2018 International Conference on Computer, Communication and Network Technology (CCNT 2018) ISBN: 978-1-60595-561-2
MCI Conversion Prediction Based on Transfer Learning
Lan LIN
1,2,*and Bai-wen ZHANG
1,2,*1
The Alzheimer’s Disease Neuroimaging Initiative (ADNI) 2
College of Life Science and Bioengineering, Beijing University of Technology, Beijing, China
*Corresponding author
Keywords: Alzheimer’s disease (AD), Mild cognitive impairment (MCI), Transfer learning, Deep learning.
Abstract. Amnestic mild cognitive impairment (MCI) commonly represents an intermediate stage situated in the spectrum between normal age-related cognitive decline and dementia. Predicting of MCI conversion to Alzheimer’s Disease (AD) plays critical roles in early diagnosis and disease-modifying therapies. We analyzed baseline 3T MRI scans in 337 MCI patients from the ADNI-GO and ANDI-2 cohorts. The subjects were divided into MCI non-converters (MCInc) and MCI converters (MCIc). To evaluate conversion rates, we aim to first extract intermediate representations of structural MRI (sMRI) by a pre-trained convolutional neural network (CNN) model, then combine principal component analysis (PCA) and sequential feature selection (SFS) for feature selection, and finally adopt support vector machine (SVM) for prediction. The method attained an accuracy of 77.58%, a sensitivity of 90.48%, a specificity of 76.42%, which may be useful and practical for clinical diagnosis.
Introduction
Alzheimer’s disease (AD) is one of the most severe age related neurodegenerative disease, accompanying by brain structural and functional changes. In 2007, approximately 26.6 million people over 60 were diagnosed with AD, and it is expected to grow fourfold by 2050. The early diagnosis of AD is necessary to slow down the disease progression and decrease socioecomic burden. Neuropathological and neuroimaging evidences [1,2] suggest that AD occurs decades before the onset of symptoms. Patients with mild cognitive impairment (MCI), specifically those with “amnestic MCI”, is associated with a higher risk of developing AD, with a conversion rate of approximately 15% per year [3]. MCI, as an intermediate cognitive state between normal aging and diseased, can possibly predict the onset of AD. However, MCI patients is very heterogeneous, as some develop AD, some may remain stable over time, or revert to a normal cognitive state. Based upon follow-up diagnosis status, MCI patients can be divided into two subgroups: MCI patients who have converted to AD (MCI converters (MCIc)), and MCI patients who have not converted to AD (MCI non-converters (MCInc)). One promising biomarkers of early AD is structural changes measured by structural MRI (sMRI), a lot of efforts have been made to establish biomarkers using to predict the onset of AD at the MCI stage [4-6] with sMRI. The development of tools to detect those who are more likely to convert from MCI to AD is important for timely therapy and possible slow AD pathology progression.
for weeks, which is not feasible for the majority of neuroimaging studies. One approach to overcome this problem is the transfer learning. This is the process of recognizing and applying knowledge and skills learned from source task to a new target task (Figure 1).
Figure 1. Use of a CNN pretrained on images from a different domain to extractor features from MRI, followed by construction of a model to predict MCI conversion.
This study set out with the aim of exploiting the transfer learning idea into learning invariant and more transferable feature from MRI, which can be applied to classify MCI patients as MCIc or MCInc. In the following Section we first introduce the proposed method, then report the results of this study, and finally discuss the results and conclude the paper.
Materials and Methods
Data
The data used in the preparation of this article were obtained from the Alzheimer's Disease Neuroimaging Initiative [9] (ADNI) Grand Opportunity (ADNI-GO) and ADNI-2 studies (http://adni.loni.usc.edu). ADNI participants of this study include 337 MCI patients, whose baseline examinations had been downloaded. The demographic characteristics of the selected study population are summarized in Table 1.The structural MRI data were collected according to the ADNI acquisition protocol using 3T scanners at multiple sites across the United States and Canada. MRI protocols ensured comparability across a variety of scanners (GE, Siemens or Philips).
Table 1. Demographic characteristics of the studied dataset.
