K
ENJIO
GAWA, K
AZUHIKOY
OSHIMATSUCyclooxygenase II
– A Role in Gastric Cancer Treatment
Rola cyklooksygenazy w leczeniu raka żołądka
Department of Surgery, Tokyo Women’s Medical University Medical Center East, Japan
Adv Clin Exp Med 2007, 16, 3, 347–352 ISSN 1230−025X
EDITORIAL
Since epidemiological studies reported that long−term users of non−steroidal anti−inflammato− ry drugs (NSAIDs) would develop colon and gas− tric cancer less frequently [1, 2], a large amount of studies on a relationship between a target enzyme of NSAIDs, cyclooxygenase (COX) or prostaglan− din (PG, especially PGE2) and cancer development
has been reported. Especially for COX−2 whose expression is induced in inflammation and tumor, the expressional status in various types of carcino− ma was established [3], and it attracts a lot of attention as a target molecule for chemoprevention and treatment of cancer. This review describes a role of COX−2 in gastric cancer and the potential clinical use of a COX−2 inhibitor.
Enhanced PGE
2Production
and Its Role in Tumor Tissue
Production of some PGs particularly PGE2in−
creases in gastrointestinal cancer, especially colon
cancer. Particularly, PGE2 production enhances
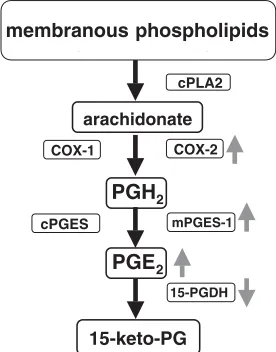
[4]. PGE2is converted from a membrane phospho−
lipid to arachidonate under cytosolic phospholi− pase A2 (cPLA2) effect, as are other PGs. Sub−
sequently, it is converted to PGH2by COX−1 or
COX−2, and further converted to PGE2by prosta−
glandin E synthase (PGES). Among the kinds of PGES that are already discovered, analyses of microsomal PGES−1 (mPGES−1) which is indu− cible type and cytosolic PGES (cPGES) which constitutively express are reported. Interestingly, cPGES and COX−1, mPGES−1 and COX−2 are functionally coupled [5, 6]. In tumor tissue, PGH2
produced excessively by COX−2 could be effi− ciently converted to PGE2by mPGES−1 (Fig. 1),
and overexpression of COX−2 and mPGES−1 in various cancers has been reported (Tables 1, 2) [7–18].
Regarding carcinogenesis, although the effect by genetic change has been analyzed, the effect of PGE2produced in tumor tissue (tumor and stroma)
is still unknown on tumor cell proliferation. In
© Copyright by Silesian Piasts University of Medicine in Wrocław
Abstract
Recent studies have demonstrated that increased amount of prostaglandin E2(PGE2) produced by overexpression
of cyclooxygenase−2 (COX−2)/microsomal PGE synthase−1 (mPGES−1) is involved in tumor proliferation. Furthermore, relationships with epidermal growth factor (EGF)/mitogen activated protein (MAP) kinase signal pathway related to cell proliferation and Akt/protein kinase B (PKB) related to resistance of apoptosis are being clarified. Association of COX−2 with gastric cancer has not been established as clearly as in colon cancer. However, increased expression of COX−2 in gastric cancer was confirmed, and in cell culture or animal models, influence of COX−2 on tumor proliferation was indicated. Thus, the usefulness of COX−2 inhibitor in treatment has been demonstrated. However, in precancerous lesions of gastric cancer, COX−2 expression is controversial and the use− fulness of COX−2 inhibitor has not been demonstrated. Further studies about COX−2 and gastric cancer including clinical trials are needed, and also more studies should be performed about other PGE2related enzymes as well as
COX−2 (Adv Clin Exp Med 2007, 16, 3, 347–352).
a study using COX−2 knockout mice, COX−2 expression was involved in microvessel density in tumor tissue, and this resulted in decreased tumor proliferation [19]. It was also shown that COX−2 and mPGES−1−derived PGE2were associated with
angiogensis via EP2 [20, 21].
