Copyright © 2000, American Society for Microbiology. All Rights Reserved.
Evaluation of the Wider System, a New Computer-Assisted
Image-Processing Device for Bacterial Identification and
Susceptibility Testing
RAFAEL CANTO´ N,* MARI´A PE´REZ-VA´ZQUEZ, ANTONIO OLIVER, BEGON˜A SA´NCHEZ DEL SAZ,
M. OLGA GUTIE´RREZ, MANUEL MARTI´NEZ-FERRER,ANDFERNANDO BAQUERO
Servicio de Microbiologı´a, Hospital Ramo´n y Cajal, Madrid 28034, Spain
Received 27 September 1999/Returned for modification 11 November 1999/Accepted 10 January 2000
The Wider system is a newly developed computer-assisted image-processing device for both bacterial identification and antimicrobial susceptibility testing. It has been adapted to be able to read and interpret commercial MicroScan panels. Two hundred forty-four fresh consecutive clinical isolates (138 isolates of the familyEnterobacteriaceae, 25 nonfermentative gram-negative rods [NFGNRs], and 81 gram-positive cocci) were tested. In addition, 100 enterobacterial strains with known-lactam resistance mechanisms (22 strains with chromosomal AmpC-lactamase, 8 strains with chromosomal class A-lactamase, 21 broad-spectrum and IRT-lactamase-producing strains, 41 extended-spectrum-lactamase-producing strains, and 8 permeability mutants) were tested. API galleries and National Committee for Clinical Laboratory Standards (NCCLS) microdilution methods were used as reference methods. The Wider system correctly identified 97.5% of the clinical isolates at the species level. Overall essential agreement (ⴞ1 log2 dilution for 3,719
organism-antimicrobial drug combinations) was 95.6% (isolates of the familyEnterobacteriaceae, 96.6%; NFGNRs, 88.0%; gram-positive cocci, 95.6%). The lowest essential agreement was observed with Enterobacteriaceae versus imipenem (84.0%), NFGNR versus piperacillin (88.0%) and cefepime (88.0%), and gram-positive isolates versus penicillin (80.4%). The category error rate (NCCLS criteria) was 4.2% (2.0% very major errors, 0.6% major errors, and 1.5% minor errors). Essential agreement and interpretive error rates for eight -lactam antibiotics against isolates of the familyEnterobacteriaceaewith known-lactam resistance mechanisms were 94.8 and 5.4%, respectively. Interestingly, the very major error rate was only 0.8%. Minor errors (3.6%) were mainly observed with amoxicillin-clavulanate and cefepime against extended-spectrum-lactamase-producing isolates. The Wider system is a new reliable tool which applies the image-processing technology to the reading of commercial trays for both bacterial identification and susceptibility testing.
Automatic or semiautomatic commercial systems for bacte-rial identification and susceptibility testing were introduced in clinical microbiology laboratories more than 20 years ago (1, 11). These systems are specifically designed to allow reliable bacterial identification by using a number of biochemical tests and MIC determinations that are interpreted according to the susceptibility and resistance criteria established by different committees (7). Most of these systems are highly automated, particularly for MIC determinations and interpretations. The final report should offer an acceptable accuracy and should reproduce the values obtained by reference methods (4, 7, 9). Bacterial identification and susceptibility testing systems vary in the methods that they use to detect bacterial growth and/or to determine endpoints. Either turbidimetric monitor-ing of bacterial growth and fluorometric detection of the flu-orescent indicator or the hydrolysis of fluorogenic substrates is extensively used (7). In contrast, image analysis technology has rarely been applied to these systems and is limited to use with certain devices that analyze inhibition zones obtained by disk susceptibility test methods (3, 10).
The Wider system (Francisco Soria Melguizo, S.A., Madrid, Spain) is a newly developed computer-assisted image-process-ing device. With the assistance of a video camera it recovers a complete image of commercial microdilution panels used for
bacterial identification and susceptibility testing. After image digitization, the Wider system automatically generates the bac-terial name and the susceptibility profile, which depend on the analysis of growth and color changes in the identification wells and the interpretation of growth parameters in the suscepti-bility testing wells, respectively. We report here the results of an evaluation of the newly developed Wider system, which has been adapted to read MicroScan panels (Dade-MicroScan, West Sacramento, Calif.). This work was specifically designed to study the accuracy of this system as a routine tool in clinical microbiology laboratories. Moreover, the susceptibility testing performance of this instrument was also determined with iso-lates of the family Enterobacteriaceae with known resistance mechanisms.
MATERIALS AND METHODS
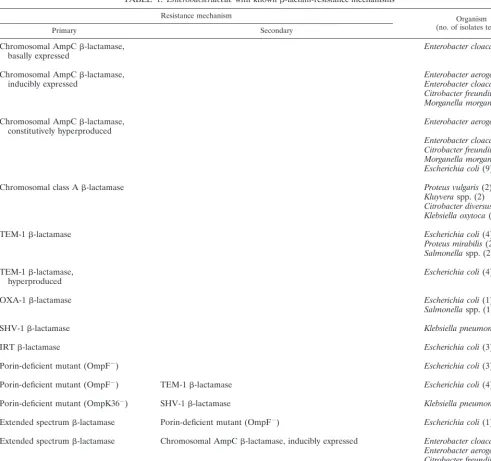
Bacterial isolates.A total of 244 fresh bacterial clinical isolates, prospectively and consecutively collected in our hospital during January and February 1999, were studied. They included 138 isolates of the familyEnterobacteriaceae, 25 nonfermentative gram-negative rods (NFGNRs), 51Staphylococcusspp., 2 Mi-crococcusspp., 22Enterococcusspp., and 6-hemolytic streptococcal isolates. Moreover, 100 clinicalEnterobacteriaceaeisolates with known resistance mech-anisms were also included (Table 1). Prior to identification and susceptibility testing, the organisms were subcultured twice onto 5% sheep blood agar plates.
Wider system.The Wider system is basically composed of a reader module assisted by a data analysis module. The reader module is an illuminated chamber with a digitizing video camera that completely reflects the image of a commercial tray used for bacterial identification and susceptibility testing. The only action required by the operator is manual insertion of the trays into the reader module with the assistance of a special support. The rest of the process is computer controlled. The digitized image is analyzed by the Wider system’s software in the data analysis module. A clear image appears on the computer screen within 5 s. * Corresponding author. Mailing address: Servicio de
Microbiolo-gı´a, Hospital Ramo´n y Cajal, Carretera de Colmenar, Km 9,100, 28034-Madrid, Spain. Phone: 34-91-3368330. Fax: 34-91-3368809. E-mail: [email protected].
