CrossMark
Published by DiscoverSys
ABSTRACT
Introduction: Depression is a chronic but curable disease that early diagnosis and treatment can lead to a higher life quality. A supplementary treatment such as exercise can reduce depressive symptoms. Tai Chi exercise is easy to learn and easy to do for older adults in nursing homes. This study investigated the effect of Tai Chi exercise on depressive symptoms in elderly residents at Sadeghieh Nursing Home.
Method & Material: This is a pre-test, post-test experimental study. Subjects included 62 elderly adults above 60 years of age who were randomly divided into four experimental subgroups and a control group. Participants were older adults who had not been participated any exercise activity during the previous month. The ten step Tai
Chi exercise performed three times per week for twelve weeks in experimental groups and a control group doing only their activity of daily living (ADL). The Beck Depression Inventory Second Edition (BDI-II) was used to assess depression.
Results: This study shows a statistically significant difference between depression mean scores in the experimental group compared to the control group (p < 0.01). After adjustment for the mean older adult`s age, the difference remained significant.
Conclusion: This study showed that Tai Chi exercise helps reduce depression in the older adult in residential homes. Social interactions through Tai Chi sessions and a sense of group belongingness may help reduce depression in older adults.
Key words: Tai Chi, Complementary Therapies, Older Adult, Depression
Cite This Article: Fakhari, M. 2017. Effects of Tai Chi exercise on depression in older adults: A randomized controlled trial. Bali Medical Journal 6(3): 679-683. DOI:10.15562/bmj.v6i3.706
Effects of Tai Chi exercise on depression in older
adults: A randomized controlled trial
Mohammad Fakhari*
INTRODUCTION
Alongside improvement of life quality and life expectancy, the population of the elderly is increas-ing. It is predicted that older adult will mount to
20% of the whole population in the U.S. by 2030.1
Old age is one of the most vulnerable stages of life. Aging and a sedentary lifestyle make the elderly susceptible to chronic health problems.2 Depression is a common factor causing disability or death in elderly.
Some older adult lives in a residential home. And residential homes should be well prepared for deal-ing with problems of this period. Approximately 50% of residents of nursing homes suffer from mild depression. The prevalence of mild depres-sion among the relatively healthy and active elderly
is higher than that of severe depression.3 Now,
depression is a curable disease; its early diagnosis and treatment can lead to a higher life quality. Yet, about 55% of the residents of nursing homes have not received any treatment.4
A supplementary treatment usually recom-mended for depression is exercise.5 It is an effi-cient and safe treatment for the less active elderly. However, due to weakness and fragility, older adults are not able to do any exercise.2 A useful and bear-able exercise in later life is Tai Chi.6 The Tai Chi is
a mind-body exercise which is both mental and physical effects.7 Since the Tai Chi exercise does not require any special tool, place, or condition, it could be done with more ease and comfort than other exercises.8 It has also been more adherence rate in long term practice of the elderly.9 However, Tai Chi, which is easy to learn and to do for older people, is more favorable with nursing home residents.10
The previous Meta-analysis showed Tai Chi exercise is effective to reduce depression in the older adult community.11 Another study showed patients with mild and moderate depression, who cope better with exercise therapy.12 Previous research has recommended conducting further research on Tai
Chi effects on homogeneous groups.11 There has
been very little convincing research on the effec-tiveness of Tai Chi exercise on residential home older adult depression. This study investigated the effect of Tai Chi exercise on depression in elderly residents at a Nursing Home.
MATERIALS AND METHODS
This was a pre-test, post-test experimental study conducted on two groups of older adults. The study population included all residents of Sadeghieh, Esfahan. Iran. This study had not been blinded.
Department of Medical Education, Medical Education Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
*Correspondence to: Mr. Mohammad Fakhari, Ph.D. student. Department of Medical Education, Medical Education Research Center, Isfahan University of Medical Sciences, Isfahan, Iran [email protected]
Received: 2017-06-26 Accepted: 2017-08-28 Published: 2017-09-1
Volume No.: 6
Issue: 3
First page No.: 679
P-ISSN.2089-1180
E-ISSN.2302-2914
All participants lived in the same condition and the same food menu. The inclusion criteria were old adults above 60 years of age who had not been having any exercise activity during the previous month, given written consent and were declared healthy enough to participate in the study by the residential home physician. While the elderly which absent in 5% of the exercise meetings consecutively or in 10% of meetings alternately were excluded.
