0095-1137/06/$08.00⫹0 doi:10.1128/JCM.02521-05
Copyright © 2006, American Society for Microbiology. All Rights Reserved.
Use of Seroconversion Panels To Estimate Delay in Detection of
Anti-Human Immunodeficiency Virus Antibodies by
Enzyme-Linked Immunosorbent Assay of Pooled
Compared to Singleton Serum Samples
Lena Novack,
1Noya Galai,
2,3Arieh Yaari,
4Mordechai Orgel,
4Eilat Shinar,
5and Batia Sarov
1*
Department of Epidemiology, Ben-Gurion University of the Negev, Beer-Sheba, Israel1; Department of Statistics, Haifa University,
Haifa, Israel2; Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland3;
Hepatitis Laboratory, Soroka University Medical Center, Beer-Sheva, Israel4; and Blood Services Center,
Magen David Adom in Israel, Tel Hashomer, Israel5
Received 5 December 2005/Returned for modification 6 February 2006/Accepted 26 May 2006
The transfusion of unsafe blood worldwide accounts for 5 to 15% of new human immunodeficiency virus (HIV) infections, most of which occur in sub-Saharan Africa. While developed countries now apply PCR testing of pooled samples, some developing countries still do not have universal screening policies. More efficient low-cost procedures for the screening of pooled samples have the potential to encourage mass screening efforts in resource-poor settings. The aim of this study was to estimate the delay in the detection of HIV antibodies in pooled serum samples compared to that in singleton serum samples by enzyme-linked immunosorbent assay (ELISA) and to evaluate the risk of transfusion-transmitted HIV infection during the window period. Serial blood samples obtained from five HIV seroconversion panels were mixed with HIV-seronegative blood samples to create pools of 6, 12, 16, 24, 32, and 48 samples. The delay in detection of the first anti-HIV antibody-positive sample in tests with pooled samples was calculated for each pool size and compared to that obtained by testing of singleton samples and statistically evaluated by a robust log-linear regression analysis. The risk of a false-negative (FN) result caused by dilution was estimated by use of the incidence risk/window period model. The additional risk of transmission related to ELISA screening of pooled samples for HIV did not exceed 9% of the current risk of an FN result (estimated to be 1/1,067,000). The countries with virus prevalence rates in donors of less than 15% are expected to save up to 30% in the number of tests. ELISA screening of pooled samples could be considered in settings where the testing of blood supplies for HIV is not routinely done.
Transfusion of unsafe blood worldwide accounts for 5 to 15% (13, 16, 26, 27) of the 80,000 to 160,000 new human immunodeficiency virus (HIV) infections each year (according to a World Health Organization [WHO] assessment [18, 29], 70% of these new cases occur in sub-Saharan Africa).
Universal screening of blood donations in developing coun-tries, as is successfully performed in industrialized councoun-tries, could significantly prevent HIV transfusion-related transmis-sion. Efforts to decrease the risk of HIV-infected blood trans-fusions resulted in an impressive drop in risk, ranging from 1:500,000 donations to 1:1,067,000 donations (8). Unfortu-nately, the situation in developing countries is far from being that successful. While industrialized countries are on their way to converting the method of routine screening for anti-HIV antibodies to nucleic acid tests (NATs), not every health care system in a developing country can afford the simple and rel-atively inexpensive antibody-based assay as a routine test for all blood donations (11, 25, 27). The assay used is usually the enzyme-linked immunosorbent assay (ELISA), designed for the detection of antibodies in serum and characterized by high levels of analytical sensitivity and specificity (approaching 100% for verified HIV-positive samples) (7). Two additional
advantages of ELISA over the NATs are its comparatively low cost (about $4 to $5 per individual test) and the logistical simplicity of application for widespread screening. The only important disadvantage of this test is a relatively long serocon-version window period (21 to 22 days, on average) (4, 10) compared to the 11-day-long window period for NATs (10).
Screening for HIV in serum pools, that is, simultaneous testing of multiple blood donations, could significantly reduce the cost of the screening procedure by reducing the number of tests needed. This approach could present a realistic solution for countries which are currently performing only partial screening of blood donations, if any (1, 7, 11, 21, 23, 25, 27).
