthisisa gen-eralresultforpartnershipcapacitycombination(nf,nm)=(4,4)and Lm>Lf(Fig.C.6inAppendixCofthesupplementarydata).Onthe
otherhand,thesameanalysisshowsthatfor(nf,nm)=(1,7),female
prevalenceisalwayslargerthanmaleprevalenceregardlessof gen-derdifferencesinsexuallyactivelifespans(so(nf,nm)=(2,6),(3,5)
liesomewhereinbetween).Thefemale-to-maleratioofHIV preva-lenceisonlyslightlyskewedtowardswomeninFig.6.However,we consideredonlyrelativelysmalldifferencesinlifespansbetween menandwomen. Wefindthat thefemale-to-male ratioofHIV prevalencebecomesmuchmoreskewedtowardswomenwhenthe female-to-maleratioofsexuallyactivelifespansalsoincreases(Fig. C.6inAppendixCofthesupplementarydata).
We conclude thatnot only is gender asymmetryin concur-rentpartnershipsassociatedwithlowerdiseaseprevalence,italso affectsthefemale-to-maleratioofprevalence.Genderasymmetry inconcurrentpartnershipsisassociatedwithanincreasedgender asymmetryindiseaseprevalence.Whilegenderasymmetryin sex-uallyactivelifespanshaslittleeffectontotalpopulationprevalence, itdoesaffectthegenderratioindiseaseprevalence.
(a) (b) (c)
>
(a)
0.0 0.1 0.2 0.3 0.4 0.5 0.6
popu
lat ion concurr
ency
0.00 0.05 0.10 0.15 0.20
fra
c
ti
o
n
case A case D
(b)
0.0 0.1 0.2 0.3 0.4 0.5 0.6
popu
lat ion concurr
ency
0.00 0.05 0.10 0.15 0.20 0.25 0.30 0.35 0.40
e
nd
em
ic
p
rev
al
en
c
e
case Acase D
(c)
Fig.7.Correlationbetweenpopulationconcurrencyand(a)R0,(b)therelativecontributionoftheacutephasetoR0,and(c)populationprevalence,whenvaryingmodel
parametersinthesensitivityanalysis(seeAppendixCofthesupplementarydata).CaseAcorrespondstotheasymmetricpolygynoussettingandcaseDcorrespondstothe symmetricsetting.
3.4. Concurrencyandepidemiologicaloutcomes
Takingtheresultsof Sections3.1–3.3together,weconclude thattheepidemiologicalquantitiesR0,therelativecontributionof theacutephase toR0,andtheendemicprevalenceare increas-ingwithincreasingconcurrencyinthepopulation(combineFig.3
witheitherFig.4,orFig.6).Theeffectofgender-asymmetric con-currencyonepidemiologicalparametersthusappearstobeinpart mediatedthroughincreasedoverallconcurrency.Moreover,inour sensitivityanalysiswhereweallowforvariationinallparameter valuessimultaneously,wefindaverystrongcorrelationbetween population-levelconcurrencyandR0andpopulationdisease preva-lence;seeFig.7(a)and(c)andAppendixCofthesupplementary datafordetails.Thissuggeststhat,althoughallsexualbehavior parametersseparatelyhaveanimpactonprevalence,the syner-gisticcombinationoftheseparametersintheconcurrencyindex
populP yieldsamuchmorepronouncedcorrelation.Thiscorrelation
ismuchlessstrong(butclearlystillexistent)whenconsideringthe relativecontributionoftheacutephasetoR0;seeFig.7(b).