Sampling
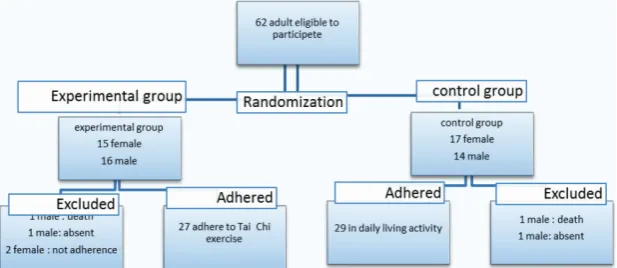
All older adults who gave written consent to participate in the study completed Beck II Inventory, and the qualified subjects were thus selected. In the next step, weight and height measurement was done, and demographic features were recorded. Next, they were examined by the residential home physician and those who were declared healthy enough entered the study. At the end 62 people ready to participate. The subjects were, then, randomly allocated to two groups by the random table. As many as 32 older adults allocated to the experimental group. They divided into four experimental subgroups where they received the intervention (Tai Chi exercise). Thirty older adults allocated in one group, with no special intervention (daily living activities only). In the course of the study, two subjects left the nursing home, and two also died, none of which was due to doing Tai Chi. No exercise injury occurred during the study. Study diagram showed in Figure 1.
Data Collection
The Beck Depression Inventory Second Edition (BDI-II), is a valid and reliable tool for determin-ing depression in older adults, with a Cronbach alpha coefficient of about 91 percent was used.13 It is a 21-item self-report tool to assess the existence and severity of symptoms of depression. Each item consists of 4 self-statements. The statements are assigned values of 0 to 3, with higher scores
indicating more severe symptom. On two items (16 and 17) there are seven options to indicate either an increase or decrease of appetite and sleep. All of the 21 items were summed to give a single score for the BDI-II.13 Beck Depression Inventory completed before the study and at the end of the study.
Intervention
Tai Chi exercise performed three times per week for twelve weeks in four experimental groups, while the control group is doing only their activity of daily living (ADL). The ten step Tai Chi exercise recommended by Wolf and colleagues suitable for the elderly adults over 50 had been used.14 We considered steps 9 and 10 of Tai Chi exercise were difficult to perform for an older adult in a residential home. To reduce the risk of falling or injury, only the qualified subjects (having physical strength and the trainer’s approval) were permitted to do steps 9 and 10. Tai Chi exercise sessions were progressively extended so that they took 20-25 minutes at the end of the first month.
Reliability of the Intervention
Two experienced trainers cooperated in the study. Subjects in the experimental group were divided into two male and two female groups. In each group, one trainer demonstrated Tai Chi move-ments while the other went over and guided the subjects, corrected them, and maintained harmony among them.
Data Analysis
Descriptive and inferential statistics were used for data analysis. Chi square test was applied for comparing ordinal variables. Independent and paired t-tests used for comparing nominal vari-ables. The significant value was set at p < 0.05.All statistical tests were done through IBM SPSS statis-tics Version 16.
RESULTS
Subjects included 62 elderly adults above 60 years of age who were randomly divided into experimen-tal and control groups. There was no significant difference between the subjects’ gender, the level of education, age, BMI, waist/hip ratio and pretest scores (table 1). The drop-out rate in the two groups was six subjects. Two male and four female subjects were excluded from the study due to not intend to participate.
Table 2 demonstrated the dependent variable of the study (total score on Beck II Inventory) in the two groups. It indicates that there was a statistically
significant decrease in depression mean scores on the post-test in the experimental group compared to pre-test assessment (p < 0.001). However, there was not so significant difference between the scores of the two groups after the intervention.
Table 3 showed no significant difference between two groups before the study, but at the end of the study, depression score in the experimental group was significantly decreased (p < 0.05). BDI-II total score revealed participant had mild to moderate depression before this study.