1339
on May 15, 2020 by guest
http://jcm.asm.org/
The software automatically detects the type of panel, assigns identification prob-ability scores as a result of the analysis of growth and color changes in the identification wells, and identifies each isolate by comparing the biochemical profile with the profiles in the software database. Moreover, growth parameters in susceptibility testing wells are analyzed in comparison with those in positive and negative control wells. The MIC of each antibiotic is defined as the lowest concentration with the absence of bacterial growth. For categorization purposes, MICs are interpreted by using either the guidelines of the National Committee for Clinical Laboratory Standards (NCCLS) (20) or those from the Spanish Antibiogram Committee (Mesa Espan˜ola para la Normalizacio´n de la Suscep-tibilidad y Resistencia a los Antimicrobianos [MENSURA]) guidelines from the Spanish Antibiogram Committee (2).
Bacterial identification and susceptibility testing with the Wider system.
Wider system 6W and 3W panels containing lyophilized antibiotics and sub-strates were used for bacterial identification and susceptibility testing for gram-negative and gram-positive bacteria, respectively. Dade-MicroScan manufac-tured these panels, which are similar to those used in the overnight WalkAway system (1). Biochemical tests used for both gram-negative and gram-positive organism identification are identical to those included in the WalkAway Mi-croScan panels. Moreover, the biochemical identification database is the same as
that used in the WalkAway system. In addition, Wider 5W panels, which only have antimicrobial agents for susceptibility testing, were also used to assay all isolates. The antibiotics used in the panels (concentration ranges) are as follows: for the Wider panel for gram-negative organisms (reference 6W), amikacin (4 to 16g/ml), amoxicillin (4 to 16g/ml), amoxicillin-clavulanate (4/2 to 32/16
g/ml), cefazolin (2 to 16g/ml), cefotaxime (0.12 to 8g/ml), cefoxitin (4 to 16
g/ml), ceftazidime (0.5 to 16g/ml), ceftazidime-clavulanate (1/4 and 8/4g/ ml), cefuroxime (1 to 16g/ml), ciprofloxacin (0.12 and 1 to 4g/ml), fosfomycin (8 to 32 g/ml), gentamicin (2 to 8g/ml), nalidixic acid (4 and 16g/ml), nitrofurantoin (64g/ml), norfloxacin (1 and 4g/ml), ticarcillin (16 to 64
g/ml), trimethoprim-sulfamethoxazole (2/38 to 4/76g/ml), and tobramycin (2 to 8g/ml); for the Wider panel for gram-positive organisms (reference 3W), amikacin (4 to 16g/ml), amoxicillin-clavulanate (4/2 to 32/16g/ml), ampicillin (0.5 to 16g/ml), cefazolin (2 to 4g/ml), cefotaxime (0.06 to 4g/ml), cefu-roxime (0.5 to 2 g/ml), chloramphenicol (8g/ml), ciprofloxacin (0.5 to 4
g/ml), clindamycin (0.5 and 2g/ml), erythromycin (0.12 and 0.5 to 2g/ml), fosfomycin (32 to 64g/ml), gentamicin (2 to 8 and 500g/ml), oxacillin (1 to 4
[image:2.612.56.548.79.540.2]g/ml), penicillin (0.06 to 8g/ml), rifampin (0.5 and 2g/ml), streptomycin (1,000g/ml), teicoplanin (1 to 16g/ml), trimethoprim-sulfamethoxazole (1/19 to 2/38g/ml), and vancomycin (1 to 16g/ml); for the supplementary panel TABLE 1. Enterobacteriaceaewith known-lactam-resistance mechanisms
Resistance mechanism Organism
(no. of isolates tested)
Primary Secondary
Chromosomal AmpC-lactamase,
basally expressed Enterobacter cloacae(1)
Chromosomal AmpC-lactamase,
inducibly expressed Enterobacter aerogenesEnterobacter cloacae(2)(1)
Citrobacter freundii(1)
Morganella morganii(2)
Chromosomal AmpC-lactamase,
constitutively hyperproduced Enterobacter aerogenes(1)
Enterobacter cloacae(2)
Citrobacter freundii(1)
Morganella morganii(2)
Escherichia coli(9)
Chromosomal class A-lactamase Proteus vulgaris(2)
Kluyveraspp. (2)
Citrobacter diversus(2)
Klebsiella oxytoca(2)
TEM-1-lactamase Escherichia coli(4)
Proteus mirabilis(2)
Salmonellaspp. (2)
TEM-1-lactamase,
hyperproduced Escherichia coli(4)
OXA-1-lactamase Escherichia coli(1)
Salmonellaspp. (1)
SHV-1-lactamase Klebsiella pneumoniae(4)
IRT-lactamase Escherichia coli(3)
Porin-deficient mutant (OmpF⫺) Escherichia coli(3)
Porin-deficient mutant (OmpF⫺) TEM-1-lactamase Escherichia coli(4)
Porin-deficient mutant (OmpK36⫺) SHV-1-lactamase Klebsiella pneumoniae(1)
Extended spectrum-lactamase Porin-deficient mutant (OmpF⫺) Escherichia coli(1) Extended spectrum-lactamase Chromosomal AmpC-lactamase, inducibly expressed Enterobacter cloacae(3)
Enterobacter aerogenes(1)
Citrobacter freundii(1)
Extended-spectrum-lactamase Chromosomal AmpC-lactamase, constitutively hyperproduced Enterobacter cloacae(1)
1340 CANTO´ N ET AL. J. CLIN. MICROBIOL.
on May 15, 2020 by guest
http://jcm.asm.org/
(reference 5W), aztreonam (0.12 to 16g/ml), cefepime (0.12 to 16g/ml), ceftriaxone (0.12 to 16g/ml), chloramphenicol (1 to 8g/ml), colistin (2 to 4
g/ml), imipenem (0.125 to 16g/ml), meropenem (0.12 to 16g/ml), ofloxacin (0.06 to 8g/ml), piperacillin (8 to 64g/ml), piperacillin-tazobactam (8/4 to 64/4g/ml), sulbactam (1 to 8g/ml), tetracycline (1 to 16g/ml), and trova-floxacin (0.06 to 4g/ml).
The panels were inoculated with a standardized inoculum by using a rehydra-tor-inoculator (RENOK) by following the guidelines provided by the manufac-turer. The inoculum was prepared with the Prompt inoculation system (29). After overnight incubation in a conventional chamber, the panels were intro-duced into the Wider system. The results of the external reactions, the oxidase test for negative organisms, and catalase and hemolysis tests for gram-positive organisms should be marked in a special square in the commercial tray. Consequently, the video camera reflects these results at the same time as the other biochemical reactions.
Reference methods.API galleries (API 20E, API 20NE, API Staph, and API Strep; BioMerieux, SA, Marcy-l’E´toile, France) were used as the reference tests for bacterial identification. Conventional biochemical tests (17) were also per-formed when discrepancies were observed. The MIC results obtained with the Wider system were compared with those obtained by the reference broth mi-crodilution method described by NCCLS (19). The final inoculum concentration was 5⫻105CFU/ml. Antimicrobial powders were obtained from their respective
manufacturers.
