INTRODUCTION
Papillary thyroid cancer (PTC) is the most common endocrine cancer, and its incidence has increased over the last three
de-cades all over the world, including Korea.1,2 Although survival
with PTC is excellent, substantial recurrence rates are prob-lematic. Growth of thyroid cancer through a tissue barrier may be a feature of the primary cancer itself or of a metastatic de-posit in a lymph node (LN), where it is described as
extranod-al extension (ENE).3 ENE is defined pathologically by tumor
cells extending beyond the lymph-node capsule into the peri-nodal fibroadipose tissue. Thus, microscopic or gross disease
beyond nodal capsule resulted in the diagnosis.3 ENE in
thy-roid cancer was first reported by Spires, et al.4 However, they
did not identify this as a significant adverse prognostic feature. They initially suggested that the presence of extrathyroidal ex-tension (ETE) and ENE was associated. Since then, ENE in PTC has been associated with an increased risk of distant
metasta-ses,5 disease persistence,3 and disease-specific mortality.6,7
Re-cently, the prognostic significance of histologic features of the involved LN rather than simply the presence of metastatic
de-posits has been highlighted.8
Even though ENE is common in PTC, death is not, and this lack of clear prognostic indication led to controversy regarding
Prognostic Value of Extranodal Extension
in Thyroid Cancer: A Meta-Analysis
Sunghwan Suh
1*, Kyoungjune Pak
2*, Ju Won Seok
3, and In Joo Kim
21Department of Internal Medicine, Dong-A University College of Medicine, Busan;
2Department of Nuclear Medicine and Biomedical Research Institute, Pusan National University Hospital, Busan; 3Department of Nuclear Medicine, Chung-Ang University College of Medicine, Seoul, Korea.
Purpose: Thyroid cancer is the most common endocrine cancer and its incidence has continuously increased in the last three de-cades all over the world. We aimed to evaluate the prognostic value of extranodal extension (ENE) of thyroid cancer.
Materials and Methods: We performed a systematic search of MEDLINE (from inception to June 2014) and EMBASE (from incep-tion to June 2014) for English-language publicaincep-tion. The inclusion criteria were studies of thyroid cancer that reported the prognos-tic value of ENE in thyroid cancer. Reviews, abstracts, and editorial materials were excluded, and duplicate data were removed. Two authors performed the data extraction independently.
Results: 6 studies including 1830 patients were eligible for inclusion in the study. All patients included in the meta-analysis had papillary thyroid cancer (PTC). Recurrence-free survival was analyzed based on 3 studies. The pooled hazard ratio for recurrence was 2.01 [95% confidence interval (CI) 1.19–3.40, p=0.009]. Disease-specific survival was analyzed based on 3 studies with 973 pa-tients. Patients of PTC with ENE showed 3.37-fold higher risk of death from the disease (95% CI 1.55–7.32, p=0.002).
Conclusion: ENE should be considered to be a poor prognostic marker in thyroid cancer; such knowledge might improve the man-agement of individual patients. This might facilitate the planning of appropriate ablation therapy and tailored patient follow-up from the beginning of treatment.
Key Words: Thyroid carcinoma, lymph nodes, prognosis
pISSN: 0513-5796 · eISSN: 1976-2437
Received: April 14, 2016 Revised: May 30, 2016 Accepted: June 8, 2016
Co-corresponding authors: Dr. In Joo Kim, Department of Nuclear Medicine and Biomedical Research Institute, Pusan National University Hospital, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea.
Tel: 82-51-240-7224, Fax: 82-51-240-7389, E-mail: [email protected] and Dr. Ju Won Seok, Department of Nuclear Medicine, Chung-Ang University College of Medicine, 102 Heukseok-ro, Dongjak-gu, Seoul 06973, Korea.
Tel: 82-2-6299-3232, Fax: 82-2-6299-3221, E-mail: [email protected] *Sunghwan Suh and Kyoungjune Pak contributed equally to this work. •The authors have no financial conflicts of interest.