Screening of serum pools for HIV was studied in the past. In 1989, two groups of researchers, Kline et al. (15) and Cahoon-Young et al. (5), came to the conclusion that testing for anti-HIV antibodies in pool sizes of 10 (5, 15) and 15 (15) with an immunoassay kit does not reduce the sensitivity of the screen-ing procedure, when sscreen-ingleton testscreen-ing is assumed to be the “gold standard.” These experiments were performed with sam-ples which had been found to be positive for anti-HIV antibody by testing of singleton samples. To the best of our knowledge, the blood samples obtained during the seroconversion window period were never tested in pools. Although the findings from previous studies showed no decrease in sensitivity when diluted anti-HIV antibody-positive samples were tested, this cannot be applied directly to blood units donated by recent
seroconvert-* Corresponding author. Mailing address: Department of Epidemi-ology and Health Services Evaluation, Ben-Gurion University of the Negev, P.O. Box 653, Beer-Sheva 84105, Israel. Phone: (972-8) 647-7448. Fax: (972-8) 647-7638. E-mail: [email protected].
2909
on May 16, 2020 by guest
http://jcm.asm.org/
ers. These samples are frequently referred to as “weak posi-tives,” due to their low ELISA readings, and, therefore, are vulnerable to any dilution. If this is true, pooled screening has the potential to extend the window period. Additional risk due to the window period arises if developing countries are con-sidered. In these epidemic regions, an increased risk of trans-fusion-transmitted HIV is expected, as shown by mathematical prediction (19).
This study aimed to (i) estimate the possible delay of anti-HIV antibody detection in pools by ELISA testing of serocon-version panels and (ii) to estimate the risk of HIV transfusion-transmitted infection if serum samples are tested in pools compared to that if singleton serum samples are tested during the window phase.
MATERIALS AND METHODS
Materials. Five HIV seroconversion panels were used (panels PRB929A, PRB924, PRB951, PRB952, and PRB959; Boston Biomedica Inc. [BBI]) and were purchased from the BBI 1999–2001 catalog. The panels included six to nine blood samples which were taken in the time interval of a minimum of 16 days to a maximum of 40 days since the first blood sample was obtained.
These panels provide a series of blood samples taken before and after sero-conversion. The anti-HIV antibody-negative samples used for the assembly of the pools were obtained from the routine work of the Magen David Adom Blood Services. The tubes with panel blood samples and the anti-HIV antibody-nega-tive samples used for dilution were kept at⫺70°C.
Pooling and testing procedures.Pooling was performed manually. Blood sam-ples from all bleeding days present in each HIV seroconversion panel were added to pools with 6, 12, 16, 24, 32, and 48 serum samples. Each pool contained 1 sample from the panel and 24 different negative samples in the volumes that corresponded to the required pool sizes for the study. Considering that testing of pooled samples has the best potential for implementation in small laboratory setups, the testing was performed with Axsym and IMx machines (Abbott Lab-oratories), which are frequently used in small laboratories. These two machines are identical in their technical performance characteristics, with the exception that Axsym is an almost automatic device and IMx is managed manually. For each seroconversion sample, testing was performed for both singleton and pooled samples and was repeated in duplicate. The sample/cutoff ratio (S/CO) level used in this analysis was equal to 0.8.
Accuracy and risk evaluation.For each pool size and each seroconversion panel, the delay in the time to detection of the first anti-HIV antibody-positive sample for testing of pooled samples was compared to that for testing of single-ton samples.
A log-linear robust regression analysis was performed to obtain a statistical estimate of the delay in the time to detection of anti-HIV antibodies in pooled samples compared to that in singleton samples in terms of the 95% confidence interval (CI) by using all datum points available. The model assumed that the log of the S/CO value was a quadratic function of the time since seroconversion. Robust estimates of the variance adjusted for possible correlations among mea-surements for a specific seroconversion panel. The estimated delay time was established when the predicted S/CO value crossed the threshold value of 0.8. The data were analyzed by using the STATA 8 package. The estimate of the delay obtained was modified into the risk of a false-negative (FN) result caused by dilution. This calculation was based on the incidence risk/window period model (12). The reference estimate of the risk of transmitting an HIV infection associated with the use of blood from a donation was the evaluation made for the American Red Cross screening data by Dodd et al. (8). According to their findings, the risk of transfusion transmission of the virus in the case of a single ELISA screening for HIV is 1:1,067,000.