Quality control.Quality control was assured by running every day the organ-isms recommended for this purpose by NCCLS (20):Escherichia coliATCC 25922 and ATCC 35218,Staphylococcus aureusATCC 29213,Enterococcus fae-calisATCC 29212, andPseudomonas aeruginosaATCC 27853. The reproduc-ibility of the MIC readings was also analyzed with the American Type Culture Collection (ATCC) strains. These strains and Proteus vulgaris ATCC 13315,
Klebsiella pneumoniaeATCC 29665,Klebsiella oxytocaATCC 49131,Salmonella enterica subsp. arizonae ATCC 12323, Enterobacter cloacae ATCC 13047,
Stenotrophomonas maltophiliaATCC 13637,Staphylococcus epidermidisATCC 12228, andListeria monocytogenesATCC 19112 were run during the evaluation as quality controls for bacterial identification.
Analysis and accuracy of results.The identification scores provided by the Wider system software were not considered in the analysis; instead, the final identification results were used. A “correctly identified” category was established when identical identifications at the species level were provided by the Wider system and by the reference method. The “partially identified” category meant that the strain identifications were coincident only at the genus level, and the “incorrectly identified” category meant that the genus assigned by the Wider system was different from that obtained assigned by the reference method.
Susceptibility testing agreements or discrepancies were analyzed by consider-ing all the organism-antimicrobial agent combinations with 18, 12, 13, 9, and 8 antimicrobial agents for theEnterobacteriaceae, NFGNRs,Staphylococcusspp. andMicrococcusspp.,Enterococcusspp., and-hemolytic streptococcal isolates, respectively. “Essential agreement” was defined when the MICs obtained with the Wider system and by the reference method were identical or⫾1 log2dilution.
Moreover, by using the interpretive NCCLS criteria (20), qualitative analysis was also performed. Those antibiotics for which the concentrations present in the evaluated panel did not allow the use of NCCLS criteria were excluded from the analysis. When the MIC was categorized as susceptible with the Wider system and as resistant by the reference method, the classification of a “very major error” was made. The endpoint “major error” was used when the MIC obtained with the Wider system was categorized as resistant and that obtained by the reference method was categorized as susceptible. The term “minor error” was used when the MIC obtained with the Wider system was categorized as inter-mediate and that obtained by the reference method was categorized as suscep-tible or resistant and when the MIC obtained with the Wider system was cate-gorized as susceptible or resistant and that obtained by the reference method was categorized as intermediate. A similar susceptibility testing analysis was per-formed with isolates of the familyEnterobacteriaceaewith known resistance mechanisms, but only the results obtained with amoxicillin-clavulanate, ticarcil-lin, cefuroxime, cefoxitin, cefotaxime, ceftazidime, cefepime, and imipenem were compared.
RESULTS
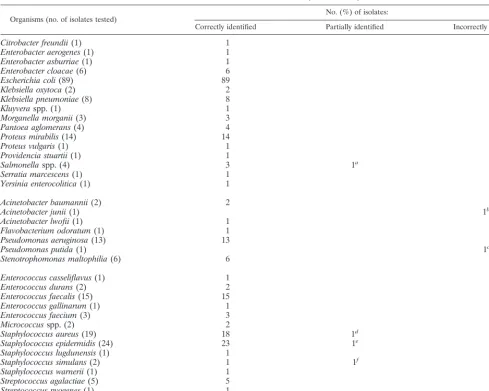
Organism identification.Table 2 shows the performance of the Wider system for bacterial identification. A total of 244 isolates routinely obtained from different clinical sources were tested. The Wider system correctly identified 97.5% of these bacterial clinical isolates: 99.3% of the isolates of the family Enterobacteriaceae, 92.0% of the NFGNRs, and 96.3% of the gram-positive organisms. Misidentifications at the genus level (incorrect identification) were limited to only two NFGNRs. In addition, one enterobacterial isolate and three staphylococcal isolates were partially identified (misidentification to the spe-cies level). It must be stressed that aSalmonellasp. isolate and
anS. aureus isolate were incorrectly identified as S. enterica subsp. arizonae and a coagulase-negative staphylococcus, re-spectively. Bacterial strains for identification quality control were always correctly identified, including S. enterica subsp. arizonaeATCC 12323 andS. aureusATCC 29213.
It is noteworthy that five isolates (two coagulase-negative staphylococci and one isolate each ofAcinetobacter baumannii, Stenotrophomonas maltophilia, andEnterococcus durans) were misidentified with the reference API system. In these cases, conventional biochemical test results for arbitration confirmed the Wider system identification result.
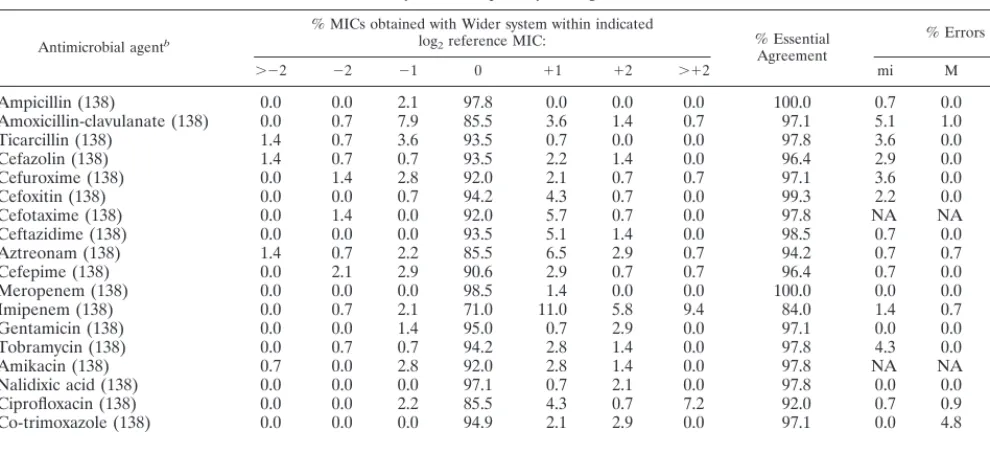
Susceptibility testing of routine isolates. A total of 3,719 organism-antimicrobial agent combinations were analyzed: 2,484 for isolates of the family Enterobacteriaceae, 300 for NFGNRs, and 893 for gram-positive isolates. The overall es-sential agreement in MICs (⫾1 log2 dilution) for all these
organism-antimicrobial agent combinations was 95.6%; 1.6% of the results with the Wider system were 2 or more dilutions lower than the reference MICs, and 2.8% of the results were 2 or more dilutions higher than the reference MICs.
