Abstract
CrescentCare, an organization in New Orleans, Louisiana, provides healthcare services and resources to uninsured and underserved populations with a specific focus on individuals with the human immunodeficiency virus (HIV). Data and input from CrescentCare staff indicate food insecurity, which is a lack of access to adequate and nutritious food, is a growing concern for people living with HIV in the Greater New Orleans area. Food insecurity and HIV
disproportionately affect low-income and minority populations, and the concurrence of these conditions may lead to an increased risk of HIV transmission, poor HIV-related health outcomes, increased medical costs, decreased quality of life, and an increase in health disparities. This paper analyzes the association between food insecurity and HIV and provides recommendations for CrescentCare to better address the high prevalence of food insecurity in the HIV positive population. These recommendations include: 1. utilization of a two-item, validated food insecurity screening instrument at initial and annual case management interviews, 2.
implementation of an acuity scale based on patients’ needs for the Food For Friends Pantry, and 3. referrals to the CrescentCare dietitians for patients who screen positive for food insecurity. These recommendations should lead to a decrease in the prevalence or severity of food insecurity in patients with HIV at CrescentCare, and successful implementation of these recommendations would provide data and guidelines for other organizations.
Introduction
The Food and Agriculture Organization (FAO) describes food insecurity as a lack of access to sufficient, safe, and nutritious food necessary for an active and healthy lifestyle due to physical, social, or economic barriers. 1 The relationship between food insecurity and the human
immunodeficiency virus (HIV) is complex, dynamic, and multi-factorial. Research suggests the occurrence of one of these conditions can increase the likelihood for the development, co-existence, or exacerbation of the other condition. Food insecurity can increase individuals’ risk for HIV or contribute to poor HIV-related health outcomes, while HIV can lead to increased medical complications and expenses that limit individuals’ abilities to work and afford adequate food.1 For example, a systematic review published by Singer et al. analyzed 19 papers from 18
consistent negative association” between food insecurity and HIV medication adherence in sixteen out of the nineteen studies. 2
Screening, prevention, and intervention efforts exist to address these issues separately, but research and efforts to address the impact of food insecurity on people with HIV still remain scarce in the United States. Since food insecurity and HIV disproportionately affect low-income and minority populations, this lack of information and intervention contributes to and worsens health disparities and inequities.3 The purpose of this paper is to describe food insecurity and
HIV, explore the association between food insecurity and HIV, and provide recommendations for an organization in New Orleans, CrescentCare, to better address food insecurity in patients with HIV.
Prevalence and Disparities
Despite major medical advancements, HIV still affects 36 million people worldwide and at least 1.1 million people in the United States according to data from the Henry J. Kaiser Family Foundation.4 Policies and organizations have increased awareness and access to preventive
methods, testing, and treatment; however, disparities continue to exist.5,6 Research from the CDC
indicates an association between poverty and HIV infection, and this association remains similar across racial and ethnic groups.5
The CDC estimates indicate that in 2015, approximately 40% of Americans living with HIV were African American.7 As of 2017, African Americans had the highest rate of new
diagnoses with eight times the rate of new diagnoses compared to white non-Hispanic Americans, and Latinos had three times the rate of new diagnoses compared to white
Americans.6 Gay and bisexual men constitute approximately 2% of the United States population,
but this group accounted for 68% of all new HIV diagnoses in 2015.4,7,8 Racial and ethnic
minorities within the gay and bisexual male community have significantly increased risks for HIV contraction due to the intersection of two high risk populations, 6 as shown in Figure 1. 9
Figure 1. New HIV Infection by Race and Transmission Groups from the United States Centers for Disease Control HIV Incidence: Estimated Annual Infections in the U.S., 2010-2016, Feb. 2019.9
History of HIV
Scientists hypothesize chimpanzees transferred the simian immunodeficiency virus (SIV) to humans in West Africa in the 1920’s or 1930’s.11 Once inside the body, the virus mutated into
HIV and eventually spread to the United States in the late 1970s.12 In 1981, doctors started
noticing groups of young, otherwise healthy gay men, developing rare forms of pneumonia and cancer in Los Angeles and New York due to severely suppressed immune systems. By the end of 1981, 45% of those affected by the disease had died. In subsequent years, people with
hemophilia, those who inject drugs, and females also developed the disease. The rapidly
progressing and unpredictable disease led to research that formally identified the HIV virus later in that decade.13
HIV Overview
majority of cases worldwide.14 Both strains of HIV attack the body’s immune system. CD4 cells,
also known as T cells, play an important role in fighting infections inside the body. Since the virus cannot replicate on its own, it uses CD4 cells for transportation and replication. After the virus replicates inside the CD4 cells, it destroys the cell and releases more HIV into the body’s bloodstream while simultaneously decreasing the number of CD4 cells.15