4. Conclusionanddiscussion
Inthisstudyweinvestigatedtheeffectofgenderasymmetry inthemaximumnumberofsimultaneouspartnershipsan individ-ualcanhave,theso-calledpartnershipcapacity,onHIVdisease dynamics.Ourstudywasqualitativeinnatureandcannotbeused tomake anyquantitativestatements.Motivatedbythefindings ofReniersandWatkins(2010),wewereespeciallyinterestedin
theextremecaseofpolygynousunions,i.e.(nf,nm)=(1,7),with
additionalinterestinothertypesofasymmetries.Wefoundthat allthreeepidemiologicaloutcomesR0,therelativecontributionof theacutephase toR0,andendemicprevalencearemuchlower inthepolygynousscenariothaninmoregendersymmetriccases. Thesefindingshighlightpolygynyasaspecialcaseofasymmetric concurrencythatmaybeparticularlyprotectiveatthepopulation level.However,theepidemiologicaloutcomeswerealsolowerin theothertwogenderasymmetricscenarios (nf, nm)=(2,6)and
(3,5)compared tothesymmetricscenario (nf,nm)=(4,4).Our
modelresultsshowthat anylevel ofasymmetryleadstolower endemicprevalencethanapopulationwithfullsymmetry. There-fore,consistentwiththefindingsofReniersandWatkins(2010), ourresultssupportthatpolygyny,evenifpracticedonlybyapart ofthepopulation,canindeedreduceHIVprevalenceascompared toafullymixedpopulationwherebothsexeshaveequalnumbers ofconcurrentpartners.However,basedonourstudy,wherewe controlledformanynetworkstatisticssuchasmeanpartnership duration,itisnotpossibletosayhowtheeffectofpolygynyinthe modelextendstoacausalexplanationfortheecologicalcorrelation betweenpolygynyandprevalenceinReniersandWatkins(2010). We also investigated the influence of gender asymme-try in sexually active lifespans Lf and Lm for women and
inthesexuallyactivepopulation, weconsideredthreedifferent cases(but seeLindauand Gavrilova,2010 for anestimation of sexuallyactivelifespansforaheterosexualpopulationintheUSA). Nevertheless,genderasymmetryinsexuallyactivelifespansdid notqualitativelychangeourfindingsaboutgenderasymmetryin partnershipcapacitiesandtheassociationwiththeepidemiological quantitiesunderconsideration.Additionally,wefoundthatincase ofgendersymmetricsexuallyactive lifespans(Lf=Lm)orlonger
sexuallyactivelifespansforwomenthanmen(Lf>Lm),the
female-to-maleratioofHIV prevalenceisskewedtowardswomen.The sensitivityofHIVprevalenceratiostodifferencesinsexuallifespans whenweconsideredabroaderrange(Fig.C.6inAppendixCofthe supplementarydata)indicatesthatmoreempiricalinformation– andattentioninmodeling–onsexuallyactivelifespansandtheir effectsisneededtobetterunderstandthesedurations.
Consistent with our findings, HIV prevalence data indeed showsthat morewomen thanmenareliving withHIVin sub-SaharanAfrica,e.g.inMalawi(UNAIDS,2013;DHSProgram,2010). Empiricalestimatesofthefemale-to-maleratioofinfectionsin sub-SaharanAfricanpopulationsrangefrom1.31to2.21(Reniersetal., 2015).Manyfactorscanleadtothesedifferences,andoneofthem couldbethedifferenceinconcurrentpartnershipsbetweenmen andwomen.Theratiosinourstudyaresmallerthantheempirical estimates,mostlikelybecauseweonlyinvestigatedtheeffectof genderasymmetryinconcurrentpartnerships.
Ourmainfocuswasontheeffectofgenderasymmetryin part-nershipcapacitiesonHIVprevalencewhilecontrollingformean partnership duration, mean lifetime number of partners, mean degree,sexuallyactivelifespan,andinfectionparameters.Wewere nottryingtoisolatetheeffectoftheseasymmetriesindependently ofoverallconcurrency,ratherwe wantedtoseethetotaleffect oftheseasymmetries(evenifpartiallymediatedthroughchanges inoverallconcurrency).Wefoundthatanyofthesexualbehavior parameters,suchaslifetimenumberofpartnersandpartnership durationcorrelatepositivelywiththeepidemiologicalquantities. Thereisaparticularlystrongcorrelationbetweenpopulation-level concurrency with R0 and population disease prevalence (Sec-tion3.4).Similarquestionsongenderasymmetryinconcurrency andHIVprevalencewereaddressedinReniersetal.(2015).Their focuswasoncomparingpolygynyandgender-symmetric concur-rencyandtheireffectonthefemale-to-maleratioofHIVprevalence usinganagent-basedmodelingapproach.Inourstudywelooked atothertypesofgender-asymmetricconcurrencybeyondpolygny. Moreover,inourstudy,thelevelsofconcurrencyinthepopulation weredeterminedbysexualbehaviorparametersthatwerekept constantthroughoutdifferentscenarios.Asaconsequence,gender asymmetryledtoaslightlylowerlevelofoverallconcurrencyinthe populationcomparedtogendersymmetry.Therefore,resultsfrom ourstudyarenotdirectlycomparablewithReniersetal.(2015). However,consistentwithourfindings,Reniersetal.(2015)found thathigherlevelsofconcurrencyareassociatedwithhigherdisease prevalence.