Results for theEnterobacteriaceae, NFGNRs, and gram-pos-itive isolates and the antimicrobial agents evaluated for each bacterial group are indicated in Tables 3, 4, and 5, respectively. The lowest essential agreement was observed with the NFGNRs, 88.0%, a value significantly lower than those ob-tained for isolates of the familyEnterobacteriaceae(96.6%) and gram-positive cocci (95.6%). Imipenem was the antimicrobial agent tested with the enterobacterial isolates (84.0%) with the lowest essential agreement in MICs. For this group of bacterial isolates, imipenem MICs were clearly displaced to higher val-ues when they were determined with the Wider system. In contrast, 100% essential agreement in MICs was observed with meropenem. Moreover, ciprofloxacin MICs were also dis-placed to higher values. Among NFGNRs, piperacillin and cefepime yielded the lowest essential agreement (80.0%). None of the antimicrobial agents analyzed yielded 100% es-sential agreement for NFGNRs (Table 4). For gram-positive cocci, the essential agreement obtained with penicillin was only 80.4%, but it was greater than 90.0% with the other antimi-crobial agents tested (Table 5). Most of the discrepancies in penicillin MICs for gram-positive cocci were due to staphylo-coccal isolates, but no interpretive errors were detected. On the contrary, 100% agreement between the results obtained with the Wider system and those obtained by the standard microdilution method was observed with the enterococcal iso-lates when results for ampicillin resistance, high-level genta-micin resistance, and high-level streptomycin resistance were compared.
The overall agreement of the interpretive categories ob-tained with the Wider system compared with those obob-tained by the standard microdilution method when the NCCLS criteria were used was 95.8%, ranging from 82.8% for NFGNRs to 97.4% for gram-positive cocci. Results for cefotaxime and ami-kacin with theEnterobacteriaceaeand gram-positive cocci and for cefazolin and erythromycin with gram-positive cocci were suppressed in the interpretive category analysis, as the antimi-crobial concentrations presented in the Wider system panels do not allow the use of NCCLS interpretive criteria (Tables 3, 4, and 5). Equal to or less than 2.0% of the errors were major (16 of 2,478) or very major (12 of 582) errors, and these were mainly due to discrepancies in interpretive categories with piperacillin and co-trimoxazole for NFGNRs. Only 48 of 3,172 (1.5%) organism-antimicrobial agent combinations tested were classified as having minor discrepancies. Again, the most important percentage of minor errors were for NFGNRs. De-spite the smaller number of NFGNRs tested, minor
on May 15, 2020 by guest
http://jcm.asm.org/
ancies appeared to be randomly distributed among these iso-lates.
The ATCC strains recommended by NCCLS were used in the quality control procedure, and these were also used to study the reproducibilities of the MIC readings. At least 25 runs were performed on different days with each ATCC strain. MICs were highly reproducible, although the MICs for certain ATCC organism-antimicrobial agent combinations were equal to or below the lowest concentration of the antimicrobial agent in the wells. With the exception of the combination penicil-lin-S. aureus ATCC 29213, MICs were within the expected ranges. The penicillin MICs for S. aureus ATCC 29213 ex-ceeded the expected range in 44% of the runs. It is noteworthy that for penicillin andE. faecalisATCC 25922, for imipenem andE. coliATCC 25922, and for imipenem andP. aeruginosa ATCC 27853, MICs were persistently near the upper limit of the MIC range.
[image:4.612.55.545.83.474.2]Susceptibility testing ofEnterobacteriaceaewith well-charac-terized-lactam resistance mechanisms.A total of 800 organ-ism-antimicrobial agent combinations were analyzed. The es-sential agreement of susceptibility testing of isolates of the family Enterobacteriaceae with known -lactam resistance mechanisms with the Wider system and by the standard mi-crodilution method was 94.8% (Table 6), which is slightly lower than that obtained with routine isolates of the family Enterobacteriaceae(97.4%). The highest essential agreement was observed with chromosomal AmpC -lactamase-produc-ing isolates (97.7%) and permeability mutants (98.4%). On the contrary, the lowest essential agreement was obtained with chromosomal class-A-lactamase-producing isolates (89.1%). The analysis of the different antimicrobial agents tested re-vealed that more than 97.0% essential agreement was observed for ticarcillin, cefuroxime, cefoxitin, cefotaxime, and ceftazi-dime. The corresponding values for amoxicillin-clavulanate,
TABLE 2. Identification of routine isolates by the Wider system
Organisms (no. of isolates tested) No. (%) of isolates:
Correctly identified Partially identified Incorrectly identified
Citrobacter freundii(1) 1
Enterobacter aerogenes(1) 1
Enterobacter asburriae(1) 1
Enterobacter cloacae(6) 6
Escherichia coli(89) 89
Klebsiella oxytoca(2) 2
Klebsiella pneumoniae(8) 8
Kluyveraspp. (1) 1
Morganella morganii(3) 3
Pantoea aglomerans(4) 4
Proteus mirabilis(14) 14
Proteus vulgaris(1) 1
Providencia stuartii(1) 1
Salmonellaspp. (4) 3 1a
Serratia marcescens(1) 1
Yersinia enterocolitica(1) 1
Acinetobacter baumannii(2) 2
Acinetobacter junii(1) 1b
Acinetobacter lwofii(1) 1
Flavobacterium odoratum(1) 1
Pseudomonas aeruginosa(13) 13
Pseudomonas putida(1) 1c
Stenotrophomonas maltophilia(6) 6
Enterococcus casseliflavus(1) 1
Enterococcus durans(2) 2
Enterococcus faecalis(15) 15
Enterococcus gallinarum(1) 1
Enterococcus faecium(3) 3
Micrococcusspp. (2) 2
Staphylococcus aureus(19) 18 1d
Staphylococcus epidermidis(24) 23 1e
Staphylococcus lugdunensis(1) 1
Staphylococcus simulans(2) 1 1f
Staphylococcus warnerii(1) 1
Streptococcus agalactiae(5) 5
Streptococcus pyogenes(1) 1
Total (244) 238 (97.5) 4 (1.6) 2 (0.8)
aIdentified with the Wider system asSalmonella entericasubsp.arizonae. bIdentified with the Wider system asEmpedobacter brevis.
cIdentified with the Wider system asAcinetobacter anitratus-A. haemolyticus. dIdentified with the Wider system asStaphylococcus simulans.
eIdentified with the Wider system asStaphylococcus auricularis. fIdentified with the Wider system asStaphylococcus hominis.
1342 CANTO´ N ET AL. J. CLIN. MICROBIOL.
on May 15, 2020 by guest
http://jcm.asm.org/
imipenem, and cefepime were 94.0, 90.0, and 83.0%, respec-tively.
Interpretive category analysis showed that only two very major errors were observed (0.8%) among isolates of the fam-ilyEnterobacteriaceaewith known-lactam resistance mecha-nisms. These were detected with amoxicillin-clavulanate and anE. colistrain that produced an extended-spectrum- -lacta-mase and with ticarcillin and a Proteus vulgaris strain that produced a chromosomal class A-lactamase. The minor er-rors represented 3.6% of the susceptibility test determinations. Forty percent of them were for extended-spectrum  -lacta-mase-producing isolates and were particularly observed for amoxicillin-clavulanate (5 of 41) and cefepime (15 of 41) de-terminations.
