Association Between Knee Extension Rate of Torque Development and
Physical Function in a Group of Older Adults with Knee Osteoarthritis
Brian Gaynor
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for graduation with honors in the
Department of Exercise and Sport Science.
Chapel Hill 2016
Approved by:
__________________________________________ Brian Pietrosimone, Thesis Advisor
__________________________________________ Eric Ryan, Reader
Abstract
Brian Gaynor: Association Between Knee Extension Rate of Torque
Development and Physical Function in a Group of Older Adults with
Knee Osteoarthritis
(Under the direction of Brian Pietrosimone)
Purpose. The purpose of this study is to investigate the relationship between knee extension rate of torque development and physical function among individuals with knee osteoarthritis.
Methods. Twenty participants (11 female, 9 male, mean age = 63.15 ± 5.613 years) with knee osteoarthritis were enrolled in this study. For each participant knee extension rate of torque development was obtained for three time intervals (0-50 ms, 0-100 ms, and 100-200 ms after the onset of contraction) during a maximal voluntary isometric contraction. Self-reported physical function was measured using the WOMAC function index and the SF-12 assessment. Physical function was also measured using three clinical tests of function: 20-meter walk, 30-second chair stand test, and a stair-climb test.
Results. A Spearman Rho test showed that there was a significant moderate negative association between knee extension rate of torque development during all three time intervals and times from the 20-meter walk test. Rate of torque
development during the first 100 ms of contraction was significantly associated with stair-climb times, displaying a moderate negative correlation. Rate of torque development was not significantly associated with self-reported physical function or scores from the 30-second chair stand test.
TABLE OF CONTENTS
CHAPTER 1: INTRODUCTION... 4
Purpose Statements... 6
Research Hypotheses... 6
Variables... 6
Operational Definitions... 7
Limitations... 7
Assumptions... 7
List of Abbreviations... 8
CHAPTER 2: REVIEW OF LITERATURE... 9
Knee Osteoarthritis Overview and Societal Burden...9
Knee Osteoarthritis and Physical Function...11
Knee Osteoarthritis and Quadriceps Dysfunction...12
CHAPTER 3: EXPERIMENTAL PROCEDURES...18
Procedures... 18
Participants... 19
Outcome Measures... 20
Statistical Analysis... 23
CHAPTER 4: RESULTS... 25
Tables and Charts... 27
CHAPTER 5: DISCUSSION... 34
CHAPTER 6: Conclusion... 38
Chapter 1
Introduction
Osteoarthritis (OA) is a degenerative joint disease that causes pain and stiffness in the affected joint, leading to progressive joint failure and disability.1
Knee OA is prevalent globally and in the United States2-4, with a prevalence of
around 5% among U.S. adults over the age of 26.5 Osteoarthritis, including knee OA,
causes a large portion of the global disability burden, measured by the metrics YLDs (years lived with disability) and DALYs (daily adjusted life years).2,3,6 Disability
caused by OA incurs a significant economic cost on society, both in the U.S. and globally.4,7 The global economic and disability burden of OA has increased by as
much as 50% in the past twenty years and is expected to continue increasing in the future as the global population ages.3,6
Individuals with knee OA display decreased physical function, measured by self-report questionnaires8,9 and clinical tests of function10-13. The WOMAC Index is a
self-report questionnaire specific to individuals with arthritis that quantifies an individual’s pain, stiffness, and function due to their arthritis.14 The SF-12
questionnaire is the abridged version of the Short-Form Health Survey (SF-36) that assesses self-reported health-related quality of life, including physical function and ability.15 The Osteoarthritis Research Society International (OARSI) recommends the
use of five performance-based measures of physical function for individuals with knee OA: a 30-second chair stand, 20-meter fast-paced walk, stair climb, timed-up-and-go, and 6-minute walk test.16
Individuals with knee OA display altered quadriceps muscle function,
including significant deficits in strength11,17-20 and voluntary activation21. Quadriceps
muscle function is an important predictor of physical function among individuals with knee OA; stronger quadriceps musculature is associated with improved physical function.11,22,23 Among individuals with knee OA, deficits in voluntary
quadriceps activation influence deficits in quadriceps strength24, contributing to
Rate of torque development (RTD) reflects the rate of rise of the torque curve generated by a muscle contraction, and it quantifies a particular muscle’s ability to produce force in a short period of time.25 Individuals with knee OA display lower
rates of knee extension torque development than healthy controls.26,27 One study
reported that knee extension rate of torque development was associated with physical function in a group of individuals receiving total knee arthroplasty (TKA) for their knee OA.27 However, the association between quadriceps rate of torque
development and physical function has not yet been thoroughly investigated in the broader population of individuals with knee OA. Among patients with hip OA, higher rates of knee extension torque development are associated with increased physical function, even after correcting for quadriceps strength.28 It is worth
investigating whether individuals with knee OA display a similar association
between knee extension rate of torque development and physical function as those with hip OA.
If greater rates of knee extension torque development are associated with higher levels of physical function in individuals with knee OA, clinical interventions to increase quadriceps rate of torque development may be implemented to improve physical function in this population. Traditional isokinetic strength training has been shown to increase knee extension rate of torque development29, and the effect
of other interventions such as cryotherapy30 and vibration therapy31 on knee
extension rate of torque development is currently being investigated.
Understanding the association between knee extension rate of torque development and physical function in individuals with knee OA would allow clinicians to
determine whether individuals would benefit from an increase in knee extension rate of torque development.
Purpose Statement
Determine the associations between knee extension rate of torque development and physical function, measured with the WOMAC function index, SF-12 questionnaire, 30-second chair-stand test, 20-meter fast-paced walk test, and a stair climb test, in a group of older adults with knee OA.
Research Hypotheses
Higher knee extension rates of torque development will be associated with higher levels of physical function among this group of older adults with knee OA. Knee extension rate of torque development will be positively associated with scores from the SF-12 questionnaire and the 30-second chair stand, and it will be negatively associated with WOMAC Index scores, 20-meter walk times, and stair climb test times. Therefore, individuals with higher rates of knee extension torque
development will self-report and display better physical function than individuals with lower rates of knee extension torque development.
Variables
Measures of Physical Function – Dependent Variables
o Self-Report Scores
WOMAC Function Index
SF-12 Questionnaire
o Performance in Clinical Tests of Function
30-second chair stand test score
20-meter fast-paced walk time
Stair climb test time
Operational Definitions
Knee Extension Rate of Torque Development: The peak slope of the torque curve generated by a maximal isometric knee extension contraction.
Maximal Voluntary Isometric Contraction: The maximal torque generated during a maximal isometric knee extension contraction.
Central Activation Ratio: The percentage of torque that can be generated voluntarily during a maximal isometric knee extension contraction with a superimposed
stimulus that maximizes the quadriceps contracting potential.
Limitations
1. The association between knee extension rate of torque development and physical function only applies to individuals with knee OA who match our inclusion criteria. The participants included in this study may not represent individuals with a central activation ratio greater than 90% or individuals who display less disability on the WOMAC function index.
2. This study employs a cross-sectional descriptive experimental design. Therefore, any association found between knee extension rate of torque development and physical function does not imply that rate of torque development directly affects physical function.
Assumptions
1. All measures are reliable and valid.
List of Abbreviations
OA- Osteoarthritis
RTD- Rate of Torque Development
MVIC- Maximal Voluntary Isometric Contraction
CAR- Central Activation Ratio
YLD- Years Lived with Disability
DALY- Daily Adjusted Life Years
TKA- Total Knee Arthroplasty
Chapter 2
Review of the Literature
Knee Osteoarthritis Overview and Societal Burden
Definition of Knee Osteoarthritis
Osteoarthritis (OA) has been defined as a “degenerative joint disease
involving the cartilage and … surrounding tissues”.1 OA often results in osteophyte,
or bone spur, formation on the ends of the articulating bones, as well as muscle weakening and ligament laxity surrounding the affected joint.1 OA can cause joint
pain and stiffness, and it generally progresses slowly to cause joint failure and disability.1 Studies8,9 comparing patients with knee OA to healthy controls display
that individuals with knee OA score lower on measures of quality of life, including the SF-36 questionnaire. The WOMAC Index is often used as a measure of disability among people with OA.8,9,14 Because the WOMAC Index is specific to individuals with
OA, it does not allow for comparison between symptomatic individuals and healthy controls.