© Copyright: Yonsei University College of Medicine 2016
This is an Open Access article distributed under the terms of the Creative Com-mons Attribution Non-Commercial License (http://creativecomCom-mons.org/licenses/ by-nc/3.0) which permits unrestricted non-commercial use, distribution, and repro-duction in any medium, provided the original work is properly cited.
the effect of ENE on survival. Therefore, ENE is not recognized in any staging system, while ETE of the primary tumor
increas-es primary tumor stage.7 LN continues to be staged solely on
location and pathologic evidence of involvement. As LN me-tastases do not all affect prognosis equally, there is a need for
risk stratification of LN metastasis.7 Therefore, we evaluated
the prognostic value of ENE in thyroid cancer patients.
MATERIALS AND METHODS
Data search and study selection
We performed a systematic search of MEDLINE (from incep-tion to June 2014) and EMBASE (from incepincep-tion to June 2014) for English-language publications using the keywords “thy-roid cancer”, “extranodal extension”, “lymph node”, “metastasis”, and “prognosis.” All searches were limited to human studies. The inclusion criteria were studies of thyroid cancer that re-ported the prognostic value of ENE in thyroid cancer. Reviews, abstracts, and editorial materials were excluded, and dupli-cate data were removed. Two authors performed the searches and screening independently, and resolved the discrepancies by consensus.
Data extraction and statistical analysis
Data were extracted from each publication independently by two reviewers, and the following information was recorded: first author, year of publication, country, definition of ENE, number of patients, and endpoints. The primary outcome was recurrence-free survival (RFS), and the secondary endpoint was disease-specific survival (DSS). Only deaths from disease were included in DSS.
The effects of ENE on survival were assessed using hazard ratios (HRs). Survival data were extracted following a published
methodology.9 A univariate HR estimate and 95% confidence
intervals (CIs) were extracted directly from each study, if pro-vided by the authors. Otherwise, p values of the log-rank tests, 95% CIs, numbers of events, and numbers of patients at risk were extracted to estimate the HR indirectly. Survival rates cal-culated from Kaplan-Meier curves were read using Engauge Digitizer version 3.0 (http://digitizer.sourceforge.net) to re-construct the HR estimate and its variance, assuming that pa-tients were censored at a constant rate during follow-up. An
HR >1 implies worse survival for patients with ENE, whereas an HR <1 implies a survival benefit for patients with ENE.
Het-erogeneity among studies was assessed using χ2 tests and I2
statistics, as described.10 Funnel plots were used to assess
pub-lication bias.11 Null hypotheses of no difference were rejected
if p-values were less than 0.05. Two authors reviewed each publication by the Cochrane risk of bias assessment tool (se-quence generation, allocation concealment, blinding,
incom-plete outcome data, selective outcome reporting).12 The data
from each study were analysed using Review Manager (Rev-Man, Version 5.2, Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012).
RESULTS
Study characteristics
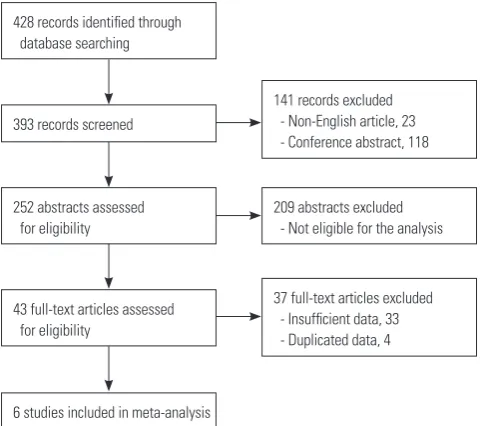
The electronic search identified 428 articles, non-English-lan-guage articles (n=23), and conference abstracts (n=118). Two hundred and nine studies that did not meet the inclusion cri-teria based on their title and abstract were excluded. After re-viewing the full text of 43 articles, six studies including 1830
patients were eligible for inclusion in the study (Table 1).13-18
[image:2.595.314.555.379.592.2]All studies were judged to have a low or unclear risk of bias in
Table 1. Studies Included in Meta-Analysis
Author Year of publication Country Institution Period Effect size Endpoints
Ganly, et al.13 2014 USA Memorial Sloan-Kettering Cancer Center 1985–2005 HR DSS
Wang, et al.17 2015 USA Memorial Sloan-Kettering Cancer Center 1986–2010 HR RFS
Ryu, et al.16 2014 Korea Asan Medical Center 2000–2006 HR RFS
Lee, et al.14 2015 Korea Asan Medical Center 2006–2010 HR RFS
Wu, et al.18 2015 USA University of California, San Francisco 1994–2004 HR DSS
Moritani15 2014 Japan Kusatsu General Hospital 1981–2008 HR DSS
[image:2.595.60.549.634.725.2]HR, hazard ratio; RFS, recurrence-free survival; DSS, disease-specific survival.