HIV transmission can only occur through body fluids that contain high enough concentrations of HIV. Those fluids include blood, semen, pre-seminal fluids, vaginal fluids, rectal fluids, and breast milk. The virus cannot remain active for long periods outside of the body, and it cannot replicate outside of a human host. Therefore transmission of HIV does not occur through air, water, saliva, sweat, insects, or pets, and it cannot be spread through kissing, touching, or sharing of dishes, food, or toilets.12 Usually, HIV transmission occurs via vaginal or
anal sex without preventive measures, such as condoms or HIV prevention medications, or through the sharing of needles, syringes, or other equipment used for drug injections. HIV can remain active for up to 42 days in a needle under the proper conditions, which makes needle sharing a risk factor for HIV. Less common methods of transmission occur during pregnancy, birth, or breastfeeding or through accidental sticks with HIV-contaminated materials.12
Stages of HIV
Although each individual experiences HIV differently, HIV infection occurs in three general stages. Stage 1 HIV refers to the acute infection period. The majority of people living with HIV begin to feel symptoms within two to four weeks of the infection. Symptoms typically last from a few days to weeks and include fever, chills, night sweats, muscle aches, sore throat, fatigue, swollen lymph nodes, and mouth ulcers. However, some individuals may be
asymptomatic for months or years.16 Regardless of the type or amount of symptoms, individuals
in the acute infection stage are highly contagious.12 During stage 2 HIV, also known as HIV
dormancy or chronic HIV, the virus is active but replicating at a slower rate, so individuals have mild symptoms or may be asymptomatic. Stage 3 HIV refers to acquired immunodeficiency syndrome (AIDS). An AIDS diagnosis occurs when an individual develops one or more opportunistic infections and/or a CD4 count below 200 per cubic millimeters of blood.16
neurologic disorders, often occur as a result of opportunistic infections rather than the virus itself.16
Diagnosis
There is a period after someone is infected where tests cannot accurately detect if a person has the virus. The window period is variable and depends on each individual person and the type of test used.12 If a person tests positive for HIV, it is important to seek and start
treatment immediately, even if the person is not currently experiencing any signs or symptoms.12
Treatment
In the last 30 years, there have been tremendous gains in HIV medication and treatment. Antiretroviral therapy (ART) was first developed in 1987, and these antiretroviral drugs have greatly reduced the mortality and morbidity rate for HIV.4,11 ART inhibits the virus’ ability to
replicate and decreases the viral load in the body. Viral load refers to the amount of virus present in the body.16 Viral suppression indicates that less than 200 copies of HIV are present per
milliliter of blood. Reaching viral suppression keeps individuals with HIV healthy and protects them from infections; however, the ultimate goal is an undetectable viral load.16 An undetectable
viral lead means that the virus is untransmittable because the virus is present in such low
amounts in an individual’s blood. An undetectable viral load requires less than 20 - 40 copies of the virus per milliliter of blood. In order to maintain an undetectable viral load, it is critical for patients to adhere to their medication regimen and to routinely have their viral load monitored.17
Seven classes of ART drugs currently exist. HIV regimens usually includes at least three medications from at least two drug classes in order to work effectively and prevent virus
mutations and subsequent drug resistance. Regimen and drug choices depends on the other medications, potency of drugs, comorbidities, potential side effects, and other individual factors like convenience.18 Today, most people with HIV can take one pill with three drugs inside, once
a day at the same time for HIV management with relatively minor side effects, such as nausea, diarrhea, and fatigue.19
these improvements do not necessarily lead to better overall health or well-being, and many individuals with HIV still face challenges regarding food and nutrition, such as food insecurity.
Food Insecurity
Food Insecurity Definition
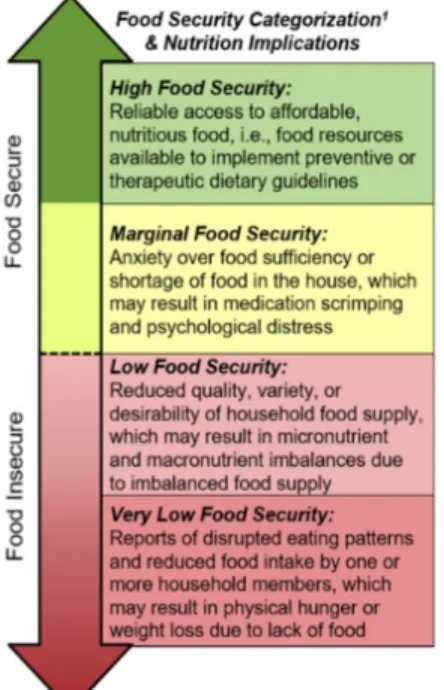
Food insecurity definitions differ among organizations, research, and countries, and most of these definitions include vague terminology and subjective measurement methods due to the complexity and multi-faceted nature of food insecurity. The United States Department of Agriculture (USDA) defines food insecurity as “lack of consistent access to enough food for a healthy, active lifestyle”. Food insecurity differs from hunger. Hunger refers to a physical sensation, while food insecurity refers to a lack of access to food. Food security describes a lack of problems accessing adequate and appropriate amounts and types of food.20 The USDA divides
food security into levels based on severity. Food security includes the high food security and marginal food security categories, while food insecurity includes the low food security and very low food security categories. Figure 2 below describes the classifications and the nutritional implications for each category. 21
Figure 2. Household Food Security Definitions and Possible Nutrition Implications
Associated with Household Food Supply from the Journal of the Academy of Nutrition and