Prevalence ofOsteoarthritis
OA is a prevalent disease. In 2005, approximately 26 million people in the United States had OA in at least one joint.1 The global prevalence of knee OA
specifically is reported at 3.8%, with a higher prevalence among females than males.2-4 The prevalence of knee OA among U.S. adults over the age of 26 was
reported at 4.9%.5 Across the board, the prevalence of knee OA has been
demonstrated to increase with age, especially after the age of 50.1,3,5 Obesity is a
strong risk factor for developing knee OA, especially when combined with weak muscular strength.1,5 Although age, weight, and gender are all risk factors for
Disability Burden of Osteoarthritis
Due to its symptoms and prevalence, OA is a significant global cause of disability. In 2010, OA contributed to 10.5% of the global disability burden,
measured in years lived with a disability (YLDs).3 More specifically, hip and knee OA
combined ranked 11th in 2010 among all disorders in contributing to global
disability, causing 17.1 million YLDs.2 The metric DALYs, or disability-adjusted life
years, is another tool used to measure the burden of a disease. DALYs are calculated by summing years of life lost (YLLs) with years lived with disability (YLDs).6 In
2010, musculoskeletal disorders accounted for 6.8% of the total DALYs globally for all diseases and injuries, of which OA made up 10%.6 In higher-income developed
countries, the disability burden from musculoskeletal disorders accounts for a higher percentage of total DALYs, whereas the disability burden from
musculoskeletal disorders is smaller relative to other diseases in developing countries.6
Economic Burden of Osteoarthritis
Every year, OA incurs a significant economic burden on individuals as well as on society as a whole. The authors of a 1997 study reported the average annual non-medical costs for an individual in the U.S. with OA at $726, a figure that has not been adjusted for inflation since 1997.7 In an Austrian study, the authors estimated
the direct costs for an individual patient with hip and knee OA at 2,747 Euros over a 12-month span.3 On a national scale, OA has been estimated to cost over $60 billion
per year in the U.S.4 In 2009, OA was the primary reason for 95% of
Medicare-funded hip and knee replacements in the U.S.; knee replacements accounted for $28.5 billion in hospital expenditures that year.5 Among other Western nations, the
annual cost of OA ranges from 1 to 2.5% of each country’s Gross National Product.4,7
An aging global population has led to an increase in the burden of
musculoskeletal disorders, including OA. Between 1990 and 2010, the percent of total global DALYs attributed to musculoskeletal disorders has increased from 4.7% to 6.8%.6 The economic burden caused by musculoskeletal disorders has in turn
increased by almost 50% in the past 20 years, and this burden is only expected to increase.3
Knee Osteoarthritis and Physical Function
Knee Osteoarthritis Decreases Function
Patients with knee OA score lower on self-report measures of physical function, including the SF-36 questionnaire.8,9 In addition to self-report
questionnaires, researchers have used objective clinical tests to measure physical function in patients with knee OA. The sit-to-stand and TUG (timed-up-and-go) tests have been shown to be reliable measures of knee function and functional mobility in individuals with knee OA.33,34 Patients with knee OA display worse
performance in clinical tests measuring physical function compared with healthy controls.10-12 In one such study, patients with knee OA scored between 16-26%
worse in a variety of physical functioning tests (TUG, stair climb, sit-to-stand, and 5-minute walk).11 The authors of another study determined that individuals with
severe knee OA (presence of knee pain along with a score of 4 on the Kellgren– Lawrence grading scale) took longer to perform a 4-times sit-to-stand task compared with healthy controls.13
Patients with knee OA demonstrate altered biomechanics and kinematics during a sit-to-stand task. They use a reduced knee ROM to complete the task35,
display increased forward lean, and significantly favor their unaffected limb more than healthy controls during the task.13,34 Patients with knee OA display altered gait
patterns, including slower gait speed and shorter strides20, as well as reduced
angular velocities at the knee while walking.19 A diagnosis of knee OA increases the
institutionalization, and even mortality”.36 The likelihood of being diagnosed with
frailty increases among patients with bilateral knee OA.36
Determinants of Function in Patients with Knee Osteoarthritis
Additional comorbidities alongside knee OA have been displayed to
exacerbate the observed deficits in physical function in symptomatic populations. Individuals with both hip and knee OA perform worse on measures of physical function than those with only knee OA.12 Patients with knee OA and decreased
quadriceps strength perform worse on measures of physical function than those with stronger quadriceps.11,22,23 Quadriceps strength is associated with higher levels
of physical activity among those with knee OA, meaning that knee OA subjects with stronger quadriceps reported spending more time doing physical activity.37 In a
2007 study, the authors reported that women with knee OA and a history of falls displayed decreased functional mobility, measured with a TUG test, compared to a similar population without a history of falls.38 This suggests that decreased
functional mobility, reliably measured by a TUG test33, may be a predictive factor in
susceptibility to falls among patients with knee OA.
Influence of Radiographic Severity on Function
While many clinicians continue to use radiographic imaging to assess the severity of knee OA, multiple studies suggest that the radiographic severity of knee OA has no association with pain levels or physical function status. The authors of these studies present evidence that a large amount of variation in physical function exists between individuals with knee OA of similar radiographic severity.39,40
Knee Osteoarthritis and Quadriceps Dysfunction
Quadriceps Strength
deficits in patients with knee OA at 19.6% compared with health controls11, and
another group of researchers reported strength deficits of 22-39%.19 Patients with
moderately severe knee OA exhibit weaker quadriceps strength than those with only mild cases of knee OA.17 In one study, subjects with early stages of knee OA
displayed deficits in eccentric quadriceps strength but not in concentric strength.18
The authors suggested that the eccentric strength deficits they observed might be causing altered gait patterns that can contribute to the progression of the disease.18
In patients with end-stage unilateral knee OA, the quadriceps of the affected limb were 20% weaker than those of the contralateral limb.41 Women with knee OA
display greater hamstring-to-quadriceps isokinetic strength ratios than healthy controls, possibly due to quadriceps strength deficits. This altered strength ratio may prevent anterior translation of the tibia in individuals with knee OA.42
Among individuals with knee OA, increased quadriceps strength has been associated with improved physical function, measured by timed walking and TUG tests.11,22 Knee extension strength has also been negatively correlated with the pain,
stiffness, and function subscales of the WOMAC questionnaire, suggesting that stronger quadriceps may reduce physical dysfunction in patients with knee OA.23
Patients with knee OA who reported higher levels of physical activity had
significantly stronger quadriceps than those who reported lower levels of physical activity37 Radiographic severity of knee OA is a poor predictor of quadriceps
strength.39,40 Patients with knee OA additionally display decreased knee ROM
compared with healthy controls, even in their unaffected limb.19
Quadriceps strength can also be a clinical predictor of physical function in older adults without knee OA. In a study attempting to identify differences between older women fallers and non-fallers, knee extension strength was the strongest predictor of fall risk.43
Quadriceps Activation
without presence of OA as compared to healthy individuals.21 However, in patients
with end-stage unilateral knee OA, voluntary quadriceps activation was 8% lower in the affected limb compared to the contralateral unaffected limb.41 In this sample of
patients with end-stage knee OA, voluntary activation explained the majority of the variance in quadriceps strength in the affected limb, whereas quadriceps cross sectional area explained more of the variance in strength in the unaffected limb.41
This finding suggests that voluntary activation deficits significantly contribute to quadriceps strength deficits in limbs with severe knee OA. It has been shown in patients with knee OA that higher levels of pain are associated with decreased quadriceps activation.44,45
Muscle activation is controlled by the motor cortex in the brain as well as spinal reflex arcs. Inhibition of the quadriceps can come from either pathway, and increasing the excitability of either pathway can lead to increased strength gains in patients with knee OA.46 However, the authors of one study reported that patients
with knee OA and healthy controls had similar resting motor thresholds, suggesting that the observed activation deficits in patients with knee OA may not stem from direct motor cortex inhibition.44
Higher levels of voluntary quadriceps activation is associated with improved physical function in patients with knee OA, and voluntary activation may be
moderating the observed relationship between quadriceps strength and physical function.22 Patients with knee OA display altered activation patterns in the muscles
surrounding the knee joint during normal walking, and these alterations are more pronounced in more severe cases of knee OA.47 Compared with healthy controls, a
group of women with knee OA displayed a greater ratio of vastus medialis/vastus lateralis EMG activity during maximal voluntary contractions. The authors of this study suggested that this altered activation ratio between the vastus medialis and the vastus lateralis may help stabilize the patella and prevent lateral tracking in the injured joint.42 A separate study reported that women with knee OA display
To mimic the effects of knee injury, researchers have tested quadriceps strength and activation in artificially effused knees of healthy subjects. The change in voluntary quadriceps activation predicted 87% of the variance in quadriceps strength in the artificially effused knees.48 In a study following a 4-week therapeutic
intervention in patients with knee OA, the researchers found that 47% of the
variance in quadriceps strength changes were explained by the observed changes in quadriceps activation.24 Interventions that increase quadriceps activation may in
turn increase quadriceps strength in knee OA patients, supporting the use of disinhibitory interventions to improve strength and function in this population.