Table 4 tabulates mean differences of the groups before and after the intervention, which showed a statistically significant difference between depres-sion reduction rates in the experimental group compared to the control group (p < 0.01).
The one-way ANCOVA test was used to adjust the age of older adult as a covariance on the after intervention BDI-II total score. To examine the assumption of the covariance analysis, there was homogeneity of regression slopes and no inter-action between the age, and after intervention, BDI-II total score in the scatter plot and a moderate correlation between them (see figure 2).
Between-subjects effects in one-way ANOVA test was not significant for this interactive effect (F = 0.25, p = 0.61). Also, the Levene’s Test of Equality of Error Variances was not significant (F = 0.04, p = 0.83). The results of covariance analysis showed a significant difference between the two groups BDI-II total score by adjusting the mean age of older adults (Table 5). There was a slight relationship between the age and the after interven-tion BDI-II total score, as indicated by a partial eta squared value of 0.31.
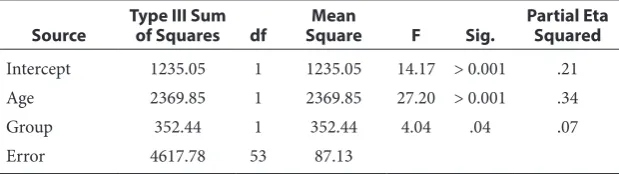
A repeated measure ANCOVA was conducted in which group was the fixed factor, age was a covariate, and the before intervention BDI-II scores (time1) and after intervention BDI-II scores (time2) were the repeated factors. There was a significant difference between groups by adjusting for age (F = 4.04, p = 0.04, partial eta square = 0.07). There was a strong relationship between the age and time, as indicated by a partial eta squared value of 0.34 (Table 6).
Table 1 Baseline characteristics of participant in experimental and control groups
Variable Experimental groupN=27 Control groupN=29 p value
Gender (male %) 51.9% 41.4% 0.605*
Age (mean ± SD) 69.19 ± 5.48 69.34 ± 5.03 0.910**
Education (illiterate %) 41.9% 51.6% 0.318***
Body mass index (mean ± SD) 23.63 ± 3.84 22.57 ± 3.63 0.295**
*Chi square test **Student t test ***Mann-Whitney U test
Table 2 Compare mean of BDI-II total score in each group before
and after intervention
BDI-II Total Score
Before Intervention (mean ± SD)
After Intervention
(mean ± SD) Paired t test df valuep Experimental
group 16.18 ± 8.27 13.33 ± 7.09 4.88 26 .001 Control group 18.55 ± 9.20 18.10 ± 8.08 1.25 28 0.219
Table 3 Compare mean of BDI-II total score between two groups
before and after intervention
BDI-II Total
Score Experimental group(n=27) group(n=29)Control T student test df valuep Before
intervention 16.18± 8.27 18.55 ± 9.20 -1.00 54 0.317 After
intervention 13.33± 7.09 18.10 ± 8.08 2.34 54 0.023
Table 4 Compare BDI-II total score mean difference between two
groups (paired t test)
Before
Intervention InterventionAfter Paired t test df p value Mean
difference 2.85 ± 3.03 0.44 ± 1.91 -3.56 54 0.001
Figure 2 General distribution and linear
DISCUSSION
This study investigated the effect of Tai Chi on depression in older adults. After adjusting the age of older adults, results indicated that Tai Chi exer-cises significantly reduce depression scores in the experimental group compared to control group.
Tai Chi exercise has multiple styles with different steps. In this study, we used the ten steps version of Tai Chi in which steps 9 and 10 had been excluded for some participants. Also, other studies used various questionnaires for measurement of depres-sion. We did not find any studies that used same Tai Chi exercise (with the same style, steps, length, and intensity) and same measurement tool. But our results are consistent with previous studies.15-18
The effectiveness of Tai Chi exercise in decrease depression may not relate to improving the fitness of older adult.19 It may be related to social interaction.17 The residents of a nursing house have constant interactions with each other; group work can increase their interaction and decrease their isolation.20 In group activities, there has also been an inverse relationship between social support and interpersonal conflicts and
depression rates.21 Social interactions through
Tai Chi sessions and a sense of group belonging-ness may help reduce depression in older adults. Although control group depression scores didn`t
statistically change, but observation of the activ-ities in the experimental group by control group participant may produce a feeling of loneliness and isolation in the control group, that could increase depression.