On the other hand, relationship between PGE2
and epidermal growth factor (EGF)−mitogen acti− vated protein (MAP) kinase signal pathway relat− ed to tumor proliferation has been recently report− ed. PGE2promotes release of transforming growth
factor−α (TGF−α), a ligand of EGF receptor (EGFR), and activates extracellular regulated MAP kinase2 (ERK2). After oral administration of PGE2to rats, phosphorylation of EGFR and ERK2
in mucosal epithelium was observed [22].
Cultured models confirmed that high and con− comitant expression of COX−2 and mPGES−1 increased cell proliferation activity and led to mor− phologic change, and showed tumorigenecity in
Fig. 1. Cascade of PGE2metabolism in premaliganat
and malignant tissue. PGH2produced excessively by
COX−2 could be efficiently converted to PGE2by
mPGES−1. Enhanced PGE2is maintained due to
decreased ability of PGE2metabolism by down−regu−
lated 15−PGDH
COX−2
mPGES−1
PGE2
cPLA2
membranous phospholipids
PGH2
arachidonate
15−keto−PG
15−PGDH COX−1
cPGES
Table 1. COX−2 expression in premalignant and malignant tissue
Organ Premalignancy Malignancy
Head and neck leukoplakia squamous cell carcinoma
Esophagus Barrett’s esophagus adenocarcinoma
squamous cell dysplasia squamous cell carcinoma
Stomach metaplasia adenocarcinoma
Colon adenoma adenocarcinoma
Liver chronic hepatitis hepatocellular carcinoma
Biliary System bile duct hyperplasia cholangiocarcinoma
adenocarcinoma of gall bladder Pancreas pancreatic intraepithelial neoplasia adenocarcinoma
Breast ductal carcinoma−in−situ adenocarcinoma
Lung atypical adenomatous hyperplasia adenocarcinoma
squamous cell carcinoma
Bladder dysplasia transitional cell carcinoma
squamous cell carcinoma Gynecologic cervical intraepithelial neoplasia squamous cell carcinoma
adenocarcinoma of cervix endometrial carcinoma
Penis penile intraepithelial neoplasia squamous cell carcinoma
Skin actinic keratoses squamous cell carcinoma
Table 2. mPGES−1 expression in premalignant and malignant tissue
Organ Premalignancy Malignancy
Head and neck leukoplakia squamous cell carcinoma
Esophagus (rat) Barrett’s esophagus squamous cell dysplasia
Stomach intestinal type adenocarcinoma
Colon adenoma adenocarcinoma
Biliary System cholangiocarcinoma
adenocarcinoma of gall bladder
Breast ductal carcinoma−in−situ adenocarcinoma
Lung tobacco smoke exposed adenocarcinoma
epithelial fibroblast squamous cell carcinoma
Bladder (rat) papilloma transitional cell carcinoma
Gynecologic adenocarcinoma of cervix
nude mice [23]. In transgenic mice in which these genes expressed in gastric mucosa, PGE2produc−
tion was enhanced and abnormal differentiation was observed. At 48 weeks old, hyperplastic tumor without dysplasia was also observed [24]. PGE2 produced excessively by COX−2 and
mPGES−1 is very important for in vivocell prolif− eration but insufficient for malignant change. A study using similar models showed that Wnt sig− nal, that played an important role in development of colon cancer, had importance also in develop− ment of gastric cancer (25).
COX−2 Expression
in Gastric Cancer
Recent epidemiological investigation reported that there were few mortalities from gastric cancer in aspirin users [26]. And also described that occurrence of gastric cancer decreased in long− term users of NSAIDs [27].
In gastric cancer as in various other cancers, COX−2 overexpressed [28]. The expression of COX−2 was mainly observed in tumor cells, but expression was also observed in stromal cells and macrophages. The COX−2 expression in gastric precancerous lesion was shown in intestinal meta− plasia and dysplasia [29, 30]. A comparison study between before and after Helicobacter pylori (H. pylori) eradication reported that COX−2 express− ion level decreased in epithelium and stroma after eradication, but that there was no change in intesti− nal metaplasia [31]. In the progression process of gastric mucosa to dysplasia and cancer, increased expression of COX−2 was observed [32]. In gastric adenoma, up−regulated COX−2 protein was detect− ed in stromal cells [33]. This indicates that COX− 2−derived PGE2 is associated with cell prolifera−
tion as in COX−2/mPGES−1 transgenic mice men− tioned above. Thus, further studies are needed to elucidate how COX−2 may be associated with genetic change in carcinogenesis in stomach that has not been clarified as well as in colon cancer. Recent reports confirmed p53 accumulation in all adenoma patients examined and indicated that 50% of the patients showed overexpression of COX−2. The same results were also found in gas− tric cancer; they demonstrated that the process of cancer development is different between gastric and colon cancer [34].