DISCUSSION
Simultaneous identification and susceptibility testing is clearly an advantage of automatic and semiautomatic commer-cial systems (4, 7). The Wider system is a newly developed semiautomatic device for bacterial identification and suscepti-bility testing which needs the classical overnight period for retrieval of results. The major attraction of this system is the image-processing technology that has been applied for the first time to the reading of commercial trays for bacterial identifi-cation and susceptibility testing. Biochemical patterns and MICs are processed by the computer and are offered to the operator both visually and, if required, on paper. Indeed, a particular advantage of image-assisted analysis is that the
sys-TABLE 3. Performance of Wider system susceptibility testing with routineEnterobacteriaceaeisolatesa
Antimicrobial agentb
% MICs obtained with Wider system within indicated
log2reference MIC: % Essential
Agreement
% Errors
⬎⫺2 ⫺2 ⫺1 0 ⫹1 ⫹2 ⬎⫹2 mi M VM
Ampicillin (138) 0.0 0.0 2.1 97.8 0.0 0.0 0.0 100.0 0.7 0.0 0.0
Amoxicillin-clavulanate (138) 0.0 0.7 7.9 85.5 3.6 1.4 0.7 97.1 5.1 1.0 0.0
Ticarcillin (138) 1.4 0.7 3.6 93.5 0.7 0.0 0.0 97.8 3.6 0.0 0.0
Cefazolin (138) 1.4 0.7 0.7 93.5 2.2 1.4 0.0 96.4 2.9 0.0 6.6
Cefuroxime (138) 0.0 1.4 2.8 92.0 2.1 0.7 0.7 97.1 3.6 0.0 0.0
Cefoxitin (138) 0.0 0.0 0.7 94.2 4.3 0.7 0.0 99.3 2.2 0.0 0.0
Cefotaxime (138) 0.0 1.4 0.0 92.0 5.7 0.7 0.0 97.8 NA NA NA
Ceftazidime (138) 0.0 0.0 0.0 93.5 5.1 1.4 0.0 98.5 0.7 0.0 0.0
Aztreonam (138) 1.4 0.7 2.2 85.5 6.5 2.9 0.7 94.2 0.7 0.7 33.3
Cefepime (138) 0.0 2.1 2.9 90.6 2.9 0.7 0.7 96.4 0.7 0.0 0.0
Meropenem (138) 0.0 0.0 0.0 98.5 1.4 0.0 0.0 100.0 0.0 0.0 0.0
Imipenem (138) 0.0 0.7 2.1 71.0 11.0 5.8 9.4 84.0 1.4 0.7 0.0
Gentamicin (138) 0.0 0.0 1.4 95.0 0.7 2.9 0.0 97.1 0.0 0.0 0.0
Tobramycin (138) 0.0 0.7 0.7 94.2 2.8 1.4 0.0 97.8 4.3 0.0 0.0
Amikacin (138) 0.7 0.0 2.8 92.0 2.8 1.4 0.0 97.8 NA NA NA
Nalidixic acid (138) 0.0 0.0 0.0 97.1 0.7 2.1 0.0 97.8 0.0 0.0 0.0
Ciprofloxacin (138) 0.0 0.0 2.2 85.5 4.3 0.7 7.2 92.0 0.7 0.9 0.0
Co-trimoxazole (138) 0.0 0.0 0.0 94.9 2.1 2.9 0.0 97.1 0.0 4.8 0.0
Total (2,484) 0.3 0.5 1.8 91.8 3.2 1.5 1.1 96.6 1.7 0.5 0.9
[image:5.612.57.552.83.309.2]aAbbreviations: NA, not applicable; mi, minor error; M, major error; VM, very major error. bValues in parentheses are the number of organism-antimicrobial agent combinations tested.
TABLE 4. Performance on Wider system susceptibility testing with routine NFGNRsa
Antimicrobial agentb
% MICs obtained with Wider system within indicated
log2reference MICs: % Essential
agreement
% Errors
⬎⫺2 ⫺2 ⫺1 0 ⫹1 ⫹2 ⬎⫹2 mi M VM
Piperacillin (25) 8.0 4.0 8.0 72.0 0.0 8.0 0.0 80.0 4.0 0.0 50.0
Piperacillin-tazobactam (25) 4.0 0.0 4.0 72.0 12.0 4.0 4.0 88.0 4.0 7.7 4.0
Ceftazidime (25) 0.0 8.0 4.0 72.0 12.0 4.0 0.0 88.0 4.0 5.2 0.0
Aztreonam (25) 8.0 0.0 20.0 68.0 4.0 0.0 0.0 92.0 4.0 0.0 12.5
Cefepime (25) 0.0 8.0 12.0 56.0 12.0 8.0 4.0 80.0 4.0 0.0 0.0
Imipenem (25) 0.0 0.0 0.0 76.0 12.0 4.0 8.0 88.0 4.0 0.0 0.0
Meropenem (25) 0.0 4.0 12.0 76.0 4.0 4.0 0.0 92.0 0.0 0.0 0.0
Gentamicin (25) 0.0 0.0 0.0 80.0 8.0 8.0 4.0 88.0 8.0 0.0 0.0
Tobramycin (25) 0.0 0.0 0.0 88.0 4.0 8.0 0.0 92.0 0.0 5.0 0.0
Amikacin (25) 0.0 0.0 0.0 80.0 12.0 8.0 0.0 92.0 NA NA NA
Ciprofloxacin (25) 0.0 4.0 4.0 84.0 0.0 8.0 0.0 88.0 0.0 0.0 16.6
Co-trimoxazole (25) 0.0 8.0 12.0 64.0 12.0 4.0 0.0 88.0 0.0 4.0 8.0
Total (300) 1.7 3.0 6.3 73.6 8.0 5.7 1.7 88.0 2.9 2.2 12.1
aAbbreviations: NA, not applicable; mi, minor error; M, major error; VM, very major error. bValues in parentheses are the number of organism-antimicrobial agent combinations tested.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:5.612.53.554.532.711.2]tem greatly facilitates reading of the results, but the results for the panels can still be interpreted directly by the microbiologist by applying classical criteria. This eliminates dependence on a fully automatic device; moreover, the technologist can adjust the video-assisted readings prior to the release of a patient’s results. This approach has previously been applied for disk diffusion antibiograms (3, 10) and also for an unsuccessful API Aladin instrument, marketed in the late 1980s, which used microdilution tray wells for bacterial identification and suscep-tibility testing (12).
In the present study, the Wider system correctly identified at the species level 95.7% of routine clinical isolates, represented by 20 genera commonly isolated in a clinical microbiology laboratory. This percentage is similar to or slightly higher than those observed in other studies with other systems (25, 31) and demonstrates that with currently accepted criteria the Wider system is an acceptable method for bacterial identification (15). For the isolates of the familyEnterobacteriaceae, the only identification problem was an atypical lactose-positiveS. en-tericaserovar Enteritidis isolate which was misidentified by the
Wider system as S. enterica subsp. arizonae. This particular problem has also been delineated with other systems (18); however, the Wider system correctly identified theS. enterica subsp.arizonaeATCC 12323 strain. As with other systems, less accuracy (92.0%) than that observed with isolates of the family Enterobacteriaceaewas shown when only NFGNRs were taken into account (8, 22, 24, 25, 27). In all cases, the API system was used as the “gold standard” for bacterial identification, as it is a well-recognized system for this purpose (25, 31). Neverthe-less, conventional biochemical tests were also performed when discrepancies between the Wider system and the API galleries were observed before assuming that the API identification was correct.