Fig. 1. Flowchart of the study selection process.
428 records identified through database searching
252 abstracts assessed for eligibility
209 abstracts excluded - Not eligible for the analysis
43 full-text articles assessed for eligibility
6 studies included in meta-analysis 393 records screened
141 records excluded - Non-English article, 23 - Conference abstract, 118
blinding of outcome assessment, incomplete outcome data, and selective reporting. The detailed procedure is shown in Fig. 1. Each of two studies from Memorial Sloan-Kettering
Can-cer Center13,17 and Asan Medical Center14,16 are included in this
meta-analysis. Although the studies from Memorial
Sloan-Ket-tering Cancer Center are duplicated, we extracted either DSS13
or RFS17 data from each study. In studies from Asan Medical
Center, each included patients of PTC with either N1a16 or N1b14
metastases. ENE was not defined in four studies;13,14,16,17
how-ever, studies by Wu, et al.18 and Moritani15 explained the
defini-tion of ENE. RFS data were extracted in three studies,14,16,17 those
of DSS in 3 studies.13,15,18 Visual inspection of the funnel plot
sug-gested no evidence of publication bias. Patient characteristics are summarized in Table 2.
Extranodal extension
Recurrence-free survival
All patients included in the meta-analysis had PTC. RFS was
analyzed based on three studies.14,16,17 Wang, et al.17 divided
their patients into two categories with patients of 45 or older (Wang 2015b) and those of less than 45 (Wang 2015a). The pooled HR for recurrence was 2.01 (95% CI 1.19–3.40, p=0.009),
and the test for heterogeneity gave no significant results (χ2=
3.26, p=0.35; I2=8%) (Fig. 2).
Disease-specific survival
DSS was analyzed based on three studies13,15,18 with 973
pa-tients. PTC patients with ENE were at 3.37-fold higher risk of death from the disease (95% CI 1.55–7.32, p=0.002), and the
test for heterogeneity gave no significant results (χ2=0.65,
p=0.72; I2=0%). The forest plots for DSS are shown in Fig. 3.
DISCUSSION
This meta-analysis evaluated the prognostic value of ENE in patients with thyroid cancer. In combined results, PTC patients with ENE had a 2.01-fold higher risk of recurrence and a 3.37-fold higher risk of death than those without ENE.
Differentiated thyroid carcinoma tends to recur in 30% of pa-tients, usually (in 66% of cases) within 10 years of initial
thera-py.19 Because prophylactic LN dissection is recommended and
performed frequently, it is not surprising that the number of cases of pathologically proven, but clinically inapparent, LN
metastasis is increasing.20 Neck LN metastases have increased
and are found in up to 70% of cases of PTC.21 Not all types of
nodal metastases have the same prognostic significance, and in particular, there is considerable controversy regarding the
clinical importance of the spectrum of nodal metastases.7 If
the clinician had information that would provide clues of the potential severity of those LNs, it could affect clinical decisions
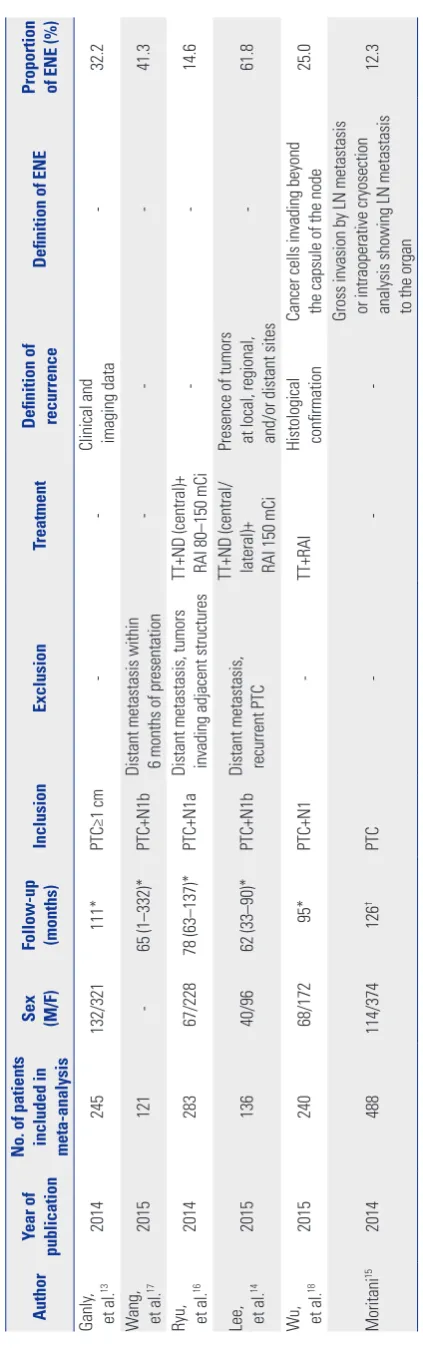
in primary treatment settings and when managing patients Table 2.