Regarding the clinicopathological findings and COX−2 expression in gastric cancer, various reports are provided. No relationship between COX−2 expression and age or gender was report− ed. The lower expression of COX−2 in cardiac gas− tric cancer was reported [35], and this supports the
data indicating that epidemiologically aspirin−use could not prevent cancer related death in patients with cardiac cancer. However, there are no other reports on difference in COX−2 expression by location thereafter. As for histological type and COX−2 expression, some reports showed a higher COX−2 expression in intestinal type [36–38], but no difference in another report [39]. Similarly, there is no consensus on the relationship between COX−2 expression and tumor depth, venous or lymphatic invasion, metastasis or stage [40–42]. Since most studies on association with prognosis were based on univariate analysis [43], further investigation using a large amount of clinical data such as meta−analysis are needed to clarify whether it can be an independent prognostic factor.
Potential of COX−2
Inhibitor in Gastric
Cancer Treatment
Using culture model, a COX−2 inhibitor, nimesulide inhibited proliferation of MKN−45 cells, and telomerase activity through blocking Akt/protein kinase B (PKB) pathway [44]. In SGC7901 cells, genetic or pharmacological inhibi− tion of COX−2 reduceded PGE2production. This
resulted that migration and tube formation of HUVEC and in vivoangiogenesis were also inhib− ited [45]. It was indicated that inhibited COX−2 prevented neovascularization related to gastric cancer. In xenograft model using MKN−45 and nude mice, another COX−2 inhibitor, NS398, inhibited tumor growth. NS398 administration decreased PGE2and PGF1αlevels in the tumor tis−
sue. In tumor cells, decreased bromodeoxyuridine (BrdU) index and increased apoptotic index were observed [46]. In other study using OCUM−2M, scirrhous type gastric cancer cell, and NF−21, gas− tric fibroblast, JTE−522, a COX−2 inhibitor, inhib− ited NF−21 proliferation but did not inhibit OCUM−2M proliferation. However, in xenograft model, the COX−2 inhibitor did not show a growth inhibition against OCUM−2M alone inoculated tumor but in contrast decreased the size of tumor inoculated with both of OCUM−2M and NF−21. In the tumor tissue, inhibited Ki67 and increased apoptosis were observed, and keratinocyte growth factor (KGF) production from NF−21 was decreased. In scirrhous type gastric cancer, it was demonstrated that COX−2 inhibitor controlled rel− evance to stromal cell proliferation [47]. In chem− ical carcinogenesis rat model, the COX−2 inhibitor, cerecoxib also reduced the incidence of gastric cancer and tumor volume [48].
ical effects of COX−2 inhibitor from the view of gastric cancer prevention. Although H. pylori carri− ers showed a high level of PGE2in gastric mucosa,
their PGE2 level, gastritis score and proliferation
indices were not improved after 2−week administra− tion of 25 mg, b.i.d. rofecoxib, a COX−2 inhibitor [49]. From another observation of rofecoxib admin− istration for 2 years, there was no difference in regression of intestinal metaplasia considered to be a precancerous lesion of gastric cancer, and COX−2 inhibitor could not return intestinal metaplasia of gastric mucosa to normal [50]. From these results, gastric cancer prevention should now be focused on H. pylori eradication. However, serum interleukin−8 (IL−8), tumor necrosis factor−α(TNF−α), progastrin and gastrin level were decreased in observation before and after administration of 25 mg, b.i.d. rofe− coxib for 2 weeks in gastric cancer patients. In addi− tion, the expression level of BAX and caspase−3 increased, and the expression level of Bcl−2 and sur− vivin decreased [51]. From these data, the above animal experiments and in vitroresults, it is expect− ed that a COX−2 inhibitor could be useful for gas− tric cancer treatment, and a large clinical trial must be needed.