Group Number Age Gender(Male/Female) MMSE CDR
MCIc 61 72.0±5.5 28/33 26.5± 1.6 0.5± 0.21
MCInc 276 71.5± 6.3 141/135 27.6 ±1.4 0.49 ±0.22
MRI Data Processing
[image:2.612.91.516.521.569.2]Features From CaffeNet
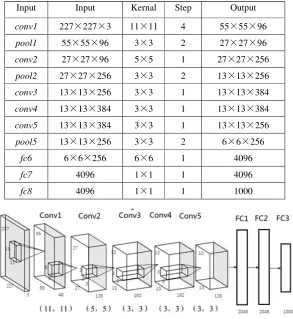
In this study, we used the CaffeNet architecture, an adaptation of AlexNet, which differs in training without any data augmentation and exchanging the form of subsample and normalization layers. The architecture of the CaffeNet is shown in Figure 2. Based on the role they accomplish, CaffeNet is split into two parts. The first part is responsible for feature learning, which is comprised of five convolutional layers; while the second part encloses three fully-connected layers with an output layer of 1000 neurons for classification. The detail parameters of CaffeNet are listed on Table 2. Features extraction was based on Caffe [11], an efficient framework that is exploited by Berkeley Vision and Learning Center (BVLC). The intermediate layers capture features that are neither too specific to the dataset the network was originally trained on, nor too general to not contain any representative information from images. Features from conv3, conv4 and conv5 of the CaffeNet were extracted. For
the conv3 and conv4 which do not have a pooling layer followed, we performed overlapping
[image:3.612.162.451.279.605.2]max-pooling within 3 × 3 regions and step size of 2 to get the final feature vectors. Features from 65 slices of each subjects were concatenated together to form the feature representation of the subject.
Table 2. Network parameters of CaffeNet.
Input Input Kernal Step Output
conv1 227×227×3 11×11 4 55×55×96
pool1 55×55×96 3×3 2 27×27×96
conv2 27×27×96 5×5 1 27×27×256
pool2 27×27×256 3×3 2 13×13×256
conv3 13×13×256 3×3 1 13×13×384
conv4 13×13×384 3×3 1 13×13×384
conv5 13×13×384 3×3 1 13×13×256
pool5 13×13×256 3×3 2 6×6×256
fc6 6×6×256 6×6 1 4096
fc7 4096 1×1 1 4096
fc8 4096 1×1 1 1000
Figure 2. Network Structure.
Feature Selection and SVM Classification
[image:3.612.161.454.280.599.2]selected features (p = 20) is much fewer than the total PCs (M = 429). 40 subjects from each group were randomly selected as the training set, the rest is the testing set. In this investigation, SVM implementation was taken from the LibSVM toolkit[13].
Results
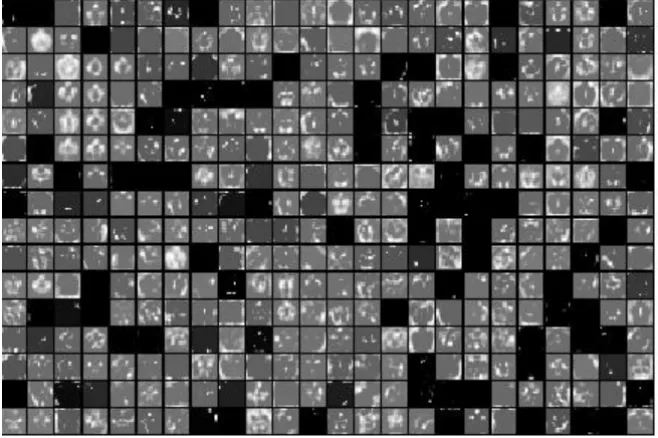
We examined the performance of different layers for predicting MCI to AD conversion. The results indicate that the best performance was obtained using features extracted from the conv3 layer. The
[image:4.612.146.475.189.408.2]activation map of the conv3 layer is shown in Figure 3.
Figure 3. Activations (features) of Conv3 using MRI data were displayed for a given subject.