Patient Characteristics
Author
Year of
publication
No. of patients included in meta-analysis Sex (M/F) Follow-up (months)
Inclusion
Exclusion
Treatment
Definition of recurrence
Definition of ENE
Proportion of ENE (%)
Ganly , et al. 13 2014 245 132/321 111* PTC≥1 cm
-Clinical and imaging data
-32.2 W ang, et al. 17 2015 121 -65 (1–332)* PTC+N1b
Distant metastasis within 6 months of presentation
-41.3
Ryu, et al.
16 2014 283 67/228 78 (63–137)* PTC+N1a
Distant metastasis, tumors invading adjacent structures TT+ND (central)+ RAI 80–150 mCi
-14.6
Lee, et al.
14 2015 136 40/96 62 (33–90)* PTC+N1b
Distant metastasis, recurrent PTC TT+ND (central/ lateral)+ RAI 150 mCi Presence of tumors at local, regional, and/or distant sites
-61.8 W u, et al. 18 2015 240 68/172 95* PTC+N1 -TT+RAI
Histological confirmation Cancer cells invading beyond the capsule of the node
25.0 Moritani 15 2014 488 114/374 126 † PTC
-Gross invasion by LN metastasis or intraoperative cryosection analysis showing LN metastasis to the organ
12.3
PTC, papillary thyroid cancer; TT
, total thyroidectomy; ND, neck dissection; RAI, radioactive iodine ablation; LN, lymph node; ENE, extranodal extension.
*Median,
with recurrent nodal disease. Ideally, the clinician should be able to use available information regarding the primary tumor to understand the potential severity of metastatic LNs. Howev-er, virtually all of the current staging systems for differentiated thyroid cancer are based on the presence of positive LNs. Re-cent literature has focused on the importance of specific fea-tures of the nodal metastases, including size, number of
posi-tive nodes, and presence of ENE.7
ENE is an important predictor of outcome in other head and neck cancers and is accepted as an indication for additional
adjuvant therapy in squamous cell carcinoma.22 However,
re-search is limited on the effect of ENE on outcome in patients
with thyroid cancer. Wang, et al.17 noted that ENE was the LN
characteristic most prognostic of nodal recurrence within the central neck compartment. A retrospective review by Clain, et
al.8 found the presence of ENE as a surrogate for more
aggres-sive disease biology, and a strong association with minimal ETE. ENE is reported to diminish the probability of a biochemi-cal complete response after treatment for regional metastatic PTC, and increase the probability of tumor persistence after
initial resection, likely from abundant metastasis.3 Several
re-cent publications note that ENE is an indicator of poor
prog-nosis and survival.18,23 The development of ENE is presumably
a late event in the progression pathway for PTC,24 in contrast
to BRAF mutation (recognized as a marker of enhanced
po-tential for tumor invasion and metastasis25). In addition, ENE
is associated with large tumor size.17,26 The rate of ENE in PTC
patients was also higher with younger age, where there was a
higher number of central neck LN metastasis.26 ENE is believed
to be an independent manifestation of an aggressive thyroid
cancer rather than a direct relationship between LN size and
ENE.8 We proved, in accord with others, that the extent of ENE
is a risk factor for recurrence and disease-related death. Recur-rence is a stressful event for both patients and surgeons be-cause of the difficulty of reoperation along the previously
dis-sected planes, and high morbidity rates.27 Collectively, ENE
categorizes patients with PTC into prognostically distinct groups, suggesting that ENE should be considered in the initial assess-ment of recurrence. We suggest that radioiodine ablation should be considered in patients with ENE as an adjuvant therapy af-ter surgery. Furthermore, this prognostic effect of ENE has im-plications for the future update of the nodal classification of staging system.