Conclusion
and Further Directions
Considering the relationship of COX−2 in development of gastric cancer, the effect of COX− 2 inhibitor in gastric cancer treatment could be hopeful. However, there are not only results show− ing prospective effect but also various concerns. Also in results of large scale clinical trial of COX− 2 inhibitor administration for patients with colon polyps including familial adenomatous polyp, increase in cardiovascular events, adverse effects of COX−2 inhibitor, were reported [52–54], and careful attention will be needed to ensure the safe− ty of long−term use. It is expected that further investigation will be performed into what relation− ship exists between gastric cancer and regulation of mPGES−1 that draws attention in colon cancer [7], or 15−prostaglandin dehydrogenase (15− PGDH), a catabolic enzyme of PGE2(Fig. 1) [55,
56]. Besides, we hope the studies in the future that the control of these enzymes can prevent or treat gastric cancer.
References
[1] Thun MJ, Namboodiri MM, Calle EE, Flanders WD, Heath CW Jr.:Aspirin use and risk of fatal cancer. Cancer Res 1993, 53, 1322–1327.
[2] Langman MJ, Cheng KK, Gilman EA, Lancashire RJ:Effect of anti−inflammatory drugs on overall risk of common cancer: case−control study in general practice research database. BMJ 2000, 320, 1642–1646.
[3] Dannenberg AJ, Altorki NK, Boyle JO, Dang C, Howe LR, Weksler BB, Subbaramaiah KCyclo−oxygenase 2: a pharmacological target for the prevention of cancer. Lancet Oncol 2001, 2, 544–551.
[4] Rigas B, Goldman IS, Levine L:Altered eicosanoid levels in human colon cancer. J Lab Clin Med 1993, 122, 518–522.
[5] Tanioka T, Nakatani Y, Semmyo N, Murakami M, Kudo I:Molecular identification of cytosolic prostaglandin E2 synthase that is functionally coupled with cyclooxygenase−1 in immediate prostaglandin E2 biosynthesis. J Biol Chem 2000, 275, 32775–32782.
[6] Murakami M, Naraba H, Tanioka T, Semmyo N, Nakatani Y, Kojima F, Ikeda T, Fueki M, Ueno A, Oh S, Kudo I:Regulation of prostaglandin E2 biosynthesis by inducible membrane−associated prostaglandin E2 syn− thase that acts in concert with cyclooxygenase−2. J Biol Chem 2000, 275, 32783–32792.
[7] Yoshimatsu K, Golijanin D, Paty PB, Soslow RA, Jakobsson PJ, DeLellis RA, Subbaramaiah K, Dannenberg AJ: Inducible microsomal prostaglandin E synthase is overexpressed in colorectal adenomas and cancer. Clin Cancer Res 2001, 7, 3971–3976.
[8] Yoshimatsu K, Altorki NK, Golijanin D, Zhang F, Jakobsson PJ, Dannenberg AJ, Subbaramaiah K:Inducible prostaglandin E synthase is overexpressed in non−small cell lung cancer. Clin Cancer Res 2001, 7, 2669–2674.
[9] Cohen EG, Almahmeed T, Du B, Golijanin D, Boyle JO, Soslow RA, Subbaramaiah K., Dannenberg, AJ:
Microsomal prostaglandin E synthase−1 is overexpressed in head and neck squamous cell carcinoma. Clin Cancer Res 2003, 9, 3425–3430.
[10] Jang TJ:Expression of proteins related to prostaglandin E2 biosynthesis is increased in human gastric cancer and during gastric carcinogenesis. Virchows. Arch. 2004, 445, 564–571.
[11] Mehrotra S, Morimiya A, Agarwal B, Konger R, Badve S:Microsomal prostaglandin E (2) synthase−1 in breast cancer: a potential target for therapy. J Pathol 2006, 208, 356–363.
[12] Golijanin D, Tan JY, Kazior A, Cohen EG, Russo P, Dalbagni G, Auborn KJ, Subbaramaiah K, Dannenberg AJ:Cyclooxygenase−2 and microsomal prostaglandin E synthase−1 are overexpressed in squamous cell carcinoma of the penis. Clin. Cance.r Res. 2004, 10, 1024–1031.
[14] Van Rees BP, Sivula A, Thoren S, Yokozaki H, Jakobsson PJ, Offerhaus GJA, Ristimaki A:Expression of microsomal prostaglandin E synthase−1 in intestinal type gastric adenocarcinoma and in gastric cancer cell lines. Int J Cancer 2003, 107, 551–556.