Thereareofcoursemanyfactorsthatcanplayarolein deter-miningdiseasedynamics.Forexample,agemixing(whereyoung womentendtoformpartnershipswitholdermen)hasbeen pro-posedasanexplanationincreatingthedifferenceinHIVprevalence in men and women (Kellyet al., 2003; Leclerc-Madlala, 2008; Maughan-Brownetal.,2014).Butnotethattherearealso longitu-dinalcohortstudiesfindingnoincreaseinHIVacquisitionamong youngwomenwitholderpartnersinSouthAfrica(Jewkersetal., 2012;Harlingetal.,2014;Balkusetal.,2015).Inourmodel,partner acquisition(orseparation)doesnotdependontheageof individu-alsatall.Changesinbehavioroverthecourseoftheepidemicand heterogeneityinbehavioracrossindividualsofagivensexarealso notconsidered.Obviouslythesefactorsmayalsobeofinfluence, althoughnon-linearitiesinepidemicsystemsmakeitdifficultto
predicttheexactnatureoftheseinfluences(butseeReniersetal., 2015wheretheyfindthatbehaviorchangeamongHIV-positive womencanenlargethegenderasymmetryindiseaseprevalence). Ourmodelalsodidnotdifferentiatebetweenlong-and short-termpartnerships. Withrespecttopartnershipduration,wedid performsensitivityanalysisthatshowedthatendemicprevalence andR0increasewithincreasingpartnershipduration.Ina popu-lationwithonlyshorttermpartnerships, endemictransmission cannotbemaintained(withoutincreasingnumbersofpartners). However,wehypothesizethatinapopulationwitha combina-tionofshortandlongpartnerships,there couldbea synergistic effectofthetwo,withshort-termpartnershipsenabling transmis-sionduringprimaryinfectionandlong-termpartnershipsensuring a sufficientlyhighreproductionnumber.Futuremodeling work that includes different types of partnerships will allow analy-sesofgender-asymmetricconcurrencyeffectsonepidemiological parameterswithinthistypeofmorerealisticsystem.
Anothermodel aspectworth mentioningis that we didnot include anydisease-relatedmortality,whichwould shortenthe infectiousperiod.Asaconsequence,infectiousindividualswould remaininthesexuallyactivepopulationforashortertime,causing fewersecondarycasesthanifthereisnodisease-relatedmortality. Inclusionofthisphenomenoncouldthenleadtolowerlevelsof diseaseprevalence.However,assumingthatdisease-related mor-talityaffectsbothgendersinthesameway,webelievethatitwill notinfluencetherelationshipsdemonstratedinthispaper.
Inconclusion,genderasymmetryinthemaximumnumberof concurrentpartnershipscanaffecttheepidemicandendemicstates ofHIVtransmissiondynamics,withtheseeffectsbeingpartially mediatedthroughchangesinoverallconcurrencylevels.Our find-ingssuggestthatincreasedasymmetryisassociatedwithdecreased endemicprevalence,R0,andtheacute-phasecontributiontoR0, particularlyinthespecialcaseofpolygyny.Thisprovidespotential mechanisticexplanationsforassociationsbetweenpolygynyand keyepidemiologicalmeasuresofdiseasetransmission.Thefindings inthisstudyhelptoroundoutpriorempiricalandmodelingstudies byaddingconsiderationsofscenariosbetweenthetwoextremes ofsymmetricconcurrencyandpolygyny.Wealsofindthatgender imbalancesinconcurrencymaypartiallyexplainhigherobserved HIVprevalenceinfemalesvs.malesincontextswheresexual lifes-pansforfemalesareatleastaslongasformales.Takentogether,our findingsindicatethatimprovedempiricalunderstandingof male-vs-female concurrency patternsand sexuallifespans,combined withourmodelinginsightsabouttheeffectsofthesequantities onHIVtransmissiondynamics,couldimprove understandingof observedepidemiologicalpatternsacrossHIV-endemicsettings.