The performance of the proposed method is evaluated by comparing the following metrics: True Positive (TP), True Negative (TN), False Positive (FP), False Negative (FN), sensitivity(SEN) , specificity(SPE) and Accuracy (ACC). Results from conv3 is given in Tables 3.
Table 3. Classification of MCIc Versus MCInc based on features from the conv3 layer.
TP FP TN FN ACC % SEN% SPE%
19 2 188 58 77.58 90.48 76.42
Discussion
We present a study here of 337 MCI patients from the ADNI cohort. A transfer learning framework was proposed by making use of CNN pretrained on image data from a different domain. The approach to accomplish this generally consists of two stages. In the first stage, features are extracted from the MRIs by transfer learning and in the second stage these features are used as predictors for predicting MCI conversion. Since training a CNN from scratch requires huge amounts of data, the use of pretrained CaffeNet provides a potentially attractive approach. The results showed that the proposed method could offer consistently and substantially performance, with an overall classification accuracy of 77.58% for recognizing MCIc and MCInc patients. MCI conversion status could be predicted reliably by use of a CNN pretrained on non-medical images. These results also suggest that CaffeNet may yield good results in other neuroimaging studies.
been scaled from a real number to eight bits integer which might cause information loss. It is interesting to extend our current method for dealing with the real number of data for further improvement of performance. Third, one limitation in the use of CNNs is the inability to confidently dissect the mechanisms through which the conclusions are drawn. Filter visualisation may be a valuable area to help the researchers to better understand and improve models.
Acknowledgement
This research was financially supported by the Scientific Research General Project of Beijing Munici pal Education Committee (KM201810005033).
References
[1]C. Jin, L. Lin, Z. Fu et al. Research advances of magnetic resonance imaging in Alzheimer's disease, Smart Healthcare, 1(1) (2015) 52-56.
[2]L. Lin, Z. Fu, X. Xu et al. Mouse brain magnetic resonance microscopy: Applications in Alzheimer disease, Microsc Res Tech. 78(5) (2015) 416-24.
[3]R. Brookmeyer, E. Johnson, K. Ziegler-Graham, et al, Forecasting the global burden of Alzheimer’s disease, Alzheimers Dement. 3(3) (2007) 186-191.
[4]S. F. Eskildsen, P. Coupé, D. García-Lorenzo, et al, Prediction of Alzheimer's disease in subjects with mild cognitive impairment from the ADNI cohort using patterns of cortical thinning, Neuroimage. 65 (2013) 511-521.
[5]Y. Cho, J. K. Seong, Y. Jeong, et al, Individual subject classification for Alzheimer's disease based on incremental learning using a spatial frequency representation of cortical thickness data, Neuroimage. 59(3) (2012) 2217-2230.
[6]R. Cuingnet, E. Gerardin, J. Tessieras, et al, Automatic classification of patients with Alzheimer's disease from structural MRI: a comparison of ten methods using the ADNI database, Neuroimage. 56(2) (2011) 766-781.
[7]M. Tian, L. Lin, B. Zhang, et al. Study on the Application of Deep Learning in Neuroimaging, China Medical Devices. 12 (2016) 4-9.
[8]A. Krizhevsky, I. Sutskever, G.E. Hinton, ImageNet classification with deep convolutional neural networks, International Conference on Neural Information Processing Systems. Curran Associates Inc. (2012) 1097-1105.
[9]M.W. Weiner, D.P. Veitch, P.S. Aisen, et al, The Alzheimer's Disease Neuroimaging Initiative: a review of papers published since its inception, Alzheimer's & dementia. 9(5) (2013) e111-e194.
[10]J. Ashburner, A fast diffeomorphic image registration algorithm, Neuroimage. 38(1) (2007) 95-113.
[11]Y. Jia, E. Shelhamer, J. Donahue, et al, Caffe: Convolutional architecture for fast feature embedding, Proceedings of the 22nd ACM international conference on Multimedia, ACM, 2014, 675-678.
[12]H. Hotelling, Analysis of a complex of statistical variables into principal components, Journal of educational psychology. 24(6) (1933) 417-441.