[image:6.612.59.552.84.289.2]The Wider system database contains information on 112 and 42 different taxa for gram-negative and gram-positive bacteria, respectively, which includes both organisms usually encoun-tered in clinical laboratories and those rarely isolated. It is remarkable that, with the exception of the oxidase test for gram-negative organisms and catalase and hemolysis tests for gram-positive organisms, the Wider system does not require
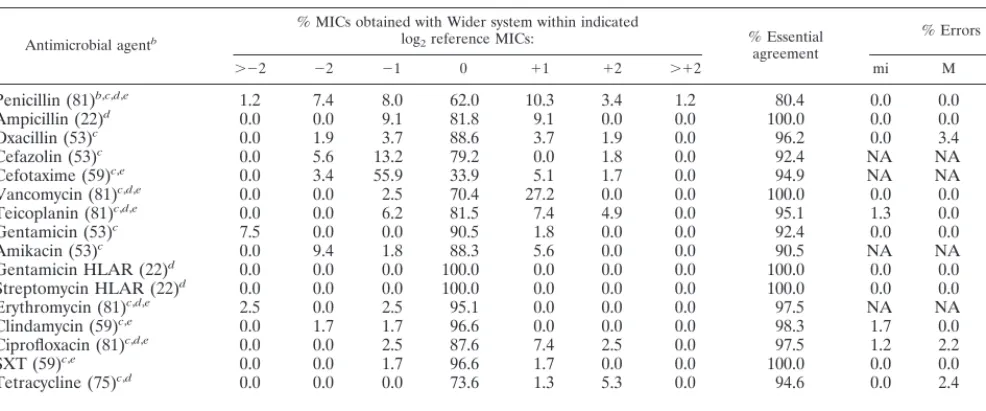
TABLE 5. Performance of Wider system susceptibility testing with gram-positive isolatesa
Antimicrobial agentb
% MICs obtained with Wider system within indicated
log2reference MICs: % Essential
agreement
% Errors
⬎⫺2 ⫺2 ⫺1 0 ⫹1 ⫹2 ⬎⫹2 mi M VM
Penicillin (81)b,c,d,e 1.2 7.4 8.0 62.0 10.3 3.4 1.2 80.4 0.0 0.0 0.0
Ampicillin (22)d 0.0 0.0 9.1 81.8 9.1 0.0 0.0 100.0 0.0 0.0 0.0
Oxacillin (53)c 0.0 1.9 3.7 88.6 3.7 1.9 0.0 96.2 0.0 3.4 0.0
Cefazolin (53)c 0.0 5.6 13.2 79.2 0.0 1.8 0.0 92.4 NA NA NA
Cefotaxime (59)c,e 0.0 3.4 55.9 33.9 5.1 1.7 0.0 94.9 NA NA NA
Vancomycin (81)c,d,e 0.0 0.0 2.5 70.4 27.2 0.0 0.0 100.0 0.0 0.0 0.0
Teicoplanin (81)c,d,e 0.0 0.0 6.2 81.5 7.4 4.9 0.0 95.1 1.3 0.0 0.0
Gentamicin (53)c 7.5 0.0 0.0 90.5 1.8 0.0 0.0 92.4 0.0 0.0 9.1
Amikacin (53)c 0.0 9.4 1.8 88.3 5.6 0.0 0.0 90.5 NA NA NA
Gentamicin HLAR (22)d 0.0 0.0 0.0 100.0 0.0 0.0 0.0 100.0 0.0 0.0 0.0
Streptomycin HLAR (22)d 0.0 0.0 0.0 100.0 0.0 0.0 0.0 100.0 0.0 0.0 0.0
Erythromycin (81)c,d,e 2.5 0.0 2.5 95.1 0.0 0.0 0.0 97.5 NA NA NA
Clindamycin (59)c,e 0.0 1.7 1.7 96.6 0.0 0.0 0.0 98.3 1.7 0.0 0.0
Ciprofloxacin (81)c,d,e 0.0 0.0 2.5 87.6 7.4 2.5 0.0 97.5 1.2 2.2 0.0
SXT (59)c,e 0.0 0.0 1.7 96.6 1.7 0.0 0.0 100.0 0.0 0.0 0.0
Tetracycline (75)c,d 0.0 0.0 0.0 73.6 1.3 5.3 0.0 94.6 0.0 2.4 0.0
Total (935) 0.7 1.9 6.9 82.5 6.0 1.7 0.1 95.5 0.4 1.6 0.6
aAbbreviations: NA, not applicable; SXT, trimethoprim-sulfamethoxazole; mi, minor error; M, major error; VM, very major error; HLRA, high-level aminoglycoside
resistance.
bValues in parentheses are the number of organism-antimicrobial agent combinations tested. cStaphylococcusandMicrococcus.
dEnterococcus.
e-Hemolytic streptococci.
TABLE 6. Results of comparison between Wider system susceptibility testing results and reference broth microdilution MIC for isolates of the familyEnterobacteriaceaewith known-lactam resistance mechanismsa
Primary resistance mechanismb % Essential
agreement
% Errors
mi M VM
Chromosomal AmpClactamase (176) 97.7 1.0 0.0 0.0
Chromosomal class A-lactamase (64) 89.1 7.1 2.7 6.2
Broad-spectrum and IRT-lactamases (168) 97.6 4.1 0.0 0.0
Extended-spectrum-lactamase (328) 92.3 3.5 2.0 0.8
Permeability mutant (64) 98.4 3.7 0.0 0.0
Total (800) 94.8 3.6 1.0 0.8
aAbbreviations: mi, minor error; M, major error; VM, very major error.
bValues in parentheses are the number of organism-antimicrobial agent combinations tested.
1344 CANTO´ N ET AL. J. CLIN. MICROBIOL.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:6.612.55.551.613.711.2]additional external reactions to provide the final identification or to improve the identification level. Other identification sys-tems need external biochemical tests other than those provided in the microdilution panels to resolve identifications with low probabilities of accuracy (8, 21). As with other devices, if a biochemical profile does not match one in the database, there may be no identification, but this did not occur with the routine isolates tested with the Wider system. As the purpose of our study was to determine the accuracy of the Wider system for the identification of bacteria that would routinely be encoun-tered in a hospital microbiology laboratory, additional studies with other relevant and uncommon organisms should be per-formed.