Low or very low food security includes or may lead to food insufficiency, poor dietary quality and diversity, and poor food safety. Food insecurity contributes to diseases, health complications, and increased medical costs that decrease individuals’ quality of life and overall well-being.1
Reasons for Food Insecurity
Food insecurity can occur for a brief or extended period of time, and it can be due to a single factor or, more likely, a combination of factors. In recent years, the lack of availability of healthy foods and long distances to supermarkets has become a popular research and intervention topic. Additionally, lack of transportation, disability, unemployment, lack of eligibility for food assistance programs or resources, and lack of adequate money or income also greatly affect individuals’ and households’ food security status.22,23 Specific state requirements, such as
citizenship, work registration for able-bodied adults, and proof of residence and identity can all hinder eligibility for food assistance.24 No or little income also plays a major role in regards to
food security. A 2014 survey from Hunger in America showed that households receiving food assistance from Feeding America had to choose between the following:
1. Food and medical care (66% of households) 2. Food and utilities (69% of households) 3. Food and transportation (67% of households) 4. Food and housing (57% of households)22
Financial uncertainty or limitations often result in households or individuals making difficult choices, and this may mean prioritizing other necessities over food, which increases the likelihood or severity of food insecurity. Another reason for food insecurity involves a lack of knowledge regarding available resources and education about cost effective food purchasing.22
Increased opportunities and interventions for resource awareness and education about thrifty food purchasing and preparation could decrease the prevalence of food insecurity.
Food Insecurity and HIV Prevalence
Twenty-four to fifty percent of people living with HIV are estimated to be food insecure.3
(11.8%) in the United States experienced low or very low food security in 2017. African American and Hispanic households were more likely to experience food insecurity.22 In 2016,
22.3% of African American households and 18.5% of Hispanic households were food insecure compared to the national average of 12.3%.23 HIV also disproportionately affects minority
populations, which may partially explain why individuals living with HIV are more likely to be food insecure.5 The concurrence of food insecurity and HIV can lead to worse health outcomes
for individuals and populations that are already experiencing health disparities.
Food Insecurity and HIV
Although the exact mechanisms and definitive causes remain unknown, research suggests food insecurity contributes to poor HIV-related health outcomes and increases transmission and risk of HIV. Individuals with undiagnosed HIV or patients with difficulty accessing HIV treatment, often experience wasting, which is the loss of fat and muscle mass, and malnutrition. Wasting impacts nutrient absorption and increases metabolic rate, and these individuals require more calories per day. However, adverse health outcomes related to untreated HIV also may result in reduced ability to work, earn money, purchase, and prepare foods.25 This limits
individuals’ dietary intake and caloric consumption, and often results in poor nutritional status, which increases mortality risk among people with HIV.1,25 This vicious cycle further perpetuates
social, economic, and health disparities for the minority populations most affected and increases the usage of costly acute care.26
In individuals receiving HIV treatment, food insecurity can lead to adverse HIV clinical outcomes due to poor nutritional status. Studies have shown food insecurity and HIV,
individually and concurrently, are associated with increased risk for chronic diseases.1,22,27,28
HIV medications, HIV itself, longer life spans, and/or any combination of these factors appears to increase individuals’ risk of chronic diseases, and research studies show an association between initiation of ART for HIV treatment and increased rates of incident cardiovascular disease, diabetes, and weight gain.28 Additional conditions or diseases add burdens, such as more
appointments, medicines, lifestyle changes, and increased costs, that discourage medication adherence or HIV treatment and contribute to harmful stress.
transmission, especially among individuals with unsuppressed viral loads. Additional adverse outcomes include: reduced healthcare utilization, increased emergency room visits, lower health-related quality of life, lower body mass index, poor response to ART treatment, and
non-adherence to ART.1,3,26 These outcomes hinder efforts to prevent the spread of HIV and to reduce
health disparities.
Poor response to ART treatment or non-adherence to ART may occur in food insecure individuals with HIV because several ART medications, such as Genvoya, Complera, and Odefsey, include instructions to take the pills with food or a meal. These medications require food for proper absorption or protection against gastrointestinal side effects. Some medications even require pills to be taken with a meal and include specific calorie or fat requirements in order for the medication to work effectively. For food insecure individuals with HIV, fear of side effects from taking ART due to lack of food can decrease medication adherence. Food insecure individuals with HIV may also have competing resources, and they may have to choose between purchasing food or paying for their medication. Some individuals resort to selling their HIV medication in order to afford food.