The applicability of the pooling method was assessed by computing the relative savings obtained from implementing screening in different pool sizes. The cal-culation was done as follows: expected percentage of tests saved⫽[(number of samples in pool⫺expected number of tests in pooling procedure)/number of samples in pool]⫻100, where the expected number of tests in the pool was calculated on the basis of a binomial distribution with the parameters Binom-(number of samples in pool, prevalence) multiplied by (1⫺specificity).
In subsequent analyses, the overall cost differential for the cost of testing of pooled samples compared to the cost of testing of singleton samples was calcu-lated, assuming prevalence rates as reported for some countries, where screening
of pooled samples was found to be beneficial in terms of the “expected percent-age of tests saved.” The rates of seroprevalence of HIV in the general population were used as the upper limit of the HIV prevalence in the donor population, since the rate in the general population is generally considered higher than that in donors. For instance, in Zimbabwe, the prevalence rates in the general and the donor populations were estimated by WHO to be 25.8% and 0.7% to 2.3%, respectively (9).
We also assumed that the approximate cost of one ELISA is $4.80 (22) and that the equipment, labor, and other overhead expenses needed to conduct screening of pooled samples do not exceed the expenditures for the procedure with singleton samples. The total annual savings from screening of pooled sam-ples can be assessed by multiplying the number of units collected annually by the expected percent savings per unit, multiplied by the cost of one test.
We further estimated the overall number of HIV infections prevented by screening of pooled samples compared to the number prevented by incomplete screening of singleton samples. This computation was carried out as follows: the estimated proportion of new HIV infections due to transfusion of an infected blood unit was assumed to be 5 to 15% (13, 16, 27) for the African countries and 2.01% for India (3), given the present number of blood units screened (and assuming that HIV screening is performed partially). The increase in the number of units tested by a factor ofXis supposed to reduce the number of new infections by the same factorX(assuming that this relationship is linear).
The estimate of the prevalence of a virus in a donor population is the most restricting factor in such an analysis and, therefore, needed special attention. The seroprevalence in the donor population in developing countries ranges from 2 to 10%, and is frequently based on nonverified data (6, 9, 20). Taking into account the high degree of accuracy of an ELISA with a singleton samples and the relatively high prevalence of HIV, the prevalence based on verified rates is expected to be close to the reported values, and therefore, the latter are used in the current analysis of the applicability of the method.
This study was approved by the local institutional review board (IRB no. 03826).
RESULTS
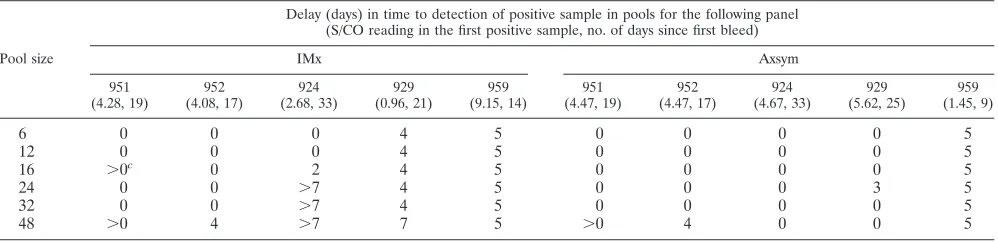
The results of ELISA testing for anti-HIV antibodies in pooled samples of five seroconversion panels are summarized in Table 1. Table 1 shows the time interval (in days) between the first day that a positive ELISA result was obtained for a single sample and the bleeding day with a positive result for each pool size. This time interval is actually the delay in the time to detection of a positive sample caused by testing of a sample in a pool instead of testing of a more concentrated singleton sample. The results are based on the average of duplicate ELISAs.