Rate of Torque Development
Rate of torque development reflects how fast a muscle can produce torque in a joint at the onset of a muscle contraction.25 Maximal rate of torque development
can be reached via electrical stimulation of a muscle, and voluntary rate of torque development is only a percentage of this maximal rate.25 Knee extension rate of
torque development has been shown to decrease with age.43 In patients with hip OA,
quadriceps rate of torque development was associated with various measures of physical function, including self-report questionnaires and a stair-climb test. This relationship between rate of torque development and physical function remained significant even after correcting for quadriceps strength (peak torque). However, rate of torque development had weaker associations with physical function in individuals with stronger quadriceps.28
Individuals with knee OA display reduced rates of knee extension torque development compared with healthy age-matched controls.26 In a study comparing
In elderly adults, increased rate of force development in hip abductors is associated with higher levels of mediolateral stability during voluntary balance activities.49 However, the authors of one study reported that rate of torque
development in knee extensors was not significantly different between elderly female fallers and non-fallers, and knee extension peak torque was more significant in differentiating between fallers and non-fallers than rate of torque development.43
Leg power, defined as the amount of work per unit time, strongly correlates with self-reported physical function in elderly women.50 Rate of torque development may
affect leg power by altering the amount of time in which a specific force can be produced. Therefore, higher rates of torque development should yield greater leg power.
Interventions to Improve Quadriceps Function
Various therapeutic modalities have been tested for their efficacy in
improving physical function, balance, and quadriceps function in patients with knee OA. A review of the literature determined that therapeutic exercises, including but not limited to aerobic exercise, strength training, and water exercise, are effective at improving balance in women with knee OA.51 Whole-body vibration (WBV) has been
shown to significantly reduce pain and improve function in patients with knee OA, but its effect on stiffness in this population is insignificant.52
It is important to address the underlying quadriceps neuromuscular deficits in patients with knee OA in order to maximize strength gains, but any intervention aimed at reducing quadriceps inhibition should be implemented alongside
traditional therapeutic exercises.46 There are various interventions that work to
increase quadriceps activation in injured populations, with varying efficacy.
Transcutaneous electrical nerve stimulation (TENS) has been shown to be effective at improving quadriceps activation in patients with knee OA, but there lacks
research on the optimal dose to maximize the benefits of TENS therapy.46
increases neuromuscular activation directly after application, but no long-term benefits have been observed.46 Vibration techniques have been shown to be effective
at acutely improving quadriceps function.46
There has been research on improving rate of torque development through various interventions, with mixed success. A water-based exercise program resulted in similar strength gains compared to a traditional resistance-training program in older women over the age of 60. Both training programs elicited increases in strength but had no effect on rate of torque development in knee extensors.53 In young healthy men, acute skin cooling on the thigh was shown to
increase initial rate of torque development in knee extensors, but skin cooling did not increase peak torque or peak rate of torque development.30 The effect of skin
cooling was only studied acutely, meaning that the study did not look at the long-term impact of skin cooling on rate of torque development. Vibration therapy was shown to significantly increase knee extension peak torque in young adults, but it had no effect on rate of torque development.31 Explosive strength training has been
Chapter 3
Experimental Procedures
This study employed a cross-sectional, descriptive laboratory research design and was intended to investigate the association between knee extension rate of torque development and five different measures of physical function in a group of older adults with knee OA. The variables tested were measures of quadriceps function, self-reported physical function, and physical performance in a series of clinical tests of function. Quadriceps function was quantified using knee extension rate of torque development. Self-reported function was measured using the WOMAC function index and SF-12 questionnaire. Physical function was also measured using three clinical tests of function: a 30-second chair-stand test, a 20-meter fast-paced walk test, and a timed stair climb test. The Internal Review Board at the University of North Carolina at Chapel Hill verified all procedures used in this study.
Procedures
Participants were first given informed consent forms to read and sign. After giving informed consent, participants filled out inclusion/exclusion criteria forms as well as self-reported forms to assess physical function. These forms consisted of the WOMAC Function Index and the SF-12 Questionnaire. After completing the self-report forms, participants had their height and weight measured. Participants then proceeded to undergo a burst superimposition test to determine the level of
voluntary quadriceps activation in their involved limb. The results from this test were also used to derive knee extension rate of torque development. Upon completion of this test, participants performed three separate clinical tests of
physical function: a 30-second chair-stand test, a 20-meter fast-paced walk test, and a timed stair-climb test. These three clinical tests have been shown to be reliable and valid measures of physical function for patients with hip and knee OA55 and are
Participants
Participants were recruited from clinics around the greater Chapel Hill area. Participants were included if they had ever received a clinical diagnosis of knee OA and had a knee x-ray taken within the last 6 months. Once recruited, participants filled out a knee injury history form. If participants responded “yes” to any of the exclusion criteria, they were withheld from this study. Participants were excluded from this study if they had received an injection in their knee in the past two weeks or had a previous knee arthroplasty, or joint replacement. Other exclusion criteria included having a pacemaker, neurodegenerative condition, rheumatoid arthritis, recent lower extremity orthopedic surgery or injury, or any cardiovascular
condition restricting the participant from exercise. Participants were also excluded from this study if they were unable to walk without a cane or other assistive device, as the outcome measures of physical function required participants to walk without assistance. Participants then filled out the WOMAC function Index. Only
participants scoring greater than 20 on the WOMAC function index were included, and participants scoring less than or equal to 20 were excluded from this study. This ensured that all included participants self-reported at least a moderate amount of physical disability due to their arthritis, with a WOMAC score of 21 as the
minimum level of disability required for inclusion. The final exclusion criterion was a central activation ratio (CAR) over 90%. Only participants with a CAR less than 90% were included, ensuring that all included participants displayed at least 10% voluntary quadriceps inhibition. It may be important to investigate knee extension rate of torque development in this subset of individuals with knee OA that display quadriceps dysfunction, as defined by a CAR less than 90%. Participants gave informed consent and were free to drop out of the study at any time.