In order to make sure about similar diet, phys-ical activity, and medication consumption of the participant, researchers remained in close contact with older adult in both groups throughout the study. During these communications, participants shared memories, life experiences (including old age experiences), and their problems. This rela-tionship could also have had a role in depression reduction.22
We haven`t determined types of depression and only rely on BDI scores. Studies have shown seasonal depression is worsened in winter and improve in summer. There is a relation between exposure to sunlight in the warm seasons and intensity of seasonal depression.23 Since this study was conducted in spring, participants could receive more sunlight in April to July that possibly could have decreased depression in older adults with seasonal depression.
Low attrition rate may be related to the type of activity. Adherence to group exercise has also been higher than individual exercise. Compared to those with mild depression, people with moderate depres-sion have displayed stronger adherence to physical exercise. The high turnover rate of residents in the nursing home made difficulties in follow up to BDI test over six months.
Residential home physician permitted healthy older adult to participate in this study. The result of this study could generalize to healthy older adult that can perform exercise. Participants took pain-reliever and sleeping pills from nurses when if necessary. Drug consumption had not been recorded by nurses. Researchers were not able to have any control over that medication consump-tion. Considering that some of the pain-reliever and sleeping drugs could cause depression and some are anti-depressants, care should be taken to control the effects of drugs in further studies.
To study the effect of Tai Chi on depression in the elderly, further study is necessary. We recom-mended that medication consumption is moni-tored, the control and experimental groups are selected from different centers and the effect of Tai Chi on depression reduction be compared with that of group activities.
CONCLUSION
This study showed that Tai Chi exercise helps reduce depression in the older adult in residential homes.
Table 5 Analysis of covariance in after intervention BDI-II total
score
Source
Type III Sum of
Squares df SquareMean F Sig.
Partial Eta Squared Corrected
Model 1407.97a 2 703.98 16.03 > 0.001 0.38 Intercept 533.68 1 533.68 12.15 .001 0.19 Age 1055.74 1 1055.73 24.05 > 0.001 0.31 Group 333.55 1 333.55 7.60 .008 0.12 Error 2326.24 53 43.89
Total 19580.00 56 Corrected
Total 3734.21 55
a. R Squared = 0.38 (Adjusted R Squared = 0.35)
Table 6 summary of repeated measure ANCOVA model for
experimental and control groups by adjusting for age
Source Type III Sum of Squares df SquareMean F Sig. Partial Eta Squared Intercept 1235.05 1 1235.05 14.17 > 0.001 .21 Age 2369.85 1 2369.85 27.20 > 0.001 .34
Group 352.44 1 352.44 4.04 .04 .07
ACKNOWLEDGEMENT
I acknowledged the authorities, staff, exercise train-ers, and all the elderly of Sadeghiyeh residential home.
CONFLICT OF INTEREST
The authors declare no conflict of interest in this study.
REFERENCES
1. Velkoff VA, He W, Sengupta M, Velkoff V. 65+ in the United States: 2005. Washingaton, DC: National Institute of Aging, National Institutes of Health, US Dept of Health and Human Services. 2005.
2. Chen KM, Hsu YC, Chen WT, Tseng HF. Well‐being of institutionalized elders after Yang‐style Tai Chi practice. Journal of Clinical Nursing. 2007;16(5):845-52.
3. Parmelee PA, Katz IR, Lawton MP. Depression among institutionalized aged: assessment and prevalence estima-tion. Journal of Gerontology. 1989;44(1):M22-M9. 4. Brown MN, Lapane KL, Luisi AF. The management of
depression in older nursing home residents. Journal of the American Geriatrics Society. 2002;50(1):69-76.