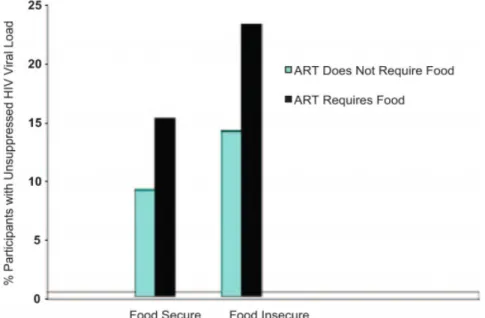
When individuals do not take their medication as prescribed, they often experience worse health-related outcomes, such as unsuppressed viral loads and lower CD4 counts, that hinder their ability to work and further increase the severity of food insecurity.2,29,30 Figure 3 from
Kalichman et al. shows the effect of food insecurity on ART adherence and HIV viral load with almost 25% of food insecure participants prescribed ART with food having unsuppressed HIV viral loads.31 It should be noted that food insecurity is just one factor in poor or non-adherence to
medication. Other factors related to stigma, lack of knowledge, emotional stress, and substance abuse also affect adherence to medication and potentially food insecurity status.2 Poor or
improper medication adherence could also lead to increased drug resistance, and an individual could develop cross resistance. Cross resistance occurs when HIV becomes resistant to a specific class of drugs, and any medication that contains that class of drug will not be effective for the individual.32
Therefore, Kalichman and et al. recommend thoroughly assessing access to food and other psychosocial factors before prescribing ART, consistently monitoring food security levels and HIV-related outcomes, and providing patients with resources and food assistance
and outlines recommendations for CrescentCare to better address food insecurity in its patients with HIV.
Figure 3. Modifying Effect of Food Insecurity on ART regimen and HIV Viral Load Suppression from Kalichman.31
Background Information for CrescentCare in New Orleans
CrescentCare began in New Orleans, Louisiana in 1983 as the NO/AIDS Task Force during the early stages of the AIDS epidemic. CrescentCare evolved and grew, and in 2013, it became a federally qualified health center (FQHC). The organization originally only served patients with HIV, but it now serves all individuals. However, the organization strives to provide care for the underserved and uninsured populations, such as minority populations, the lesbian, gay, bisexual, transgender, queer, plus (LGBTQ+) community, immigrants, and people living with HIV. CrescentCare acts as a medical home with care coordination, and they offer the following services: primary medical care, behavioral health, medical nutrition therapy, women’s health, LGBTQ+ health services, pre-exposure prophylaxis (PrEP) and post-exposure
if uninsured and eligible. CrescentCare receives funding from the Ryan White HIV/AIDS Program, and therefore, the organization can provide additional services and resources for patients with HIV. These services include HIV medical clinic care, legal services, case management, Food For Friends pantry and home-delivered meals, health education, and peer support.33
CrescentCare and Local Demographics
CrescentCare mainly serves residents from the Greater New Orleans Area, also referred to as the New Orleans Metropolitan Statistical Area (MSA), which includes eight parishes. Twenty-five percent of CrescentCare’s 31,261 patients reside in Orleans Parish, and 3,275 of CrescentCare’s patients have HIV. As of 2019, Louisiana ranks fourth in the nation for HIV case rates and third in AIDS case rates. The New Orleans MSA ranks fourth in HIV case rates and sixth for AIDS case rates for metropolitan areas. Although the number of new HIV/AIDS diagnoses is decreasing in Louisiana, the number of Louisianans living with HIV is increasing.34
As of March 2019, 22,119 residents in Louisiana and 8,564 residents in the New Orleans MSA are living with HIV. Similar to data reports from other regions in the United States, HIV disproportionately affects minority populations in Louisiana, specifically African Americans. In 2018, 70% of newly diagnosed HIV cases and 72% of newly diagnosed AIDS cases were among African Americans. African Americans comprise 60.8% of the Orleans Parish population, and Orleans Parish accounts for 23.7% of all HIV cases in Louisiana.34,35 One-fourth of
CrescentCare’s HIV patients reside in Orleans Parish, and the parish contains a high percentage of people living with HIV and populations vulnerable to contracting HIV.33 Therefore, the
following data on poverty and food insecurity will focus on Orleans Parish.
The United States Census Bureau estimates that 25.4% of residents in Orleans Parish are living at or below the established federal poverty level, while the percentage is much lower for the state overall at 19.6%.36 The African American population contains the highest percentage of
residents living in poverty in Orleans Parish at 33.2%.35,36 As of 2017, 21.8% of Orleans Parish
residents were food insecure compared to 17.3% of residents in Louisiana.20,37
greater than one mile from the nearest supermarket or grocery store. Conversely, the Food Environment Atlas described Orleans Parish as having a high amount of fast food restaurants for its population with 0.79 fast food restaurants per 1,000 residents.38 These statistics emphasize
that food insecurity and risk factors for food insecurity, such as poverty and poor food
environments, are significant for residents in Louisiana, and Orleans Parish in particular. With a large HIV population and a significant portion of the New Orleans area impacted by food insecurity, it is critical to address these two issues, which can be syndemic.
Efforts to Address Food Insecurity and Opportunities for Improvement Case Management
CrescentCare currently has measures in place to address food insecurity in its HIV population. CrescentCare provides case management services for patients living with HIV. Case managers conduct initial and annual assessments. During these assessments, case managers ask if the patients have access to the following: Supplemental Nutrition Assistance Program (SNAP), Women, Infants, and Children (WIC), Food For Friends Pantry, home-delivered meals,
congregate meals, and nutrition counseling. Case managers ask if patients would like to access any of these services in the future, and they can help determine patients’ eligibility and provide resources or referrals.