The susceptibility testing results obtained with the Wider system in tests with routine clinical isolates showed an overall essential agreement of 95.6% and an overall category interpre-tation error of 4.2%. Combined major and very major errors were less than 3%. These results meet the performance criteria for susceptibility testing (7, 9, 18). It is of note that these results were compiled by considering the results for both gram-nega-tive and -posigram-nega-tive isolates and a large number of antimicrobial agents for each isolate. When analyzed with respect to the organisms tested, the highest essential agreements were ob-served with isolates of the familyEnterobacteriaceae(96.6%) and gram-positive organisms (95.6%). As other investigators have noted with other systems (22, 23), lower essential agree-ment was observed with NFGNRs (88.0%). Nevertheless, in contrast to automated instrument systems with short incuba-tion times (14, 15), susceptibility testing results could be ob-tained for all organisms considered to be slowly growing or-ganisms.
When analyzed with respect to the antimicrobial agents tested, the lowest essential agreement for isolates of the family Enterobacteriaceaewas observed with imipenem (84.0%). It is remarkable that 26.2% of the imipenem MICs obtained with the Wider system were higher than those obtained by the reference method, but the percentage of interpretive errors was limited to only 1.4 and 0.7% minor and major errors, respectively, with no very major errors. This difference is clearly related to the intrinsic activity of imipenem (modal MIC, 0.25g/ml for isolates of the familyEnterobacteriaceae) and the relatively high MIC breakpoint for susceptibility (4 g/ml). For NFGNRs, the essential agreement for imipenem was 88.0%. Again, nearly 25% of the imipenem MICs obtained with the Wider system were higher than those obtained by the reference method. These higher imipenem MICs could be due to insufficient adjustment of inoculum size or to a decline in antimicrobial activity during storage. The former possibility was well corroborated by Doern et al. (6), who demonstrated that an inappropriately large inoculum size in automatic sus-ceptibility testing devices significantly modified the results, par-ticularly for cell wall-active antibiotics. False positive results for resistance may occur when the inoculum size is too large, and the numbers of major and minor errors are increased. In our study, the inoculum for the Wider system was prepared with the Prompt inoculation system (28), as recommended by the manufacturer. In contrast, the inoculum for the reference microdilution method was controlled nephelometrically. On the other hand, it has been shown that the activity of imipenem is particularly affected during storage (5, 26) and is a well-recognized cause of false-positive resistance with commercial microdilution panels (23, 28). It is not a surprise that the imipenem MICs forE. coli ATCC 25922 and P. aeruginosa ATCC 27853 were persistently near the upper limit of the MIC range recommended by NCCLS (20). The same problem of stability during storage could be responsible for the higher
penicillin MICs forS. aureusATCC 29213 and routine gram-positive isolates.
In previous evaluations of susceptibility testing devices, spe-cific attention has been given to resistant isolates (31). In our evaluation, although a limited number of resistant isolates were included among the clinical isolates (data not shown), no problems with specific issues of resistance specifically studied with other automatic susceptibility testing devices were de-tected, such as oxacillin resistance in staphylococci (13) and high-level aminoglycoside resistance in enterococci (30). Moreover, when assessing susceptibility testing instrument per-formance, in addition to fresh or stock clinical isolates and quality control strains, a set of organisms with known resis-tance mechanisms should be included (7, 9). One hundred isolates of the familyEnterobacteriaceaewith known-lactam resistance mechanisms were studied, and 800 organism-anti-microbial agent combinations were evaluated. Essential agree-ment and interpretive errors for eight -lactam antibiotics were 94.8 and 5.4%, respectively. Interestingly, the proportion of very major errors with this set of strains was limited to 0.8%. The lowest essential agreement was observed with extended-spectrum and chromosomal class A -lactamase-producing isolates. Slight variations in the inoculum size could affect the amount of these-lactamases and would be the reason for the lower essential agreement. The case of cefepime is illustrative, as this antibiotic has been shown to be very stable during storage (26) but is particularly affected by an increase in inoc-ulum size for those isolates with extended-spectrum -lacta-mases (R. Canto´n and A. Oliver, unpublished data). Interest-ingly, no decreases in the MICs with the Wider system were observed with ceftazidime and cefotaxime for extended-spec-trum-lactamase producing isolates of the family Enterobac-teriaceae, thus avoiding false-positive detection of isolates with these enzymes. The design of panels is essential for retrieval of results that can serve as indicators of the presence of extended-spectrum-lactamase-producing isolates (16). The wide range of concentrations for ceftazidime (0.5 to 16g/ml) and cefo-taxime (0.12 to 8g/ml) in the Wider system panels facilitates the detection of these isolates. In addition, the Wider system panels for gram-negative isolates possess the combination of ceftazidime plus clavulanate to facilitate the detection of these -lactamase-producing isolates.
In conclusion, our evaluation showed accurate and accept-able results with both routine clinical isolates and a set of isolates of the familyEnterobacteriaceaewith known-lactam resistance mechanisms. The Wider system is a new reliable tool which applies the image-processing technology for the reading of commercial trays for bacterial identification and suscepti-bility testing.
ACKNOWLEDGMENTS
We are grateful to Isabel Soler for continuous technical assistance.
REFERENCES
1.Baker, C. N., S. A. Stocker, D. L. Rhoden, and C. Thornsberry.1986. Evaluation of the MicroScan antimicrobial susceptibility system with the AutoScan-4 automated reader. J. Clin. Microbiol.19:744–747.
2.Baquero, F., J. Martı´nez-Beltra´n, R. Canto´n, y los Restantes Miembros de la Mesa Espan˜ola de Normalizacio´n de la Sensibilidad y Resistencia a los Antimicrobianos.1997. Criterios del Grupo MENSURA para la definicio´n de los puntos crı´ticos de sensibilidad a los antibio´ticos. Rev. Esp. Quimioter.
10:303–313.
3.Berke, I., and P. M. Tierno, Jr.1996. Comparison of efficacy and cost-effectiveness of BIOMIC VIDEO and Vitek antimicrobial susceptibility test systems for use in the clinical microbiology laboratory. J. Clin. Microbiol.
34:1980–1984.
4.Cherubin, C., R. Eng, and M. A. Appleman.1987. A critique of semiauto-mated susceptibility systems. Rev. Infect. Dis.9:655–659.
on May 15, 2020 by guest
http://jcm.asm.org/
5.Daly, J. S., D. B. DeLuca, S. R. Hebert, R. A. Dodge, and D. T. Soja.1994. Imipenem stability in a predried susceptibility panel. J. Clin. Microbiol.
32:2584–2587.
6.Doern, G. V., A. B. Brueggemann, R. Perla, J. Daly, D. Halkias, R. N. Jones, and M. A. Saubolle.1997. Multicenter laboratory evaluation of the bio-Merieux Vitek antimicrobial susceptibility testing system with 11 antimicro-bial agents versus members of the familyEnterobacteriaceaeand Pseudomo-nas aeruginosa. J. Clin. Microbiol.35:2115–2119.