According to the data presented in Table 1, we can conclude that pools of 6 and 12 samples are associated with a maximum delay of 5 days in detecting the first positive sample (see panel 959 for pools 6 and 12 samples). Larger pools (consisting of 16, 24, 32, and 48 samples) cause delays of 0, 4, 5, and 7 days (and even more than 7 days, which is assigned a value of⬎7 in Table 1), respectively, compared with the delay encountered by test-ing of a stest-ingleton sample.
Table 2 shows the delay in the time to detection of the first positive sample (with 95% confidence intervals estimated by regression analysis) and the risk of infection transmission due to screening of pools. Thus, if the window period increases by 5%, then the risk of transmission of the infection via a blood donation is expected to grow by the same percentage.
The findings shown in Table 2 indicate that, as expected, the delay in the time to detection of the first positive sample increased with the pool size. For all pools with equal to or less than 24 samples, the upper limit of the confidence interval of the estimated time to delay of detection of a positive pool did not exceed 2 days.
The additional risk of HIV transmission caused by screening
on May 16, 2020 by guest
http://jcm.asm.org/
of samples in pools compared to that by screening of a single-ton sample did not exceed 9% of the current risk of an FN result (equal to 1/1,067,000). On the basis of a comparison of the 95% CIs around the estimated risk of transmission calcu-lated for the Axsym and the IMx systems, these two systems are characterized by statistically different parameters of safety. Nevertheless, both of them achieve an extremely low level of a risk of transmission, so that even for pools with 48 samples, the estimate of the risk is less than 0.00000110. The report of the risk of transfusion-transmitted HIV for developing countries is very high and inaccurate (28). The relative increase in the window period obtained in this study (maximum of 9%) can be applied directly to the risk of an FN result because the donor is in the seroconversion stage, whenever a reliable estimate is reported.
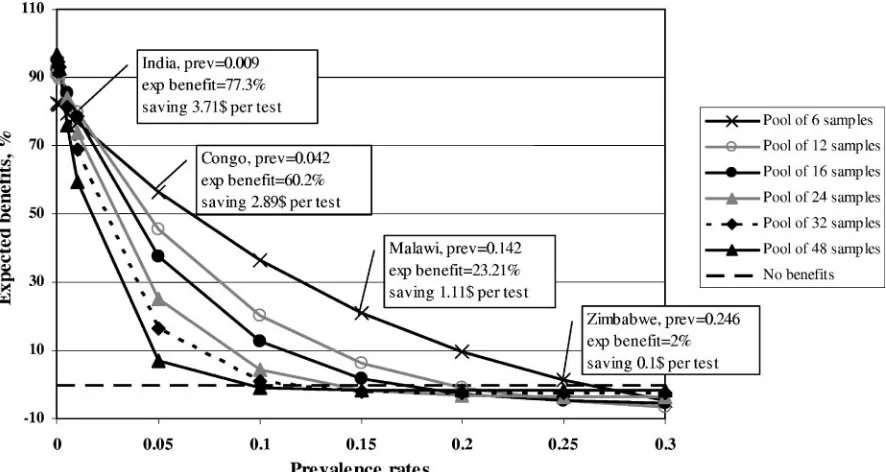
Figure 1 shows the results of the calculation of the relative savings in the numbers of tests, by pool size, obtained by screening of pooled samples compared to that by regular screening of singleton samples. The prevalence rates appear to be the main limiting factor for obtaining benefits from the pooled screening method. This limitation is mostly evident in the context of large pools, due to the increased probability that they containing at least one infected donation. Therefore, smaller pools are expected to gain higher benefits. According to the data in Fig. 1, in order to save at least 10 to 30% in the number of tests by testing pools of 6 to 12 samples, the prev-alence rate in the donor population should not exceed 15/100. This is relevant to many countries, such as Malawi, the population
of which has a seroprevalence of 10.7% (6); the Democratic Republic of Congo, the population of which has a seroprevalence of 6.4% (20); Zimbabwe, the population of which has a sero-prevalence of 2.1%, as reported in 1988 (9); and India, the pop-ulation of which has a seroprevalence of 0.06% (14).