Funding
K.Y.L.issupportedbytheNetherlandsOrganisationfor Scien-tificResearch(NWO)[grantMozaïek017.009.082]andtheSwedish ResearchCouncil(VR)[grant2015-050153].K.A.P.issupportedby theNationalInstitutesofHealth(NIH)[grantKL2TR001109].
Acknowledgements
We thanktwoanonymousreviewersforcarefulreading and usefulsuggestionsthathelpedimprovedthearticle.
AppendixA. Supplementarydata
References
Altmann,M.,1995.Susceptible-infected-removedepidemicmodelswithdynamic
partnerships.J.Math.Biol.33,661–675.
Balkus,J.E.,Nair,G.,Montgomery,E.T.,Mishra,A.,Palanee-Philips,T.,Ramjee,G., Panchia,R.,Selepe,P.,Richardson,B.A.,Chirenje,Z.M.,Marrazzo,J.M.,2015.
Age-disparatepartnershipsandriskofHIV-1acquisitionamongSouthAfrica womenparticipatingintheVOICEtrial.J.Acquir.ImmuneDefic.Syndr.70, 212–217.
Ball,F.,Neal,P.,2008.Networkepidemicmodelswithtwolevelsofmixing.Math. Biosci.212,69–87.
Bellan,S.E.,Dushoff,J.,Galvani,A.P.,Meyers,L.A.,2015.ReassessmentofHIV-1 acutephaseinfectivity:accountingforheterogeneityandstudydesignwith simulatedcohorts.PLoSMed.12(3),e1001801.
Boily,M.-C.,Alary,M.,Baggaley,R.F.,2011.Neglectedissuesandhypotheses regardingtheimpactofsexualconcurrencyonHIVandsexuallytransmitted infections.AIDSBehav.16(2),304–311.
DemographicandHealthSurveys,2015.DHSProgramSTATcompiler,Avaliable:
http://beta.statcompiler.com/(accessed:15.10.15).
DHSProgram,2010.(DemographicandHealthSurveys)HIVFactSheets,Available:
http://dhsprogram.com/publications/publication-HF34-HIV-Fact-Sheets.cfm
(accessed:05.08.15).
Diekmann,O.,deJong,M.C.M.,Metz,J.A.J.,1998.Adeterministicepidemicmodel takingaccountofrepeatedcontactsbetweenthesameindividuals.J.Appl. Prob.35(2),448–462.
Dietz,K.,Hadeler,K.P.,1988.Epidemiologicalmodelsforsexuallytransmitted diseases.J.Math.Biol.26,1–25.
Eaton,J.W.,Hallett,T.B.,Garnett,G.P.,2011.Concurrentsexualpartnershipsand primaryHIVinfection:acriticalinteraction.AIDSBehav.15(4),687–692.
Eaton,J.W.,Johnson,L.F.,Salomon,J.A.,Barnighausen,T.,Bendavid,E.,Bershteym, A.,Bloom,D.E.,Cambiano,V.,Fraser,C.,Hontelez,J.A.C.,Humair,S.,Klein,D.J., Long,E.F.,Philips,A.N.,Pretorius,C.,Stover,J.,Wenger,E.A.,Williams,B.G., Hallett,T.B.,2012.HIVtreatmentasprevention:systematiccomparisonof mathematicalmodelsofthepotentialimpactofantiretroviraltherapyonHIV incidenceinSouthAfrica.PLoSMed.9(7),e1001245.
Epstein,H.,Morris,M.,2011.ConcurrentpartnershipsandHIV:aninconvenient truth.J.Int.AIDSSoc.14,13.
Fiscus,S.A.,Pilcher,C.D.,Miller,W.C.,Powers,K.A.,Hoffman,I.F.,Price,M., Chilongozi,D.A.,Mapanje,C.,Krysiak,R.,Gama,S.,Martinson,F.E.,Cohen,M.S., 2007.Rapid,real-timedetectionofacuteHIVinfectioninpatientsinAfrica.J. Infect.Dis.195,416–424.
Glynn,J.R.,Dube,A.,Kayuni,N.,Floyd,S.,Molesworth,A.,Parrott,F.,French,N., Crampin,A.C.,2012.Measuringconcurrency:anempiricalstudyofdifferent methodsinalargepopulation-basedsurveyinnorthernMalawiand evaluationoftheUNAIDSguidelines.AIDS26(8),977–985.