This is the first study that meta-analyzed the prognostic val-ue of ENE. However, using ENE as a prognostic factor raises the concern about interobserver variability because of lack of
stringent criteria for the definition of ENE.24 In addition, some
institutions do not routinely report the presence of ENE. These issues need to be addressed in future studies. As the number of metastatic nodes detected depends on both the extent of LN dissection by the surgeons and the scrutiny of pathologists,
it may be less reliable than the examination for ENE,18 which
cannot be detected preoperatively by imaging modalities such as ultrasound or computed tomography.
[image:4.595.77.550.71.331.2]In conclusion, ENE should be considered a poor prognostic marker in thyroid cancer. This might help plan the radioactive iodine ablation and the disease monitoring.
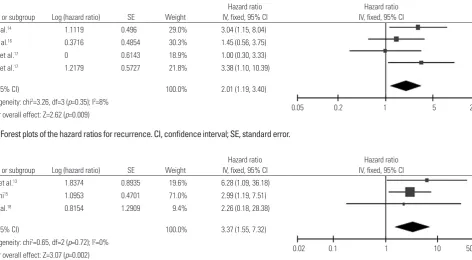
Fig. 2. Forest plots of the hazard ratios for recurrence. CI, confidence interval; SE, standard error.
Study or subgroup Log (hazard ratio) SE Weight
Hazard ratio IV, fixed, 95% CI
Hazard ratio IV, fixed, 95% CI Lee, et al.14 1.1119 0.496 29.0% 3.04 (1.15, 8.04)
Ryu, et al.16 0.3716 0.4854 30.3% 1.45 (0.56, 3.75)
Wang, et al.17 0 0.6143 18.9% 1.00 (0.30, 3.33)
Wang, et al.17 1.2179 0.5727 21.8% 3.38 (1.10, 10.39)
Total (95% CI) 100.0% 2.01 (1.19, 3.40)
Heterogeneity: chi2=3.26, df=3 (p=0.35); I2=8%
[image:4.595.59.554.76.195.2]Test for overall effect: Z=2.62 (p=0.009) 0.05 0.2 1 5 20
Fig. 3. Forest plots of hazard ratios for deaths from thyroid cancer. CI, confidence interval; SE, standard error.
Study or subgroup Log (hazard ratio) SE Weight
Hazard ratio IV, fixed, 95% CI
Hazard ratio IV, fixed, 95% CI Ganly, et al.13 1.8374 0.8935 19.6% 6.28 (1.09, 36.18)
Moritani15 1.0953 0.4701 71.0% 2.99 (1.19, 7.51) Wu, et al.18 0.8154 1.2909 9.4% 2.26 (0.18, 28.38)
Total (95% CI) 100.0% 3.37 (1.55, 7.32)
Heterogeneity: chi2=0.65, df=2 (p=0.72); I2=0%
ACKNOWLEDGEMENTS
This work was supported by Dong-A University research fund.
REFERENCES
1. Pellegriti G, Frasca F, Regalbuto C, Squatrito S, Vigneri R. World-wide increasing incidence of thyroid cancer: update on epidemiol-ogy and risk factors. J Cancer Epidemiol 2013;2013:965212. 2. Kweon SS, Shin MH, Chung IJ, Kim YJ, Choi JS. Thyroid cancer is
the most common cancer in women, based on the data from pop-ulation-based cancer registries, South Korea. Jpn J Clin Oncol 2013; 43:1039-46.
3. Lango M, Flieder D, Arrangoiz R, Veloski C, Yu JQ, Li T, et al. Extra-nodal extension of metastatic papillary thyroid carcinoma: correla-tion with biochemical endpoints, nodal persistence, and systemic disease progression. Thyroid 2013;23:1099-105.
4. Spires JR, Robbins KT, Luna MA, Byers RM. Metastatic papillary carcinoma of the thyroid: the significance of extranodal extension. Head Neck 1989;11:242-6.
5. Yamashita H, Noguchi S, Murakami N, Kawamoto H, Watanabe S. Extracapsular invasion of lymph node metastasis is an indicator of distant metastasis and poor prognosis in patients with thyroid pap-illary carcinoma. Cancer 1997;80:2268-72.