The opportunity for improvement lies in moving beyond asking if they have access to food assistance and instead directly assessing food insecurity using a validated tool. Availability and use of food assistance do not mean that individuals or households are necessarily food secure. Steven Carlson, a research analyst for the Center on Budget and Policy Priorities, reports that as of 2019, almost half of SNAP participants still experience food insecurity and do not have access to foods necessary to promote an active, healthy lifestyle.39 The USDA creates a Thrifty
Food Plan to determine SNAP benefits that will provide adequate nutrition. However, Carlson explains the Thrifty Food Plan does not account for fluctuations in food prices and the amount of time and resources necessary to prepare meals.39 The Thrifty Food Plan assumes people purchase
raw ingredients and prepare meals from scratch, when in reality, most individuals have to buy more convenient, more expensive options due to time restraints. Research estimates that SNAP recipients need approximately $11 more per week to be able to purchase and prepare
food insecurity. It is critical to have a standardized method to directly assess food insecurity and to record the prevalence of food insecurity in CrescentCare’s HIV positive population.
Food For Friends Pantry
CrescentCare currently houses the Food For Friends Pantry funded by the Ryan White HIV/AIDS Program. Eligibility requirements include: HIV positive diagnosis, residence in the New Orleans metropolitan area, finances at or below 200% of the federal poverty level, and proper screening by a case manager for other food assistance programs. Patient eligibility is renewed every 6 months as long as the patient still meets eligibility requirements and has not missed three consecutive months of receiving pantry items. Patients receive 40 pounds of food, beverages, personal hygiene products, and cleaning products every month.33
Unfortunately, due to the high demand and limited funding, staffing, and space, most patients must be put on a waiting list for the pantry. Discussions with the registered dietitian and a case manager at CrescentCare revealed that patients with more resources and less risk of food insecurity or poor nutritional status often become eligible for the Food For Friends Pantry before individuals with higher needs and less resources. Since the Ryan White HIV/AIDS Program acts as a “last resort”, it would be beneficial to implement an acuity scale to prioritize patients on the waiting list who have a greater need for food assistance and pantry access. The acuity scale would only apply to patients on the waiting list and not patients who are renewing their eligibility since this would place undue burden on case managers and the re-eligibility process already includes specific requirements.
Dietitians and Medical Nutrition Therapy
Currently, there is no official dietitian referral process for patients who experience food insecurity, and patients may not know to ask to see a dietitian to help with food security related issues. Often, the dietitians discover that a patient is experiencing food insecurity during their assessments in sessions. However, many patients experiencing food insecurity are not referred to the dietitians due to a lack of screening. Once the food insecurity screening is implemented, it would be beneficial to refer patients who screen positive for food insecurity to one of the dietitians. This increased opportunity for medical nutrition therapy could reduce, delay, or prevent health and nutrition-related complications that can occur from medical conditions associated with food insecurity and HIV, such as obesity, diabetes, and cardiovascular disease.
Recommendations for CrescentCare in New Orleans to Improve Screening for Food Insecurity in People Living with HIV
The following recommendations for CrescentCare utilized research, evidence-based best practices, personal experience at the organization, and input from staff and patients. The goal of these recommendations is to improve food insecurity screening and interventions for
CrescentCare’s HIV population.
1. Include the following validated food insecurity questions in the initial and annual case management interviews.
Table 1. Food Insecurity Questionnaire Within the past 12 months, I was worried whether my food would run out before I got money for more.
- Often True - Sometimes True - Never True
Within the past 12 months, the food I bought just did not last, and I did not have money to get more.
- Often True - Sometimes True - Never True
An answer of “Often True” or “Sometimes True” for either or both questions listed in Table 1 results in a positive food insecurity screening.40 Medical providers and facilities use
completed (ICD10 code Z659) and to indicate a positive screen for food insecurity (ICD10 code Z59.4).40
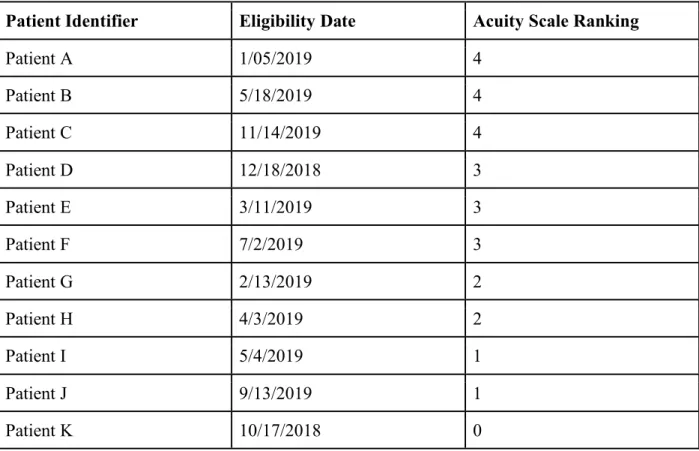
2. Implement the utilization of an acuity scale to rank patients on the waiting list for Food For Friends Pantry to assure patients with the greatest need receive food assistance first.