[15] Mehrotra S, Morimiya A, Agarwal B, Konger R, Badve S:Microsomal prostaglandin E2 synthase−1 in breast cancer: a potential target for therapy J Pathol 2006, 208, 356–363.
[16] Martey CA, Baglole CJ, Gasiewicz TA, Sime PJ, Phipps RP:The aryl hydrocarbon receptor is a regulator of cigarette smoke induction of the cyclooxygenase and prostaglandin pathways in human lung fibroblasts Am J Physiol Lung Cell Mol Physiol 2005, 289, L391–L399.
[17] Shi Y, Cui L, Dai G, Chen J, Pan H, Song L, Cheng S, Wang X:Elevated prostaglandin E2 level via cPLA2− COX−2−mPGES−1 pathway involved in bladder carcinogenesis induced by terephthalic acid−calculi in Wistar rat. Prostaglandins Leukot Essent Fatty Acids 2006, 74, 309–315.
[18] Rask K, Zhu Y, Wang W, Hedin L, Sundfeldt K:Ovarian epithelial cancer: a role for PGE2−synthesis and sig− nalling in malignant transformation and progression. Mol Cancer 2006, 5, 62.
[19] Williams CS, Tsujii M, Reese J, Dey SK, DuBois RN:Host cyclooxygenase−2 modulates carcinoma growth. J Clin Invest 2000, 105, 1589–1594.
[20] Seno H, Oshima M, Ishikawa TO, Oshima H, Takaku K, Chiba T, Narumiya S, Taketo MM:
Cyclooxygenase 2− and prostaglandin E(2) receptor EP(2)−dependent angiogenesis in Apc(Delta716) mouse intestinal polyps. Cancer Res 2002, 62, 506–511.
[21] Sonoshita M, Takaku K, Sasaki N, Sugimoto Y, Ushikubi F, Narumiya S, Oshima M, Taketo MM:
Acceleration of intestinal polyposis through prostaglandin receptor EP2 in Apc(Delta 716) knockout mice. Nat Med 2001, 7, 1048–1051.
[22] Pai R, Soreghan B, Szabo IL, Pavelka M, Baatar D, Tarnawski AS:Prostaglandin E2 transactivates EGF receptor: a novel mechanism for promoting colon cancer growth and gastrointestinal hypertrophy. Nat Med 2002, 8, 289–293.
[23] Kamei D, Murakami M, Nakatani Y, Ishikawa Y, Ishii T, Kudo I:Potential role of microsomal prostaglandin E synthase−1 in tumorigenesis. J Biol Chem 2003, 278, 19396–19405.
[24] Oshima H, Oshima M, Inaba K, Taketo MM:Hyperplastic gastric tumors induced by activated macrophages in COX−2/mPGES−1 transgenic mice. EMBO J 2004, 23, 1669–1678.
[25] Oshima H, Matsunaga A, Fujimura T, Tsukamoto T, Taketo MM, Oshima M:Carcinogenesis in mouse stom− ach by simultaneous activation of the Wnt signaling and prostaglandin E2 pathway. Gastroenterology. 2006, 131, 1086–1095.
[26] Thun MJ, Namboodiri MM, Calle EE, Flanders WD, Heath CW Jr.: Aspirin use and risk of fatal cancer. Cancer Res 1993, 53, 1322–1327.
[27] Langman MJ, Cheng KK, Gilman EA, Lancashire RJ:Effect of anti−inflammatory drugs on overall risk of common cancer: case−control study in general practice research database. BMJ. 2000, 320, 1642–1646.
[28] Ristimaki A, Honkanen N, Jankala H, Sipponen P, Harkonen M:Expression of cyclooxygenase−2 in human gastric carcinoma. Cancer Res 1997, 57, 1276–1280.
[29] Yamagata R, Shimoyama T, Fukuda S, Yoshimura T, Tanaka M, Munakata A:Cyclooxygenase−2 expression is increased in early intestinal−type gastric cancer and gastric mucosa with intestinal metaplasia. Eur J Gastroenterol Hepatol 2002, 14, 359–363.