6. Yamashita H, Noguchi S, Murakami N, Toda M, Uchino S, Watanabe S, et al. Extracapsular invasion of lymph node metastasis. A good indicator of disease recurrence and poor prognosis in patients with thyroid microcarcinoma. Cancer 1999;86:842-9.
7. Randolph GW, Duh QY, Heller KS, LiVolsi VA, Mandel SJ, Steward DL, et al. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of ex-tranodal extension. Thyroid 2012;22:1144-52.
8. Clain JB, Scherl S, Dos Reis L, Turk A, Wenig BM, Mehra S, et al. Ex-trathyroidal extension predicts extranodal extension in patients with positive lymph nodes: an important association that may af-fect clinical management. Thyroid 2014;24:951-7.
9. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival end-points. Stat Med 1998;17:2815-34.
10. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring in-consistency in meta-analyses. BMJ 2003;327:557-60.
11. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629-34. 12. Higgins JP, Altman DG, Gøtzsche PC, Jøni P, Moher D, Oxman AD,
et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928.
13. Ganly I, Ibrahimpasic T, Rivera M, Nixon I, Palmer F, Patel SG, et al. Prognostic implications of papillary thyroid carcinoma with
tall-cell features. Thyroid 2014;24:662-70.
14. Lee CW, Roh JL, Gong G, Cho KJ, Choi SH, Nam SY, et al. Risk fac-tors for recurrence of papillary thyroid carcinoma with clinically node-positive lateral neck. Ann Surg Oncol 2015;22:117-24. 15. Moritani S. Impact of invasive extranodal extension on the
prog-nosis of patients with papillary thyroid carcinoma. Thyroid 2014; 24:1779-83.
16. Ryu IS, Song CI, Choi SH, Roh JL, Nam SY, Kim SY. Lymph node ra-tio of the central compartment is a significant predictor for locore-gional recurrence after prophylactic central neck dissection in patients with thyroid papillary carcinoma. Ann Surg Oncol 2014; 21:277-83.
17. Wang LY, Palmer FL, Nixon IJ, Tuttle RM, Shah JP, Patel SG, et al. Lateral neck lymph node characteristics prognostic of outcome in patients with clinically evident N1b papillary thyroid cancer. Ann Surg Oncol 2015;22:3530-6.
18. Wu MH, Shen WT, Gosnell J, Duh QY. Prognostic significance of extranodal extension of regional lymph node metastasis in papil-lary thyroid cancer. Head Neck 2015;37:1336-43.
19. Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med 1994;97:418-28.
20. American Thyroid Association (ATA) Guidelines Taskforce on Thy-roid Nodules and Differentiated ThyThy-roid Cancer, Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. Revised Ameri-can Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009; 19:1167-214.
21. Noguchi S, Noguchi A, Murakami N. Papillary carcinoma of the thyroid. I. Developing pattern of metastasis. Cancer 1970;26:1053-60. 22. Wang LY, Palmer FL, Nixon IJ, Thomas D, Shah JP, Patel SG, et al.
Central lymph node characteristics predictive of outcome in pa-tients with differentiated thyroid cancer. Thyroid 2014;24:1790-5. 23. Ito Y, Fukushima M, Tomoda C, Inoue H, Kihara M, Higashiyama T,
et al. Prognosis of patients with papillary thyroid carcinoma having clinically apparent metastasis to the lateral compartment. Endocr J 2009;56:759-66.
24. Ricarte-Filho J, Ganly I, Rivera M, Katabi N, Fu W, Shaha A, et al. Papillary thyroid carcinomas with cervical lymph node metasta-ses can be stratified into clinically relevant prognostic categories using oncogenic BRAF, the number of nodal metastases, and ex-tra-nodal extension. Thyroid 2012;22:575-84.
25. Pak K, Suh S, Kim SJ, Kim IJ. Prognostic value of genetic mutations in thyroid cancer: a meta-analysis. Thyroid 2015;25:63-70. 26. Lee YS, Lim YS, Lee JC, Wang SG, Kim IJ, Son SM, et al. Nodal status
of central lymph nodes as a negative prognostic factor for papil-lary thyroid carcinoma. J Surg Oncol 2013;107:777-82.