We estimated that 19 participants would be needed to identify a significant moderate correlation (d=0.6) in this cross-sectional study with an alpha level of 0.05 and a 1- of 0.8. We predicted a significant moderate correlation between knee β
function, including both self-reported assessments and clinical tests of function, due to the previously reported moderate correlation between knee extension strength and physical function.11,22,23 We elected to recruit and evaluate outcomes in 20
participants in case a participant was found to be an outlier during analysis.
Outcome Measures
Rate of Torque Development
Participants were seated in the Humac dynamometer located in the Sports Medicine Lab at the University of North Carolina at Chapel Hill. They were
positioned at 85° of hip flexion and 70° of knee flexion, as some individuals with knee OA may be unable to achieve 90° of knee flexion. Restrictive straps were secured over the shoulders and hips in order to limit excessive movement during testing. The distal tibia of the participant’s involved limb was fastened to the arm of the dynamometer with a Velcro strap. For participants with bilateral knee OA, participants were asked which knee was more symptomatic, and the knee with more severe symptoms was used for testing. Participants were taken through a series of warm-up isometric knee extension contractions, first at 25% and then at 50% of their maximal exertion. After participants were taken through the series of warm-ups, they were asked to extend their knee into the dynamometer with as much force and as quickly as possible. These instructions are recommended in order to obtain valid MVIC and rate of force development data.56 Participants
crossed their arms over their chest to minimize the use of muscles besides the quadriceps. Researchers counted down from three and then encouraged the participants to kick as hard as possible. This maximal voluntary isometric
contraction (MVIC) procedure was repeated at least three times to determine each participant’s average MVIC. Participants then completed two maximal isometric contractions with a superimposed stimulus delivered to the quadriceps musculature via electrodes once the participant reached his or her average MVIC. This
which was then used to calculate each participant’s central activation ratio (CAR). CAR was calculated by dividing the participant’s MVIC by the peak torque elicited from the superimposed stimulus. The torque curves generated by these two maximal contractions with a superimposed stimulus were used to derive knee extension rate of torque development.
This procedure yielded a torque curve representing the torque produced by the participant’s maximal quadriceps contraction over time. Rate of torque
development refers to the rate of rise of this torque curve. In this study, we
calculated the peak rate of torque development during three distinct time intervals for each MVIC trial. These three intervals all measure rate of torque development during the initial stages of contraction, defined as the first 300 ms after the onset of contraction.56 We hypothesize that these measures of rate of torque development
may be an important indicator of physical function, as previous research recommends the use of rate of force development during the initial stages of contraction56. We calculated peak rate of torque development during three unique
time periods following the onset of contraction, previously defined as 2% of the participant’s MVIC for that trial.26,56 The time periods used were 0-50 ms, 0-100 ms,
and 100-200 ms. We took the peak rate of torque development during each time interval and then divided each of those three RTD values by the peak torque from that MVIC trial in order to correct for the relative strength of each participant. Previous research26 suggests that knee extension rate of torque development is
proportional to the strength of the individual, and dividing by peak torque corrects for this underlying variable. Each participant performed two maximal contractions, and we used the greater of the two rates of torque development during each time interval. The resulting three values were used as the measures of RTD that will reflect the quadriceps function of each participant in this study.
Self-Reported Function
(WOMAC) and the Short-Form 12 Questionnaire (SF-12). An investigator watched the participants fill out the self-report forms and explained each section as needed. The WOMAC Index consists of a pain, stiffness, and function subsection. Only the function subsection was used to measure self-reported physical function. The function subsection of the WOMAC consists of 17 questions; each question asks about a participant’s self-reported degree of difficulty during a specific activity. The answer choices are none, mild, moderate, severe, and extreme, and the answers correspond to a number from 0-4. The numbers are then added up to determine each participants WOMAC function score on a scale of 0-68. Only participants scoring 21 or above on the WOMAC function index were included.
The SF-12 Questionnaire was used to quantify each participant’s self-reported health-related quality of life. It consists of 12 questions asking about the participant’s general health and how a participant’s physical and emotional health affects his or her daily functioning, including a participant’s ability to climb stairs and perform physical activity of moderate intensity. The SF-12 was scored using a program that generates a score from 0-100, with 100 reflecting the highest quality of life and 0 reflecting the lowest self-reported quality of life.
Physical Performance Tests
20-meter Fast-paced Walk Test:
30-second Chair-stand Test:
The participants started seated on a 47 cm tall chair. The participant were instructed to stand up from the chair and then sit back down as many times in 30 seconds as possible, with the participant’s arms crossed over his or her chest. The timed test started as soon as the participant lifted off the chair for the first time. The investigators counted the number of stands completed in 30 seconds, and this score was recorded for each trial. This procedure was repeated three times, and
we then selected the highest score from the three trials to use as an outcome measure for each participant.
Timed Stair Climb Test
The participants started at the bottom of a 190 cm tall flight of stairs. Each stair was 19 cm tall, and there were 10 stairs in the entire flight. The participants were instructed to climb the flight of stairs, turn around at the top, and then descend the stairs as quickly as possible. The participants were instructed to touch every individual stair on the way up and down and to avoid using the handrail. However, touching the handrail for balance as needed was accepted and would not disqualify a trial. The investigators started the stopwatch as soon as the participant initiated his or her first step, and then the stopwatch was stopped when the participant reached the bottom of the flight of stairs. The time taken to complete this task was recorded as the score for the test, and the test was repeated three times for each participant. We selected the lowest time recorded from the three trials to use as an outcome measure for each participant.