The following provides a calculation of the expected savings in the regions cited above. Here we used the more updated data provided by WHO and the Avert organization regarding the prevalence rates of HIV positivity in the general popula-tion in 2003 for the countries menpopula-tioned above (2, 3). Thus, the maximum seroprevalence rates in Malawi, Congo, Zimbabwe, and India are assumed to be 14.2%, 4.2%, 24.6%, and 0.9%, respectively. The expected savings per test in these countries by performing screening of pools of six samples instead of single-ton samples are $1.11 (Malawi), $2.89 (Congo), $0.10 (Zimba-bwe), and $3.71 (India). Despite the worst scenario analyzed here, the benefit even in Zimbabwe remained positive. If we perform a brief sensitivity analysis of the HIV seroprevalence rates and slightly adjust them to obtain a rate for the blood donor population by artificially decreasing the prevalence rates by a factor of 5, the estimates of savings for one test will be $3.21, $3.73, $2.72, and $3.91, respectively, in the same coun-tries.
[image:3.585.44.543.90.211.2]The total annual estimated savings obtained by screening samples in pools for India, where 158 blood banks are known to annually collect and test about 1,028,000 blood units (31), might amount to (1,028,000⫻0.7732⫻$4.8)⫽$3,815,278. In
TABLE 1. Delay in time to detection of the first positive pooled sample in seroconversion panelsacompared to the time
to detection of the first positive samplebin singleton testing for anti-HIV antibodies by ELISA
Pool size
Delay (days) in time to detection of positive sample in pools for the following panel (S/CO reading in the first positive sample, no. of days since first bleed)
IMx Axsym
951 (4.28, 19)
952 (4.08, 17)
924 (2.68, 33)
929 (0.96, 21)
959 (9.15, 14)
951 (4.47, 19)
952 (4.47, 17)
924 (4.67, 33)
929 (5.62, 25)
959 (1.45, 9)
6 0 0 0 4 5 0 0 0 0 5
12 0 0 0 4 5 0 0 0 0 5
16 ⬎0c 0 2 4 5 0 0 0 0 5
24 0 0 ⬎7 4 5 0 0 0 3 5
32 0 0 ⬎7 4 5 0 0 0 0 5
48 ⬎0 4 ⬎7 7 5 ⬎0 4 0 0 5
aThe panels used in the experiments were PRB929A, PRB924, PRB951, PRB952, and PRB959 (BBI 1999–2001 catalog). bThe threshold for a positive sample is an S/CO value of 0.8.
cThe delays listed with a greater than symbol (⬎) denote that in that specific pool size, a positive sample was not detected at all, but the delay is expected to be higher
[image:3.585.45.541.617.709.2]than the stated number of days.
TABLE 2. Estimated delay in detecting anti-HIV antibodies by testing of pooled samples and singleton samples by ELISAawith two types
of equipment and different pool sizes, with 95% CIs and the risk of transmitting HIV infection for screening of pools
Pool size Estimated time delay (days关95% CI兴) Estimated additional risk of HIV transfusion
b
(95% CI)
Axsym IMx Axsym IMx
6 0 (0; 0.31) 0.05 (0; 0.48) 1/1,067,000 (1/1,067,000; 1/1,051,231) 1/1,064,466 (1/1,067,000;1/1,043,156) 12 0.19 (0; 0.46) 1.36 (0.88; 1.84) 1/1,057,482 (1/1,067,000; 1/1,044,031) 1/1,002,102 (1/1,024,086;1/981,042) 16 0.75 (0.65; 0.85) 1.80 (1.36; 2.23) 1/1,029,922 (1/1,034,917; 1/1,025,961) 1/982,763 (1/1,002,102; 1/964,571) 24 1.14 (1.05; 1.22) 1.54 (1.07; 2.00) 1/1012,334 (1/1016,190; 1/1,008,416) 1/994,099 (1/1,015,270;1/974,217) 32 1.31 (1.19; 2.43) 2.92 (2.42; 3.42) 1/1,004,348 (1/1,009,779; 1/956,338) 1/936,747 (1/956,746; 1/915,568) 48 1.93 (1.68; 2.19) 3.06 (2.56; 3.56) 1/977,191 (1/987,963; 1/966,235) 1/931,297 (1/951,061; 1/912,337)
aThe threshold for a positive sample is an S/CO value of 0.8.
bThe window period used for calculation of the risk of transmission is 3 weeks (21 days).
on May 16, 2020 by guest
http://jcm.asm.org/
all, India has 449 blood banks (30), and therefore, the overall national benefit is expected to be significantly higher.