The inclusion of an acuity scale would allow CrescentCare to rank patient eligibility for Food For Friends Pantry services based on their acuity scale score and length of time on the waiting list. The acuity scale score ranges from zero to five, with five indicating the highest acuity. This acuity scale was adapted from the eligibility guidelines determined by Food and Friends, an organization that provides food and meals to patients with HIV/AIDS, cancer, or other serious illnesses.41 The five selected conditions include:
1. Positive food insecurity screen
2. HIV Wasting Syndrome diagnosis within the past year or significant unintentional weight loss (≥ 5% in 1 month or ≥ 10% in 6 months)
3. BMI ≤ 19 (underweight classification) 4. Confirmed pregnancy
Table 2. Example Food For Friends Pantry Waiting List
Patient Identifier Eligibility Date Acuity Scale Ranking
Patient A 1/05/2019 4
Patient B 5/18/2019 4
Patient C 11/14/2019 4
Patient D 12/18/2018 3
Patient E 3/11/2019 3
Patient F 7/2/2019 3
Patient G 2/13/2019 2
Patient H 4/3/2019 2
Patient I 5/4/2019 1
Patient J 9/13/2019 1
Patient K 10/17/2018 0
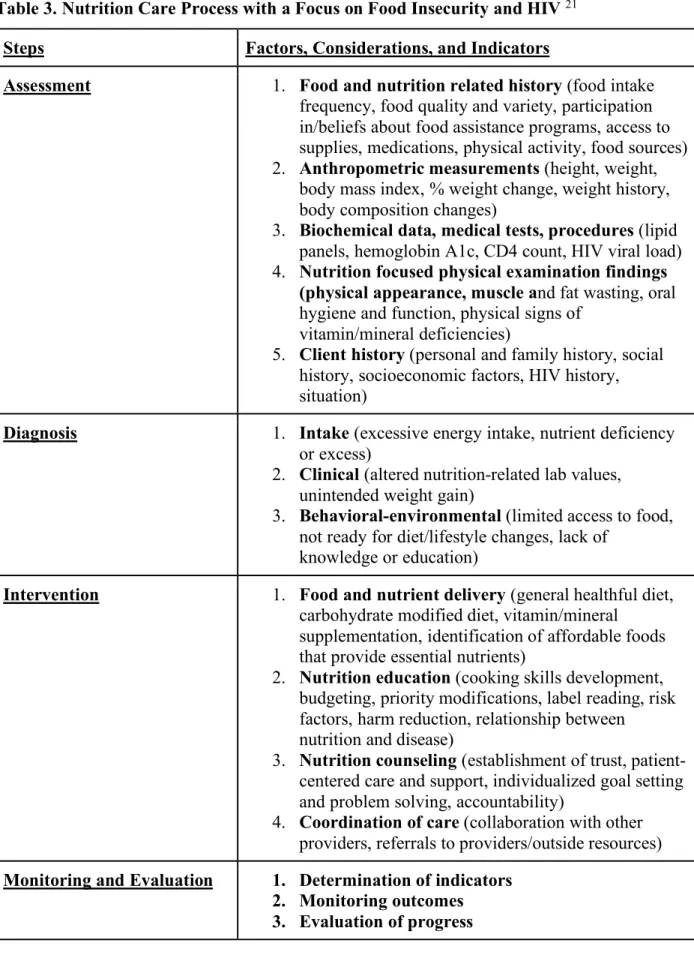
3. Refer patients to the registered dietitian for medical nutrition therapy (MNT) and education when they screen positive for food insecurity.
The dietitians will utilize the nutrition care process (NCP), as shown in Table 3 below, to assess the patients’ medical conditions, needs, and barriers. The NCP includes assessing,
Table 3. Nutrition Care Process with a Focus on Food Insecurity and HIV 21
Steps Factors, Considerations, and Indicators
Assessment 1. Food and nutrition related history(food intake frequency, food quality and variety, participation in/beliefs about food assistance programs, access to supplies, medications, physical activity, food sources) 2. Anthropometric measurements (height, weight,
body mass index, % weight change, weight history, body composition changes)
3. Biochemical data, medical tests, procedures (lipid panels, hemoglobin A1c, CD4 count, HIV viral load) 4. Nutrition focused physical examination findings
(physical appearance, muscle and fat wasting, oral hygiene and function, physical signs of
vitamin/mineral deficiencies)
5. Client history (personal and family history, social history, socioeconomic factors, HIV history, situation)
Diagnosis 1. Intake (excessive energy intake, nutrient deficiency or excess)
2. Clinical (altered nutrition-related lab values, unintended weight gain)
3. Behavioral-environmental (limited access to food, not ready for diet/lifestyle changes, lack of
knowledge or education)
Intervention 1. Food and nutrient delivery (general healthful diet, carbohydrate modified diet, vitamin/mineral
supplementation, identification of affordable foods that provide essential nutrients)
2. Nutrition education (cooking skills development, budgeting, priority modifications, label reading, risk factors, harm reduction, relationship between nutrition and disease)
3. Nutrition counseling (establishment of trust, patient-centered care and support, individualized goal setting and problem solving, accountability)
4. Coordination of care (collaboration with other providers, referrals to providers/outside resources)
Implications for Future Research
Food insecurity is a multidimensional problem that occurs on a spectrum and requires more constant monitoring and the use of multi-assessment tools to truly understand the problem and its etiology. Food insecurity is dynamic, and individuals’ food security may change over periods of time at different frequencies due to environmental, social, physical, or financial reasons, and future tools should assess and consider these changes and fluctuations. As previously mentioned in this paper, organizations and healthcare professionals define and measure food insecurity differently. More concrete, uniform definitions and measurements are necessary in order to better collect and analyze data and implement interventions. Research regarding the effect of medical nutrition therapy by a registered dietitian on food security remains scarce, and more information could provide evidence for the use and effectiveness of dietitians in this area. Additionally, research remains limited on the prevalence of food insecurity in the HIV population and its effect on health and overall quality of life.