Statistical Analysis
performed a Shapiro-Wilkes Test on each of the outcome measures to test each data set for normality. If all of the data sets were normal, we then used Pearson Product Moment tests to test the association between the outcome measures. We tested two-tailed bivariate associations between peak rate of torque development and all of the other outcome measures of physical function independently. If a data set was not normally distributed, we used a Spearman Rho test for every association
Chapter 4
Results
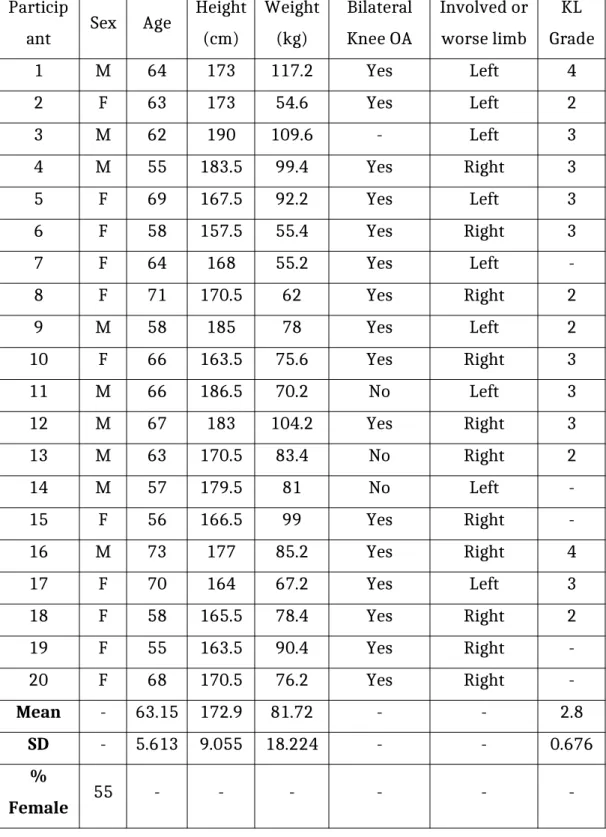
Thirty participants were recruited and screened for inclusion in this study. Nine participants were excluded because they exhibited a CAR over 90%, and one participant was excluded for having previously received a hip replacement. Twenty participants (9 males, 11 females) met the inclusion criteria during the screening session and were included in this study. Demographic data is presented in Table 1. The participants’ mean age was 63.15 ± 5.613 years, which reflects the population of individuals with knee OA as the prevalence of the disease increases after the age of 501. Their involved limbs received an average KL grade of 2.8 ± 0.676, indicating
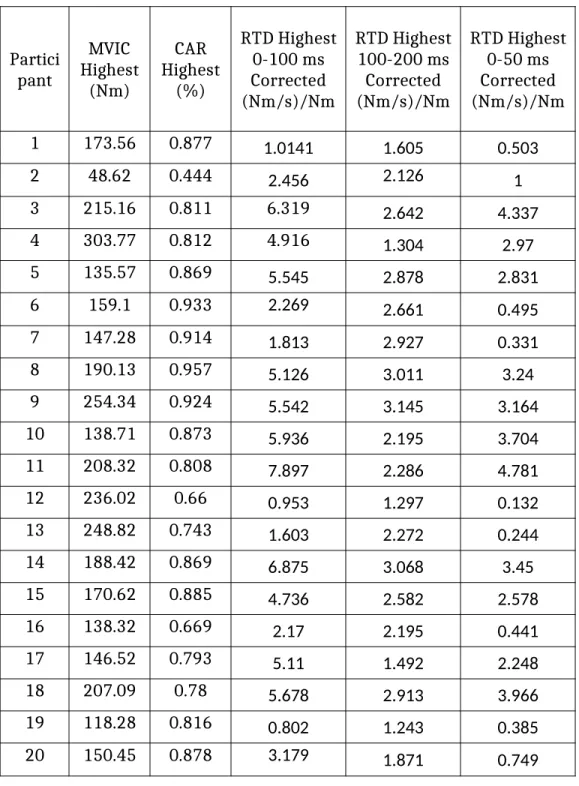
moderately severe radiographic knee OA57. Strength, activation, and raw rate of
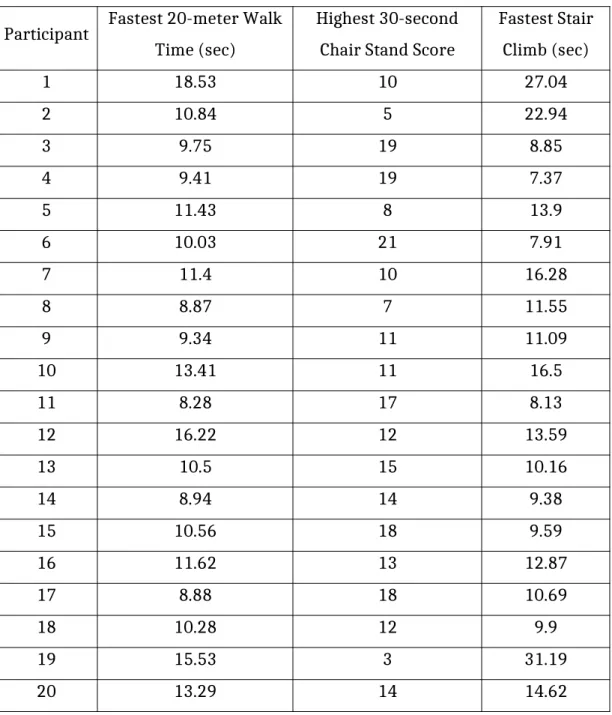
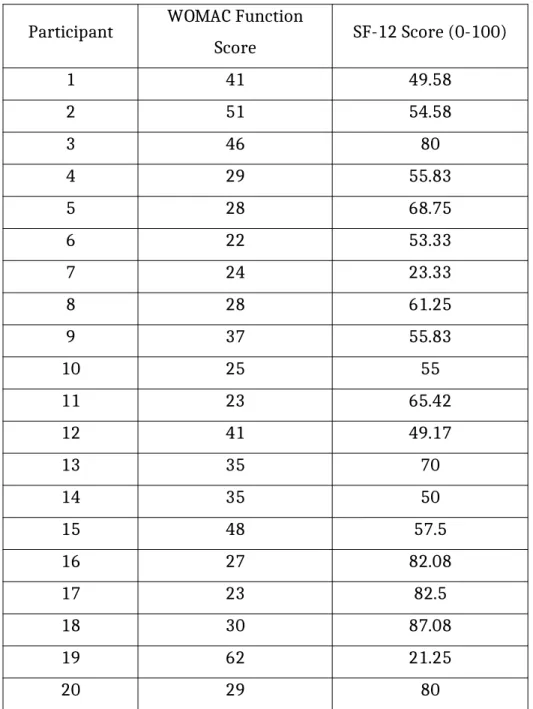
torque development data are presented in Table 2. The outcomes from the physical function tests and self-reported assessments are presented in Tables 3 and 4,
respectively.
Rate of torque development values during the intervals of 0-100 ms and 100-200 ms were shown to be normally distributed using a Shapiro-Wilkes test for normality. The rate of torque development data during the interval 0-50 ms was not normally distributed. The 30-second stair climb scores were normally distributed, but the times from the two other physical function tests (20-meter walk and stair climb) were found to be non-normally distributed. Scores from both the WOMAC function test and SF-12 assessment were normally distributed.
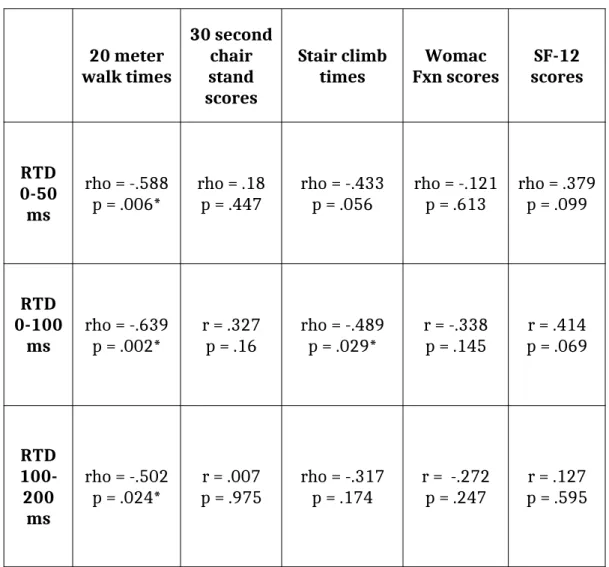
The associations between the main outcome measures (RTD values and measures of physical function) are presented in Table 5, and graphs of the
significant correlations are presented. Significant moderate negative correlations were found between all three measures of knee extension rate of torque
during three separate time intervals, walked 20 meters faster than those with lower knee extension rates of torque development.
Additionally, rate of torque development during the first 100 ms after the onset of contraction was moderately associated with stair climb times (rho= -.489, p= .029). This significant negative correlation means that participants with higher rates of torque development during the first 100 ms of contraction were able to ascend and descend stairs faster. Although associations between rates of torque development during the other two time intervals and stair climb times were not significant, they both displayed moderate negative correlations: RTD 0-50 ms (rho= -.433, p=.056) and RTD 100-200 ms (rho=-.317, p=.174).