The reduction in the number of new infections is expected to be proportionate to the increased benefits. This kind of calcu-lation is more relevant for Africa, where screening for HIV is frequently partial and we can potentially increase the number of tested units. For instance, if the benefits expected for the entire continent are as in Malawi and equal 0.232 for each blood unit (Fig. 1), then the number of blood units tested can increase by a factor of 1.3 [1/(1 ⫺ 0.232)], which in turn is expected to decrease the current proportion of transfusion-transmitted HIV by 0.768 (1⫺0.232). By following this logic, this proportion for Malawi is estimated to be 7.7% [10% (the midpoint for the proportion of new infections due to transfu-sion in the African region, estimated to be 5 to 15%)⫻0.768]. If we assume the same estimates for the entire continent and an annual number of 2.4 million new infections (24), of which 240,000 are due to blood transfusions, then screening of pools of six samples is expected to prevent about 57,600 new HIV infections in Africa.
DISCUSSION
The aim of this study was to estimate the possible delay of anti-HIV antibody detection by ELISA testing of pools of serum samples and the additional risk of this method caused by an increased risk of an FN result for a donor at seroconversion stage. The availability of such an estimate would legitimate the use of screening of pooled samples in developing countries when an increased risk of FN is of concern.
The estimated delay in the time to detection of the first positive sample in pools of up to 24 samples did not exceed 2 days compared with the time to detection by screening of singleton samples. If the average incubation period for HIV is
considered to be about 3 weeks (21 days), the delays observed for small pools of 6 to 12 samples each may not have a signif-icant impact on the risk of transmission of HIV by transfusion. The current investigation revealed that the risk of transfu-sion-transmitted HIV infection due to screening of pooled samples rather than screening of singleton samples does not exceed 9% of the baseline risk (defined as 1/1,067,000). Since the window period is considered the main reason that FN results are obtained (17) and the accuracy of screening of pooled samples was shown to be the same as that of screening of singleton samples, the overall risk from the screening of pooled samples is expected to be small.
The prevalence of a virus in a donor population seems to be a restricting factor for the implementation of screening of pooled samples in developing countries. This is because a higher prevalence increases the probability of having a positive sample in a pool and, therefore, the number of positive pools for which a full resolution will be needed. Thus, a scenario of screening of pools of 10 samples and a 10% prevalence of HIV infection is not expected to provide any benefits. According to the more accurate calculations performed in this study, when the prevalence rate in the donor population does not exceed 15%, screening of pools of 6 to 12 samples is expected to provide savings of up to 30% of tests. This is relevant to many countries, such as Malawi, (6) Congo, (20) India, (14), and Zimbabwe (9). According to our estimates, pooling of samples turns out to be highly beneficial, especially when the preva-lence rates are adjusted to the rates in the donor population. Screening of pools of six samples can prevent thousands of new HIV cases after transfusion cases each year and save substan-tial expenditures, based on the worst scenario used in the cost analysis (Fig. 1).
[image:4.585.71.514.69.305.2]Although the sample size and prevalence rates of the virus
FIG. 1. Expected (exp) savings in number of tests from screening of pooled samples compared to cost of screening of singleton samples for different prevalence (prev) rates.
on May 16, 2020 by guest
http://jcm.asm.org/
involved in this analysis have the most crucial effects on the benefits from screening of pooled samples, other factors can-not be totally neglected if a more accurate estimate of benefits is needed. A more profound analysis should take into account the cost of treatment of the patients infected by transfusion of a blood donation containing the virus due to an FN result because the donor was in the seroconversion or a later period, work disability, and decreased life expectancy, as well as the altered testing procedure, the need for additional training of laboratory personnel, and a change in the time of the testing procedure. The lack of consideration of these factors in the current analysis is the study’s main limitation.