5. Moquin B, Blackman MR, Mitty E, Flores S. Complementary and alternative medicine (CAM). Geriatric Nursing. 2009;30(3):196-203.
6. Lee LYK, Lee DTF, Woo J. Effect of Tai Chi on state self‐ esteem and health‐related quality of life in older Chinese residential care home residents. Journal of Clinical Nursing. 2007;16(8):1580-2.
7. Wang WC, Zhang AL, Rasmussen B, Lin LW, Dunning T, Kang SW, et al. The effect of Tai Chi on psychosocial well-being: a systematic review of randomized controlled trials. Journal of acupuncture and meridian studies. 2009;2(3):171-81.
8. Chen KM, Snyder M, Krichbaum K. Clinical use of tai chi in elderly populations. Geriatric Nursing. 2001;22(4):198-200.
9. Fisher KJ, Li F, Shirai M. Promoting health through Tai Chi: results from a controlled study. Calif J Health Promot. 2003;4:79-87.
10. Chen KM, Chen WT, Huang MF. Development of the simplified Tai Chi exercise program (STEP) for frail older adults. Complementary therapies in medicine. 2006;14(3):200-6.
11. Wang C, Bannuru R, Ramel J, Kupelnick B, Scott T, Schmid C. Tai Chi on psychological well-being: systematic review and meta-analysis. BMC complementary and alter-native medicine. 2010;10(1):23.
12. Blumenthal JA, Ong L. A commentary on ‘Exercise and Depression’(): And the verdict is…. Mental health and physical activity. 2009;2(2):97.
13. Kheirabadi GR, Maracy MR, Barekatain M, Salehi M, Sadri GH, Kelishadi M, et al. Risk factors of postpar-tum depression in rural areas of Isfahan Province, Iran. Archives of Iranian medicine. 2009;12(5):461-7.
14. Wolf SL, Coogler C, Xu T. Exploring the basis for Tai Chi Chuan as a therapeutic exercise approach. Archives of physical medicine and rehabilitation. 1997;78(8):886-92. 15. Chou K-L, Lee PW, Yu EC, Macfarlane D, Cheng Y-H,
Chan SS, et al. Effect of Tai Chi on depressive symptoms amongst Chinese older patients with depressive disorders: a randomized clinical trial. International journal of geriat-ric psychiatry. 2004;19(11):1105-7.
16. Frye B, Scheinthal S, Kemarskaya T, Pruchno R. Tai chi and low impact exercise: Effects on the physical function-ing and psychological well-befunction-ing of older people. Journal of Applied Gerontology. 2007;26(5):433-53.
17. Cho K. Effect of Tai Chi on depressive symptoms amongst Chinese older patients with major depression: the role of social support. 2008.
18. Redwine LS, Tsuang M, Rusiewicz A, Pandzic I, Cammarata S, Rutledge T, et al. A Pilot Study Exploring the Effects of a 12-Week T’ai Chi Intervention on Somatic Symptoms of Depression in Patients with Heart Failure. The Journal of Alternative and Complementary Medicine. 2012;18(8):744-8.
19. Arent S, Landers M. The Effects of Exercise on Mood in Older Adults: A Meta-Analytic. Journal of Ageing and Physical Activity. 2000;8:407-30.
20. Findlay RA. Interventions to reduce social isolation amongst older people: where is the evidence? Ageing and Society. 2003;23(5):647-58.
21. Strine TW, Kroenke K, Dhingra S, Balluz LS, Gonzalez O, Berry JT, et al. The Associations Between Depression, Health-Related Quality of Life, Social Support, Life Satisfaction, and Disability in Community-Dwelling US Adults. The Journal of Nervous and Mental Disease. 2009;197(1):61-4 10.1097/NMD.0b013e3181924ad8. 22. Lin YC, Dai YT, Hwang SL. The effect of reminiscence on
the elderly population: a systematic review. Public health nursing. 2003;20(4):297-306.
23. Praschak-Rieder N, Willeit M, Sitte H, Meyer JH, Kasper S. FC29-05 - Season, sunlight, and brain serotonin function. European Psychiatry. 2011;26, Supplement 1(0):1981.