Table 1. Demographics Particip
ant Sex Age
Height (cm)
Weight (kg)
Bilateral Knee OA
Involved or worse limb
KL Grade
1 M 64 173 117.2 Yes Left 4
2 F 63 173 54.6 Yes Left 2
3 M 62 190 109.6 - Left 3
4 M 55 183.5 99.4 Yes Right 3
5 F 69 167.5 92.2 Yes Left 3
6 F 58 157.5 55.4 Yes Right 3
7 F 64 168 55.2 Yes Left
-8 F 71 170.5 62 Yes Right 2
9 M 58 185 78 Yes Left 2
10 F 66 163.5 75.6 Yes Right 3
11 M 66 186.5 70.2 No Left 3
12 M 67 183 104.2 Yes Right 3
13 M 63 170.5 83.4 No Right 2
14 M 57 179.5 81 No Left
-15 F 56 166.5 99 Yes Right
-16 M 73 177 85.2 Yes Right 4
17 F 70 164 67.2 Yes Left 3
18 F 58 165.5 78.4 Yes Right 2
19 F 55 163.5 90.4 Yes Right
-20 F 68 170.5 76.2 Yes Right
-Mean - 63.15 172.9 81.72 - - 2.8
SD - 5.613 9.055 18.224 - - 0.676
%
-Table 2. Strength, Activation, and Rates of Torque Development Partici pant MVIC Highest (Nm) CAR Highest (%) RTD Highest 0-100 ms Corrected (Nm/s)/Nm RTD Highest 100-200 ms Corrected (Nm/s)/Nm RTD Highest 0-50 ms Corrected (Nm/s)/Nm
1 173.56 0.877 1.0141 1.605 0.503
2 48.62 0.444 2.456 2.126 1
3 215.16 0.811 6.319 2.642 4.337
4 303.77 0.812 4.916 1.304 2.97
5 135.57 0.869 5.545 2.878 2.831
6 159.1 0.933 2.269 2.661 0.495
7 147.28 0.914 1.813 2.927 0.331
8 190.13 0.957 5.126 3.011 3.24
9 254.34 0.924 5.542 3.145 3.164
10 138.71 0.873 5.936 2.195 3.704
11 208.32 0.808 7.897 2.286 4.781
12 236.02 0.66 0.953 1.297 0.132
13 248.82 0.743 1.603 2.272 0.244
14 188.42 0.869 6.875 3.068 3.45
15 170.62 0.885 4.736 2.582 2.578
16 138.32 0.669 2.17 2.195 0.441
17 146.52 0.793 5.11 1.492 2.248
18 207.09 0.78 5.678 2.913 3.966
19 118.28 0.816 0.802 1.243 0.385
20 150.45 0.878 3.179 1.871 0.749
MVIC = Maximal voluntary isometric contraction CAR = Central activation ratio
Table 3. Physical Function Tests
Participant Fastest 20-meter Walk Time (sec)
Highest 30-second Chair Stand Score
Fastest Stair Climb (sec)
1 18.53 10 27.04
2 10.84 5 22.94
3 9.75 19 8.85
4 9.41 19 7.37
5 11.43 8 13.9
6 10.03 21 7.91
7 11.4 10 16.28
8 8.87 7 11.55
9 9.34 11 11.09
10 13.41 11 16.5
11 8.28 17 8.13
12 16.22 12 13.59
13 10.5 15 10.16
14 8.94 14 9.38
15 10.56 18 9.59
16 11.62 13 12.87
17 8.88 18 10.69
18 10.28 12 9.9
19 15.53 3 31.19
Table 4. Self-Reported Physical Function
Participant WOMAC Function
Score SF-12 Score (0-100)
1 41 49.58
2 51 54.58
3 46 80
4 29 55.83
5 28 68.75
6 22 53.33
7 24 23.33
8 28 61.25
9 37 55.83
10 25 55
11 23 65.42
12 41 49.17
13 35 70
14 35 50
15 48 57.5
16 27 82.08
17 23 82.5
18 30 87.08
19 62 21.25
20 29 80
Table 5. Associations between RTD and Measures of Physical Function
20 meter walk times
30 second chair stand scores
Stair climb
times Fxn scoresWomac scoresSF-12
RTD 0-50 ms
rho = -.588
p = .006* rho = .18p = .447 rho = -.433p = .056 rho = -.121p = .613 rho = .379p = .099
RTD 0-100
ms rho = -.639p = .002* r = .327p = .16 rho = -.489p = .029* r = -.338p = .145 p = .069r = .414
RTD 100-200
ms
rho = -.502
p = .024* p = .975r = .007 rho = -.317p = .174 r = -.272p = .247 p = .595r = .127
* denotes statistical significance
0 1 2 3 4 5 6 7 8 9 0 2 4 6 8 10 12 14 16 18 20
Knee Extension RTD (0-100 ms) and
20-Meter Walk Times
Peak Knee Extension RTD from 0-100 ms - Corrected for MVIC ((Nm/s)/Nm)
2 0 -M et er W al k T im es ( se co n d s)
1 1.5 2 2.5 3 3.5
0 2 4 6 8 10 12 14 16 18 20
Knee Extension RTD (100-200 ms) and
20-Meter Walk Times
Peak Knee Extension RTD from 100-200 ms - Corrected for MVIC ((Nm/s)/Nm)
0 1 2 3 4 5 6 0 2 4 6 8 10 12 14 16 18 20
Knee Extension RTD (0-50 ms) and
20-Meter Walk Times
Peak Knee Extension RTD from 0-50 ms - Corrected for MVIC ((Nm/s)/Nm)
2 0 -M et er W al k T im es ( se co n d s)
0 1 2 3 4 5 6 7 8 9
0 5 10 15 20 25 30 35
Knee Extension RTD 0-100 ms and Stair
Climb Times
Peak Knee Extension RTD 0-100 ms - Corrected for MVIC ((Nm/s)/Nm)
Chapter 5
Discussion
Main Findings
The main objective of this study was to determine the association between knee extension rate of torque development and physical function among individuals with knee OA. Knee extension rate of torque development was not associated with scores from the self-reported measures of function but was significantly associated with scores from the clinical tests of function. Individuals who displayed greater rates of torque development were able to complete the 20-meter walk test faster than individuals with lower rates of torque development. While knee extension rate of torque development during all three time intervals measured was significantly associated with 20-meter walk times, only rate of torque development measured during the first 100 ms of muscle contraction was significantly associated with scores from the stair climb test. Knee extension rate of torque development displayed a moderate negative correlation with both the 20-meter walk and stair climb test. Rate of torque development was not associated with scores from the 30-second chair stand test.
Importance of Association Between RTD and Walking Speed
Previous research58,59 suggests that walking speed is an important predictor
of various measures of health in an aging population. A decline in walking speed among older adults is associated with increased disability58, and older adults with
slower walking speeds face an increased mortality risk.59 Walking speed is a
significant concern for individuals with knee OA, as individuals with knee OA walk slower than their healthy counterparts.60 Individuals with knee OA are also at
greater risk of experiencing a rapid decline in walking speed.61
speeds than peak torque or voluntary activation. Neither peak torque (rho=-.430, p=0.058) nor central activation ratio (rho=-.125, p=0.6) were significantly
associated with 20-meter walk times. Since only rate of torque development was significantly associated with 20-meter walk times, rate of torque development may be a more sensitive indicator of slow walking pace than quadriceps strength or activation. While previous research has indicated that quadriceps strength11,23 or
activation22 play a role in the decreased physical function of individuals with knee
OA, this study indicates that knee extension rate of torque development is also significantly related to physical function, especially fast-paced walking speed. Based on these findings, low knee extension rates of torque development may be a
potential mechanism to explain slow walking speeds among individuals with knee OA.
Non-Significant Associations
Knee extension rate of torque development was not significantly associated with scores from the 30-second chair stand test, WOMAC function assessment, and SF-12. Previous research27 linking knee extension RTD with physical function
among individuals receiving knee arthroplasty also found significant associations between RTD and speed in walking and stair climbing tests, but this study did not use a chair-stand test as an outcome measure. Our findings suggest that knee extension rate of torque development may be more associated with performance in walking and stair climb tests than a chair-stand test among individuals with knee OA. While a 30-second chair stand test has been previously used as a measure of muscle endurance62, rate of torque development is generally linked with muscle
power and performance in short-duration powerful activities25. This may explain
why knee extension rate of torque development was not significantly associated with scores from the 30-second chair stand in this study.