While discussing screening of pooled samples for anti-HIV antibodies, we cannot neglect the existence of NATs and their wide application in industrialized countries. Can the applica-tion of this analytically sensitive assay with very large pools be economically beneficial, despite its high cost for singleton sam-ples? The authors see several problems with this solution, for instance, technical difficulties in performing NATs with large pools of samples, which require the collection of a large num-ber of blood units daily; satisfactory training of the laboratory personnel; and the current level of technical support for the infrastructure. All of these are very hard to achieve under the conditions encountered in many developing countries.
On the basis of the rough estimates provided here, screening of pooled samples can be considered for use in developing countries where testing is not performed at all or only occa-sionally due to its high cost. In these countries, screening of blood donations will make transfusion safer, even though not all positive units will be detected. The implementation of such a methodology requires a change from the “all-or-none” con-cept and could serve as a bridge prior to implementation of testing of singleton samples in some developing countries.
ACKNOWLEDGMENT
This study was funded by the U.S. Agency for International Devel-opment, Middle East Regional Committee (US-AID MERC).
This study is part of the Ph.D. dissertation of L. Novack.
REFERENCES
1.Anonymous.CDC finds Kenya’s blood stocks unsafe. AIDS Anal. Afr. 1995.5:2.
2.Avert.2006. HIV and AID statistics for Africa. [Online.] http://www.avert .org/subaadults.htm. Accessed 25 February 2006.
3.Avert.2006. Indian HIV and AIDS statistics. [Online.] http://www.avert .org/indiaadults.htm. Accessed 25 February 2006.
4.Busch, M., S. H. Kleinman, and G. J. Nemo.2003. Current and emerging infectious risks of blood transfusions. JAMA289:959–962.
5.Cahoon-Young, B., A. Chandler, T. Livermore, J. Gaudino, and R. Benjamin. 1989. Sensitivity and specificity of pooled versus individual sera in a human immunodeficiency virus antibody prevalence study. J. Clin. Microbiol.27:1893–1895.
6.Candotti, D., C. Mundi, G. Kadewele, W. Nkhoma, I. Bates, and J. P. Allain.
2001. Serological and molecular screening for viruses in blood donors from Ntcheu, Malawi: high prevalence of HIV-1 subtype C and of markers of hepatitis B and C viruses. J. Med. Virol.65:1–5.
7.Constantine, N.2005. HIV antibody assays. [Online.] http://hivinsite.ucsf .edu/InSite?page⫽kb-02&doc⫽kb-02-02-01. Accessed 31 August 2005. 8.Dodd, R. Y., E. P. Notari IV, and S. L. Starmer.2002. Current prevalence
and incidence of infectious disease markers and estimated window-period risk in the Red Cross blood donor population. Transfusion42:975–979.
9.Emmanuel, J. C., M. T. Basset, H. J. Smith, and J. A. Jacobs.1988. Pooling of sera for human immunodeficiency virus (HIV) testing: an economical method for use in developing countries. J. Clin. Pathol.41:582–585. 10.Fauci, A. S., and L. H. Clifford.2001. Human immunodeficiency virus (HIV)
disease: AIDS and related disorders, p. 1852–1913.InE. Braunwald, A. S. Fausi, D. L. Kasper, S. L. Hauser, D. L. Longo, and J. L. Jameson (ed.), Harrison’s principles of internal medicine, 15th international ed. The McGraw-Hill Companies, Inc., New York, N.Y.
11.Gibbs, W. N., and P. Corcoran.1994. Blood safety in developing countries. Vox Sang.67:377–381.
12.Glynn, S. A., S. H. Kleinman, D. J. Wright, and M. P. Busch.2002. Inter-national application of the incidence rate/window period model. Transfusion
42:966–972.
13.Heymann, S. J., and T. F. Brewer.1992. The problem of transfusion-asso-ciated acquired immunodeficiency syndrome in Africa: a quantitative ap-proach. Am. J. Infect. Control20:256–262.
14.Kapur, S., and A. Mittal.1998. Incidence of HIV infection and its predictors in blood donors in Delhi. Indian J. Med. Res.108:45–50.