Goodreau,S.M.,2011.Adecadeofmodellingresearchyieldsconsiderableevidence fortheimportanceofconcurrency:aresponsetoSawersandStillwaggon.J. Int.AIDSSoc.14,12.
Halperin,D.,Epstein,H.,2004.Concurrentsexualpartnershipshelptoexplain Africa’shighprevalence:implicationsforprevention.Lancet364,4–6.
Harling,G.,Newell,M.-L.,Tanser,F.,Kawachi,I.,Subramanian,S.V.,Bärnighausen, T.,2014.Doage-disparaterelationshipsdriveHIVincidenceinyoungwomen? EvidencefromapopulationcohortinruralKwaZulu-Natal,SouthAfrica.J. Acquir.ImmuneDefic.Syndr.66,443–451.
Hollingsworth,T.D.,Anderson,R.M.,Fraser,C.,2008.HIV-1transmission,bystage ofinfection.J.Infect.Dis.198(5),687–693.
House,T.,Keeling,M.J.,2011.Insightsfromunifyingmodernapproximationsto infectionsonnetworks.J.R.Soc.Interface8,67–73.
Hughes,J.P.,Baeten,J.M.,Lingappa,J.R.,Magaret,A.S.,Wald,A.,deBruyn,G.,Kiarie, J.,Inambao,M.,Kilembe,W.,Farquhar,C.,Celum,C.,Thepartnersinprevention HSV/HIVtransmissionstudyteam,2012.Determinantsofper-coital-actHIV-1 infectivityamongAfricanHIV-1-serodiscordantcouples.J.Infect.Dis.205, 358–365.
Jewkers,R.,Dunkle,K.,Nduna,M.,JamaShai,N.,2012.TransactionalsexandHIV incidenceinacohortofyoungwomenintheSteppingStoneTrial.J.AIDSClin. Res.3.
Kelly,R.J.,Gray,R.H.,Sewankambo,N.K.,Serwadda,D.,Wabwire-Mangen,F., Lutalo,T.,Wawer,M.J.,2003.Agedifferencesinsexualpartnersandriskof HIV-1infectioninruralUganda.J.Acquir.ImmuneDefic.Syndr.32,446–451.
Kretzschmar,M.,Caraël,M.,2012.IsconcurrencydrivingHIVtransmissionin sub-SaharanAfricansexualnetworks?Thesignificanceofsexualpartnership typology.AIDSBehav.16(7),1746–1752.
Kretzschmar,M.,White,R.G.,Caraël,M.,2010.Concurrencyismorecomplexthan itseems.AIDS24(2),313–315.
Leclerc-Madlala,S.,2008.Age-disparateandintergenerationalsexinSouthern Africa:thedynamicsofhypervulnerability.AIDS22(Suppl.4),S17–S25.
Leung,K.Y.,Kretzschmar,M.E.E.,2015.ConcurrencycanmoveR0forHIVacrossthe epidemicthreshold.AIDS29,1097–1103.
Leung,K.Y.,Kretzschmar,M.E.E.,Diekmann,O.,2012.Dynamicconcurrent partnershipnetworksincorporatingdemography.Theor.Popul.Biol.82, 229–239.
Leung,K.Y.,Kretzschmar,M.E.E.,Diekmann,O.,2015.SIinfectionofadynamic partnershipnetwork:characterizationofR0.J.Math.Biol.71,1–56.
Lindau,S.T.,Gavrilova,N.,2010.Sex,health,andyearsofsexuallyactivelifegained duetogoodhealth:evidencefromtwoUSpopulationbasedcrosssectional surveysofageing.BMJ340,c810.
Lurie,M.N.,Rosenthal,S.,2010.ConcurrentpartnershipsasadriveroftheHIV epidemicinsub-SaharanAfrica?Theevidenceislimited.AIDSBehav.14, 17–24.
Mah,T.L.,Halperin,D.T.,2010.ConcurrentsexualpartnershipsandtheHIV epidemicsinAfrica:evidencetomoveforward.AIDSBehav.14,11–16.
Maughan-Brown,B.,2013.Concurrentsexualpartnershipsamongyoungadultsin
CapeTown,SouthAfrica:howisconcurrencychanging?Sex.Health10, 246–252.