A previous study28 found that individuals with hip OA with higher quadriceps
perhaps because the sample used was not large enough. Among this sample of twenty individuals with knee OA, greater rates of torque development were correlated with better self-reported function, but the associations were not statistically significant. If an association does exist between rate of torque
development and self-reported physical function, then a larger sample size would have more power in detecting significance than our sample of twenty participants.
Interventions to Increase Rate of Torque Development
If knee extension rate of torque development is significantly associated with faster walking speeds among individuals with knee OA, it may be beneficial to employ interventions aimed at increasing RTD in this population. In a younger population, explosive strength and plyometric training has been shown to increase knee extension rate of torque development63, likely due to neural changes64. An
explosive strength training intervention was also successful at increasing plantar flexion rate of torque in an elderly population54. Future research should investigate
whether a strength training intervention could successfully increase knee extension rate of torque development among individuals with knee OA, with the goal that greater rates of torque development will lead to increased walking speeds and improved physical function. However, this may be difficult to implement in this population due to functional and pain-related limitations among individuals with knee OA. Other interventions, such as whole-body vibration52 and TENS therapy65,
are being investigated for their neuromuscular effects on individuals with knee OA. It is worthwhile to investigate whether these interventions have any impact on rate of torque development in this population.
Limitations and Areas for Further Investigation
This study had two significant limiting factors. Only twenty participants were included. While enough to show significant associations between RTD and measures of function, the number of participants was not enough to generalize these findings to the greater population of all individuals with knee OA. All
quadriceps activation deficits, so these results cannot be generalized to individuals who do not fit this study’s inclusion criteria. Further research should continue investigating the association between knee extension rate of torque development and physical function in a larger, more diverse sample that better represents all individuals with knee OA. The associations that we found that were not significant may be underpowered to detect significance. A larger sample size may provide greater power to detect a significant association between rate of torque
development and measures of physical function in this population, especially self-reported physical function.
Additionally, this study only tested participants at one point in time.
Therefore, we were only able to determine a correlational association between the outcome measures. In order to investigate a causal relationship between knee extension rate of torque development and physical function, a longitudinal study is needed to measure the change in outcome measures over time. Future research should investigate whether changes in knee extension rate of torque development associate with increases in walking speed over time, and whether an intervention that increases rate of torque development could be effective at increasing the walking speed in this population. Future research into this association could affect how clinicians aim to improve physical function in patients with knee OA.
Chapter 6
Conclusion
In a group of individuals with knee OA, greater knee extension rate of torque development associated with faster 20-meter walking pace and lower stair climb times. Knee extension rate of torque development was not significantly associated with 30-second chair stand test scores, and two of the three measures of RTD were not associated with faster stair climb times. There were no significant associations between knee extension RTD and self-reported function, measured with the
WOMAC Function Index and SF-12 assessment.
While knee extension rate of torque development in isolation was not significantly associated with all outcome measures of physical function, the
References:
1. Litwic A, Edwards MH, Dennison EM, Cooper C. Epidemiology and burden of osteoarthritis. Br Med Bull. 2013;105:185-199.
2. Cross M, Smith E, Hoy D, et al. The global burden of hip and knee
osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1323-1330.
3. March L, Smith EU, Hoy DG, et al. Burden of disability due to musculoskeletal (MSK) disorders. Best Pract Res Clin Rheumatol. 2014;28(3):353-366.
4. Buckwalter JA, Saltzman C, Brown T. The impact of osteoarthritis: implications for research. Clin Orthop Relat Res. 2004(427 Suppl):S6-15. 5. Murphy L, Helmick CG. The impact of osteoarthritis in the United States: a
population-health perspective. Am J Nurs. 2012;112(3 Suppl 1):S13-19. 6. Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for
291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197-2223.
7. March LM, Bachmeier CJ. Economics of osteoarthritis: a global perspective. Baillieres Clin Rheumatol. 1997;11(4):817-834.
8. Alkan BM, Fidan F, Tosun A, Ardicoglu O. Quality of life and self-reported disability in patients with knee osteoarthritis. Mod Rheumatol.
2014;24(1):166-171.
9. Guillemin F, Rat AC, Roux CH, et al. The KHOALA cohort of knee and hip osteoarthritis in France. Joint Bone Spine. 2012;79(6):597-603.
10. Kim HS, Yun DH, Yoo SD, et al. Balance control and knee osteoarthritis severity. Ann Rehabil Med. 2011;35(5):701-709.
11. Liikavainio T, Lyytinen T, Tyrvainen E, Sipila S, Arokoski JP. Physical function and properties of quadriceps femoris muscle in men with knee osteoarthritis. Arch Phys Med Rehabil. 2008;89(11):2185-2194.
12. Edwards MH, van der Pas S, Denkinger MD, et al. Relationships between physical performance and knee and hip osteoarthritis: findings from the European Project on Osteoarthritis (EPOSA). Age Ageing. 2014;43(6):806-813.
13. Turcot K, Armand S, Fritschy D, Hoffmeyer P, Suva D. Sit-to-stand alterations in advanced knee osteoarthritis. Gait Posture. 2012;36(1):68-72.
14. Ackerman IN, Tacey MA, Ademi Z, Bohensky MA, Liew D, Brand CA. Using WOMAC Index scores and personal characteristics to estimate Assessment of Quality of Life utility scores in people with hip and knee joint disease. Qual Life Res. 2014;23(8):2365-2374.
15. Shou J, Ren L, Wang H, et al. Reliability and validity of 12-item Short-Form health survey (SF-12) for the health status of Chinese community elderly population in Xujiahui district of Shanghai. Aging Clin Exp Res. 2015. 16. Dobson F, Hinman RS, Roos EM, et al. OARSI recommended
17. Diracoglu D, Baskent A, Yagci I, Ozcakar L, Aydin R. Isokinetic strength measurements in early knee osteoarthritis. Acta Reumatol Port.
2009;34(1):72-77.
18. Serrao PR, Vasilceac FA, Gramani-Say K, et al. Men with early degrees of knee osteoarthritis present functional and morphological impairments of the quadriceps femoris muscle. Am J Phys Med Rehabil. 2015;94(1):70-81. 19. Messier SP, Loeser RF, Hoover JL, Semble EL, Wise CM. Osteoarthritis of the
knee: effects on gait, strength, and flexibility. Arch Phys Med Rehabil. 1992;73(1):29-36.
20. Cheing GL, Hui-Chan CW. The motor dysfunction of patients with knee osteoarthritis in a Chinese population. Arthritis Rheum. 2001;45(1):62-68. 21. Pietrosimone BG, Hertel J, Ingersoll CD, Hart JM, Saliba SA. Voluntary
quadriceps activation deficits in patients with tibiofemoral osteoarthritis: a meta-analysis. PM R. 2011;3(2):153-162; quiz 162.
22. Fitzgerald GK, Piva SR, Irrgang JJ, Bouzubar F, Starz TW. Quadriceps activation failure as a moderator of the relationship between quadriceps strength and physical function in individuals with knee osteoarthritis. Arthritis Rheum. 2004;51(1):40-48.
23. Serrao PR, Gramani-Say K, Lessi GC, Mattiello SM. Knee extensor torque of men with early degrees of osteoarthritis is associated with pain, stiffness and function. Rev Bras Fisioter. 2012;16(4):289-294.
24. Pietrosimone BG, Saliba SA. Changes in voluntary quadriceps activation predict changes in quadriceps strength after therapeutic exercise in patients with knee osteoarthritis. Knee. 2012;19(6):939-943.
25. de Ruiter CJ, Kooistra RD, Paalman MI, de Haan A. Initial phase of maximal voluntary and electrically stimulated knee extension torque development at different knee angles. J Appl Physiol (1985). 2004;97(5):1693-1701.