7.Ferraro, M. J., and J. H. Jorgensen.1999. Susceptibility testing instrumen-tation and computerized expert systems for data analysis and interpreinstrumen-tation, p. 1593–1600.InP. R. Murray, E. J. Baron, M. A. Pfaller, F. C. Tenover, and R. H. Yolken (ed.), Manual of clinical microbiology, 7th ed. American Society for Microbiology, Washington, D.C.
8.Flunke, G., D. Monnet, C. DeBernardis, A. von Graevenitz, and J. Freney.
1998. Evaluation of the Vitek 2 system for rapid identification of medically relevant gram-negative rods. J. Clin. Microbiol.36:1948–1952.
9.Food and Drug Administration.1991. Federal guidelines. Review criteria for assessment of antimicrobial susceptibility testing device. Food and Drug Administration. Rockville, Md.
10. Hejblum, G., V. Jarlier, J. Grosset, and A. Aurengo.1993. Automated in-terpretation of disk diffusion antibiotic susceptibility test with the radial profile analysis algorithm. J. Clin. Microbiol.31:2396–2401.
11. Isenberg, H. D., A. Reichler, and D. Wiseman.1971. Prototype of a fully automated device for determination of bacterial antibiotic susceptibility test-ing in the clinical laboratory. Appl. Microbiol.22:980–986.
12. Jorgensen, J. H.1991. Antibacterial susceptibility tests: automated or instru-ment-based methods, p. 1166–1172.InA. Balows, W. J. Hausler, Jr., K. L. Herrmann, H. D. Isenberg, and H. J. Shadomy (ed.), Manual of clinical microbiology, 5th ed. American Society for Microbiology, Washington, D.C. 13. LaTemple, D., and C. Cruz.1994. Evaluation of MicroScan rapid gram-positive panels for detection of oxacillin-resistant staphylococci. J. Clin. Microbiol.32:1058–1059.
14. McGregor, A., F. Schio, S. Beaton, V. Boulton, M. Perman, and G. Gilbert.
1995. The MicroScan WalkAway diagnostic microbiology system. An evalu-ation. Pathology27:172–176.
15. Miller, J. M., and C. M. O’Hara.1999. Manual and automated systems for microbial identification, p. 193–201.InP. R. Murray, E. J. Baron, M. A. Pfaller, F. C. Tenover, and R. H. Yolken (ed.), Manual of clinical microbi-ology, 7th ed. American Society for Microbimicrobi-ology, Washington, D.C. 16. Moland, E. S., C. C. Sanders, and K. S. Thomson.1998. Can results obtained
with commercially available MicroScan microdilution panels serve as an indicator of-lactamase production amongEscherichia coliandKlebsiella
isolates with hidden resistance to expanded-spectrum cephalosporins and aztreonam? J. Clin. Microbiol.36:2575–2579.
17. Murray, P. R., E. J. Baron, M. A. Pfaller, F. C. Tenover, and R. H. Yolken (ed.).1999. Manual of clinical microbiology, 7th ed. American Society for Microbiology, Washington, D.C.
18. National Committee for Clinical Laboratory Standards.1994. Development of in vitro susceptibility testing criteria and quality control parameters:
ap-proved guideline. Document M23-A. National Committee for Clinical Lab-oratory Standards, Wayne, Pa.
19. National Committee for Clinical Laboratory Standards.1997. Method for dilution antimicrobial susceptibility tests for bacteria that grow aerobically, 4th ed. Approved standard. Document M7-A4. National Committee for Clinical Laboratory Standards, Wayne, Pa.
20. National Committee for Clinical Laboratory Standards.1999. Performance standards for antimicrobial susceptibility testing. Ninth informational sup-plement. Document M100-S9. National Committee for Clinical Laboratory Standards, Wayne, Pa.
21. O’Hara, C. M., F. C. Westbrook, and J. M. Miller.1993. Parallel comparison of accuracy of API 20E, Vitek GNI, MicroScan Walk/Away Rapid ID, and Becton Dickinson Cobas Micro ID-E/NF for identification of members of the familyEnterobacteriaceaeand common gram-negative, non-glucose-fer-menting bacilli. J. Clin. Microbiol.31:3165–3169.
22. O’Hara, C. M., G. L. Westbrook, and J. M. Miller.1997. Evaluation of Vitek GNI⫹and Becton Dickinson Microbiology Systems Crystal E/NF identifi-cation systems for identifiidentifi-cation of members of the familyEnterobacteriaceae
and other gram-negative, glucose-fermenting and non-glucose-fermenting bacilli. J. Clin. Microbiol.35:3269–3273.
23. O’Rourke, E. J., K. G. Lambert, K. C. Parsonnet, A. B. Macone, and D. A. Goldmann.1991. False resistance to imipenem with a microdilution suscep-tibility testing system. J. Clin. Microbiol.29:827–829.
24. Simoons-Smit, A. M., and D. M. MacLaren.1994. Comparison of Vitek and Cobas Micro systems with semiautomated conventional microsystem for identification and susceptibility testing of gram-negative bacilli. J. Clin. Pathol.47:71–75.
25. Stager, C. E., and J. R. Davis.1992. Automated systems for identification of microorganisms. Clin. Microbiol. Rev.5:302–327.
26. Valdezate, S., J. M. Martı´nez-Beltra´n, L. de Rafael, F. Baquero, and R. Canto´n.1996.-Lactam stability in frozen microdilution PASCO MIC pan-els using strains with known resistance mechanisms as biosensors. Diagn. Microbiol. Infect. Dis.26:53–61.
27. Visser, M. R., L. Bogaards, M. Rozenberg-Arska, and J. Verhoef.1992. Comparison of the autoSCAN-W/A and Vitek Automicrobic systems for identification and susceptibility testing of bacteria. Eur. J. Clin. Microbiol. Infect Dis.11:979–984.
28. White, R. L., M. B. Kays, L. V. Friedrich, E. W. Brown, and J. R. Koonce.
1991. Pseudoresistance ofPseudomonas aeruginosaresulting from degrada-tion of imipenem in an automated susceptibility testing system with predried panels. J. Clin. Microbiol.29:398–400.
29. Wicks, J. H., R. L. Nelson, and G. E. Krejcarek.1983. Rapid inoculum standardization system: a novel device for standardization of inocula in antimicrobial susceptibility testing. J. Clin. Microbiol.17:1114–1119. 30. Woods, G. L., B. DiGiovanni, M. Levison, P. Pitsakis, and D. LaTemple.
1993. Evaluation of MicroScan rapid panels for detection of high-level ami-noglycoside resistance in enterococci. J. Clin. Microbiol.31:2786–2787. 31. York, M. K., G. F. Brooks, and E. H. Fiss.1992. Evaluation of the
auto-SCAN-W/A Rapid System for identification and susceptibility testing for gram-negative fermentative bacilli. J. Clin. Microbiol.30:2903–2910.
1346 CANTO´ N ET AL. J. CLIN. MICROBIOL.