[30] Li HX, Chang XM, Song ZJ, He SX:Correlation between expression of cyclooxygenase−2 and angiogenesis in human gastric adenocarcinoma. World J Gastroenterol 2003, 9, 674–677.
[31] Sung JJ, Leung WK, Go MY, To KF, Cheng AS, Ng EK, Chan FK: Cyclooxygenase−2 expression in Helicobacter pylori−associated premalignant and malignant gastric lesions. Am J Pathol 2000, 157, 729–735.
[32] van Rees BP, Saukkonen K, Ristimaki A, Polkowski W, Tytgat GN, Drillenburg P, Offerhaus GJ:
Cyclooxygenase−2 expression during carcinogenesis in the human stomach. J Pathol 2002, 196, 171–179.
[33] Tatsuguchi A, Sakamoto C:COX−2 and gastric cancer Cancer Fronteer 2004, 16, 29–34 (in Japanese).
[34] Smith GV, Feakins R, Farthing MJG, Ballinger A:Cyclooxygenase 2, p53, b−catenin, and APC protein expres− sion in gastric adenomatous polyp. Am J Clin Pathol 2005, 123, 415–420.
[35] Ratnasinghe D, Tangrea JA, Roth MJ, Dawsey SM, Anver M, Kasprzak BA, Hu N, Wang QH, Taylor PR:
Expression of cyclooxygenase−2 in human adenocarcinomas of the gastric cardia and corpus. Oncol Rep 1999, 6, 965–968.
[36] Yamagata R, Shimoyama T, Fukuda S, Yoshimura T, Tanaka M, Munakata A:Cyclooxygenase−2 expression is increased in early intestinal−type gastric cancer and gastric mucosa with intestinal metaplasia. Eur J Gastroenterol Hepatol 2002, 14, 359–363.
[37] Saukkonen K, Nieminen O, van Rees B, Vilkki S, Harkonen M, Juhola M, Mecklin JP, Sipponen P, Ristimaki A:Expression of cyclooxygenase−2 in dysplasia of the stomach and in intestinal−type gastric adeno− carcinoma. Clin Cancer Res. 2001, 7, 1923–31.
[38] Joo YE, Oh WT, Rew JS, Park CS, Choi SK, Kim SJ:Cyclooxygenase−2 expression is associated with well− differentiated and intestinal−type pathways in gastric carcinogenesis. Digestion 2002, 66, 222–229.
[39] Lim HY, Joo HJ, Choi JH, Yi JW, Yang MS, Cho DY, Kim HS, Nam DK, Lee KB, Kim HC:Increased expres− sion of cyclooxygenase−2 protein in human gastric carcinoma. Clin Cancer Res 2000, 6, 519–525.
[40] Yamamoto H, Itoh F, Fukushima H, Hinoda Y, Imai K:Overexpression of cyclooxygenase−2 protein is less frequent in gastric cancers with microsatellite instability. Int J Cancer 1999, 84, 400–403.
[42] Kawabe A, Shimada Y, Uchida S, Maeda M, Yamasaki S, Kato M, Hashimoto Y, Ohshio G, Matsumoto M, Imamura M:Expression of cyclooxygenase−2 in primary and remnant gastric carcinoma: comparing it with p53 accumulation, Helicobacter pylori infection, and vascular endothelial growth factor expression. J Surg Oncol 2002, 80, 79–88.
[43] Leung WK, To KF, Ng YP, Lee TL, Lau JY, Chan FK, Ng EK, Chung SC, Sung JJ:Association between cyclo−oxygenase−2 overexpression and missense p53 mutations in gastric cancer. Br J Cancer 2001, 84, 335–339.
[44] Baoping Y, Guoyong H, Jieping Y, Zongxue R, Hesheng L:Cyclooxygenase−2 inhibitor nimesulide suppress− es telomerase activity by blocking Akt/PKB activation in gastric cancer cell line. Dig Dis Sci 2004, 49, 948–953.
[45] Fu YG, Sung JJ, Wu KC, Wu HP, Yu J, Chan M, Chan VY, Chan KK, Fan DM, Leung WK:Inhibition of gastric cancer−associated angiogenesis by antisense COX−2 transfectants. Cancer Lett 2005, 224, 243–252.