Although these recommendations are based on research and evidence, several gaps in the literature and data exist regarding HIV. Further research is needed regarding the biological, physical, and social connection between chronic diseases and HIV. Few studies exist that
examine the effect of interventions to address food insecurity in the HIV population or the rising prevalence of chronic diseases for people with HIV. Ideally, the recommendations provided for CrescentCare would allow them to collect data, implement interventions, and analyze outcomes and results that would provide more information regarding this topic.
Conclusion
References
1. Anema A, Fielden SJ, Castleman T, Grede N, Heap A, Bloem M. Food Security in the Context of HIV: Towards Harmonized Definitions and Indicators. 2013.
doi:10.1007/s10461-013-0659-x
2. Singer AW, Weiser SD, McCoy SI. Does Food Insecurity Undermine Adherence to Antiretroviral Therapy? A Systematic Review. AIDS Behav. 2015;19(8):1510-1526. doi:10.1007/s10461-014-0873-1
3. Willig A, Wright L, Galvin TA. Practice Paper of the Academy of Nutrition and
Dietetics: Nutrition Intervention and Human Immunodeficiency Virus Infection. Journal
of the Academy of Nutrition and Dietetics.2018;118(3):486-498.
doi:10.1016/j.jand.2017.12.007.
4. The HIV/AIDS Epidemic in the United States: The Basics. The Henry J. Kaiser Family Foundation. https://www.kff.org/hivaids/fact-sheet/the-hivaids-epidemic-in-the- united-states-the-basics/. Published 2019. Accessed September 8, 2019.
5. Today's HIV/AIDS Epidemic. Centers for Disease Control and Prevention; 2016.
https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/todaysepidemic-508.pdf. Accessed November 2019.
6. CDC. HIV Surveillance Report, Diagnoses of HIV Infection in the United States and Dependent Areas, 2017. Vol. 29; November 2018. HIV diagnosis data are estimates from 50 states, the District of Columbia, and 6 U.S. dependent areas. Estimates for 2017 are preliminary and are not included in trend calculations.
7. CDC. Supplemental Surveillance Report. Estimated HIV Incidence and Prevalence in the United States 2010-2015. Vol 23. No. 1. 2018.
8. CDC. HIV Surveillance Supplemental Report, Monitoring Selected National HIV Prevention and Care Objectives by Using HIV Surveillance Data. Vol. 23, No. 4; June 2018.
9. HIV Incidence: Estimated Annual Infections in the U.S., 2010-2016. Centers for Disease Control. Published February 2019. Accessed September 20, 2019.
10. Fields-Gardner C. Position of the American Dietetic Association: Nutrition Intervention and Human Immunodeficiency Virus Infection. J Am Diet Assoc. 2010;110(7).
doi:10.1016/j.jada.2010.05.020
11. History of HIV and AIDS Overview. AVERT. https://www.avert.org/professionals/ history-hiv-aids/overview. Published 2018. Accessed August 22, 2019.
12. About HIV/AIDS | HIV Basics. CDC. https://www.cdc.gov/hiv/basics/whatishiv.html. Published 2019. Accessed August 22, 2019.
14. HIV strains and types. AVERT. https://www.avert.org/professionals/hiv-science/types- strains. Published 2019. Accessed August 22, 2019.
15. How HIV infects the body and the lifecycle of HIV. AVERT.
https://www.avert.org/about-hiv-aids/how-infects-body. Published 2019. Accessed August 22, 2019.
16. HIV Basics. U.S. Department of Health and Human Services. https://www.hiv.gov/hiv- basics. Accessed August 26, 2019.
17. What does undetectable mean? Avert. https://www.avert.org/living-with-hiv/ antiretroviral-treatment/what-does-undetectable-mean. Published 2019. Accessed September 20, 2019.
18. HIV Treatment: The Basics. AIDSinfo. https://aidsinfo.nih.gov/understanding -hiv-aids/fact-sheets/21/51/hiv-treatment--the-basics. Published 2019. Accessed September 20, 2019.
19. Antiretroviral Drug Discovery and Development. NIH: National Institute of Allergy and Infectious Diseases. https://www.niaid.nih.gov/diseases-conditions/antiretroviral -drug-development. Accessed September 8, 2019.