15.Kline, R. L., T. A. Brothers, R. Brookmeyer, S. Zeger, and T. Quinn.1989. Evaluation of human immunodeficiency virus seroprevalence in population surveys using pooled sera. J. Clin. Microbiol.27:1449–1452.
16.Lackritz, E. M.1998. Prevention of HIV transmission by blood transfusion in the developing world: achievements and continuing challenges. AIDS
12(Suppl. A):S81–S86.
17.Lackritz, E. M., G. A. Satten, J. Aberle-Glasse, R. Y. Dodd, V. P. Raimondi, R. S. Janssen, et al.1995. Estimated risk of transmission of the human immunodeficiency virus by screened blood in the United States. N. Engl. J. Med.333:1721–1725.
18.Larkin, M.2000. WHO’s blood safety initiative: a vain effort. Lancet355:
1245.
19.Litvak, E., J. E. Siegel, S. G. Pauker, M. Lallemant, H. V. Fineberg, and M. C. Weinstein.1987. Whose blood is safer? The effect of the stage of the epidemic on screening for HIV. Med. Decision Making17:455–463. 20.Mbendi Nlombi, C., B. Longo-Mbenza, S. Mbendi Nsukini, J. J. Muye
Tamfum, H. Situakibanza Nanituma, and D. Vangu Ngoma.2001. Preva-lence of HIV and HBs antigen in blood donors. Residual risk of contami-nation in blood recipients in East Kinshasa, Democratic Republic of Congo. Med. Trop.61:139–142.
21.Moore, A., G. Herrera, J. Nyamongo, E. Lackritz, T. Granade, B. Nahlen, et al.2001. Estimated risk of HIV transmission by blood transfusion in Kenya. Lancet358:657–660.
22.National Center for Biotechnology Information. 2006. Adaptation of a model for economic impact of testing and treating HIV positive pregnant women and their babies in Minnesota. [Online.] http://www.ncbi.nlm.nih.gov /books/bv.fcgi?rid⫽hstat6.section.1250. Accessed 25 February 2006. 23.Raufu, A.2000. Rising HIV infection through blood transfusion worries
Nigerian health experts. AIDS Anal. Afr.11:15.
24.Salomon, J. A., D. R. Hogan, J. Stover, K. A. Stanecki, N. Walker, P. D. Ghys, and B. Schwartlander.2005. Integrating HIV prevention and treat-ment: from slogans to impact. PLoS Med.2:e16.
25.Schmunis, G. A., F. Zicker, F. Pinheiro, and D. Brandling-Bennet.1998. Risk for transfusion-transmitted infections diseases in Central and South America. Emerg. Infect. Dis.4:5–11.
26.Shrestha, P. N.1996. Transmission of HIV through blood or blood products in the eastern Mediterranean region. Eastern Mediterranean Health J.
2:283–289.
27.Wake, D. J., and W. A. Cutting.1998. Blood transfusion in developing countries: problems, priorities and practicalities. Trop. Doct.28:4–8. 28.Weinberg, P. D., J. Hounshell, L. A. Sherman, J. Godwin, S. Ali, C. Tomori,
et al.2002. Legal, financial, and public health consequences of HIV contam-ination of blood and blood products in the 1980s and 1990s. Ann. Intern. Med.136:312–319.
29.World Health Organization.2004. AIDS epidemic update: December 2004. Joint United Nations Program on HIV/AIDS, Geneva, Switzerland. [Online.] http://www.unaids.org/wad2004/EPI_1204_pdf_en/EpiUpdate04_en.pdf. Accessed 2 September 2005.
30.World Health Organization.2006. Blood centres in South-East Asia: collec-tion of blood. [Online.] http://w3.whosea.org/bct/blood_centers/ch9f.htm. Accessed 25 February 2006.
31.World Health Organization.2006. Strengthening of quality assurance in HIV and viral hepatitis in blood banks. World Health Organization, Geneva, Switzerland. [Online.] http://w3.whosea.org/EN/Section10/Section17/Section58 /Section879_3561.htm. Accessed 25 February 2006.