[46] Sawaoka H, Kawano S, Tsuji S, Tsujii M, Gunawan ES, Takei Y, Nagano K, Hori M:Cyclooxygenase−2 inhibitors suppress the growth of gastric cancer xenografts via induction of apoptosis in nude mice. Am J Physiol. 1998, 274, G1061–G1067.
[47] Yashiro M, Nakazawa K, Tendo M, Kosaka K, Shinto O, Hirakawa K:Selective cyclooxygenase−2 inhibitor downregulates the paracrine epithelial−mesenchymal interactions of growth in scirrhous gastric carcinoma. Int J Cancer 2007, 120, 686–693.
[48] Hu PJ, Yu J, Zeng ZR, Leung WK, Lin HL, Tang BD, Bai AH, Sung JJ:Chemoprevention of gastric cancer by celecoxib in rats. Gut 2004, 53, 195–200.
[49] Kim TI, Lee YC, Lee KH, Han JH, Chon CY, Moon YM, Kang JK, Park IS:Effects of nonsteroidal anti− inflammatory drugs on Helicobacter pylori−infected gastric mucosae of mice: apoptosis, cell proliferation, and inflammatory activity. Infect Immun 2001, 69, 5056–5063.
[50] Leung WK, Ng EK, Chan FK, Chan WY, Chan KF, Auyeung AC, Lam CC, Lau JY, Sung JJ:Effects of long−term rofecoxib on gastric intestinal metaplasia: results of a randomized controlled trial. Clin Cancer Res 2006, 12, 4766–4772.
[51] Konturek PC, Konturek SJ, Bielanski W, Kania J, Zuchowicz M, Hartwich A, Rehfeld JF, Hahn EG:
Influence of COX−2 inhibition by rofecoxib on serum and tumor progastrin and gastrin levels and expression of PPARgamma and apoptosis−related proteins in gastric cancer patients. Dig Dis Sci 2003, 48, 2005–2017.
[52] Bertagolli MM, Eagle CJ, Zauber AG, Redston M, Solomon SD, Kim KM, Tang J, Rosenstein RB, Wittes J, Corle D, Hess TM, Woloj M, Boisserie F, Anderson WF, Viner JL, Bagheri D, Burn J, Chung DC, Dewar T, Foley TR, Hoffman N, Macrae F, Pruitt RE, Saltzman JR, Salzberg B, Sylwestrowicz T, Gordon GB, Hawk ET:Celecoxib for the prevention of sporadic colorectal adenomas. N Engl J Med 2006, 355, 873–884.
[53] Arber N, Eagle CJ, Spicak J, Racz I, Dite P, Hajer J, Zavoral M, Lechuga MJ, Gerletti P, Tang J, Rosenstein RB, Macdonald K, Bhadra P, Fowler R, Wittes J, Zauber AG, Solomon SD, Levin B: PreSAP Trial Investigators Celecoxib for the prevention of colorectal adenomatous polyps. N Engl J Med 2006, 355, 885–895.
[54] Baron JA, Sandler RS, Bresalier RS, Quan H, Riddell R, Lanas A, Bolognese JA, Oxenius B, Horgan K, Loftus S, Morton DG:APPROVe Trial Investigators. A randomized trial of rofecoxib for the chemoprevention of colorectal adenomas. Gastroenterology 2006, 131, 1674–1682.
[55] Backlund MG, Mann JR, Holla VR, Buchanan FG, Tai HH, Musiek ES, Milne GL, Katkuri S, DuBois RN:
15−Hydroxyprostaglandin dehydrogenase is down−regulated in colorectal cancer. J Biol Chem 2005, 280, 3217–3223.
[56] Myung SJ, Rerko RM, Yan M, Platzer P, Guda K, Dotson A, Lawrence E, Dannenberg AJ, Lovgren AK, Luo G, Pretlow TP, Newman RA, Willis J, Dawson D, Markowitz SD:15−Hydroxyprostaglandin dehydroge− nase is an in vivo suppressor of colon tumorigenesis. Proc Natl Acad Sci USA 2006, 103, 12098–12102.
Address for correspondence:
Kenji Ogawa
Department of Surgery
Tokyo Women’s Medical University Medical Center East 2−1−10 Nishiogu, Arakawaku, Tokyo
116−8567, Japan Tel.: +81−3−3810−1111
E−mail: [email protected]
Conflict of interest: None declared