26. Callahan DM, Tourville TW, Slauterbeck JR, et al. Reduced rate of knee extensor torque development in older adults with knee osteoarthritis is associated with intrinsic muscle contractile deficits. Exp Gerontol. 2015. 27. Winters JD, Christiansen CL, Stevens-Lapsley JE. Preliminary investigation of
rate of torque development deficits following total knee arthroplasty. Knee. 2014;21(2):382-386.
28. Pua YH, Wrigley TV, Collins M, Cowan SM, Bennell KL. Self-report and physical performance measures of physical function in hip osteoarthritis: relationship to isometric quadriceps torque development. Arthritis Rheum. 2009;61(2):201-208.
29. Miller LE, Pierson LM, Nickols-Richardson SM, et al. Knee extensor and flexor torque development with concentric and eccentric isokinetic training. Res Q Exerc Sport. 2006;77(1):58-63.
30. Shimose R, Ushigome N, Tadano C, et al. Increase in rate of force development with skin cooling during isometric knee extension. J Electromyogr Kinesiol. 2014;24(6):895-901.
32. Agaliotis M, Mackey MG, Jan S, Fransen M. Burden of reduced work productivity among people with chronic knee pain: a systematic review. Occup Environ Med. 2014;71(9):651-659.
33. Alghadir A, Anwer S, Brismee JM. The reliability and minimal detectable change of Timed Up and Go test in individuals with grade 1-3 knee osteoarthritis. BMC Musculoskelet Disord. 2015;16:174.
34. Boonstra MC, De Waal Malefijt MC, Verdonschot N. How to quantify knee function after total knee arthroplasty? Knee. 2008;15(5):390-395.
35. Bouchouras G, Patsika G, Hatzitaki V, Kellis E. Kinematics and knee muscle activation during sit-to-stand movement in women with knee osteoarthritis. Clin Biomech (Bristol, Avon). 2015;30(6):599-607.
36. Misra D, Felson DT, Silliman RA, et al. Knee osteoarthritis and frailty: findings from the Multicenter Osteoarthritis Study and Osteoarthritis Initiative. J Gerontol A Biol Sci Med Sci. 2015;70(3):339-344.
37. Pietrosimone B, Thomas AC, Saliba SA, Ingersoll CD. Association between quadriceps strength and self-reported physical activity in people with knee osteoarthritis. Int J Sports Phys Ther. 2014;9(3):320-328.
38. Alencar MA, Arantes PM, Dias JM, Kirkwood RN, Pereira LS, Dias RC. Muscular function and functional mobility of faller and non-faller elderly women with osteoarthritis of the knee. Braz J Med Biol Res. 2007;40(2):277-283.
39. Tuna S, Balci N. The relationship between radiological severity and functional status in patients with knee osteoarthritis. Clin Rheumatol. 2014;33(5):667-670.
40. Barker K, Lamb SE, Toye F, Jackson S, Barrington S. Association between radiographic joint space narrowing, function, pain and muscle power in severe osteoarthritis of the knee. Clin Rehabil. 2004;18(7):793-800.
41. Petterson SC, Barrance P, Buchanan T, Binder-Macleod S, Snyder-Mackler L. Mechanisms underlying quadriceps weakness in knee osteoarthritis. Med Sci Sports Exerc. 2008;40(3):422-427.
42. Patsika G, Kellis E, Kofotolis N, Salonikidis K, Amiridis IG. Synergetic and antagonist muscle strength and activity in women with knee osteoarthritis. J Geriatr Phys Ther. 2014;37(1):17-23.
43. Crozara LF, Morcelli MH, Marques NR, et al. Motor readiness and joint torque production in lower limbs of older women fallers and non-fallers. J
Electromyogr Kinesiol. 2013;23(5):1131-1138.
44. Kittelson AJ, Thomas AC, Kluger BM, Stevens-Lapsley JE. Corticospinal and intracortical excitability of the quadriceps in patients with knee
osteoarthritis. Exp Brain Res. 2014;232(12):3991-3999.
45. Callaghan MJ, Parkes MJ, Hutchinson CE, Felson DT. Factors associated with arthrogenous muscle inhibition in patellofemoral osteoarthritis.
Osteoarthritis Cartilage. 2014;22(6):742-746.
47. Rutherford DJ, Hubley-Kozey CL, Stanish WD. Changes in knee joint muscle activation patterns during walking associated with increased structural severity in knee osteoarthritis. J Electromyogr Kinesiol. 2013;23(3):704-711. 48. Pietrosimone B, Lepley AS, Murray AM, Thomas AC, Bahhur NO, Schwartz TA.
Changes in voluntary quadriceps activation predict changes in muscle strength and gait biomechanics following knee joint effusion. Clin Biomech (Bristol, Avon). 2014;29(8):923-929.
49. Chang SH, Mercer VS, Giuliani CA, Sloane PD. Relationship between hip abductor rate of force development and mediolateral stability in older adults. Arch Phys Med Rehabil. 2005;86(9):1843-1850.
50. Foldvari M, Clark M, Laviolette LC, et al. Association of muscle power with functional status in community-dwelling elderly women. J Gerontol A Biol Sci Med Sci. 2000;55(4):M192-199.
51. Silva A, Serrao PR, Driusso P, Mattiello SM. The effects of therapeutic exercise on the balance of women with knee osteoarthritis: a systematic review. Rev Bras Fisioter. 2012;16(1):1-9.
52. Zafar H, Alghadir A, Anwer S, Al-Eisa E. Therapeutic Effects of Whole-Body Vibration Training in Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Arch Phys Med Rehabil. 2015;96(8):1525-1532.
53. Bento PC, Rodacki AL. Muscle function in aged women in response to a water-based exercises program and progressive resistance training. Geriatr Gerontol Int. 2014.
54. Kobayashi Y, Ueyasu Y, Yamashita Y, Akagi R. Effects of 4 Weeks of Explosive-type Strength Training for the Plantar Flexors on the Rate of Torque
Development and Postural Stability in Elderly Individuals. Int J Sports Med. 2016.
55. Dobson F, Hinman RS, Hall M, Terwee CB, Roos EM, Bennell KL. Measurement properties of performance-based measures to assess physical function in hip and knee osteoarthritis: a systematic review. Osteoarthritis Cartilage.
2012;20(12):1548-1562.
56. Maffiuletti NA, Aagaard P, Blazevich AJ, Folland J, Tillin N, Duchateau J. Rate of force development: physiological and methodological considerations. Eur J Appl Physiol. 2016.
57. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494-502.
58. Artaud F, Singh-Manoux A, Dugravot A, Tzourio C, Elbaz A. Decline in Fast Gait Speed as a Predictor of Disability in Older Adults. J Am Geriatr Soc. 2015;63(6):1129-1136.
59. Tabue-Teguo M, Le Goff M, Avila-Funes JA, et al. Walking and psychomotor speed in the elderly: concordance, correlates and prediction of death. J Nutr Health Aging. 2015;19(4):468-473.
61. White DK, Niu J, Zhang Y. Is symptomatic knee osteoarthritis a risk factor for a trajectory of fast decline in gait speed? Results from a longitudinal cohort study. Arthritis Care Res (Hoboken). 2013;65(2):187-194.
62. Lin PS, Hsieh CC, Cheng HS, Tseng TJ, Su SC. Association between Physical Fitness and Successful Aging in Taiwanese Older Adults. PLoS One.
2016;11(3):e0150389.
63. Thompson BJ, Stock MS, Shields JE, et al. Barbell deadlift training increases the rate of torque development and vertical jump performance in novices. J Strength Cond Res. 2015;29(1):1-10.
64. Behrens M, Mau-Moeller A, Bruhn S. Effect of plyometric training on neural and mechanical properties of the knee extensor muscles. Int J Sports Med. 2014;35(2):101-119.
65. Pietrosimone BG, Saliba SA, Hart JM, Hertel J, Kerrigan DC, Ingersoll CD. Effects of transcutaneous electrical nerve stimulation and therapeutic