20. Coleman-Jensen A, Rabbitt MP, Gregory CA, Singh A. Household Food Security in the
United States in 2017.; 2018. www.ers.usda.gov. Accessed September 11, 2019.
21. Wetherhill MS, White KC, Rivera C. Food Insecurity and the Nutrition Care Process: Practical Applications for Dietetics Practitioners. J Acad Nutr Diet.
22. Weinfield NS, Mills WG, Borger C, et al. Hunger in America 2014 National Report
Prepared for Feeding America.; 2014. Accessed September 17, 2019.
23. Healthy People 2020: Food Insecurity. Office of Disease Prevention and Health
Promotion. https://www.healthypeople.gov/2020/topicsobjectives/topic/social
-determinants -health/interventions-resources/food-insecurity#2. Accessed September 20, 2019.
24. Supplemental Nutrition Assistance Program (SNAP). | Department of Children & Family Services: State of Louisiana.
http://www.dcfs.la.gov/index.cfm?md=pagebuilder&tmp=home&nid=326&pid=93#unde fined. Accessed September 15, 2019.
25. Mangili A, Murman DH, Zampini AM, Wanke CA. Nutrition and HIV Infection: Review of Weight Loss and Wasting in the Era of Highly Active Antiretroviral Therapy from the
Nutrition for Healthy Living Cohort. Vol 42.; 2006.
https://academic.oup.com/cid/article-abstract/42/6/836/286703. Accessed September 8, 2019.
26. Weiser SD, Hatcher A, Frongillo EA, et al. Food insecurity is associated with greater acute care utilization among HIV-infected homeless and marginally housed individuals in San Francisco. J Gen Intern Med. 2013;28(1):91-98. doi:10.1007/s11606-012-2176-4 27. Seligman HK, Laraia BA, Kushel MB. Food insecurity is associated with chronic disease
28. Miles-Chan JL, Carmichael OT, Chrousos GP, Kumar S, Samaras K. The Impact of Weight Gain During HIV Treatment on Risk of Pre-diabetes, Diabetes Mellitus, Cardiovascular Disease, and Mortality. Front Endocrinol | www.frontiersin.org. 2018;9:705. doi:10.3389/fendo.2018.00705
29. Young S, Wheeler AC, McCoy SI, Weiser SD. A review of the role of food insecurity in adherence to care and treatment among adult and pediatric populations living with HIV and AIDS. AIDS Behav. 2014;18 Suppl 5(0 5):S505-15. doi:10.1007/s10461-013-0547-4 30. de Pee S, Grede N, Mehra D, Bloem MW. The Enabling Effect of Food Assistance in
Improving Adherence and/or Treatment Completion for Antiretroviral Therapy and Tuberculosis Treatment: A Literature Review. AIDS Behav. 2014;18(S5):531-541. doi:10.1007/s10461-014-0730-2
31. Kalichman SC, Washington C, Grebler T, et al. Treatment outcomes among people living with HIV who are food insecure and prescribed antiretrovirals taken with food. J Prim
Care Community Health. 2015;6(1):35-40. doi:10.1177/2150131914549055
32. Drug Resistance. AIDS Info. https://aidsinfo.nih.gov/understanding-hiv-aids/ fact-sheets/21/56/drug-resistance/. Published 2019. Accessed September 23, 2019.
33. CrescentCare. CrescentCare. https://crescentcarehealth.org/. Accessed September 19, 2019.
34. Gruber D, Johnson C, Burgess S, Assefa T. Louisiana HIV, AIDS, and Early Syphilis
Surveillance Quarterly Report - March 31, 2019. New Orleans; 2019.
http://dhh.louisiana.gov/hiv.
35. American FactFinder. U.S. Census Bureau. https://factfinder.census.gov/faces/nav /jsf/pages/index.xhtml. Accessed September 23, 2019.
36. Maps and Data. Poverty USA. http://www.povertyusa.org/data/2017/LA/orleans-parish. Published 2017. Accessed September 23, 2019.
37. Food Insecurity in Orleans Parish. Feeding America.
https://map.feedingamerica.org/county/2017/overall/louisiana/county/orleans. Published 2017. Accessed September 23, 2019.
38. Food Environment Atlas. United States Department of Agriculture: Economic Research Service. https://www.ers.usda.gov/data-products/food-environment-atlas/go-to-the-atlas/. Published 2015. Accessed September 23, 2019.
39. Carlson S. More Adequate SNAP Benefits Would Help Millions of Participants Better Afford Food. Center on Budget and Policy Priorities.
https://www.cbpp.org/research/food-assistance/more-adequate-snap-benefits-would-help-millions-of-participants-better. Published July 30, 2019. Accessed October 14, 2019. 40. Hager ER, Quigg AM, Black MM, et al. Development and Validity of a 2-Item Screen to
Identify Families at Risk for Food Insecurity. Pediatrics. 2010;126(1). doi:10.154/peds.2009-3146.
Appendix
1. Questions Used to Assess the Food Security of Households in the CPS Food Security Supplement. 20