Maughan-Brown,B.,Kenyon,C.,Lurie,M.N.,2014.Partneragedifferencesand concurrencyinSouthAfrica:implicationsforHIV-infectionriskamongyoung women.AIDSBehav.18(12),2469–2476.
Miller,J.C.,Slim,A.C.,Volz,E.M.,2012.Edge-basedcompartmentalmodellingfor infectiousdiseasespread.J.R.Soc.Interface9(70),890–906.
Morris,M.,Kretzschmar,M.,1997.ConcurrentpartnershipsandthespreadofHIV. AIDS11,641–648.
Morris,M.,Kretzschmar,M.,2000.Amicrosimulationstudyoftheeffectof concurrentpartnershipsonthespreadofHIVinUganda.Math.Popul.Stud.8 (2),109–133.
Pilcher,C.D.,Joaki,G.,Hoffman,I.F.,Martinson,F.E.A.,Mapanje,C.,Stewart,P.W., Powers,K.A.,Galvin,S.,Chilongozi,D.,Gama,S.,Price,M.A.,Fiscus,S.A.,Cohen, M.S.,2007.AmplifiedtransmissionofHIV-1:comparisonofHIV-1
concentrationsinsemenandbloodduringacuteandchronicinfection.AIDS 21,1723–1730.
Powers,K.A.,Ghani,A.C.,Miller,W.C.,Hoffman,I.F.,Pettifor,A.E.,Kamanga,G., Martinson,F.E.A.,Cohen,M.S.,2011a.TheroleofacuteandearlyHIVinfection inthespreadofHIVandimplicationsfortransmissionpreventionstrategiesin Lilongwe,Malawi:amodellingstudy.Lancet378,256–268.
Powers,K.A.,Hoffman,I.F.,Ghani,A.C.,Hosseinipour,M.C.,Pilcher,C.D.,Price,M.A., Pettifor,A.E.,Chilongozi,D.A.,Martinson,F.E.A.,Cohen,M.S.,Miller,W.C., 2011b.SexualpartnershippatternsinMalawi:implicationsforHIV/STI transmission.Sex.Transm.Dis.38,657–666.
Powers,K.A.,Miller,W.C.,Pilcher,C.D.,Mapanje,C.,Martinson,F.E.A.,Fiscus,S.A., Chilongozi,D.A.,Namakhwa,D.,Price,M.A.,Galvin,S.R.,Hoffman,I.F.,Cohen, M.S.,2007.ImproveddetectionofacuteHIV-1infectioninsub-SaharanAfrica: developmentofariskscorealgorithm.AIDS21,2237–2242.
Powers,K.A.,Poole,C.,Pettifor,A.E.,Cohen,M.S.,2008.Rethinkingthe heterosexualinfectivityofHIV-1:asystematicreviewandmeta-analysis. LancetInfect.Dis.8,553–563.
Quinn,T.,Wawer,M.J.,Sewankambo,N.,Serwadda,D.,Li,C.,Wabwire-Mangen,F., Meehan,M.,Lutalo,T.,Gray,R.,FortheRakaiprojectstudygroup,2000.Viral loadandheterosexualtransmissionofhumanimmunodeficiencyvirustype1. RakaiProjectStudyGroup.N.Engl.J.Med.342,921–929.
Reniers,G.,Armbruster,B.,Lucas,A.,2015.Sexualnetworks,partnershipmixing, andthefemale-to-maleratioofHIVinfectionsingeneralizedepidemics:an agent-basedsimulationstudy.Demogr.Res.33,425–450.
Reniers,G.,Watkins,S.,2010.PolygynyandthespreadofHIVinsub-Saharan Africa:acaseofbenignconcurrency.AIDS24,299–307.
Sawers,L.,Stillwaggon,E.,2010.Concurrentsexualpartnershipsdonotexplainthe HIVepidemicsinAfrica:asystematicreviewoftheevidence.J.Int.AIDSSoc. 13,34.
UNAIDS,2013.(JointUnitedNationsProgrammeonHIV/AIDS)GlobalReport: UNAIDSReportontheGlobalAIDSEpidemic,Available:http://www.unaids. org/sites/default/files/mediaasset/UNAIDSGlobalReport2013en1.pdf. Volz,E.M.,Meyers,L.A.,2007.Susceptible-infected-recoveredepidemicsin